
We audited a multi-program treatment center last month with 247 blog posts on the site. The marketing director walked us through the content library proudly.
Eighteen months of weekly publishing. Cycling topics across addiction, mental health, family support, and recovery. Every post was 800 to 1,200 words. Every byline read “Editorial Team.”
The pages produced 11,400 organic sessions a month. The admissions team could not trace a single admit back to a blog post in the prior six months.
This is the most common pattern we see in behavioral health content marketing. The publishing cadence is real. The traffic is real. The admit-attributed conversion is zero, because the content the operator is publishing is not the content that drives admits.
The nine content types below are the ones we have watched produce measurable admit-attributed conversion across our content SEO program for treatment centers.
They are ordered by where they sit in the admit funnel, from the family-member first-touch at 11 PM down to the late-funnel comparison page the prospect reads the night before they call.
The 247-post library above had almost none of these nine types built well. The fix was not “publish more.” The fix was “publish the right nine.”
Key Takeaways
- Most treatment center content libraries publish high-volume informational content that ranks for the wrong queries and converts almost nothing. The fix is type-specific content built around what family members, patients, and referral sources actually search for at each stage of the admit funnel.
- Family-facing “what to do when…” content is the highest-converting category in behavioral health because family members initiate roughly 60 percent of inquiry calls in residential treatment. Most facilities under-invest in family-voice content by a factor of 5 to 10.
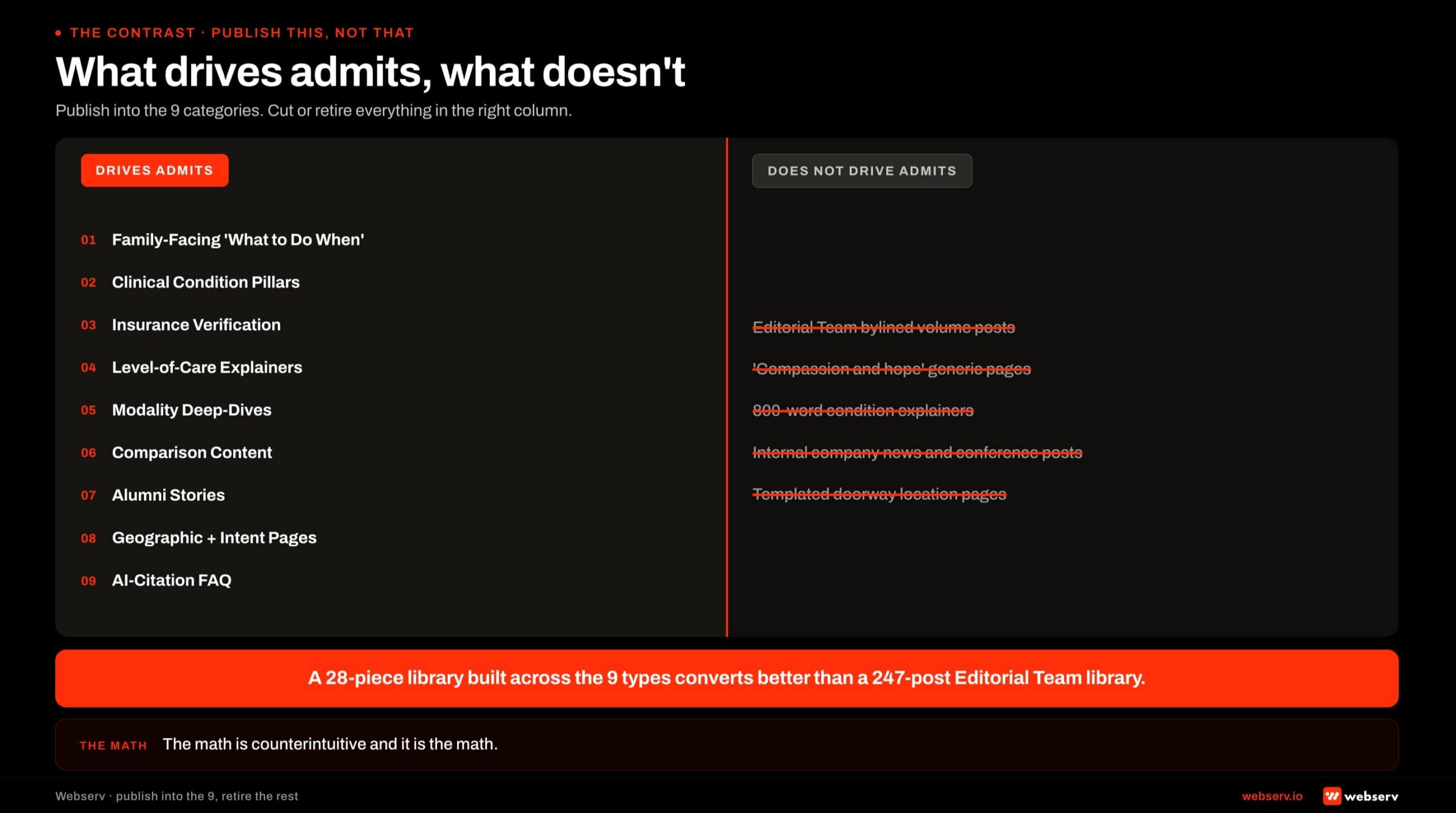
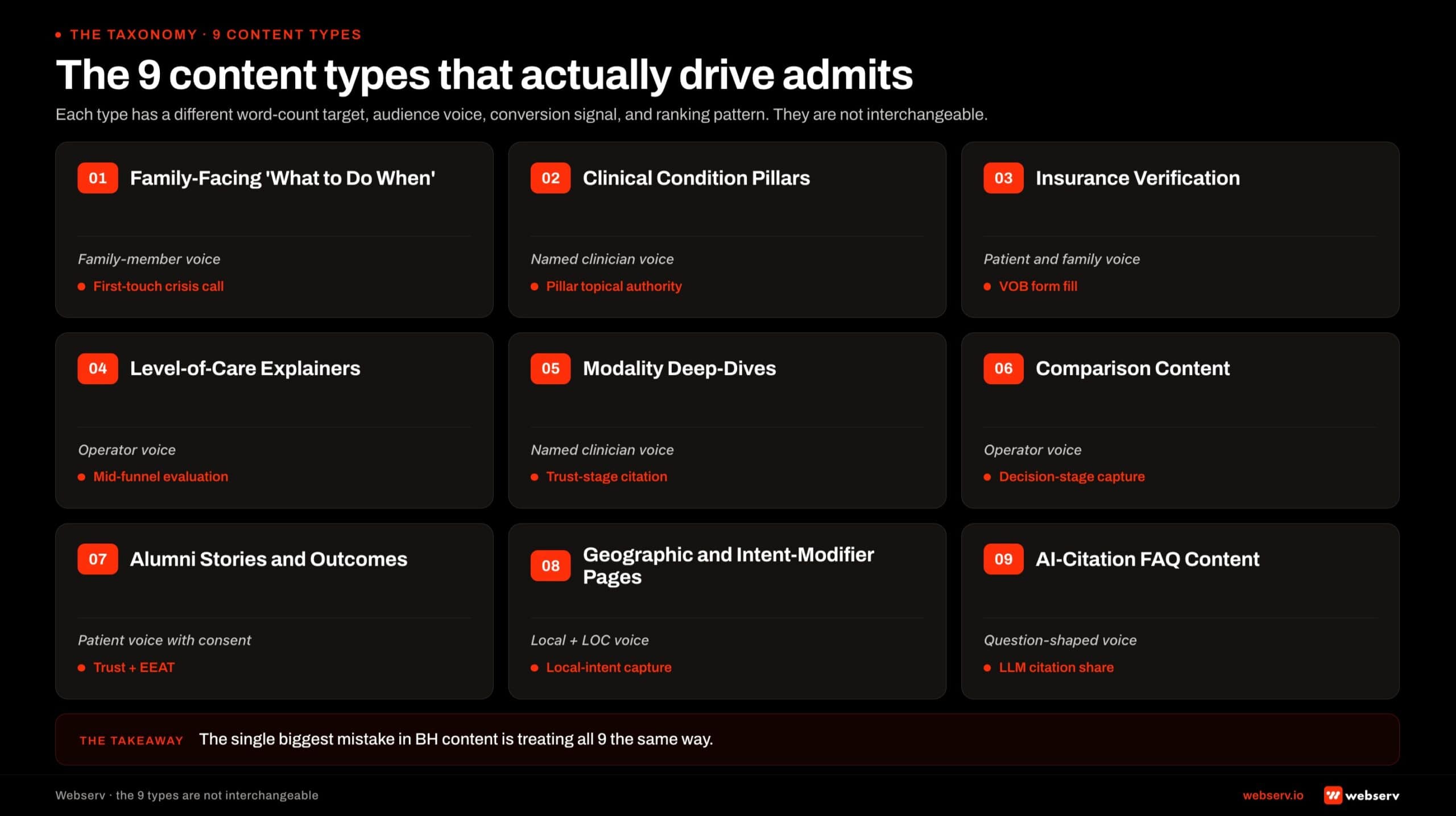
- The nine admit-driving content types span the full funnel: family-facing first-touch content, clinical condition pillars, insurance verification, level-of-care explainers, modality deep-dives, comparison pages, alumni stories, geographic intent pages, and AI-citation-optimized FAQ content.
- Each type has a different word-count target, audience voice, conversion signal, and ranking pattern. The single biggest mistake in behavioral health content is treating all nine the same way (same length, same tone, same internal linking, same CTA pattern). The 9 types succeed or fail on the differences.
- The 247-post Editorial Team library converts worse than a 28-piece library built deliberately across the 9 types. The math is counterintuitive and it is the math.
1. Family-Facing “What to Do When…” Content
The single highest-converting content category in behavioral health is content addressed directly to the family member of a person in active addiction or mental health crisis.
Family members are the load-bearing decision-makers for residential treatment admissions. They place the first call. They run the insurance verification. They pay the deposit.
SAMHSA’s National Survey on Drug Use and Health consistently documents the gap between people who meet criteria for SUD treatment and those who actually enter treatment, and the family member is overwhelmingly the bridge between the two states.
The vocabulary of family search is different from clinical vocabulary. A mother of a 22-year-old in active opioid use does not search “substance use disorder residential treatment.”
She searches “what to do when your son is using fentanyl,” “how to get my child into rehab,” and “how do I know if it’s time for treatment.”
Family-facing content that addresses the mother directly (acknowledging the panic, the timeline pressure, the financial fear, the relationship strain) outperforms patient-voice content across behavioral health conversion metrics. The reason is structural.
The patient is rarely the one researching at 11 PM. The patient is in a hotel room, a basement, or an ER bay. The family member is the one with the laptop.
What makes this category convert: directness about the situation the family is actually in, concrete next-step language, no jargon without translation, and a CTA that respects the time pressure (a phone number, not a 12-field intake form).
Length is in the 1,800 to 2,800 word range. The family member is not browsing; she is researching one specific decision and she will read every word.
What kills this category: clinical voice, generic “compassion and hope” framing, and content that addresses the patient as the reader.
We cover the deeper read on this in the case against generic healthcare content farms in addiction treatment. The short version is that the family member can spot AI-generated, voice-of-nobody content in 15 seconds and clicks back to the SERP.
The Reddit strategy for AEO citations in behavioral health is the closest adjacent read on the family-voice problem we solve from a different angle.
2. Clinical Condition Pillar Pages With Named Authorship
The next category is the core E-E-A-T anchor for the entire content cluster.
Condition pillar pages (alcohol use disorder, opioid use disorder, anxiety disorders, depression, co-occurring disorders, eating disorders, trauma) are the pages Google’s healthcare-specific Quality Rater Guidelines evaluate against the strictest YMYL E-E-A-T threshold, and the pages that anchor topical authority across everything else.
A condition pillar runs 3,500 to 6,000 words. Named clinical author. Named clinical reviewer. Inline peer-reviewed citations to SAMHSA, NIDA, NIMH, JAMA Psychiatry, or ASAM publications. Clinical-vocabulary register paired with patient-vocabulary equivalents so the page ranks for both registers of search.
What makes this category convert: the pillar is rarely the page that produces the admit, but it is the page that produces the topical authority that makes the cluster rank, and the page the family member or patient ends up reading the day before they call.
The pillar’s job is to establish that the facility is the authority on this condition. The cluster pages around it produce the actual conversion.
The named-author signal is load-bearing. Author bios that build E-E-A-T for behavioral health blogs covers the bio anatomy that carries weight.
Without named authorship and reviewer credit, the condition pillar performs as if it does not exist for YMYL ranking. With named authorship and reviewer credit, the pillar produces the topical authority lift that makes every cluster sibling rank better.
What kills this category: 1,200-word condition explainers, Editorial Team bylines, citations to other blog posts instead of peer-reviewed sources, and writing the page as if Google were the reader rather than the patient or family member.
A 247-post Editorial Team library producing 11,400 monthly sessions and zero admit-attributed conversions is the most expensive failure mode in behavioral health content.
The fix is never “publish more.” The fix is to cut the library to the 9 types that actually move admits, written under named clinicians, with the discipline the YMYL frame requires.
Preston Powell, CEO of Webserv
3. Insurance Verification and “Does My Insurance Cover Rehab” Content
The highest commercial intent in behavioral health search lives on the insurance side. Queries like “does Blue Cross cover rehab,” “rehab covered by Anthem,” “Aetna inpatient treatment,” and “how to verify my insurance for treatment” all sit one step away from the inquiry call.
The conversion pattern is direct. The family member or patient lands on the page asking a specific insurance question, gets a specific answer, and is given a single next step.
That next step is to verify insurance now, by phone or by the facility’s online VOB form. Content that answers the question and routes to verification converts admits at a materially higher rate than content that meanders through legal disclaimers and ends with a generic “contact us.”
What makes this category convert: clear answers about the specific payor, transparency about in-network vs out-of-network status (without bashing the payor), a same-page VOB CTA, and operator-direct voice. The page should respect that the reader is one decision away from picking up the phone.
What kills this category: “every case is unique, contact us to learn more,” vague references to “most major insurance accepted,” and forms with more than 4 fields. The patient or family member abandons. The competitor who answered the same question in 200 fewer words gets the admit.
The compliance frame matters here. Insurance content should not promise coverage or commit to a specific reimbursement. The page should give the reader the next step (verification) without pretending to be a benefits determination. The legal review pass on this category is short and important.
4. Level-of-Care Explainers With Operational Specifics
Detox, residential, partial hospitalization (PHP), intensive outpatient (IOP), outpatient, sober living, and aftercare each deserve a dedicated page. The level-of-care explainer is where the prospect transitions from “this facility might help me” to “I understand what they actually do.”
A level-of-care page runs 1,500 to 2,500 words. Clinical voice paired with operational specifics. The typical day. The clinical hours. The medical oversight. The insurance pattern. The length of stay. The transition criteria to the next level of care.
The page should read as if the clinical director walked the family member through the program.
What makes this category convert: operational specificity (not generic “individualized treatment” language), clarity on who fits this level of care and who does not, transparency about the admissions process, and named clinician contributions where possible.
The reader is making a clinical-fit assessment, and the page either earns the assessment or loses it.
The level-of-care page is also the page Google and AI Overviews most often pull from when a reader asks “what is PHP” or “what is the difference between residential and IOP.”
Strong topical authority anchored across the level-of-care pages is the difference between AI Overviews citing the facility and AI Overviews citing a competitor’s content.
What kills this category: 800-word stub pages, identical templated copy across all five level-of-care pages, and “every patient is unique” framing that avoids saying anything specific.
5. Modality Deep-Dives
Cognitive behavioral therapy (CBT), dialectical behavior therapy (DBT), EMDR, MAT, trauma-informed care, ketamine-assisted therapy, TMS, family therapy, group therapy.
Modality pages are the category that earns the educated patient and family-member traffic, the patients who have already done some research and are evaluating which clinical approach fits.
The clinicians-as-AEO-moat framing is the deeper read on why named-clinician modality content carries outsized E-E-A-T weight in this category.
A modality deep-dive runs 2,000 to 3,500 words. Clinical voice. Named clinical author.
Specifics about how the facility delivers the modality, who is qualified to deliver it, what conditions it is most effective for, what the evidence base looks like, and how it fits inside the broader treatment plan.
What makes this category convert: clinical depth that respects the reader’s intelligence, transparency about what the modality cannot do, integration with the facility’s broader clinical philosophy, and peer-reviewed citation discipline.
The reader on a modality page is often the most clinically literate prospect in the funnel, and the page either earns or loses credibility in the first 300 words.
The modality pages are also load-bearing for AI search citation. AI assistants answering questions about specific treatment modalities pull from facilities with depth on the modality, named clinical authors, and structured citation patterns. Facilities with strong modality pages get cited; facilities with thin modality pages do not.
What kills this category: marketing-voice descriptions of clinical modalities, claims that exceed the evidence base, and absent clinical authorship.
The patient is rarely the one researching at 11 PM. The patient is in a hotel room, a basement, or an ER bay.
The family member is the one with the laptop. Content written to the family member as the actual reader outperforms patient-voice content on every admit-attributed metric we track.
Preston Powell, CEO of Webserv
6. Comparison Content (PHP vs IOP, 30 vs 90 Day, MAT vs Abstinence)
Late-funnel evaluation traffic lives on comparison content. By the time a family member is searching “PHP vs IOP,” “30 day vs 90 day rehab,” “MAT vs abstinence-based recovery,” or “in-network vs out-of-network treatment,” they are inside two weeks of the inquiry call.
Comparison pages run 1,800 to 3,000 words. The structure that works is a clear framework (when each option fits, when each does not), an honest tradeoff discussion, and a specific recommendation about how to choose between the two.
The page should respect that the reader is making an informed decision and provide the information they need to make it.
What makes this category convert: honesty about the tradeoff (not “every patient is unique”), specificity about clinical and operational differences, and a clear next step (a clinical assessment call to determine which option fits).
The reader is in evaluation mode and the page that helps them resolve the comparison gets the inquiry.
What kills this category: vague “both have their place” framing, marketing-voice praise of every option equally, and refusal to make a specific recommendation about how to choose. The reader is not asking the facility to be neutral. They are asking the facility to help them think.
The comparison pages also rank well for the late-funnel commercial intent terms that produce the highest admit-attributed conversion. The publishing investment per piece is moderate; the conversion payoff is high.
7. Alumni Stories and Outcomes Content
Alumni stories and outcome content build the late-funnel trust that converts a prospect from “evaluating this facility” to “calling tomorrow.”
The category is harder to do at scale because each piece requires real alumni participation, signed consent (HIPAA and 42 CFR Part 2 compliance), and editorial craft to produce a story that reads as real rather than marketing copy.
What works: anonymized alumni stories with enough specific detail to feel real, paired with outcome data the facility can substantiate (90-day retention, 12-month sobriety rates, completion rates). The piece should read as a clinical narrative, not a testimonial.
What kills this category: glossy testimonial-style content that reads as marketing; outcome claims that exceed what the facility can defend; and stories that are too clean to be believable.
Family members in particular can detect inauthentic alumni stories in seconds and lose trust in the rest of the site as a result.
The compliance frame is real. 42 CFR Part 2 prohibits identifying SUD patient information without explicit written consent. The narrative should be anonymized to the point that the patient is not identifiable, even by family members.
The legal review pass on this category is materially longer than the other 8 types and should be planned for in the editorial timeline.
Done right, alumni and outcomes content carries late-funnel trust signal no other content type can produce. Done wrong, it undermines the rest of the site.
8. Geographic and Intent-Modifier Pages
“Alcohol rehab in [city],” “drug treatment in [state],” “PHP near me,” “rehab close to [location].” Geographic intent pages capture the local-search traffic that converts at a higher rate than national-intent traffic because the prospect has already made the geographic decision.
A geographic page runs 1,500 to 2,500 words and is anchored in real facility presence. The pages need substantive content about the local treatment landscape, what makes the facility distinct in the geography, the in-state insurance pattern, and operational specifics tied to the location.
Templated near-duplicate location pages across 50 cities trip the doorway pages framework and produce ranking drag rather than ranking lift.
What makes this category convert: real facility presence in the geography (not a virtual address), local operational depth (admissions team based in the geography, intake response times tied to the local timezone), and integration with the facility’s broader clinical positioning.
Local intent traffic is the highest-converting traffic on the site when the page can substantiate the local presence.
What kills this category: doorway pages built across 50 cities the facility has no actual presence in, templated copy that swaps city names but says nothing specific about the location, and absent local proof signals.
For the deeper tactical read on local-intent paid media that pairs with this category, see the exclude-zip strategy for out-of-network family targeting.
9. AI-Citation-Optimized FAQ and Question-Shaped Content
The 2026-specific category. AI Overviews, ChatGPT, Claude, and Perplexity now intercept a meaningful share of behavioral health queries, and the citations those systems issue go to content structured for extraction.
Question-shaped content that opens each section with a direct 40 to 60 word answer gets pulled into AI citations at a higher rate than narrative content that buries the answer in context.
The category includes FAQ pages, individual question-and-answer articles (“how long does detox last,” “what does a typical day at rehab look like,” “how does insurance verification work”), and structured FAQ blocks embedded inside the other 8 content types.
Each piece should be built with both human readability and AI extraction in mind.
What makes this category convert: direct first-paragraph answers, FAQPage schema deployment, Speakable schema for assistant-tier queries, and integration with the facility’s broader AI search infrastructure (AI Information page, schema stack, llms.txt, MCP server if applicable).
The Webserv Open Knowledge Format bundle is the relational layer that sits on top of the FAQ content for the facilities ready to push into agentic search.
The category does not convert directly in most cases. The conversion pattern is upstream: the AI citation drives the brand impression that drives the eventual visit to the facility’s site through a different query.
Facilities that earn AI citation share on the question-shaped content for their condition cluster see compounding lift across the other 8 content types.
What kills this category: FAQ blocks that bury the answer in 200 words of context, missing schema, and content that reads as keyword-stuffed rather than question-answering. The deeper read on how to get cited by ChatGPT, Perplexity, Claude, and Google AI Overviews covers the structural requirements.
What Doesn’t Drive Admits (And Most Facilities Publish Anyway)
The other half of the equation. Five content types we see in almost every facility’s blog library that produce no measurable admit-attributed conversion.
Editorial Team bylined volume blog posts. The 200-post backlog with no named author, no reviewer credit, no peer-reviewed citations. Produces sessions, produces no admits.
Generic “compassion and hope” pages. “We believe every person deserves…” Pages that say something the reader already assumes and provide no decision-useful information.
800-word condition explainers. Too short for YMYL ranking, too generic for patient or family-member trust, too brief for AI citation. The middle ground that does nothing.
Internal company news and “we attended this conference” posts. Nobody outside the facility cares. The conference attendance does not signal authority. Publish to LinkedIn if you must; do not publish to the blog.
Templated doorway location pages. “Alcohol rehab in [50 different cities]” with near-identical content.
This trips the doorway pages framework, drags ranking across the entire site, and was a 2018 tactic that does not work in 2026. The cost of doorway pages on behavioral health sites is real and measurable.
How to Sequence the Build Across the 9 Types
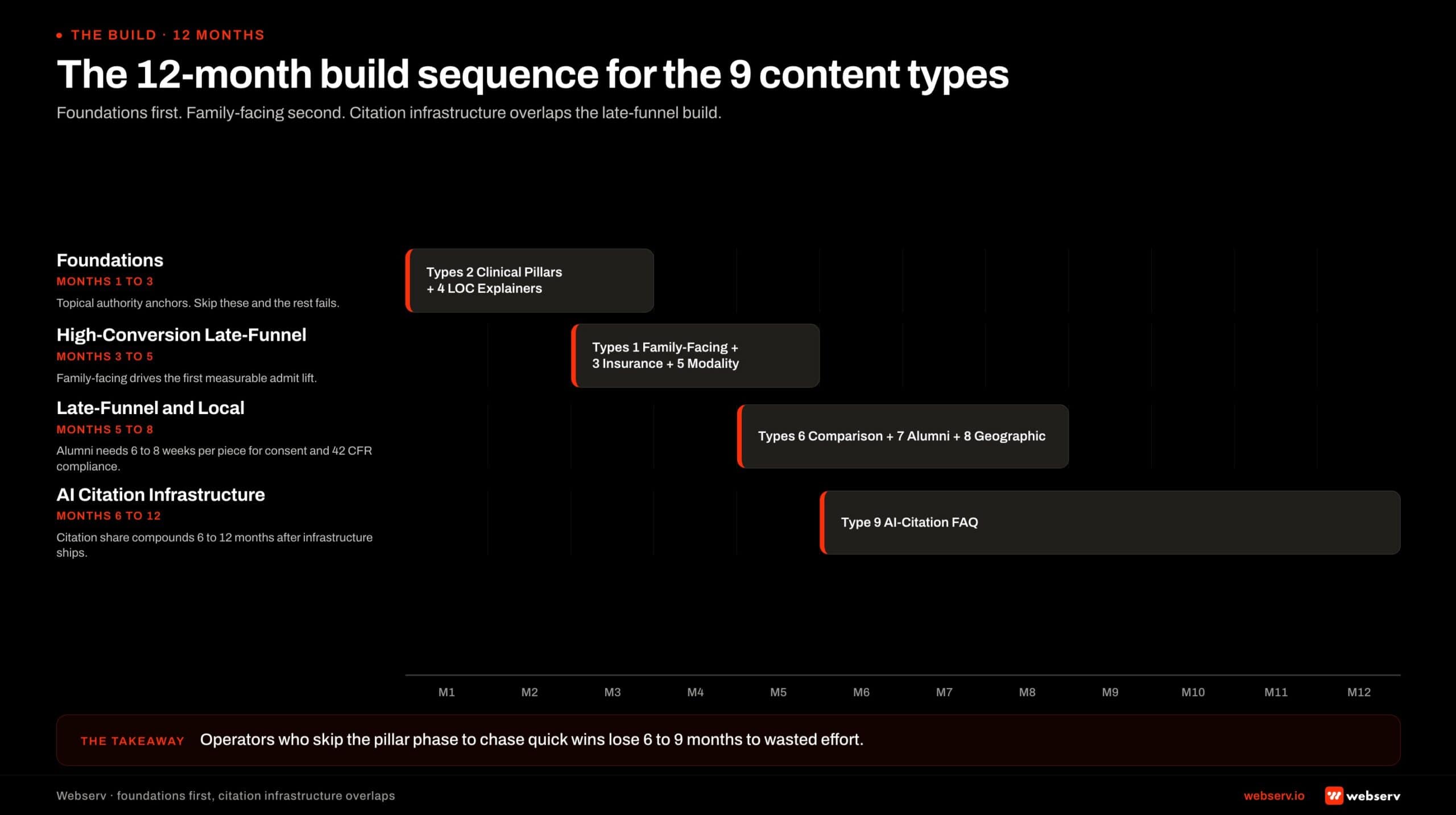
The 9 types do not build in parallel. They sequence across the first 12 months of program build, with each phase setting up the next.
Months 1-3: Foundations. Build out the 4 to 6 clinical condition pillars (Type 2) and the 5 to 7 level-of-care explainers (Type 4). These are the topical authority anchors that make every other category rank better. The author-reviewer infrastructure for named clinicians has to be in place before publishing starts.
Most operators try to skip this phase to chase quick wins on Type 1 family-facing content. The shortcut produces 6 to 9 months of wasted effort because the family-facing content needs the pillar topical authority underneath it to rank.
Months 3-5: High-conversion late-funnel. Family-facing content (Type 1), insurance verification (Type 3), and modality deep-dives (Type 5) layer in once the topical authority is established. The family-facing content drives the first measurable admit-attributed lift in most programs we build.
The publishing cadence at this phase is 4 to 6 pieces per month across the three types. Quality stays high; volume stays controlled.
Months 5-8: Late-funnel and local. Comparison content (Type 6), alumni stories (Type 7), and geographic pages (Type 8) build out the late-funnel evaluation traffic and the local-intent capture.
The alumni category needs the longest editorial timeline because of consent and 42 CFR Part 2 compliance. Plan 6 to 8 weeks per alumni story from consent through publish.
Months 6-12: AI citation infrastructure. AI-citation FAQ content (Type 9) builds out alongside the schema deepening, AI Information page, llms.txt, and OKF bundle work.
The AI citation share compounding shows up 6 to 12 months after the infrastructure is live, which is why this phase overlaps with the late-funnel build rather than waiting until after.
Throughout: Content gap closure on the existing library. Run the content gap analysis methodology quarterly. Cut the legacy posts that produce sessions but no admits, 301-redirect them to the relevant category hubs, and refresh the pages worth keeping under named clinical authorship.
By month 12, the program is producing compounding lift across all 9 types and the editorial calendar is running on a stable 4-to-6 pieces per month cadence. The system pays back across years rather than quarters.
Frequently Asked Questions
How long should each of the 9 content types be?
The word-count targets vary by type because the audience and conversion job vary. Family-facing first-touch content runs 1,800 to 2,800 words. Clinical condition pillars run 3,500 to 6,000 words. Insurance verification pages run 800 to 1,800 words. Level-of-care explainers run 1,500 to 2,500 words.
Modality deep-dives run 2,000 to 3,500 words. Comparison content runs 1,800 to 3,000 words. Alumni stories run 1,200 to 2,200 words. Geographic pages run 1,500 to 2,500 words. AI-citation FAQ content runs 800 to 1,800 words.
Word count is the byproduct of complete answers, not the goal. A 4,000-word condition pillar that pads to hit the count underperforms a 3,500-word pillar that answers the family-member and patient questions tightly. A 2,000-word insurance page that buries the answer in legal disclaimers underperforms an 800-word page that gives the reader a direct answer and routes them to verification.
The hierarchy is substance, structure, then length. Length follows the other two; never the other way around.
Do we need a clinician to author every one of the 9 types?
Four of the nine types require named clinical authorship and reviewer credit: condition pillars (Type 2), level-of-care explainers (Type 4), modality deep-dives (Type 5), and any alumni stories (Type 7) that touch clinical claims. These are the YMYL pages Google evaluates against the strictest E-E-A-T threshold and the pages AI search systems cite from most heavily.
The other five types can be authored by the marketing team with a clinical reviewer pass for accuracy. Family-facing content (Type 1) benefits from a clinical voice but does not need a clinician as primary author. Insurance verification (Type 3), comparison (Type 6), geographic (Type 8), and FAQ (Type 9) all work with marketing authorship and clinical review.
Treatment centers without clinician bandwidth for the four authorship-required types should reduce cadence rather than publish under “Editorial Team” bylines. Two strong condition pillars per quarter beat eight thin pillars with no clinical author.
How do we measure whether the 9 types are working?
Three metrics layered together. First, organic ranking position and traffic by type. The condition pillars and modality deep-dives should rank within 12 to 18 months of publish. The family-facing and insurance content should rank within 6 to 9 months because the keyword competition is lower.
Second, AI citation share across ChatGPT, Perplexity, Claude, Gemini, and Google AI Overviews on prompts that match the content types. Most operators use a monthly manual sampling protocol against 15 to 20 representative prompts per content type, plus a citation-tracking tool subscription.
Third, admit-attributed conversions traced from organic content to inquiry to admit, lagged 60 to 120 days for the behavioral health conversion cycle. Sessions and time-on-page are diagnostic; admits are the metric the content system optimizes against. Operators measuring on sessions alone optimize for the wrong outcome.
Should we cut our existing 200-post library before building the 9 types?
Yes, in most cases. A 200-post Editorial Team library is dragging on ranking and competing for crawl budget with the 9 types you actually need. The fix is not deletion in most cases but consolidation: identify the thin posts that produce zero admit-attributed conversion, 301-redirect them to the relevant category hub, and rebuild the cluster from there.
The cut should be substantive. We typically recommend removing 30 to 50 percent of the existing library on most treatment center sites we audit. That sounds aggressive until the operator runs the audit and sees how few of the posts are actually earning admit-attributed traffic.
The pages worth keeping are the ones that already rank for commercial-intent terms or that fit one of the 9 admit-driving categories. The pages worth cutting are the ones that produce sessions but no admits, the Editorial Team byline articles, and the templated location pages that trip the doorway pages framework.
Will AI search change which of the 9 types matter most?
Yes and no. The 9 categories as types of content remain stable, but the weight inside the funnel is shifting. Family-facing content (Type 1) and AI-citation FAQ content (Type 9) are gaining relative weight because both pair with the AI-search interception pattern.
The categories losing relative weight are the ones that depend on click-through from informational queries (some of Type 5 modality content and Type 4 LOC pages, which AI Overviews now answer directly).
These types still matter for AI citation eligibility and for the late-funnel visitor who clicks through after the AI answer, but the upstream traffic from informational queries is compressing.
The strategic frame is that all 9 types still belong in the program, but the family-facing and AI-citation categories deserve a slightly larger share of new investment than they did 18 months ago. The condition pillars and modality deep-dives remain the topical authority anchors that make the other types rank.
Build the Nine, Cut the Rest
The most common conversation we have with treatment center marketing directors is some version of “we publish a lot of content and none of it converts.”
The fix is rarely more content. The fix is the 9 admit-driving types built deliberately, under named clinical authorship, with the editorial discipline the YMYL frame requires.
The 247-post library converts worse than the 28-piece library built deliberately across these 9 types. The math is counterintuitive at first. It is the math after audit after audit. Volume without the system underneath produces traffic without admits.
We help treatment center operators audit their existing libraries against the 9 types, build the missing categories, cut the underperforming legacy posts, and sequence the editorial calendar against the 12-month build above. The work pairs with the broader SEO and AEO program that compounds across years.
Book an intro meeting to walk through your current content library, where the gaps against the 9 types likely sit, and what a 12-month build would produce for your facility.
For the broader picture of how content fits inside a full treatment center marketing program, see our ultimate guide to behavioral health marketing and our SEO timeline reality for rehab websites for the cycle the content investment plays out on.
Trevor Gage is the Director of Marketing at Webserv. Webserv works with behavioral health and addiction treatment centers on SEO, paid media, and full-funnel admissions strategy.





