A treatment center we audited last spring had 47 pages live on the site with titles like “Drug Rehab in Pasadena,” “Drug Rehab in Glendale,” “Drug Rehab in Burbank,” and 44 more. The pages were 320 to 380 words each.
Forty-six of them shared the exact same template, with the city name swapped in seven places and a single line about “serving the [City] community” added at the bottom.
The facility itself had one physical address, in Orange County, with no offices, staff, or operations in any of those 47 cities.
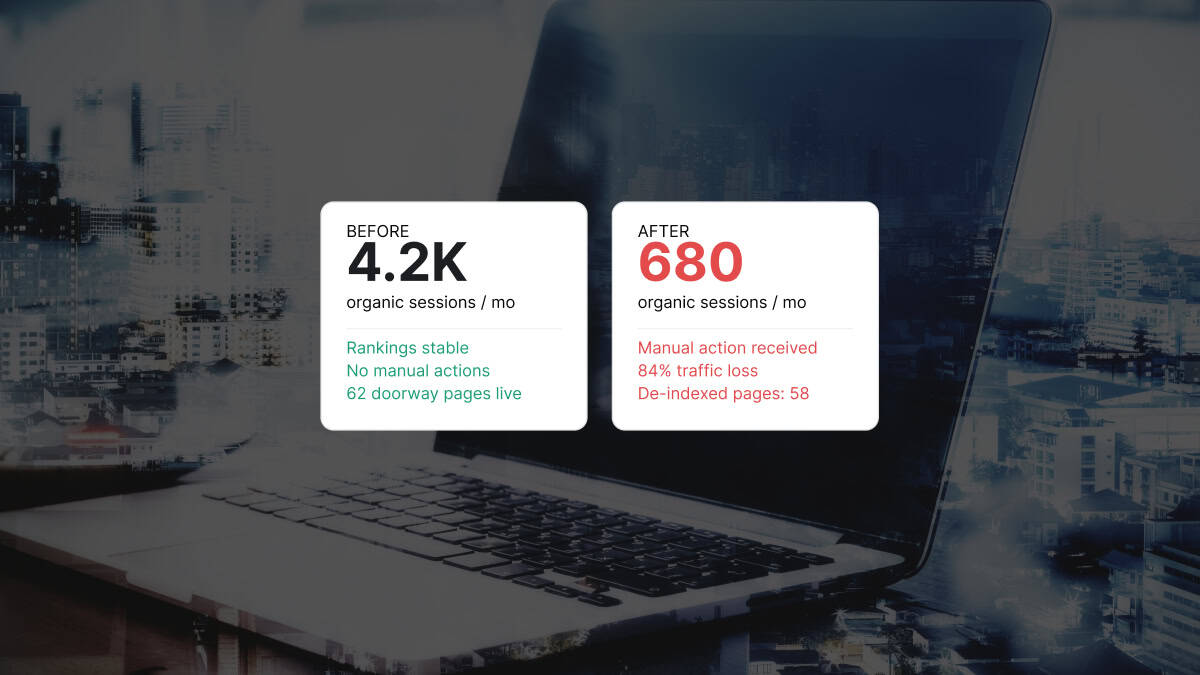
That site received a manual action three weeks after our audit started. The Search Console notification cited “Pure spam: Doorway abuse.” Organic admissions inquiries dropped 81 percent in the following 30 days. The fix took four months and a partial rebuild.
The agency that built the 47 pages had pitched them as a “local SEO program.”
If you are a treatment center operator and any part of that story sounds familiar, the next 2,000 words are worth reading carefully. Doorway pages have been a Google policy violation since 2015, but the enforcement reality in 2026 has shifted.
The March 2026 core update wiped out city-page volume across multiple behavioral health sites we monitor. The April 2026 spam-report rule change means a competitor or former employee can now trigger a manual action by reporting your doorway pages directly, with the submission text forwarded verbatim to your site.
The cost-of-getting-caught math has changed, and most operators have not updated their site to match. This is the same pattern Webserv’s SEO program flags first when we audit a new behavioral health site.
Below is what doorway pages actually are, how they show up in this category, how to tell if you have them, and how to fix them without losing the rankings you do have.
Key Takeaways
- Doorway pages are sets of pages built to rank for similar queries (usually city + service combos) that funnel users to the same destination, with little or no unique value per page. Google’s spam policy has prohibited them since 2015.
- In behavioral health, doorway patterns most commonly appear as templated location pages, insurance pages, and modality pages where the only difference between pages is the variable in the title.
- The 2026 enforcement environment is harsher than the previous cycle: the March 2026 core update suppressed doorway-heavy sites, and the April 2026 spam-report rule means competitors can now trigger manual actions on your site directly.
- The self-audit is short. Compare any 5 of your city pages side by side. If the unique content per page is under 30 percent, you have doorway pages.
- The fix is not “delete and pray.” Real consolidation, real differentiation, and proper redirects are required to recover the equity already in the cluster.
What Google actually means by “doorway pages”
The official definition lives in Google’s spam policies documentation under the heading “Doorway abuse.” The policy describes the pattern across four signals.
The signals are: multiple sites or pages with slight variations targeting the same query intent, and multiple domains funneling users to one destination.
Also flagged: pages generated to funnel users into the actual usable section of a site, and near-identical pages that sit closer to search results than to a clearly defined site hierarchy.
The intent test is what matters. Google is not banning location pages. It is banning location pages built primarily to rank, not to serve the user once they land.
The line the policy draws is between content that exists to answer a query and content that exists to capture a query.
A real location page describes a real facility at a real address with real staff serving real patients. It carries unique local information that could not have been generated by template. A real local SEO playbook starts here, not at programmatic page generation.
The same logic applies to the rest of the commercial layer. A real service page for PHP, IOP, or residential treatment is built around the specific clinical reality of that program, not around a keyword combination.
A doorway page describes a generic offering with a city name swapped in. The page exists because the operator wanted to rank for “[service] in [city],” not because the operator has anything specific to say about that city.
Most operators do not set out to build doorway pages. They hire an agency. The agency proposes a “local SEO” program. The program produces 30 to 60 city pages on a template. The operator approves them because they look like SEO work.
Google’s quality systems flag them because the pattern they form is doorway abuse.
How doorway patterns show up on behavioral health sites
MOST DAMAGING PATTERN
Templated city pages for cities you do not operate in. “Drug Rehab in Anaheim,” “Drug Rehab in Long Beach,” 40 more — same facility copy, city name swapped in, no local address, no local staff, no payer specificity. Google reads this exactly the way it looks: a doorway pattern. The one that gets penalties applied at the section level, not the page level.
Five patterns account for most of the doorway issues we see in this category.
Templated city pages with no local content. A facility in Costa Mesa publishes “Drug Rehab in Anaheim,” “Drug Rehab in Long Beach,” “Drug Rehab in Riverside,” and 40 more cities the facility does not physically operate in.
Each page describes the facility’s program with the city name dropped in. There is no local address, no local staff, no local payer information, no local context.
Insurance + service combinations on a template. Pages like “Aetna Drug Rehab in [City],” “BCBS Detox in [City],” and “Cigna Outpatient in [City]” multiplied across a payer matrix.
The pages exist to capture insurance + service + geo queries. The content is the same boilerplate insurance explanation with the variables swapped in.
Level-of-care + city combinations. “PHP in [City],” “IOP in [City],” “Residential in [City]” multiplied across 30 cities. Same template, same content, only the level of care and city change.
Modality + city combinations. “TMS Therapy in [City],” “Ketamine-Assisted Therapy in [City],” “EMDR in [City]” multiplied across cities. Often these are even worse because the underlying modality content is itself a thin description with no clinical depth.
Microsite networks. A single operator running 4 to 8 separate domains, each targeting a different city or region, all funneling calls to the same intake line.
This is the heaviest pattern Google’s policy specifically names. It is also the easiest pattern to detect from outside, and the most likely to trigger a competitor spam report.
The pattern shows up most often on sites built by legacy SEO agencies in this category that productized programmatic page generation a decade ago and never updated the playbook.
If your site does any of the first four at scale, the doorway risk is significant. If your operation runs the fifth, the risk is severe and the timeline for action should be measured in weeks, not quarters.
How to tell if you have doorway pages
The self-audit is short. It takes about an hour and does not require any tooling beyond a browser and a spreadsheet.
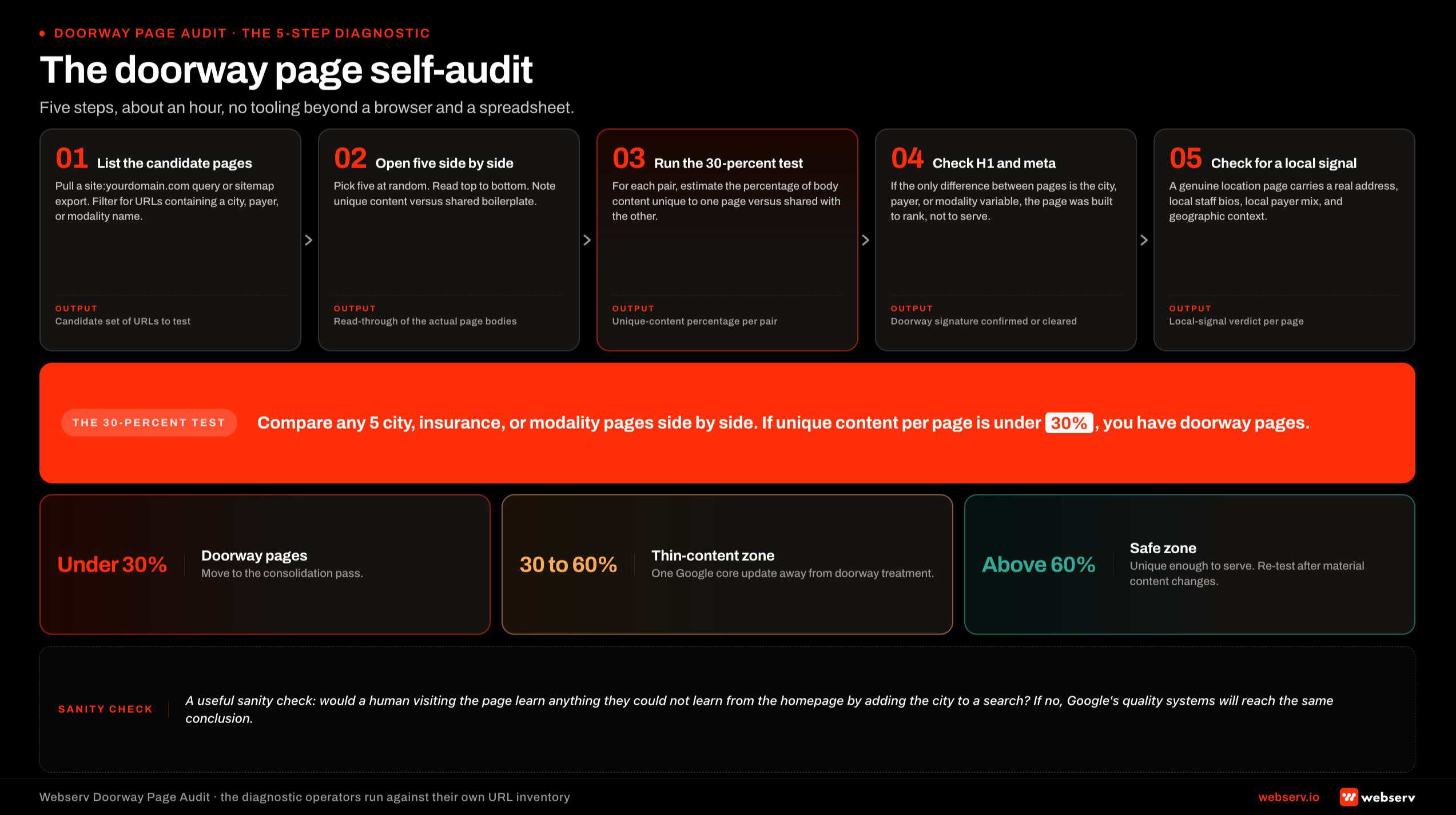 Infographic titled ‘The doorway page self-audit’ showing the five-step diagnostic that a behavioral health operator runs against their own site to determine whether they have doorway pages. Step 1 list the candidate pages by pulling a site colon yourdomain query and filtering for URLs with city, payer, or modality variables. Step 2 open five side by side and note unique content versus shared boilerplate. Step 3 run the thirty-percent test estimating the percentage of body content unique per page versus shared with the others. Step 4 check the H1, meta title, and meta description for whether the only difference is the city, payer, or modality variable. Step 5 check for a real local signal including local address, local staff bios, local payer mix, and local geographic context. Diagnostic result band: under thirty percent is doorway, thirty to sixty percent is thin-content zone, above sixty percent is the safe zone.
Infographic titled ‘The doorway page self-audit’ showing the five-step diagnostic that a behavioral health operator runs against their own site to determine whether they have doorway pages. Step 1 list the candidate pages by pulling a site colon yourdomain query and filtering for URLs with city, payer, or modality variables. Step 2 open five side by side and note unique content versus shared boilerplate. Step 3 run the thirty-percent test estimating the percentage of body content unique per page versus shared with the others. Step 4 check the H1, meta title, and meta description for whether the only difference is the city, payer, or modality variable. Step 5 check for a real local signal including local address, local staff bios, local payer mix, and local geographic context. Diagnostic result band: under thirty percent is doorway, thirty to sixty percent is thin-content zone, above sixty percent is the safe zone.Step 1: List every location, insurance, and modality page. Pull a site:yourdomain.com query in Google or export the URL list from your sitemap. Filter for any URL containing a city name, payer name, or modality name. This is your candidate set.
Step 2: Open five of them side by side. Pick five at random from the candidate set. Read them top to bottom. Note what content is unique to each page versus what is shared boilerplate.
Step 3: Run the 30-percent test. For each pair of pages, estimate the percentage of body content that is unique to one page versus shared with the other. If the unique content is under 30 percent across the pairs, you have doorway pages.
If most pairs land between 30 and 60 percent, you have a thin-content problem that is one Google update away from being treated as doorway abuse. Above 60 percent is the safe zone.
Step 4: Check the H1, meta title, and meta description. If the only difference between pages is the city, the payer, or the modality variable, the page was built to rank, not to serve. That is the doorway signature.
Step 5: Check for a real local signal. A genuine location page carries a local address, local staff bios, local payer mix details, local trust signals, and local geographic context like neighborhoods or counties served.
If none of those appear, the page is not a location page in any meaningful sense. It is a doorway with a city name on the door.
A useful sanity check: ask whether a human visiting the page would learn anything they could not learn from the homepage by adding the city to a search. If the answer is no, Google’s quality systems are likely to reach the same conclusion.
What doorway pages actually cost you
The cost is rarely a single number. It is layered across four categories, and the total is often two to three years of compounding decline before the operator realizes what is happening.
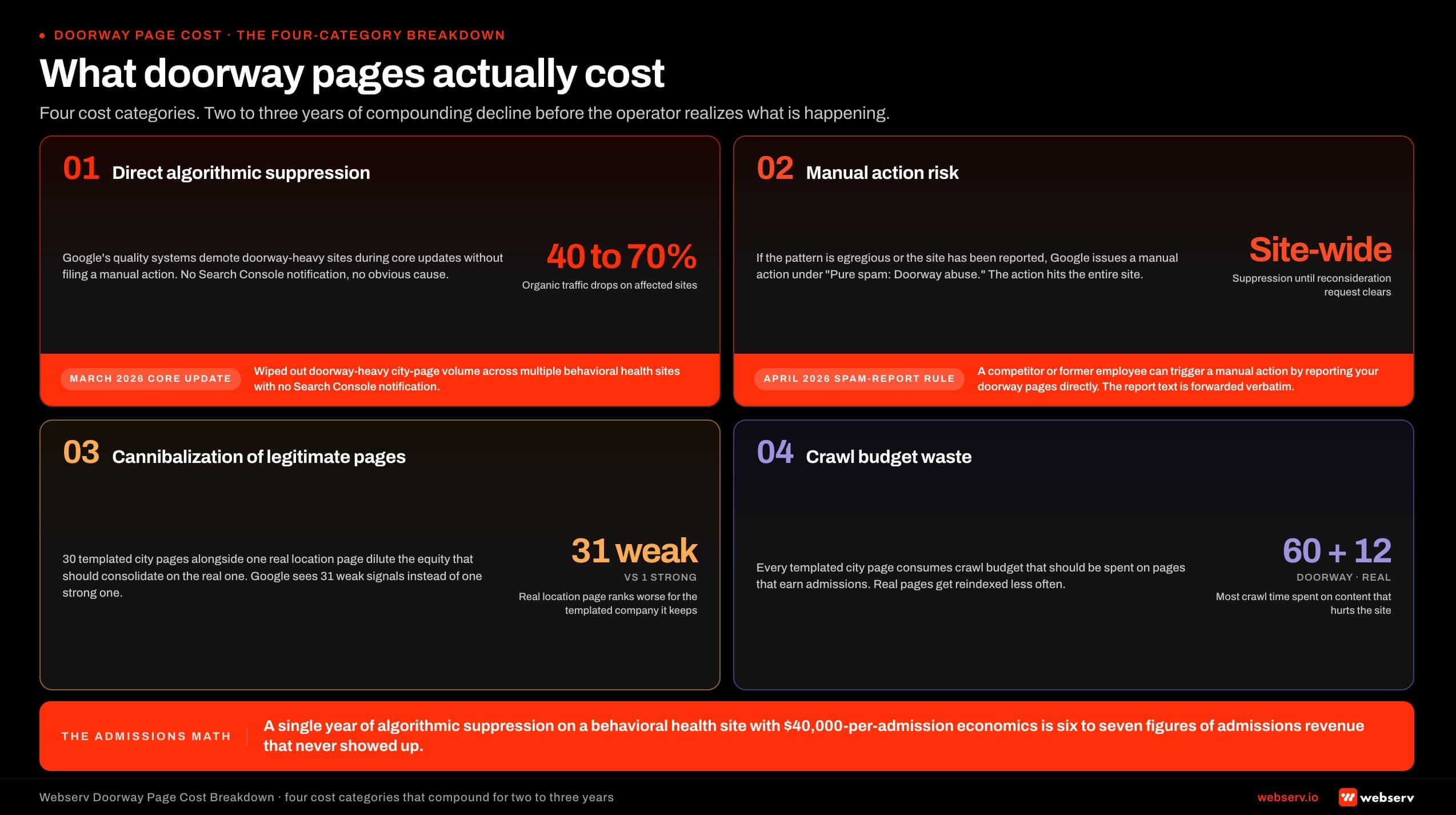 Infographic titled ‘What doorway pages actually cost’ showing the four-category cost breakdown that compounds across two to three years of decline on behavioral health sites with doorway pages, arranged as four impact cards in a two-over-two grid. Card 1 direct algorithmic suppression caused by Google’s quality systems demoting doorway-heavy sites during core updates without a manual action; March 2026 core update wiped doorway-heavy city-page volume across multiple behavioral health sites; quantified impact is forty to seventy percent organic traffic drops. Card 2 manual action risk under Pure spam Doorway abuse; April 2026 spam-report rule lets a competitor or former employee trigger a manual action by reporting your doorway pages directly. Card 3 cannibalization of legitimate pages dilutes the equity that should consolidate on the real one. Card 4 crawl budget waste consumes time on templated pages instead of pages that earn admissions. Admissions math: a year of suppression at forty thousand dollars per admission is six to seven figures in missed revenue.
Infographic titled ‘What doorway pages actually cost’ showing the four-category cost breakdown that compounds across two to three years of decline on behavioral health sites with doorway pages, arranged as four impact cards in a two-over-two grid. Card 1 direct algorithmic suppression caused by Google’s quality systems demoting doorway-heavy sites during core updates without a manual action; March 2026 core update wiped doorway-heavy city-page volume across multiple behavioral health sites; quantified impact is forty to seventy percent organic traffic drops. Card 2 manual action risk under Pure spam Doorway abuse; April 2026 spam-report rule lets a competitor or former employee trigger a manual action by reporting your doorway pages directly. Card 3 cannibalization of legitimate pages dilutes the equity that should consolidate on the real one. Card 4 crawl budget waste consumes time on templated pages instead of pages that earn admissions. Admissions math: a year of suppression at forty thousand dollars per admission is six to seven figures in missed revenue.Direct algorithmic suppression. Google’s quality systems demote doorway-heavy sites during core updates without filing a manual action. The site does not get a Search Console notification. It just stops ranking.
The March 2026 core update wiped out doorway-heavy city-page volume across multiple behavioral health sites we monitor. Operators on those sites saw 40 to 70 percent organic traffic drops with no notification and no obvious cause.
Manual action risk. If the pattern is egregious or if the site has been reported, Google can issue a manual action under “Pure spam: Doorway abuse.” The action affects the entire site, not just the offending pages.
Per Google’s Search Console Help documentation on manual actions, the recovery process requires removing or fundamentally rewriting the doorway content before submitting a reconsideration request.
Cannibalization of legitimate pages. If you have one real, well-built location page for the city where your facility actually operates, and 30 templated city pages alongside it, the templated pages dilute the equity that should consolidate on the real one.
Google sees 31 weak signals for the city instead of one strong one. The legitimate page often ranks worse because of the templated company it keeps.
This is the same dilution problem topical authority frameworks try to solve at the cluster level.
Crawl budget waste. Every templated city page consumes crawl budget that should be spent on pages that earn admissions. On a site with 60 doorway pages and 12 real ones, Google’s crawler is spending most of its time on content that hurts the site.
The real pages get reindexed less often, updates take longer to register, and the site’s overall responsiveness in search degrades. The problem compounds on sites with mobile-first indexing issues already in play, because the doorway pages also waste mobile crawl cycles.
The compounding cost across these four is the part most operators underestimate. A single year of algorithmic suppression on a behavioral health site with $40,000 per admission economics is six to seven figures of admissions revenue that never showed up.
How SoCal Sunrise generated 85 admissions and 2,297% ROI from SEO in 6 months
A ground-up SEO rebuild using the Pathfinder Parents Methodology turned an invisible online presence into a top-ranking admissions engine.
Read the case study →85 admits and 3,152 leads attributed to organic
How to fix doorway pages without losing the rankings you do have
The wrong move is to delete every templated page and watch what happens. The doorway pages have probably accumulated some links, some traffic, and some rankings. Deleting them without a plan throws away the equity along with the problem.
This is also why a full site rebuild rarely helps for sites with doorway problems: the consolidation pass below preserves more equity than a rebuild would.
The right approach is a four-step consolidation pass.
Step 1: Identify the one or two pages per cluster worth saving. For the city-page cluster, the page worth saving is usually the city where your facility actually operates. For the insurance-page cluster, it is the page for the payer that drives the most admissions.
For the modality cluster, it is the modality your clinical team is most known for. Everything else gets consolidated into those saved pages.
Step 2: Rebuild the saved pages with real local, payer, or clinical content.
A real city page includes the physical address, photos of the actual facility, staff bios for the people working at that location, payer details specific to that market, and geographic context (counties served, surrounding cities, public transit notes, nearby hospitals or clinical partners).
The page should be 1,200 to 2,000 words of content that could not have been generated by template.
Step 3: 301 redirect the doorway pages to the rebuilt versions. Every templated city page gets a 301 to the rebuilt page for that cluster. This preserves the link equity from any incoming references and signals to Google that the consolidation is intentional.
Do not let the doorway pages go to 404 or to the homepage. The redirect target should be the closest topical match in the consolidated set.
Step 4: Update internal links and sitemap. The internal links pointing to the deleted doorway pages need to be updated to the rebuilt destinations. The XML sitemap needs to be regenerated without the deleted URLs.
The technical SEO pass that catches the orphan internal links should run on the same day as the redirects to keep the site clean.
This sequence usually recovers 60 to 80 percent of the pre-decline organic visibility within 90 to 120 days.
The remaining 20 to 40 percent depends on the site’s broader technical SEO foundation and on whether the operator can resist the agency pitch to rebuild the doorway pattern under a different name a year later.
The line between programmatic location pages and doorway pages
This is the question most operators ask once they see the pattern: where is the line between a programmatic page strategy that works and one that gets penalized?
The line is differentiation, not volume. Google does not have a policy against scale. It has a policy against pages that exist to rank without serving, which is why a real keyword strategy starts from intent and clinical reality rather than from a city-by-city query expansion.
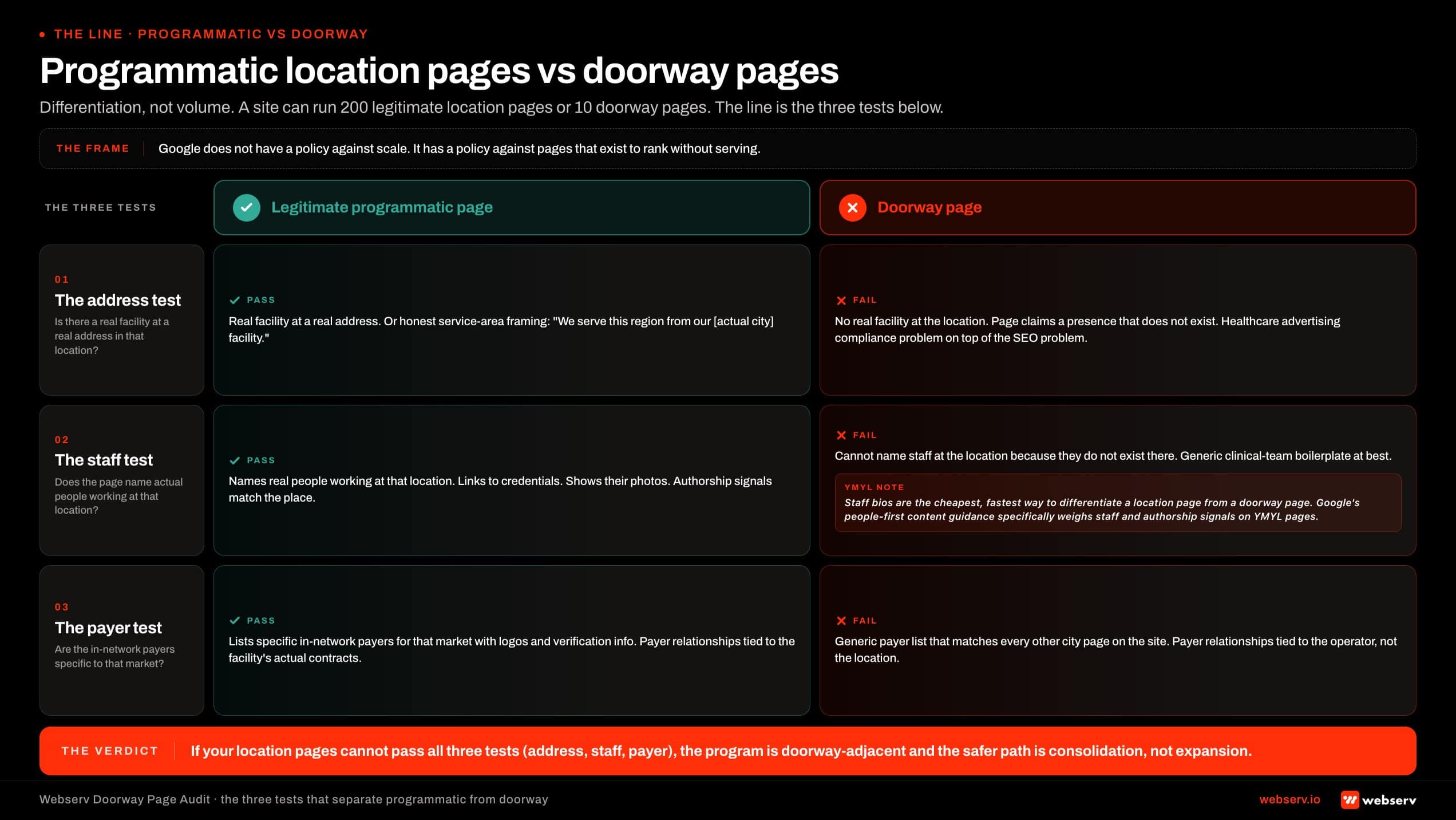 Infographic titled ‘The line between programmatic location pages and doorway pages’ showing the three-test comparison that separates legitimate programmatic location pages from doorway pages, arranged as a two-column side-by-side with three rows. Row 1 the address test: legitimate has a real facility at a real address or honest service-area framing; doorway claims a presence that does not exist. Row 2 the staff test: legitimate names actual people working at that location with credentials and photos; doorway carries generic clinical-team boilerplate because the staff do not exist there. Row 3 the payer test: legitimate lists specific in-network payers for that market with payer logos; doorway carries a generic payer list that matches every other city page. Verdict frame: if location pages cannot pass all three tests, the program is doorway-adjacent and the safer path is consolidation.
Infographic titled ‘The line between programmatic location pages and doorway pages’ showing the three-test comparison that separates legitimate programmatic location pages from doorway pages, arranged as a two-column side-by-side with three rows. Row 1 the address test: legitimate has a real facility at a real address or honest service-area framing; doorway claims a presence that does not exist. Row 2 the staff test: legitimate names actual people working at that location with credentials and photos; doorway carries generic clinical-team boilerplate because the staff do not exist there. Row 3 the payer test: legitimate lists specific in-network payers for that market with payer logos; doorway carries a generic payer list that matches every other city page. Verdict frame: if location pages cannot pass all three tests, the program is doorway-adjacent and the safer path is consolidation.A site can run 200 location pages legitimately if each page carries enough unique, local, useful content that a human visiting it would learn something specific to that location. The same site can run 10 location pages illegitimately if each one is a city-name swap on a template.
The clearest line is the address test. If you have a real facility at the location, you can build a real page for it.
If you do not have a real facility at the location, the page has to either be honest about that (a “service-area” page that says clearly “we serve this region from our [actual city] facility”) or it should not exist.
Pretending to have a facility where none exists is also a healthcare advertising compliance problem, not just an SEO one.
A second test is the staff test. A real location page can name actual people who work at that location, link to their credentials, and show their photos. A templated city page cannot do that because the staff do not exist there.
Staff bios are the cheapest, fastest way to differentiate a location page from a doorway page, and per Google’s people-first content guidance, quality systems specifically weigh staff and authorship signals on YMYL pages.
The third test is the payer test. A real location page can list specific in-network payers for that market, with payer logos and verification information. A templated city page cannot because the payer relationships are tied to the facility’s actual contracts, not to the city.
If your location pages cannot pass all three tests (address, staff, payer), the program is doorway-adjacent and the safer path is consolidation, not expansion. The same principle is why we recommend service-pages-first ordering on every audit: one strong commercial page beats many thin ones, every time.
“If your agency is selling you 50 city pages and cannot point to which staff member at which physical facility is doing the work in each city, you are not buying SEO. You are buying a Google manual action with a six-month delay.”
Preston Powell, Chief Executive Officer, Webserv
The pull quote is uncomfortable because the math is uncomfortable. The cost of getting caught in 2026 is higher than the cost of having fewer pages, and most operators have not done the comparison.
The broader behavioral health marketing program only compounds when the foundation is clean. Doorway clusters are the most common reason it does not, and the cleanup also resets the entity profile that AI search models use to decide which treatment center to cite for a query.
Frequently Asked Questions
How does Google decide whether a location page is a doorway page?
Google’s quality systems look at the unique value per page relative to the cluster. If 30 pages on a site share 70 percent of their content and the unique 30 percent is just the city name and a generic “serving the [city] community” sentence, the cluster reads as doorway abuse.
The signals include text overlap across pages, similarity of meta titles and H1s, lack of unique local citations, and the presence of programmatic patterns in URL structure.
The 2026 quality systems use both algorithmic detection (which suppresses doorway-heavy sites during core updates without notification) and human review (which feeds into manual actions). The April 2026 spam-report rule change adds a third path: a competitor or former employee can file a spam report through Search Console, and the report can trigger a manual action that includes the original report text in the notification to the site owner. The practical implication for operators is that doorway abuse is no longer a slow-burn risk. It is an active enforcement target with three independent detection paths.
Can a behavioral health site rank for “[service] in [city]” queries without doorway pages?
Yes, and the sites that do it well are the ones who treat each location page as a real local page, not as a template fill. The formula is one strong page per real facility, plus a local SEO playbook for Google Business Profile, citations, reviews, and local link building.
That combination wins more “[service] in [city]” queries than 50 doorway pages do, and it does not carry policy risk. For markets where the operator does not have a physical facility, the right answer is usually a service-area page that names the region honestly.
“We serve patients across [region] from our [actual city] facility, including [list of cities].” That page can rank for “service in region” queries without claiming a facility that does not exist. The shortcut of templated city pages used to work in 2015 and partially worked in 2020. It works less every year, and the cost-of-getting-caught math in 2026 makes the shortcut unprofitable on any reasonable time horizon.
What if our doorway pages are still ranking well right now?
The pattern we see most often is that a site with doorway pages ranks well for two to four years, then loses the rankings during a core update or after a competitor spam report. The decline is sharp when it comes, and the recovery is slower than the operator expects because the consolidated content has to re-earn the equity that the doorway pages diluted.
Operators who fix the doorway pattern proactively, while the rankings are still healthy, recover faster and lose less. Operators who wait for the suppression event tend to lose 40 to 70 percent of organic before they have a clean version of the site to recover with.
The cost of acting early is lower than the cost of acting after, full stop. If your doorway pages are currently ranking, the right framing is that you are in the window before enforcement, not in a sustainable position. Use the window to consolidate.
Are insurance-page and modality-page templates also doorway pages?
Yes, when the template fill is the only difference between pages. An “Aetna Drug Rehab” page that is identical to a “BCBS Drug Rehab” page except for the payer logo and one boilerplate paragraph is doorway abuse under the same policy. Same for “TMS in [City]” pages that share content with “Ketamine in [City]” pages.
The fix is the same as for city pages: consolidate to one strong page per real differentiator, and let the page carry enough unique content (real payer details, real clinical depth, real patient pathways) to read as a real page.
A site that has done this for insurance and modality usually ends up with 6 to 10 strong pages where the doorway version had 40 to 80 weak ones, and the strong version converts at a higher rate. The same logic that powers our service-pages-first ordering applies: one strong commercial page beats many thin ones, every time.
What does a clean migration off doorway pages look like in the calendar?
Most operators can move off doorway pages in 90 to 120 days if the work is sequenced cleanly. The shape is: week 1 to 2 for the audit and consolidation plan, week 3 to 8 for rewriting the saved pages, week 9 for the redirect push and sitemap update.
Week 10 to 12 covers the technical pass and the paid search compliance check that often surfaces related issues. Month four onward is monitoring the recovery in Search Console.
The biggest scheduling risk is rebuilding the saved pages with real content. Real local pages take a week each to do well because they require sourcing real staff bios, real photos, real payer information, and real geographic context. Operators who try to rebuild 6 to 10 pages in a sprint often end up shipping pages that are still too thin to do the consolidation work.
The perspective in this article comes from 9 years working exclusively inside behavioral health.
We are a team built by people in recovery who understand that behind every admission is someone asking for help. If that resonates, get to know us.
Trevor Gage is the Director of Earned & Owned Media at Webserv, where he leads SEO, content strategy, and organic acquisition for behavioral health treatment centers.
He has overseen audits of more than 200 behavioral health sites and writes about the technical and editorial SEO standards Webserv applies to client work.