
Topical authority has been the most misunderstood concept in healthcare SEO for the last three years. Most treatment center operators read about it through the lens of 2020 SEO content. Publish a lot of articles about a topic, link them together, watch the rankings come. That model is what most SEO programs for treatment centers are still running, even though Google retired it in stages between 2022 and 2026.
That model was already weakening when the Helpful Content System launched in August 2022. The August 2024 core update killed it for YMYL verticals. The March 2025 and December 2025 core updates closed the loopholes that had been left open.
What replaced page-count topical authority is harder to game and easier to fail at. Google now evaluates treatment center websites at the domain level for topical identity.
A site that covers ten unrelated topics shallowly is treated differently from one that covers two topics deeply. Even when individual pages are adequate, a fractured topical identity can suppress an entire domain’s perceived authority.
Industry tracking from 2025 shows that 73% of top-ranking YMYL pages now display detailed author credentials, up from 58% the year before.
This article is the operator-facing version of what we run with treatment center clients. The definition, the seven-step build playbook, the most expensive mistakes we audit and see repeated, what changes when AI search enters the picture, and what we believe about how this vertical actually wins.
Most treatment centers don’t have a content problem. They have an architecture problem dressed up as one. Publishing more pages won’t fix it. Publishing fewer of the right ones will.
Trevor Gage, Director of Earned & Owned Media, Webserv
Key Takeaways
- Topical authority is a sitewide credibility signal, not a per-page property. Google reads it from where your trust signals live, what proportion of your indexed pages serve buyer intent, and whether your architecture concentrates or dilutes earned authority.
- Page-count topical authority died in stages between August 2022 (Helpful Content System) and December 2025 (core update). The site that answers 50 questions about substance use disorder beats the site that answers one question each about 50 unrelated health topics — every time.
- 73% of top-ranking YMYL pages now show author credentials. Treatment centers with clinical authorship buried on the /about/ page (or absent entirely) are at a structural disadvantage. The credentials need to live on the level-of-care pages where families decide to call.
- The seven-step build playbook: audit indexed-page composition before publishing, concentrate rather than multiply, move trust signals to conversion pages, build around the singular specialization, schema where Google needs to see expertise, internal linking from authority to conversion, and measure by indexed-page composition and AI citation share.
- AI search raises the penalty for fractured topical identity, not lowers it. The center that exclusively treats one population gets cited; the generic center that mentions the population on page three of the nav gets summarized and not cited. Same architecture works for Google, ChatGPT, Perplexity, and Claude.
The piece below works in four moves: a working definition that aligns with how Google reads topical authority in 2026, two recent audits that show how the signal breaks at different layers, the seven-step playbook we run with treatment center clients, and the platform-specific picture once AI search enters the equation.
What topical authority actually is
Topical authority is a sitewide credibility signal, not a per-page property. Google reads it from three things: where your trust signals live, what proportion of your indexed pages serve buyer intent, and whether your architecture concentrates or dilutes the authority you have already earned.
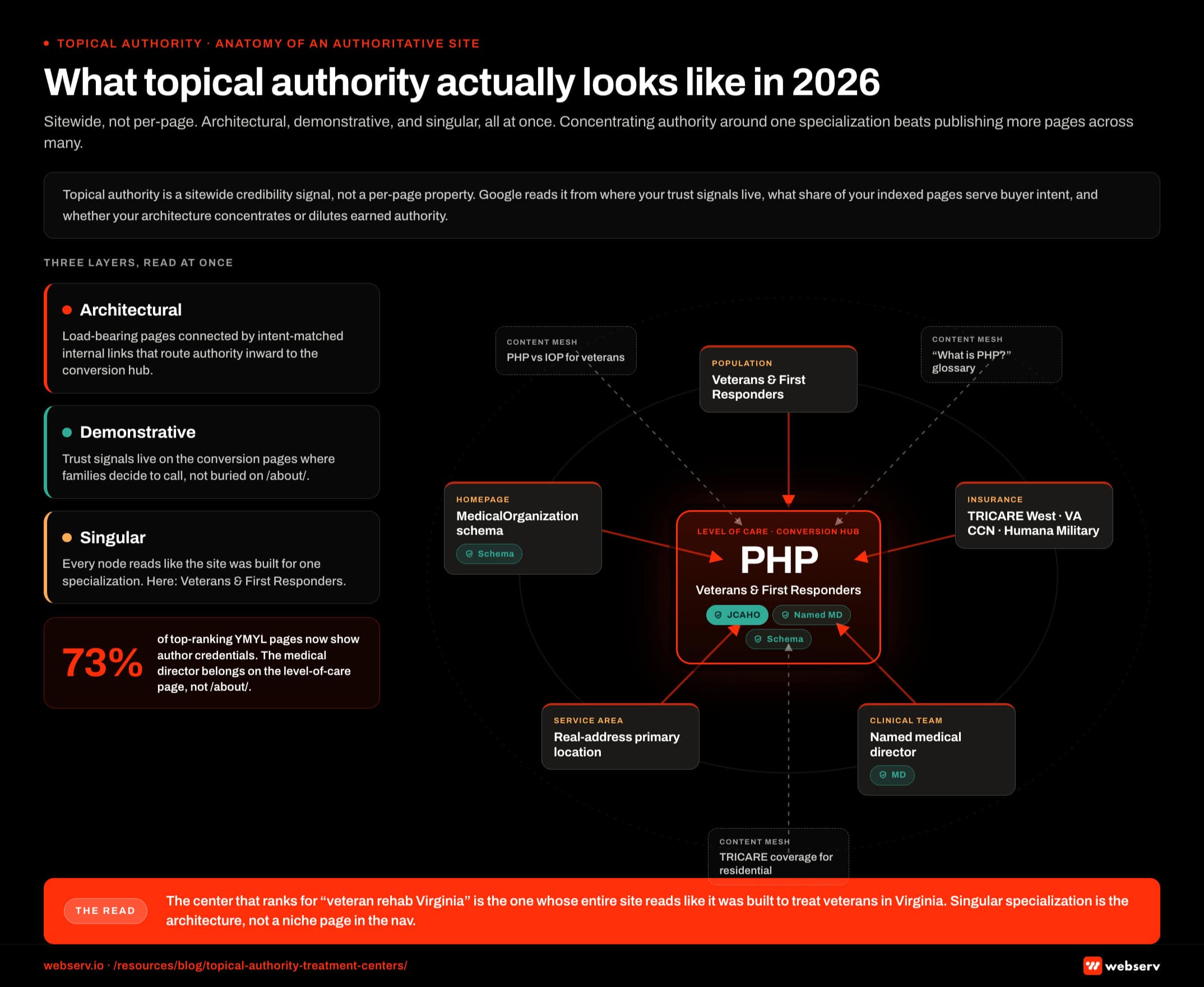 Infographic titled ‘What topical authority actually looks like for a treatment center in 2026’ showing the sitewide hub-and-spoke architecture that signals topical authority to Google. At the center is a large red node labeled PHP (Partial Hospitalization Program for veterans and first responders), representing the load-bearing level-of-care conversion page. A first ring of five supporting service-mesh nodes surrounds the hub: the population page for Veterans and First Responders, the insurance page covering TRICARE West, VA CCN, and Humana Military, the clinical team page, a homepage carrying MedicalOrganization schema, and a real-address service-area page. A second outer ring shows the supporting blog cluster of glossaries and Micros that link inward to the hub, including pages like What is PHP, PHP versus IOP for veterans, and TRICARE coverage for residential treatment. Trust-signal badges overlay the hub and first-ring nodes, including the Joint Commission seal, named medical director credentials with PhD and clinical license, accreditation badges, payer logos, and a MedicalWebPage schema indicator. Arrows flow inward from authority-bearing content toward the conversion hub, with anchor text matching the exact-match query the hub is built to rank for. A left-side legend identifies three layers: Architectural is the structure, Demonstrative is the trust-signal layer, and Singular is the specialization label running across every node. Top strip callout: topical authority is a sitewide credibility signal, not a per-page property, and Google reads it from where trust signals live, what proportion of indexed pages serve buyer intent, and whether the architecture concentrates or dilutes earned authority. Right margin callout: 73 percent of top-ranking YMYL pages now show author credentials, and treatment centers with the medical director buried on the about page are at a structural disadvantage because the credentials need to live on the level-of-care pages where families decide to call. Bottom strip: the center that ranks for veteran rehab Virginia is the one whose entire site reads like it was built to treat veterans in Virginia, because singular specialization is the architecture, not a niche page in the navigation.
Infographic titled ‘What topical authority actually looks like for a treatment center in 2026’ showing the sitewide hub-and-spoke architecture that signals topical authority to Google. At the center is a large red node labeled PHP (Partial Hospitalization Program for veterans and first responders), representing the load-bearing level-of-care conversion page. A first ring of five supporting service-mesh nodes surrounds the hub: the population page for Veterans and First Responders, the insurance page covering TRICARE West, VA CCN, and Humana Military, the clinical team page, a homepage carrying MedicalOrganization schema, and a real-address service-area page. A second outer ring shows the supporting blog cluster of glossaries and Micros that link inward to the hub, including pages like What is PHP, PHP versus IOP for veterans, and TRICARE coverage for residential treatment. Trust-signal badges overlay the hub and first-ring nodes, including the Joint Commission seal, named medical director credentials with PhD and clinical license, accreditation badges, payer logos, and a MedicalWebPage schema indicator. Arrows flow inward from authority-bearing content toward the conversion hub, with anchor text matching the exact-match query the hub is built to rank for. A left-side legend identifies three layers: Architectural is the structure, Demonstrative is the trust-signal layer, and Singular is the specialization label running across every node. Top strip callout: topical authority is a sitewide credibility signal, not a per-page property, and Google reads it from where trust signals live, what proportion of indexed pages serve buyer intent, and whether the architecture concentrates or dilutes earned authority. Right margin callout: 73 percent of top-ranking YMYL pages now show author credentials, and treatment centers with the medical director buried on the about page are at a structural disadvantage because the credentials need to live on the level-of-care pages where families decide to call. Bottom strip: the center that ranks for veteran rehab Virginia is the one whose entire site reads like it was built to treat veterans in Virginia, because singular specialization is the architecture, not a niche page in the navigation.Most SEO content writes about topical authority as if it were a page-count problem. Publish 200 articles on a topic and you are an authority on it. That model died with the August 2024 core update and the Helpful Content System refinements that followed. The March 2025 update added a layer of EEAT scrutiny that previously only applied to medical and financial pages.
The December 2025 update extended EEAT requirements beyond traditional YMYL topics and increased the weight of technical performance signals.
What replaced page-count authority is harder to game. Google now reads topical authority through the composition of your indexed page set. One treatment center site that answers 50 questions about substance use disorder will outperform one that answers one question each about 50 unrelated health topics.
For a treatment center website specifically, topical authority means three things at the same time:
Architectural. Your service pages, level-of-care pages, and population-specific pages are the load-bearing pages of the site. They must be indexed, technically clean, and connected to each other by internal links that flow from authority-bearing content. The same technical foundation we walk through in the technical SEO guide for treatment center websites is the prerequisite for any topical authority work compounding.
If those pages are not indexed, no amount of domain authority will help. The hub-and-spoke content model, where a central topic hub links to detailed subtopic spokes that link back, is the architecture Google currently rewards.
Demonstrative. Your clinical credentials, accreditations, payer contracts, named medical leadership, and population specialization need to live on the pages where families decide whether to call. Not on /about/. Not in the footer. On the conversion pages, above the fold.
73% of top-ranking YMYL pages now show author credentials. Treatment centers without visible clinical authorship are at a structural disadvantage in 2026.
Singular. The center that ranks for “veteran rehab Virginia” is the one whose entire site reads like it was built to treat veterans in Virginia.
The center that tries to rank for veterans, adolescents, executives, dual diagnosis, eating disorders, and trauma at the same time will rank for none of them. Google’s pattern recognition since the March 2025 update increasingly penalizes fractured topical identity even at strong domains.
What Google actually rewards in 2026
A working definition. Topical authority is what Google reads when it asks: when a user searches for help inside this category, is this site the source the answer should come from? The helpful, reliable, people-first content guidance is the doc that codifies how Google answers that question.
The signals it weighs:
Coverage of the buyer’s question. Not coverage of the keyword. The query “alcohol rehab in Texas” is a buyer asking which residential program treats their family member. The page that answers it specifically and authoritatively, with the right credentials surfaced and the right clinical proof, outranks the page that ranks well for the keyword but answers a different question. The Helpful Content System penalty has shifted from punishing thin content to punishing content that ranks for queries it does not actually serve.
Distribution of authority signals. Schema, authorship, medical review, and accreditation badges need to live on the pages that Google needs to evaluate.
A medical reviewer credential block on a blog post about benzodiazepine identification does not help Google understand whether your residential program is qualified. It needs to be on the residential program page. The schema implementation matters as much as the content of the page.
Internal architecture. Topical authority compounds through internal links from authority-bearing content to conversion-intent pages. If your highest-authority page is a blog post and the blog post does not link to your level-of-care pages, the authority is stuck. The hub-and-spoke model exists because Google’s ranking systems read it as evidence of intentional topical depth.
Indexed page composition. Pages Google chooses to index are the pages Google has decided are worth indexing. If a site has 700 pages eligible for indexing and Google indexes 35, the 665 that were dropped are sending a signal to the index that decides which 35 stay. Templated location pages, thin blog posts, and orphaned author pages dilute the indexed set in ways that pull commercial pages down with them.
The December 2025 update made this more punitive. Technical excellence stopped being optional. Sites with high indexed-page counts but poor crawl efficiency lost rankings on commercial terms even when the commercial pages themselves were strong. The patterns I covered in the technical SEO fix list are the prerequisite cleanup before topical authority work compounds.
Citation in AI answers. The newer signal, and the one most operators underestimate. Recent industry analysis from 5W’s 2026 AI Platform Citation Source Index found that the top 15 domains capture 68% of all consolidated AI citation share. That concentration is more extreme than anything Google PageRank ever produced.
The sites cited in AI answers are the ones whose distinctive expertise is recognizable to an LLM doing retrieval. Generic content gets summarized and not cited. Specific clinical leadership, named protocols, and population specialization get cited.
What this looks like in practice
Two recent audits at our agency illustrate how topical authority breaks at different layers.
The first was a California adolescent behavioral health center with Joint Commission accreditation, links from Forbes, Healthline, Smithsonian, Women’s Health, and Wikipedia, a real medical reviewer with PhD and LMFT credentials, and a clean parent-child URL structure.
Every individual service page looked textbook. Schema was in place. Author bylines were real.
The site went from 722 indexed pages in August 2025 to 35 in May 2026. A 95% loss in nine months. Every residential, PHP, and IOP page sat at zero organic traffic. Four URLs carried 83% of the traffic the site still had.
The pattern that broke it is one we see across treatment center websites running an outdated playbook. The good schema and the credentialed authorship lived in the blog. The crawl budget got eaten by 52 templated city pages, 40+ of them in cities the operator did not have an office in. By the time the Helpful Content System took a position on the pattern, the level-of-care pages had been deindexed.
The second center serves veterans and first responders exclusively. It is one of the few accredited residential programs built specifically for that population. Domain Rating 57. Over 900 referring domains including va.gov, the American Legion, Forbes, Police Magazine, and Military Families Magazine. Referring domains grew 117% in 24 months.
Organic traffic in the same window: flat. The homepage and one personal blog post carry 70% of all traffic. The mission page named after the population the program exclusively treats gets 11 visits a month.
These are not poorly run treatment centers. Both have clinical leadership that deserves to rank. Both have the authority signals Google rewards. Neither has built topical authority the way it actually works in 2026. The first failed at architecture. The second failed at signaling. Both patterns are common enough that the playbook below addresses them directly.
How treatment centers actually build topical authority
This is the playbook we run for treatment center clients. Seven steps, in order. Skipping ahead is the fastest way to repeat the patterns above.
 Infographic titled ‘The 7-step sequence to build topical authority for a treatment center’ showing the ordered build playbook used with treatment center clients. Step 1 Audit indexed-page composition before publishing anything new: pull 24 months of Ahrefs indexed pages history and the Google Search Console indexed page set, compare, and identify which pages got dropped and what they have in common, including templated locations, thin posts, or title and H1 mismatches; most operators get this wrong by starting the engagement publishing more content; output is a documented list of dropped pages and their shared patterns. Step 2 Concentrate, do not multiply: target fewer than 100 indexed pages including the homepage, five to seven level-of-care pages, two to four population pages, one service-area page per real market, a clinical team page, a medical reviewer hub, and a small set of high-quality blog posts; most operators publish a city page for every market within driving distance; output is a stable or shrinking indexed page count with commercial pages held in. Step 3 Move trust signals to the conversion pages: re-host the Joint Commission seal, named medical director, accreditations, and payer contracts on level-of-care and population pages above the fold; most operators leave the Joint Commission seal only on the about page and payer logos only on the admissions insurance page; output is the same trust modules visible on every conversion page with both conversion rate and organic signal rewiring. Step 4 Build around the singular specialization: homepage hero, level-of-care pages, blog topics, and author bios all read in the voice of the population the program serves; most operators use generic rehab framing with the niche relegated to one navigation item; output is a site that reads end-to-end like the specialization is the only thing the program does. Step 5 Schema where Google needs to see expertise: MedicalOrganization on the homepage, MedicalWebPage on every level-of-care page, Physician on clinical leadership, and Service on level-of-care pages; most operators have rich schema auto-generated on blog posts and no schema on commercial pages; output is custom schema implemented on the load-bearing pages and validated in Search Console. Step 6 Internal linking flows from authority to conversion: homepage and link-magnet blog posts link to level-of-care and population pages with the exact-match query as anchor text; most operators use Learn More and Click here anchors and leave authority stuck on the Forbes-linked blog post; output is authority routed from authority-bearing content to conversion pages with rankings moving on commercial terms. Step 7 Measure by indexed-page composition and AI citation share: track indexed page count trended, indexed page composition by commercial versus content marketing, cost per acquired indexed page, and AI citation share across ChatGPT, Google AI Overviews, Perplexity, and Claude; most operators track Domain Rating or Ahrefs Health Score as the topical authority metric; output is weekly visibility on the four metrics that actually predict topical authority growth. Left margin callout: steps 1 through 3 are foundation steps that should not be skipped because the Helpful Content System reacts to patterns and once a pattern on the site is unhelpful the lens widens and level-of-care pages get caught in the wave. Right margin callout near step 7: page count is not the metric, Domain Rating is not the metric, Ahrefs Health Score is not the metric, and the four metrics that actually predict topical authority growth are indexed page count trended, indexed page composition, cost per acquired indexed page, and AI citation share. Bottom strip: for most operators the right architecture is fewer than 100 indexed pages, with less content and more depth, fewer pages and more weight per page, because the instinct to publish a city page for every market within driving distance is the instinct that gets adolescent treatment centers deindexed.
Infographic titled ‘The 7-step sequence to build topical authority for a treatment center’ showing the ordered build playbook used with treatment center clients. Step 1 Audit indexed-page composition before publishing anything new: pull 24 months of Ahrefs indexed pages history and the Google Search Console indexed page set, compare, and identify which pages got dropped and what they have in common, including templated locations, thin posts, or title and H1 mismatches; most operators get this wrong by starting the engagement publishing more content; output is a documented list of dropped pages and their shared patterns. Step 2 Concentrate, do not multiply: target fewer than 100 indexed pages including the homepage, five to seven level-of-care pages, two to four population pages, one service-area page per real market, a clinical team page, a medical reviewer hub, and a small set of high-quality blog posts; most operators publish a city page for every market within driving distance; output is a stable or shrinking indexed page count with commercial pages held in. Step 3 Move trust signals to the conversion pages: re-host the Joint Commission seal, named medical director, accreditations, and payer contracts on level-of-care and population pages above the fold; most operators leave the Joint Commission seal only on the about page and payer logos only on the admissions insurance page; output is the same trust modules visible on every conversion page with both conversion rate and organic signal rewiring. Step 4 Build around the singular specialization: homepage hero, level-of-care pages, blog topics, and author bios all read in the voice of the population the program serves; most operators use generic rehab framing with the niche relegated to one navigation item; output is a site that reads end-to-end like the specialization is the only thing the program does. Step 5 Schema where Google needs to see expertise: MedicalOrganization on the homepage, MedicalWebPage on every level-of-care page, Physician on clinical leadership, and Service on level-of-care pages; most operators have rich schema auto-generated on blog posts and no schema on commercial pages; output is custom schema implemented on the load-bearing pages and validated in Search Console. Step 6 Internal linking flows from authority to conversion: homepage and link-magnet blog posts link to level-of-care and population pages with the exact-match query as anchor text; most operators use Learn More and Click here anchors and leave authority stuck on the Forbes-linked blog post; output is authority routed from authority-bearing content to conversion pages with rankings moving on commercial terms. Step 7 Measure by indexed-page composition and AI citation share: track indexed page count trended, indexed page composition by commercial versus content marketing, cost per acquired indexed page, and AI citation share across ChatGPT, Google AI Overviews, Perplexity, and Claude; most operators track Domain Rating or Ahrefs Health Score as the topical authority metric; output is weekly visibility on the four metrics that actually predict topical authority growth. Left margin callout: steps 1 through 3 are foundation steps that should not be skipped because the Helpful Content System reacts to patterns and once a pattern on the site is unhelpful the lens widens and level-of-care pages get caught in the wave. Right margin callout near step 7: page count is not the metric, Domain Rating is not the metric, Ahrefs Health Score is not the metric, and the four metrics that actually predict topical authority growth are indexed page count trended, indexed page composition, cost per acquired indexed page, and AI citation share. Bottom strip: for most operators the right architecture is fewer than 100 indexed pages, with less content and more depth, fewer pages and more weight per page, because the instinct to publish a city page for every market within driving distance is the instinct that gets adolescent treatment centers deindexed.Step 1. Audit indexed-page composition before publishing anything new
Most agencies start a topical authority engagement by publishing more content. That is the wrong first move. The first move is figuring out what Google is currently indexing and why. The agencies that lead with this audit step are the ones worth shortlisting.
Pull the Ahrefs indexed pages history for the last 24 months. Pull the Google Search Console indexed page set. Compare. If the indexed set has shrunk, the question is which pages got dropped and what they had in common. Templated locations? Thin blog posts? Pages with title and H1 mismatches? Orphaned employee pages?
The Helpful Content System reacts to patterns. Once it has decided a pattern on your site is unhelpful, it widens the lens. The level-of-care pages can get caught in a deindex wave triggered by templated city pages those level-of-care pages had nothing to do with. The cleanup has to happen first.
Step 2. Concentrate, do not multiply
Treatment center websites do not need more pages. They need their existing pages to earn the right to be indexed.
For most operators, the right architecture is fewer than 100 indexed pages. The homepage. Five to seven level-of-care pages. Two to four population-specific pages. One service-area page per market where the facility actually accepts patients. A clinical team page. A medical reviewer credentials hub. A small set of high-quality blog posts that earn citations and link back to the commercial pages they support.
That is it. The instinct to publish a city page for every market within driving distance is the instinct that gets adolescent treatment centers deindexed. It connects directly to the patterns in our local SEO playbook — real-address Primary Location Pages, no exceptions.
Step 3. Move trust signals to the conversion pages
The trust signals exist on most treatment center sites. They are just in the wrong place.
The Joint Commission seal lives on /about/. It belongs above the fold on every level-of-care page. The named medical director with the PhD credentials lives on the team page. The bio block belongs on the page where families are deciding whether to admit.
The TRICARE West, Humana Military, and VA CCN credentials live on /admissions/insurance/. They belong on the veteran population page that families read first when they search for that population.
Same trust modules. Same content. Different location. The change rewires the page’s signal to Google and rewires the page’s conversion rate for the family reading it.
Step 4. Build around the singular specialization
The center that exclusively treats veterans and first responders should have a site that reads like that is the only thing it does. The center built for adolescent behavioral health should have a site that reads like adolescents are the only patients it sees.
That means the homepage hero is about the specialization, not about treatment in general. The level-of-care pages read in the voice of the population the program serves. The blog topics cluster around the questions that population asks. The author bios surface the team’s specific experience with that population.
Most treatment center sites read like generic rehab sites with a niche page somewhere in the navigation. The right read is the inverse. Generic rehab is the secondary frame. The specialization is the headline. The keyword mapping for this work is what we cover in the keyword strategy guide for rehab and mental health.
Step 5. Schema where Google needs to see expertise
Schema markup is the structured signal Google uses to validate what your pages claim. For a treatment center, the schema that matters is:
MedicalOrganization on the homepage with the full name, license numbers, accreditations, and parent organization properties filled in. MedicalWebPage on every level-of-care page with the specialty, condition treated, and primary audience properties filled in.
Physician schema on the medical director and clinical leadership pages with the credentials, license, and specialties populated. Service schema on the level-of-care pages with the description, area served, and provider properties filled in.
Most treatment center sites have schema. Most have it in the wrong places. The schema is rich on blog posts (because the blog plugin generates it automatically) and absent on the commercial pages where Google needs the validation. The fix is custom schema implementation on the load-bearing pages.
Step 6. Internal linking flows from authority to conversion
If your highest-authority page is your homepage, the homepage needs to link directly to your level-of-care pages with descriptive anchor text that matches the search intent of those pages. Not “Learn More.” Not “Click here.” The exact match query the page is built to rank for.
If your second-highest-authority page is a blog post that picked up the Forbes link, that blog post needs to link to the level-of-care pages and the population pages that the blog post is contextually adjacent to. The authority that came in through the Forbes link is currently stuck on the blog post. Internal links route it to the pages that need it.
If your authority-bearing pages do not link to your commercial pages with intent-matched anchor text, the topical authority you have earned does not reach the pages that have to convert.
Step 7. Measure topical authority by indexed-page composition and AI citation share
Page count is not the metric. Domain Rating is not the metric. Ahrefs Health Score is not the metric.
The metrics that predict whether topical authority is being built or eroded are:
Indexed page count, trended. Stable or growing is healthy. Falling is a signal that pages are getting dropped from the index and the rest of the site is at risk.
Indexed page composition. What percentage of your indexed set is commercial intent (level-of-care, service area, population pages) versus content marketing? If commercial pages are getting dropped while blog posts stay indexed, the topical authority is decaying from the load-bearing side.
Cost per acquired indexed page. If you publish 20 articles a month and the indexed set stays flat, the publishing program is feeding a content treadmill rather than building topical authority.
AI search citation share. OtterlyAI, Profound, AI Rank Lab, or Ahrefs Brand Radar pull citation share for your brand across ChatGPT, Google AI Overviews, Perplexity, and Claude. The 5W research shows citation share can shift within weeks rather than months.
ChatGPT’s Reddit citation share fell from roughly 60% to 10% over six weeks in late 2025 after a single Google parameter change. Treatment centers need to be tracking citation share weekly, not quarterly.
How SoCal Sunrise generated 85 admissions and 2,297% ROI from SEO in 6 months
A ground-up SEO rebuild using the Pathfinder Parents Methodology turned an invisible online presence into a top-ranking admissions engine.
Read the case study →85 admits and 3,152 leads attributed to organic
The most expensive mistakes treatment centers make
Five patterns we audit and see repeated:
1. The location scale strategy. Publishing a templated city page for every market within driving distance, including markets where the operator does not have a physical office. The Helpful Content System treats this pattern as a signal that the site is not built for the user. Once it widens the lens, the level-of-care pages get caught in the deindex wave. This pattern was the proximate cause of the 95% indexed-page loss in our first audit.
2. EEAT only in the blog. Author bylines, medical reviewer credentials, and citation depth living exclusively on blog content. The schema and the authorship signal Google needs are absent from the commercial pages that have to rank. The center looks like a content publisher, not a treatment provider. With 73% of top-ranking YMYL pages now showing author credentials, the gap on a treatment center page without visible authorship is now structural.
3. Trust signals buried on /about/. Joint Commission seal, accreditations, payer contracts, and named clinical leadership living on the about page. Families do not start at /about/. They land on the level-of-care page or the population page. If the trust signals are not there, the page is interchangeable with forty other treatment centers.
4. Generic positioning on a niche brand. A program built for one population trying to rank for everything. The site reads as generic rehab with a niche page somewhere in the navigation. The Forbes link, the va.gov link, the American Legion link came in because the program is the authority on that niche. The site fails to claim it. The March 2025 update made this kind of fractured topical identity directly suppressive of domain-level rankings.
5. Confusing domain authority with topical authority. Domain Rating measures earned link equity. Topical authority measures whether your site has been built to convert that link equity into rankings on commercial terms. A treatment center can have all the backlinks in the world and not rank for the queries families search when they need help. DR 57 with flat organic traffic is one of the most common diagnoses in our audit deck.
What changes when AI search enters the picture
The two audits in the section above were both written for a SERP world. The next set of audits will be written for a SERP plus AI Overviews plus ChatGPT plus Perplexity plus Claude plus Gemini world. The full playbook for the AI side lives in our guide to getting cited in Google AI Overviews and ChatGPT.
 Infographic titled ‘What changes when AI search enters the topical authority picture’ comparing how topical authority signals get re-weighted when retrieval shifts from a Google SERP to a large language model doing retrieval. The left column is labeled Google SERP era and the right column is labeled AI search era covering AI Overviews, ChatGPT, Perplexity, Claude, and Gemini. Five signal rows compare the two retrieval modes. Position 1 ranking: in the SERP era it was the gating criterion for clicks; in the AI era it is no longer the gating criterion for citation because pages at positions six through ten with strong EEAT get cited 2.3 times more than first-ranked pages with weak authority; direction is down. Singular specialization: in the SERP era it helps rank and fractured topical identity is penalized under the March 2025 update; in the AI era the LLM picks the source distinctively right for the query, generic content gets summarized, and distinctive content gets cited and quoted; direction is up. Named clinical leadership: in the SERP era it is an EEAT signal on YMYL pages with 73 percent of top-ranking YMYL pages now showing author credentials; in the AI era the penalty for absence is higher because LLM retrieval favors named expertise and ChatGPT cites Wikipedia-style authority in 26 to 48 percent of top citations; direction is up. Trust signals on conversion pages: in the SERP era they help rank the conversion page; in the AI era the same load-bearing-page architecture works for Google, ChatGPT, Perplexity, and Claude; direction is up. Indexed-page composition: in the SERP era the Helpful Content System reads composition at the domain level; in the AI era the same domain-level read applies and the top 15 domains capture 68 percent of all consolidated AI citation share according to the 5W 2026 AI Platform Citation Source Index; direction is up. A platform-specific citation pattern strip beneath the comparison shows ChatGPT favoring Wikipedia-style authority and named clinical expertise with Wikipedia in 26 to 48 percent of top citations, Perplexity prioritizing Reddit discussions and community-validated sources with Reddit in 46.7 percent of top citations, Google AI Overviews balancing professional and social content with a mixed pattern where no single source dominates, and across all platforms the concentration being more extreme than PageRank ever produced with the top 15 domains capturing 68 percent of consolidated AI citation share. Top strip callout: topical authority shifts inside an LLM, Google’s ranking system reads a long list of signals and weighs them probabilistically, an LLM doing retrieval reads a shorter list and looks for the source that is distinctively the right one, generic content gets summarized and not cited, and distinctive expertise gets cited and quoted. Center divider callout near the position 1 row: pages at ranking positions six through ten with strong EEAT signals get cited 2.3 times more frequently in AI answers than first-ranked pages with weak authority, and position is no longer the gating criterion because authority depth is. Bottom strip: one body of work, five distribution channels, Google rankings, AI Overviews citations, ChatGPT recommendations, Perplexity sources, and Claude sources, because the center that builds topical authority correctly now has a multi-platform compounding asset.
Infographic titled ‘What changes when AI search enters the topical authority picture’ comparing how topical authority signals get re-weighted when retrieval shifts from a Google SERP to a large language model doing retrieval. The left column is labeled Google SERP era and the right column is labeled AI search era covering AI Overviews, ChatGPT, Perplexity, Claude, and Gemini. Five signal rows compare the two retrieval modes. Position 1 ranking: in the SERP era it was the gating criterion for clicks; in the AI era it is no longer the gating criterion for citation because pages at positions six through ten with strong EEAT get cited 2.3 times more than first-ranked pages with weak authority; direction is down. Singular specialization: in the SERP era it helps rank and fractured topical identity is penalized under the March 2025 update; in the AI era the LLM picks the source distinctively right for the query, generic content gets summarized, and distinctive content gets cited and quoted; direction is up. Named clinical leadership: in the SERP era it is an EEAT signal on YMYL pages with 73 percent of top-ranking YMYL pages now showing author credentials; in the AI era the penalty for absence is higher because LLM retrieval favors named expertise and ChatGPT cites Wikipedia-style authority in 26 to 48 percent of top citations; direction is up. Trust signals on conversion pages: in the SERP era they help rank the conversion page; in the AI era the same load-bearing-page architecture works for Google, ChatGPT, Perplexity, and Claude; direction is up. Indexed-page composition: in the SERP era the Helpful Content System reads composition at the domain level; in the AI era the same domain-level read applies and the top 15 domains capture 68 percent of all consolidated AI citation share according to the 5W 2026 AI Platform Citation Source Index; direction is up. A platform-specific citation pattern strip beneath the comparison shows ChatGPT favoring Wikipedia-style authority and named clinical expertise with Wikipedia in 26 to 48 percent of top citations, Perplexity prioritizing Reddit discussions and community-validated sources with Reddit in 46.7 percent of top citations, Google AI Overviews balancing professional and social content with a mixed pattern where no single source dominates, and across all platforms the concentration being more extreme than PageRank ever produced with the top 15 domains capturing 68 percent of consolidated AI citation share. Top strip callout: topical authority shifts inside an LLM, Google’s ranking system reads a long list of signals and weighs them probabilistically, an LLM doing retrieval reads a shorter list and looks for the source that is distinctively the right one, generic content gets summarized and not cited, and distinctive expertise gets cited and quoted. Center divider callout near the position 1 row: pages at ranking positions six through ten with strong EEAT signals get cited 2.3 times more frequently in AI answers than first-ranked pages with weak authority, and position is no longer the gating criterion because authority depth is. Bottom strip: one body of work, five distribution channels, Google rankings, AI Overviews citations, ChatGPT recommendations, Perplexity sources, and Claude sources, because the center that builds topical authority correctly now has a multi-platform compounding asset.Topical authority shifts inside an LLM. Google’s ranking system reads a long list of signals and weighs them probabilistically. An LLM doing retrieval reads a shorter list and looks for the source that is distinctively the right one. Generic content gets summarized and not cited. Distinctive expertise gets cited and quoted.
Recent citation analysis shows that pages with strong EEAT signals at ranking positions #6 to #10 get cited 2.3 times more frequently in AI answers than #1-ranked pages with weak authority signals. Position is no longer the gating criterion. Authority depth is.
For a treatment center, this means the topical authority strategy that works for AI Overviews and ChatGPT is the same strategy that works for the Helpful Content era of Google. Singular specialization. Trust signals on the load-bearing pages. Clinical leadership that is real and surfaced. Architecture that concentrates authority instead of dispersing it.
The penalty for the location scale strategy and the blog-only EEAT pattern is higher in the AI era, not lower. An LLM citing one source on “veteran rehab Virginia” will cite the program that exclusively treats that population, not the generic treatment center that mentions veterans on page three of the navigation.
The platform-specific picture matters too. ChatGPT favors Wikipedia-style authority and cites Wikipedia in 26% to 48% of its top citations. Perplexity prioritizes Reddit discussions in 46.7% of its top citations. Google AI Overviews balances professional and social content.
Treatment centers cannot ignore Reddit if they want to be cited by Perplexity, and they cannot ignore named clinical expertise if they want to be cited by ChatGPT. Both need attention. Both are part of topical authority in 2026.
The opportunity is also higher. The center that builds topical authority correctly now has a multi-platform compounding asset. Google rankings. AI Overviews citations. ChatGPT recommendations. Perplexity sources. One body of work, five distribution channels.
Frequently asked questions about topical authority for treatment centers
How long does it take to build topical authority?
Most treatment centers see the first meaningful topical authority signal at 4 to 6 months when the publishing discipline is correct (named clinical authorship, evidence-backed content, full topical clusters with internal linking). Measurable ranking and citation lift typically follows at 6 to 9 months. The 12-month mark is where compounding starts, and it does not stop compounding once it does.
Topical authority is not a content volume game. A center publishing four well-built cluster pieces per month consistently outperforms a center publishing twelve thin articles per month. The variable that moves authority is depth and structure, not raw post count. The center publishing four pieces also burns less editorial capacity, which means the program is sustainable past month six instead of collapsing at month three.
Programs that switch SEO partners every 6 to 9 months lose the authority compounding entirely. Each transition resets the publishing rhythm and breaks the cluster mesh. The 12 to 24 month horizon is what produces real authority. Operators evaluating partners should weight tenure and consistency higher than novelty.
Should we publish more frequently or focus on depth per topic?
Depth per topic produces more topical authority lift than publishing frequency, especially under the 2025-2026 Helpful Content updates. A treatment center that publishes one comprehensive 3,500-word UG with named clinical authorship and full topical coverage outperforms a center publishing eight 500-word thin posts on adjacent topics. The first builds authority. The second produces noise.
The right rhythm for most treatment centers is one comprehensive pillar piece per quarter plus two to four supporting Micros per month inside the same cluster. The pillar earns the topical authority signal. The Micros build the internal linking mesh that distributes it. Together they form a cluster that ranks the whole topic, not just the pillar URL.
Treatment centers publishing thin content at high frequency get penalized faster in 2026 than they did in 2024. The Helpful Content System now actively demotes shallow YMYL content rather than just refusing to reward it. The cost of publishing for volume’s sake is higher than the cost of publishing less.
Can a new treatment center build topical authority faster than an established one?
New treatment centers can build topical authority on a similar 6 to 12 month horizon as established ones when the foundational work is done correctly. The advantage they have is no legacy content baggage. The disadvantage is no existing domain authority. Net, the timeline is comparable, but the path is cleaner because there is less to undo.
Established centers with thin or stale content carry a structural disadvantage. The Helpful Content System reads outdated or low-quality pages as a site-wide signal, dragging the whole domain down even when the new content is strong. The first 90 days of an authority program for an established center usually involves removing or rewriting historical content before the new content can compound.
The window matters either way. The category is concentrating fast in 2026. Treatment centers that start building topical authority now have a meaningful window before the rest of the category catches up. Twelve months from now, the same starting position will cost more in time and budget to build from.
Is topical authority the same thing as E-E-A-T?
They are related but distinct. E-E-A-T (Experience, Expertise, Authoritativeness, Trustworthiness) is the page-level quality framework Google uses to evaluate individual pieces of content. Topical authority is the site-level framework Google uses to evaluate whether a domain is the right answer for a topic broadly. E-E-A-T feeds topical authority, but topical authority requires more than just strong E-E-A-T on individual pages.
A treatment center can have strong E-E-A-T on each page (named clinicians, evidence citations, accurate medical content) and still not have topical authority if the cluster mesh is missing, the publishing cadence is irregular, or the internal linking is broken. Topical authority requires the architecture, not just the page quality.
For YMYL content, both matter. E-E-A-T is the gate that lets a page rank at all. Topical authority is what lets the page rank against the publishers with more raw authority signal. Treatment centers that invest in only one of the two underperform centers that invest in both as a system.
How do we measure topical authority growth?
Track four metrics over time: organic ranking share across your priority cluster keywords, AI citation share across ChatGPT and Google AI Overviews on those same keywords, organic traffic to the cluster pages, and admissions attributed to organic search from that cluster. The first two are leading indicators. The last two are trailing.
The metric most operators track is generic organic traffic, which is not the same as topical authority. A site can grow traffic from a few high-ranking pages without growing the underlying authority of the topic. The cluster-level view shows whether the program is actually building authority across the topic or just farming a handful of high-volume queries.
Authority signals also compound non-linearly. A cluster at 12 months produces meaningfully more organic admits per month than the same cluster at 6 months at the same content volume, because the internal mesh has densified and the AI citation share has built. Operators evaluating authority programs should weight the 12-month and 24-month numbers, not the 90-day report.
What the centers that win actually do
Most treatment center websites read like every other treatment center website. The clinical credentials are real. The location footprint is real. The story is missing.
Topical authority in 2026 is built by the centers that show their work. Real clinicians on the page. Specific populations treated. Distinctive protocols described in the team’s own voice. Indexed pages that carry their weight. Architecture that concentrates the authority the operator has earned.
The centers we audit who are losing rankings are usually doing more of what worked in 2020 and less of what works now. The ones gaining ground are doing the opposite. Less content, more depth. Fewer pages, more weight per page. Less keyword chasing, more singular positioning.
The center that wins the topical authority game in this vertical is the center that is willing to be the answer to one question really well. Not the answer to twenty questions in a way nobody trusts.
If you want to talk through whether your site is building topical authority or eroding it, book a discovery call. We will run the indexed-page composition audit and tell you what we see. No assumptions about what we find.
The perspective in this article comes from 9 years working exclusively inside behavioral health.
We are a team built by people in recovery who understand that behind every admission is someone asking for help. If that resonates, get to know us.
Trevor Gage is the Director of Earned & Owned Media at Webserv. Webserv works with behavioral health and addiction treatment centers on SEO, paid media, and full-funnel admissions strategy.






