Treatment center operators evaluating marketing in 2026 face a structural decision before they evaluate any specific tactic. Behavioral health is the most constrained marketing category in consumer healthcare.
The constraint stack, which includes YMYL ranking standards, HIPAA-restricted tracking, LegitScript certification gates, FTC enforcement on outcome claims, Google’s Healthcare and Medicines policy, Meta’s self-harm classification, and a layer of state-by-state advertising regulation, narrows what is permitted in ways that disqualify most general marketing playbooks operators arrive with.
The operators winning admissions in 2026 are not running better tactics inside the constraints. They are running integrated marketing programs across five pillars where each pillar compounds the others, and where the constraint stack functions as a forcing function rather than a creative ceiling.
We have seen this pattern repeat across dozens of treatment center engagements: the centers running channel-isolated tactics produce category-average cost per admit, and the centers running integrated five-pillar programs produce cost per admit ranges 30 to 50% below the category average.
This guide is the strategic frame: what behavioral health marketing actually includes in 2026, how the five pillars compound, what each pillar costs at each operator spend tier, what a working reporting framework looks like, and how to evaluate whether your current marketing program is producing the compounding effect or running 16 parallel tactics that never connect to admissions.
Behavioral health marketing is the discipline of promoting behavioral health services, which include addiction treatment (residential, PHP, IOP, outpatient, detox), mental health care (depression, anxiety, trauma, dual diagnosis), eating disorder treatment, and co-occurring disorder programs, to prospective patients, referring clinicians, payers, and their families under the compliance constraints of HIPAA, 42 CFR Part 2, EKRA, and state-by-state advertising regulations. This guide covers the full parent category. For addiction treatment specifically, see our rehab lead generation playbook and best marketing agencies for rehabs companion pieces.
Key Takeaways
- Behavioral health marketing is the most constrained consumer healthcare category. Seven distinct compliance layers (YMYL, HIPAA, LegitScript, FTC, Google, Meta, state) disqualify most general marketing playbooks before any tactic is chosen.
- The five-pillar framework compounds. Organic Admissions, Paid Admissions, Admission Ops, Creative, and General Marketing strategy each feed the others. Channel-isolated programs underperform integrated programs at every spend tier.
- Cost benchmarks by total program tier. Tier 1 ($25K to $50K monthly) is foundational. Tier 2 ($75K to $150K) is the floor for compounding programs. Tier 3 ($200K to $500K) is multi-state operator territory. Tier 4 ($500K+) is national.
- Timeline: 12 to 18 months for the compounding moat. First measurable lift on paid lands at month 1 to 3. Organic compounding starts at month 9 to 12. Integrated programs produce defensible cost per admit improvements at month 12+.
- The compliance and tracking layer underwrites everything. Operators who underfund LegitScript certification, HIPAA-compliant tracking, and FTC-defensible creative produce above-category CPAs regardless of channel mix or spend level.
- AEO has moved the discovery layer. AI search engines (ChatGPT, Perplexity, Claude, Google AI Overviews) are now primary discovery surfaces for treatment center queries. Programs not measuring AI citation share are reporting on a layer that no longer drives all the demand.
- Reporting has to tie to admissions, not leads. Programs that report on rankings, traffic, and cost per lead without admit attribution cannot defend their budgets at scale.
- Agency selection is upstream of everything. Most operators underperform because they picked an agency without the operating system underneath. The framework an agency runs matters more than any specific tactic.
Why behavioral health marketing is the most constrained category in consumer healthcare
Operators arriving from ecommerce, SaaS, or even general healthcare marketing repeatedly make the same mistake: they apply playbooks that worked in other verticals to behavioral health and watch the programs underperform without understanding why. The reason is structural. Behavioral health sits at the intersection of seven distinct compliance and policy layers that narrow the creative and operational space available to marketers in ways no other consumer category faces.
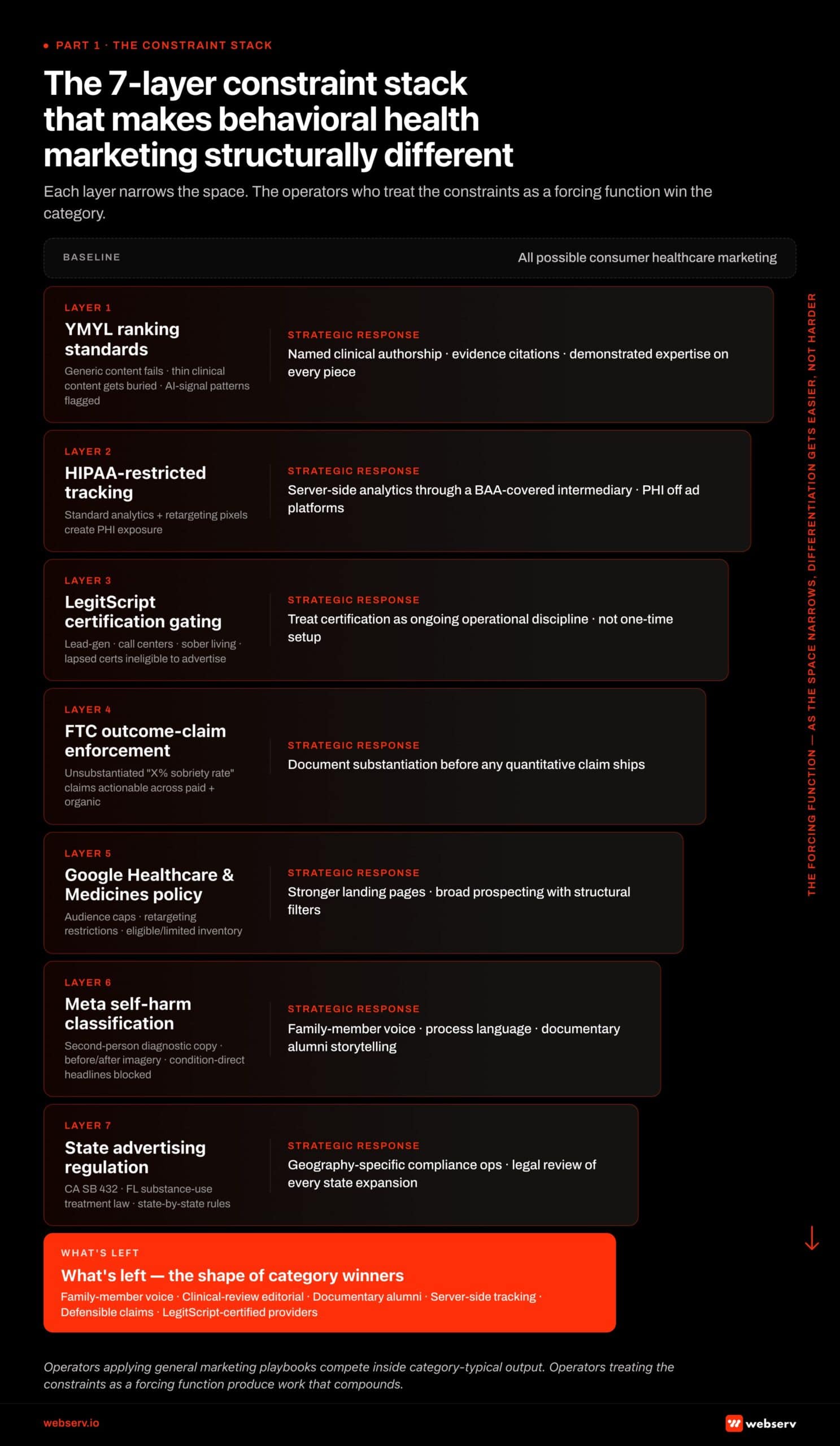 Infographic titled ‘The 7-layer constraint stack that makes behavioral health marketing structurally different.’ Vertical 7-tier stack showing each compliance and policy layer narrowing the marketing space available to behavioral health operators. Tier 1 (widest) represents all possible consumer healthcare marketing. Tier 2 YMYL ranking standards restricts generic content rankings, thin clinical content gets buried, and AI-signal patterns get flagged; strategic response is named clinical authorship plus evidence citations plus demonstrated expertise on every piece. Tier 3 HIPAA-restricted tracking restricts standard analytics and retargeting pixels that create PHI exposure; strategic response is server-side analytics through BAA-covered intermediaries with PHI kept off ad platforms. Tier 4 LegitScript certification gating excludes lead-gen, call centers, sober living, and lapsed certifications from advertising; strategic response is treating certification as ongoing operational discipline. Tier 5 FTC enforcement on outcome claims makes unsubstantiated quantitative claims actionable across paid and organic; strategic response is documenting substantiation before any quantitative claim ships. Tier 6 Google’s Healthcare and Medicines policy applies audience caps, retargeting restrictions, and eligible/limited inventory routing; strategic response is stronger landing pages and broader prospecting with structural filters. Tier 7 Meta’s self-harm classification blocks second-person diagnostic copy plus before-and-after imagery plus condition-direct headlines; strategic response is family-member voice, process language, and documentary alumni storytelling. Tier 8 state advertising regulations (California SB 432, Florida substance use treatment law, state-by-state rules) require geography-specific compliance ops and legal review of every state expansion. Survivor band at the bottom: family-member voice, clinical-review editorial workflow, documentary alumni storytelling, server-side tracking, defensible claims, LegitScript-certified providers.
Infographic titled ‘The 7-layer constraint stack that makes behavioral health marketing structurally different.’ Vertical 7-tier stack showing each compliance and policy layer narrowing the marketing space available to behavioral health operators. Tier 1 (widest) represents all possible consumer healthcare marketing. Tier 2 YMYL ranking standards restricts generic content rankings, thin clinical content gets buried, and AI-signal patterns get flagged; strategic response is named clinical authorship plus evidence citations plus demonstrated expertise on every piece. Tier 3 HIPAA-restricted tracking restricts standard analytics and retargeting pixels that create PHI exposure; strategic response is server-side analytics through BAA-covered intermediaries with PHI kept off ad platforms. Tier 4 LegitScript certification gating excludes lead-gen, call centers, sober living, and lapsed certifications from advertising; strategic response is treating certification as ongoing operational discipline. Tier 5 FTC enforcement on outcome claims makes unsubstantiated quantitative claims actionable across paid and organic; strategic response is documenting substantiation before any quantitative claim ships. Tier 6 Google’s Healthcare and Medicines policy applies audience caps, retargeting restrictions, and eligible/limited inventory routing; strategic response is stronger landing pages and broader prospecting with structural filters. Tier 7 Meta’s self-harm classification blocks second-person diagnostic copy plus before-and-after imagery plus condition-direct headlines; strategic response is family-member voice, process language, and documentary alumni storytelling. Tier 8 state advertising regulations (California SB 432, Florida substance use treatment law, state-by-state rules) require geography-specific compliance ops and legal review of every state expansion. Survivor band at the bottom: family-member voice, clinical-review editorial workflow, documentary alumni storytelling, server-side tracking, defensible claims, LegitScript-certified providers.The seven layers, taken together, define what is possible and what is not in BH marketing:
- YMYL (Your Money or Your Life): Google’s quality framework for content that affects health, finance, or safety decisions. Treatment center content is treated with the strictest scrutiny, requiring named clinical authorship, evidence citations, and demonstrated expertise to rank.
- HIPAA: The Health Insurance Portability and Accountability Act restricts what data can flow between a treatment center’s website and third-party ad platforms. The standard browser pixels and Custom Audiences that work on an ecommerce site are non-compliant on a treatment center site.
- LegitScript certification: Required by Google and Meta before any paid ads serve for addiction treatment. The certification is not a one-time hurdle but an ongoing operational requirement.
- FTC enforcement on outcome claims: The Federal Trade Commission issued 30 warning letters to substance use disorder treatment providers in March 2026 about advertising claims. Unsubstantiated outcome claims like “85% sobriety rate” carry legal risk regardless of platform.
- Google’s Healthcare and Medicines policy: Routes addiction treatment ads through a separate review and approval stack with audience caps, retargeting restrictions, and limited inventory.
- Meta’s self-harm classification: Substance use disorder ads are routed through Meta’s self-harm enforcement stack, which is operationally stricter than mental health enforcement. Second-person diagnostic copy, before-and-after imagery, and direct condition references get flagged.
- State advertising regulations: California’s SB 432, Florida’s substance use treatment marketing law, and similar state-by-state rules add a layer of geography-specific compliance most operators are unaware of until enforcement reaches them.
Research from the FTC’s 2024 Health Products Compliance Guidance reinforces the regulatory layer: unsubstantiated quantitative claims in marketing creative are actionable across paid search, paid social, and organic content alike. The compliance discipline cannot be a paid-side concern only.
The compound effect of these seven layers is that most operators default to creative and operational defaults that are technically compliant and competitively interchangeable. The treatment centers winning the category use the constraints as a creative forcing function. The HIPAA limit on testimonials becomes the case for documentary alumni storytelling produced with full consent.
The Meta self-harm classification becomes the case for family-member voice that converts higher anyway. The Healthcare and Medicines audience cap becomes the case for stronger landing pages and clearer trust signals. Each constraint, taken seriously, becomes a competitive advantage rather than a creative ceiling.
Operators who internalize this framing have a different strategic posture than operators chasing the next tactic. The operators chasing tactics ask “what is working in Meta ads right now?” The operators running integrated programs ask “given our constraint stack, what is the right five-pillar allocation that produces compounding admissions over 18 months?”
How the five pillars compound
The framework we use to evaluate every treatment center marketing program organizes the work into five pillars. The pillars are not channels. They are operational layers, each with its own discipline, and each compounding the others.
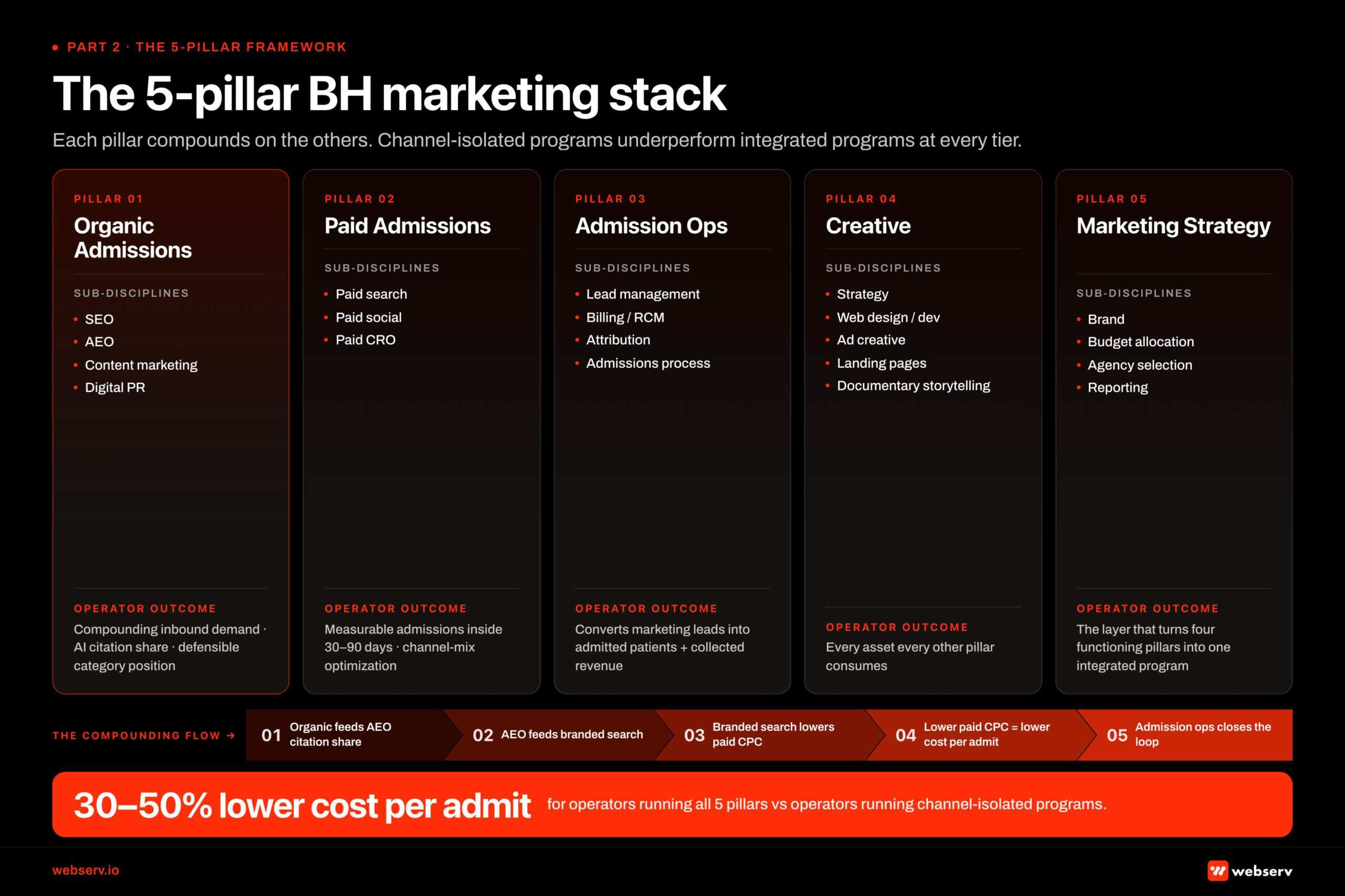 Infographic titled ‘The 5-pillar BH marketing stack’ showing the integrated framework for behavioral health marketing that produces compounding admissions for treatment centers. Pillar 1 Organic Admissions includes SEO, AEO, content marketing, and digital PR — produces compounding inbound demand, AI citation share, and defensible category position. Pillar 2 Paid Admissions includes paid search, paid social, and paid CRO — produces measurable admissions inside 30 to 90 days with channel-mix optimization. Pillar 3 Admission Ops includes lead management, billing and revenue cycle management, attribution, and the admissions process itself — converts marketing-generated leads into admitted patients and collected revenue. Pillar 4 Creative includes strategy, web design and development, ad creative, landing pages, and documentary alumni storytelling — produces every asset every other pillar consumes. Pillar 5 General Marketing strategy includes brand, budget allocation across pillars, agency selection, and reporting framework — the layer that turns four functioning pillars into one integrated program. Compounding flow visualized: organic feeds AEO citation share, which feeds branded search, which lowers paid CPC, which lowers cost per admit, which admission ops closes the loop on. Bottom band: operators running all 5 pillars produce cost per admit 30 to 50 percent below operators running channel-isolated programs.” class=”wp-image-24149″/>
Infographic titled ‘The 5-pillar BH marketing stack’ showing the integrated framework for behavioral health marketing that produces compounding admissions for treatment centers. Pillar 1 Organic Admissions includes SEO, AEO, content marketing, and digital PR — produces compounding inbound demand, AI citation share, and defensible category position. Pillar 2 Paid Admissions includes paid search, paid social, and paid CRO — produces measurable admissions inside 30 to 90 days with channel-mix optimization. Pillar 3 Admission Ops includes lead management, billing and revenue cycle management, attribution, and the admissions process itself — converts marketing-generated leads into admitted patients and collected revenue. Pillar 4 Creative includes strategy, web design and development, ad creative, landing pages, and documentary alumni storytelling — produces every asset every other pillar consumes. Pillar 5 General Marketing strategy includes brand, budget allocation across pillars, agency selection, and reporting framework — the layer that turns four functioning pillars into one integrated program. Compounding flow visualized: organic feeds AEO citation share, which feeds branded search, which lowers paid CPC, which lowers cost per admit, which admission ops closes the loop on. Bottom band: operators running all 5 pillars produce cost per admit 30 to 50 percent below operators running channel-isolated programs.” class=”wp-image-24149″/>Pillar 1: Organic Admissions. Search engine optimization, AI search optimization, content marketing, and digital PR. The work that produces compounding inbound demand over 12 to 18 months. Operators who skip this pillar produce no compounding effect and remain paid-dependent.
Pillar 2: Paid Admissions. Paid search (Google Ads), paid social (Meta, TikTok, others), and paid conversion rate optimization (landing pages, A/B testing). The work that produces measurable admissions inside 30 to 90 days when run with the right compliance stack.
Pillar 3: Admission Ops. Lead management, revenue cycle management, marketing-to-admissions attribution, and the admissions process itself. The work that converts marketing-generated leads into admitted patients and collected revenue. Marketing without admission ops is leakage.
Pillar 4: Creative. Creative strategy, brand foundation, web design and development, ad creative production, landing pages, and documentary alumni storytelling. The work that produces the assets every other pillar consumes.
Pillar 5: General Marketing strategy. Budget allocation across the other four pillars, agency selection, reporting and measurement framework, and the C-suite oversight layer. The work that turns four functioning pillars into one integrated program.
The compounding effect across pillars is what separates integrated programs from channel-isolated programs. Examples:
- Organic content quality (Pillar 1) determines AEO citation share (Pillar 1) which determines branded search volume (Pillar 1) which lowers paid search CPC (Pillar 2) which lowers cost per admit (Pillar 3).
- Documentary alumni storytelling (Pillar 4) becomes hero video on landing pages (Pillar 2) AND organic blog content (Pillar 1) AND social ad creative (Pillar 2) AND AEO citation feedstock (Pillar 1) from one production budget.
- HIPAA-compliant tracking architecture (Pillar 5 + Pillar 3) lets Meta optimize on real admit data (Pillar 2) which produces 2 to 4x admit volume on the same ad spend.
- Strong brand foundation (Pillar 4) produces higher-converting landing pages (Pillar 2) AND better-cited organic content (Pillar 1) AND stronger reporter pitches for digital PR (Pillar 1).
Operators who run any pillar in isolation produce a fraction of the integrated program’s output. Operators who skip pillars entirely produce a fraction of the operators who execute on all five. The strategic question for any treatment center operator is not “which pillar should we focus on” but “what does our current five-pillar allocation look like, and where are the gaps.”
PILLAR 1 · ORGANIC ADMISSIONS
Pillar 1: Organic Admissions
Organic admissions is the pillar that compounds. Every other pillar produces a measurable result tied to current activity. Organic produces results tied to all prior activity, which is why operators who treat organic as a 6-month line item underperform operators who treat it as an 18-month compounding investment.
The pillar has four functional sub-disciplines.
Search engine optimization (SEO)
The technical foundation, keyword strategy, local SEO, and on-page optimization that produce rankings and inbound traffic from Google’s traditional search index. SEO for behavioral health is structurally different from general SEO because of the YMYL classification, HIPAA-restricted analytics, and the clinical-review editorial standard that YMYL queries demand.
Treatment centers that build a sound foundation on the technical SEO layer, develop a deliberate keyword strategy, and invest in the local SEO playbook across their service geographies produce compounding inbound demand that operators relying solely on paid never match.
Answer engine optimization (AEO)
The new layer of organic that emerged through 2024 and 2025. AI search engines (ChatGPT, Perplexity, Claude, and Google AI Overviews) now intermediate a sizable portion of treatment center search demand. Operators who do not measure AI citation share are operating without visibility into one of their primary discovery surfaces.
The full AEO playbook for treatment centers covers the seven layers of work that produce citation share. The short version: clinical authorship, structured citations, schema markup, digital PR, Reddit and community presence, video, and site architecture all contribute. AEO is not a separate discipline from SEO; it is the layer that sits on top of SEO and produces the multiplier.
What changed at Google I/O in May 2026 reshapes how AEO actually works. Gemini 3.5 Flash now powers AI Mode globally, and the new Intelligent Search Box trains users to write longer, multi-faceted prompts instead of short keywords. The unit of search shifted from keyword to compound prompt.
A typical operator query in 2026 reads like “I need a private rehab in LA that takes my insurance and treats anxiety alongside addiction.” That maps to four pages on the operator’s website at once.
AI Mode picks the 3 to 5 sources that satisfy the full prompt, not the source ranking for one keyword. The selection logic shifted; the unit of search shifted with it.
Pages that answer only one slice of the compound prompt get edged out. Pages that address the adjacent slices on the same document, or carry footer entity blocks completing the prompt, become the cited sources. AEO work in 2026 is compound-prompt work.
Content marketing
The editorial discipline that produces the content the SEO and AEO layers depend on. For behavioral health, content marketing is not generic blog production. It is a clinical-review editorial workflow with named authors, named medical reviewers, structured citation requirements, and a review cadence that matches the YMYL standard.
The same editorial discipline underwrites topical authority, which is the cluster-level signal Google’s quality systems and AI engines both reward. Operators who underinvest in editorial discipline produce content that ranks briefly and then loses position as Google’s quality systems detect the lack of E-E-A-T (Experience, Expertise, Authoritativeness, Trustworthiness) signals.
The Google Search Central documentation on helpful, reliable, people-first content explicitly names author expertise, evidence of first-hand experience, and clear sourcing as core signals for ranking YMYL content. Treatment center content that meets these signals compounds; content that does not, decays.
Digital PR and earned media
The discipline of earning coverage in behavioral health publications, mainstream healthcare journalism, and trade media. Digital PR produces three downstream benefits: backlink authority for SEO, citation authority for AEO (AI engines weight named-publication sources heavily), and operator-level brand trust that lifts every other surface.
The operators who treat digital PR as link-building outreach get inconsistent results. The operators who treat it as a relationship-building discipline with healthcare journalists produce 4 to 6 placements a year that compound into category authority.
The compounding pattern across the four sub-disciplines is what makes Organic Admissions the single most consequential pillar over an 18-month horizon. Treatment centers that started investing in organic in 2023 are now capturing AI citation share that paid-only competitors cannot afford to match.
The window for new programs is narrowing as more operators recognize the compounding effect, but it remains the most important investment a treatment center makes if the operator can absorb the 12-month timeline before compounding kicks in.
PILLAR 2 · PAID ADMISSIONS
Pillar 2: Paid Admissions
Paid admissions is the pillar that produces measurable admissions inside 30 to 90 days when run with the right compliance stack and tracking architecture. Operators frequently start here because the timeline is shorter and the attribution feels cleaner. Both perceptions are partially true.
Paid admissions in behavioral health works, but it works inside tighter constraints than any other paid media category, and the operators winning it have a tracking and compliance stack most treatment centers have not built.
Paid search (Google Ads)
The dominant paid channel for treatment center inbound. Google Ads for behavioral health is gated by LegitScript certification, governed by Google’s Healthcare and Medicines policy, and routed through a separate enforcement stack from general healthcare advertising. The Webserv coverage of the full LegitScript certification process documents the operational reality.
The five-stage application, the 4 to 6 week median timeline, the documentation requirements, and the post-certification operational discipline operators need to maintain are all preconditions to running paid search at all.
Inside the compliance gate, the strategic decisions that determine cost per admit are the in-network vs out-of-network playbook split, the campaign structure (intent tier segmentation, level of care, brand defense), the bidding strategy progression (Max Clicks for early-stage accounts, Max Conversions for sustained 30+ conversions per month, Target CPA after 90 days of stable performance), and the budget allocation across campaigns.
Operators who run Google Ads without thinking through these structural decisions burn budget on misallocated campaigns and never reach the optimization threshold where Smart Bidding starts working.
Paid social (Meta, TikTok, others)
Paid social for behavioral health in 2026 looks structurally different from 2022. Meta moved healthcare advertisers into a sensitive category framework starting in January 2025, HHS-OCR civil enforcement actions on tracking technologies doubled year over year, and platform-level audience targeting has narrowed simultaneously.
The operators winning paid social are running an integrated channel mix (Meta dominant at 60 to 75% of social spend, YouTube secondary, TikTok or Reddit for young-adult populations), a HIPAA-safe tracking stack with server-side Meta Conversions API through a BAA-covered intermediary, and a creative framework built around family-member voice and platform-specific compliance.
The audience strategy decision that determines paid social performance is family-vs-patient targeting. For residential treatment, PHP, and high-acuity outpatient programs, the family member is the buyer 70 to 85% of the time. For outpatient programs and MAT, the patient is the direct decision-maker. Mixed-acuity facilities run both playbooks in parallel campaign structures because the buyer pattern, voice, audience signals, and conversion economics all diverge.
Paid CRO and landing pages
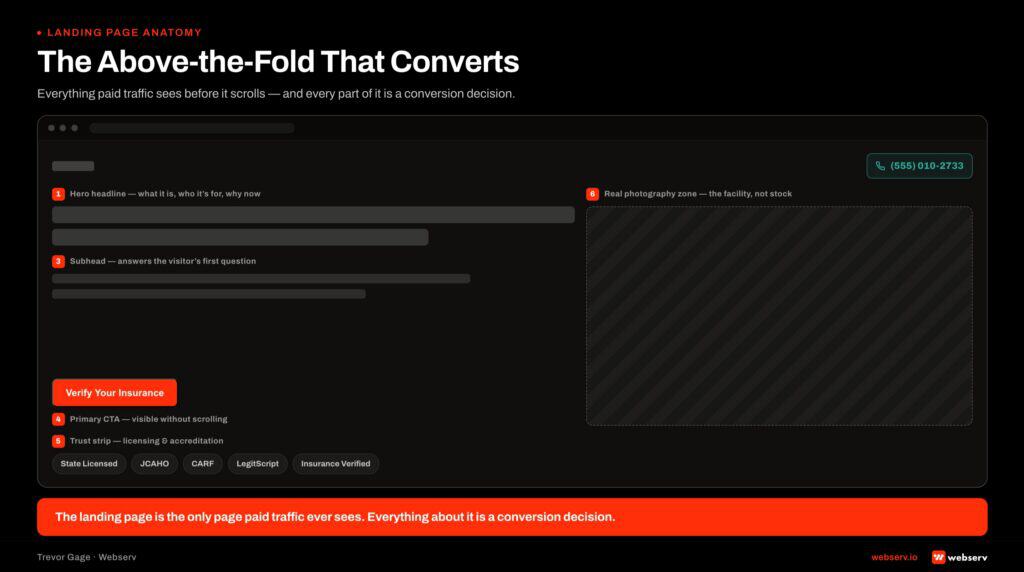
The conversion mechanics that determine how much of the paid traffic becomes a phone call. The biggest single lever on cost per admission for a paid acquisition program is the landing page the traffic lands on. A high-converting page can take the same media spend and produce 3 to 6 times the admission calls of a generic page.
Most rehab operators are running generic pages built for the brand team rather than for a family member in crisis on a phone. The mobile-first reality, the trust signal stack, the confidentiality framing operators underuse, and the call-versus-form CTA architecture are all specific operational decisions that compound into cost per admit.
The compliance gate that gates the entire paid pillar deserves explicit attention. Guidance from the HHS Office for Civil Rights on online tracking technologies confirms that IP addresses combined with health information constitute PHI under HIPAA. Standard Google Ads and Meta pixels firing on a treatment center’s insurance verification page or symptom-assessment page create direct exposure.
The right tracking pattern routes through a server-side intermediary, not a browser-side pixel. Operators who skip this work and run paid programs anyway are running the same paid playbook with disabled ad accounts in their future.
PILLAR 3 · ADMISSION OPS
Pillar 3: Admission Ops
Admission operations is the pillar that converts marketing-generated leads into admitted patients and collected revenue. Treatment center marketing programs without strong admission ops produce admissions inquiries that never become admits, or admits that never become collected revenue. Both are leakage, and both are invisible in most marketing reports because most marketing reports stop at the form-fill or phone call.
The pillar has four functional sub-disciplines: lead management, billing and revenue cycle management, marketing-to-admissions attribution, and the admissions process itself.
Lead management
The discipline of capturing marketing-generated leads in a CRM, routing them to the right admissions counselor inside the right service-level-agreement window, and managing the lead lifecycle from first contact through admission. Speed-to-lead is the single biggest operational lever: admissions inquiries reached inside 5 minutes convert at 4 to 6 times the rate of inquiries reached at 60 minutes.
Most operators have a CRM but no enforced SLA, no automated routing logic, and no visibility into where the leakage happens.
Billing and revenue cycle management
Revenue cycle management for treatment centers is the operational layer that determines whether marketing-generated admits become collected revenue. The full coverage of RCM for treatment centers documents the six levers of a functioning operation: setup verification, verification of benefits, utilization review, claim submission, denial management, and claims follow-up and collections.
The math at the core of the article is operator-distinctive: on $9M of expected revenue, a billing operation running at 75% collection versus 90% collection is a $1.35M annual difference. Most operators chase the wrong lever (lower billing fees) and miss the larger lever (higher collection rates).
For operators running out-of-network or hybrid programs (the majority of behavioral health), the OON billing strategy layer matters more than the in-network mechanics. Patient financial counseling, single-case agreement negotiation, network gap exception requests, and the use of mental health parity law are all operator disciplines that separate OON programs that collect 60 to 75% of billed revenue from OON programs that collect 30 to 45%.
The delta on a typical 90-bed residential operator is $1.5M to $3M annually on a $10M revenue base.
Marketing-to-admissions attribution
The reporting layer that connects marketing spend to admitted-patient revenue. Attribution in behavioral health is harder than in ecommerce because the conversion is offline (a phone call) and the path from inquiry to admit is often multi-touch and multi-channel over days or weeks.
Operators relying on Google Analytics 4 alone see session-to-form-fill data but cannot close the loop to admit. The right attribution stack connects the website analytics (GA4), the call tracking platform, and the intake CRM into a single dataset that reports cost per admit by channel, not just cost per lead by channel.
The admissions process itself
The end-to-end operational system that handles the inquiry from first call through admission. First-60-seconds call script discipline, clinical assessment bridge, pre-qualification checklist, no-show reduction tactics, and level-of-care assessment quality all determine what percentage of marketing-generated inquiries become admits.
The single biggest determinant of conversion is the human at the other end of the phone: admissions counselors trained on the clinical content of the program, the financial reality the family is facing, and the empathy required for someone calling about a loved one in crisis.
Marketing without admission ops is leakage at every stage. The operators winning behavioral health are the ones who treat marketing and admission ops as one integrated program, not two functions that hand off and finger-point when admissions are below target.
How Profound Treatment drove 31 admits and a 42% drop in cost per viable in one quarter
Broad match pivot, negative keyword management, and intake-level conversion tracking turned a fragmented paid strategy into a predictable admissions engine.
Read the case study →68 viable VOBs at $4,529 cost per viable
PILLAR 4 · CREATIVE
Pillar 4: Creative
Creative is the pillar that produces the assets every other pillar consumes. Paid social runs on creative variants. Landing pages run on hero video and trust signal imagery. Organic content runs on clinical photography and named-clinician video. AEO runs on documentary alumni storytelling as a primary citation feedstock.
Brand-level positioning runs through every operator decision from website to ad copy to pitch deck. Underfunding creative is underfunding every other pillar simultaneously.
The pillar has five functional sub-disciplines.
Creative strategy and brand foundation
The upstream decisions about voice, audience, visual identity, message architecture, and format mix that every downstream creative asset reflects. Creative strategy for behavioral health marketing is the layer underneath every ad, landing page, video, email, and organic asset a treatment center ships.
The operators who run it explicitly produce work that compounds. The operators who let category convention dictate the strategy produce work that looks technically correct and converts at category-average rates.
Web design and development
The digital surface of the brand. The treatment center website is the conversion endpoint for organic, paid, AEO citations, and direct-traffic search. Web design for treatment centers is not a one-time project but an ongoing investment in mobile-first design, trust signal placement, conversion-tested user experience, and the technical foundation that determines whether the SEO and AEO work even reaches the index.
Operators who rebuild their website without planning the migration carefully lose rankings predictably, which is the failure pattern Webserv has documented across dozens of treatment center engagements.
Ad creative
Paid ad creative production at the volume the platforms require. Meta’s Advantage+ campaigns require 20 to 30 active creative variants per campaign and continuous refresh every 2 to 4 weeks. Google Ads Responsive Search Ads require 15 headlines and 4 descriptions per ad group, tailored to the intent of each ad group.
Operators running paid social with 5 creative variants and no refresh cadence are starving the algorithm of the signal it needs to optimize.
Landing pages
The conversion endpoint that turns paid clicks into phone calls. Treatment center landing pages built for high-conversion paid traffic look different from brand pages and different from organic content pages. Sticky phone above the fold, real facility photography (not stock), specific operator USPs that distinguish the facility from category-typical messaging, mobile-first design, and trust signal architecture that addresses the family-member-in-crisis reality all matter.
Most operators run landing pages that were built for a clinical director’s approval and not for a family member on a phone.
Documentary alumni storytelling
The highest-converting creative format in behavioral health, and the asset most operators underproduce. Documentary alumni stories produced with full HIPAA-compliant consent and documentary craft (interview, B-roll, story arc, music, edit) outperform stock photography and generic clinician imagery by 30 to 50% on landing page conversion.
The same production budget produces 12 distribution assets: a full-length film, paid social cutdowns, landing page hero video, organic social, podcast guest appearances, blog post embeds, and AEO citation surfaces. Operators who treat alumni storytelling as a one-off video shoot produce one asset and miss the multiplier.
The constraint stack from the opening section shapes what is possible in creative more than any other pillar. HIPAA restrictions on testimonials. Meta’s self-harm classification’s restrictions on second-person diagnostic copy. FTC restrictions on unsubstantiated outcome claims.
LegitScript’s restrictions on lead-generator and call-center business models. Each of these eliminates a category of creative work that would be acceptable in other healthcare verticals. The brands that win in BH treat each restriction as a creative forcing function and produce documentary, family-voiced, evidence-backed, defensibly-claimed creative that competitors who treat the restrictions as ceilings cannot match.
PILLAR 5 · STRATEGY
Pillar 5: Strategy, oversight, and budget allocation
Pillar 5 is the meta-layer that turns four functioning pillars into one integrated program. Brand positioning, budget allocation, agency selection, and the C-suite reporting framework all live here.
Most operators underinvest in this pillar because the work sits upstream of any specific tactic. The value is hard to see until you compare a program with strong Pillar 5 against one without it.
Brand positioning is the articulation of what makes the facility distinctive. Not “compassionate, evidence-based care.” Specific: the only adolescent residential program in California with on-site academic credit.
The veteran-built program with the only TRICARE West contract in its regional service area. The boutique program with 24-hour direct access to the medical director. If the operator cannot say the positioning in one paragraph, marketing cannot route the right traffic to the right value proposition.
Agency selection is the single most consequential operator decision at this layer. Operators who succeeded with a prior agency typically moved to Webserv because the prior partner could not scale.
Operators who failed with a prior agency typically picked one without an underlying operating system. The Client Brain operating system covers the eight components that separate agencies that compound from agencies that ship category-typical work.
The rest of Pillar 5 gets operational treatment in the sections below: program sizing by tier, the realistic 3-to-24-month timeline, when to build versus hire, what a reporting framework that ties to admissions contains, and the common operator mistakes at this layer.
The treatment centers that compound are the ones treating marketing as five integrated pillars, not five separate budgets. The ones that decline treat marketing as the line item the CFO cuts first when admissions are below target. The difference is whether the operator’s reporting framework can defend the program in the budget conversation.
Preston Powell, CEO, Webserv
Cost benchmarks by program tier
Operators evaluating marketing investment frequently ask “how much should we be spending?” before they ask “what should we be spending on?” The order is backwards. The right starting question is “what does our operator profile look like, what tier of program does that profile require, and what is the right allocation pattern across the five pillars at that tier?”
The four tiers we observe across treatment center marketing programs map roughly to operator scale, facility count, and geographic footprint. The dollar ranges and pillar allocations below are illustrative; specific operator situations vary based on payer mix, level of care, regional competition, and brand maturity. Verify the right tier for your facility against current performance and benchmarks before allocating.
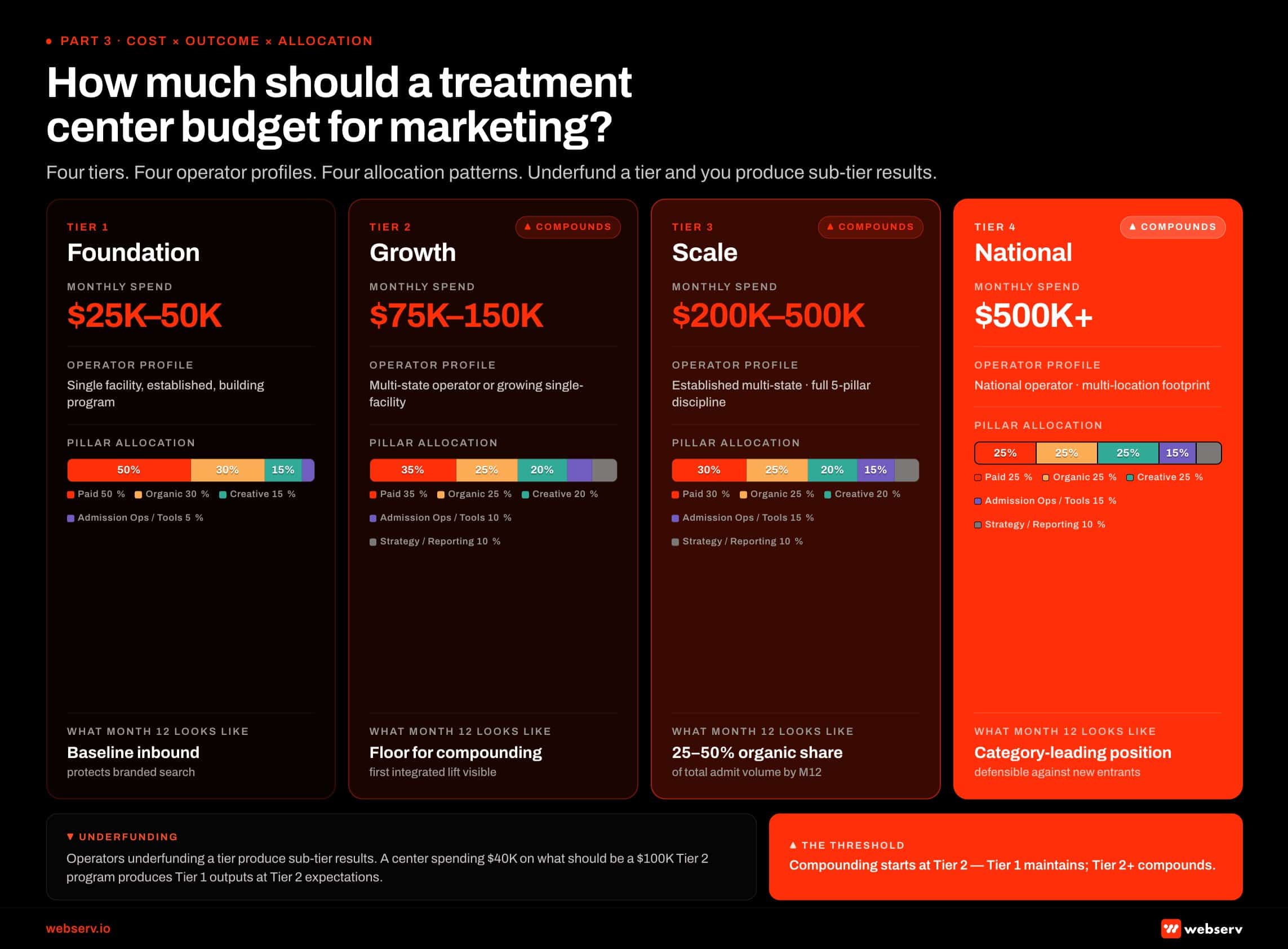 Infographic titled ‘How much should a treatment center budget for marketing?’ showing the four-tier behavioral health marketing investment framework. Tier 1 Foundation: $25K to $50K monthly spend, applies to single-facility established operators building program, pillar allocation runs 30 percent paid search + 20 percent paid social + 30 percent organic + 15 percent creative + 5 percent tools and operations, produces baseline inbound that protects branded search. Tier 2 Growth: $75K to $150K monthly, applies to multi-state or growing single-facility operators, pillar allocation runs 35 percent paid + 25 percent organic + 20 percent creative production + 10 percent admission ops tech + 10 percent reporting, this is the floor for compounding programs. Tier 3 Scale: $200K to $500K monthly, applies to established multi-state operators running full 5-pillar discipline, pillar allocation runs 30 percent paid + 25 percent organic + 20 percent creative + 15 percent admission ops + 10 percent strategy and reporting, organic carries 25 to 50 percent of total admit volume by month 12. Tier 4 National: $500K and above monthly, applies to national operators with multi-location footprints, pillar allocation runs 25 percent paid + 25 percent organic + 25 percent creative + 15 percent admission ops + 10 percent strategy, produces a category-leading position the operator can defend against new entrants. Bottom callout: operators underfunding a tier produce sub-tier results, so a center spending $40K monthly on what should be a $100K Tier 2 program produces Tier 1 outputs at Tier 2 expectations.
Infographic titled ‘How much should a treatment center budget for marketing?’ showing the four-tier behavioral health marketing investment framework. Tier 1 Foundation: $25K to $50K monthly spend, applies to single-facility established operators building program, pillar allocation runs 30 percent paid search + 20 percent paid social + 30 percent organic + 15 percent creative + 5 percent tools and operations, produces baseline inbound that protects branded search. Tier 2 Growth: $75K to $150K monthly, applies to multi-state or growing single-facility operators, pillar allocation runs 35 percent paid + 25 percent organic + 20 percent creative production + 10 percent admission ops tech + 10 percent reporting, this is the floor for compounding programs. Tier 3 Scale: $200K to $500K monthly, applies to established multi-state operators running full 5-pillar discipline, pillar allocation runs 30 percent paid + 25 percent organic + 20 percent creative + 15 percent admission ops + 10 percent strategy and reporting, organic carries 25 to 50 percent of total admit volume by month 12. Tier 4 National: $500K and above monthly, applies to national operators with multi-location footprints, pillar allocation runs 25 percent paid + 25 percent organic + 25 percent creative + 15 percent admission ops + 10 percent strategy, produces a category-leading position the operator can defend against new entrants. Bottom callout: operators underfunding a tier produce sub-tier results, so a center spending $40K monthly on what should be a $100K Tier 2 program produces Tier 1 outputs at Tier 2 expectations.Tier 1: Foundation ($25K to $50K monthly)
Single-facility operators, established but building. The Tier 1 program is foundational maintenance plus light growth investment. Pillar allocation typically lands at 30% paid search, 20% paid social, 30% organic (SEO foundation, light AEO, light content production), 15% creative production, and 5% tools and reporting.
Tier 1 produces a baseline of inbound admissions and protects the operator’s branded search traffic. It does not produce compounding admission volume without progression to Tier 2.
Tier 2: Growth ($75K to $150K monthly)
Multi-state or growing operators. The Tier 2 program is the floor for integrated five-pillar execution that produces compounding admit volume over 12 to 18 months.
Allocation typically lands at 35% paid (split across paid search and paid social), 25% organic (full SEO foundation, AEO investment, content production cadence, digital PR pilot), 20% creative production (documentary alumni storytelling cadence, ad creative refresh), 10% admission ops tech and process investment, and 10% reporting and attribution infrastructure. Operators who underfund Tier 2 produce Tier 1 results.
Tier 3: Scale ($200K to $500K monthly)
Established multi-state operators or single-location operators with a strong inbound brand. The Tier 3 program runs the full five-pillar discipline at scale.
Allocation typically lands at 30% paid (with broader platform mix and population-specific campaigns), 25% organic (full SEO, AEO, content marketing, digital PR all running at production cadence), 20% creative (full documentary alumni cadence, ad creative production at volume, web property maintenance), 15% admission ops (RCM partner, attribution infrastructure, lead management discipline), and 10% strategy and reporting (agency partner relationships, monthly executive reporting, quarterly strategic review).
Tier 4: National ($500K+ monthly)
National operators with multi-location footprints. Tier 4 programs run all five pillars at scale across multiple service geographies, with internal teams managing brand and clinical leadership content while agency partners run the operational execution. Allocation typically lands at 25% paid, 25% organic, 25% creative production at scale, 15% admission ops infrastructure, and 10% strategy and reporting.
The defining characteristic of Tier 4 is that the integrated five-pillar discipline produces a category-leading position the operator can defend against new entrants.
Operators who underfund a tier produce sub-tier results. A treatment center spending $40K monthly on what should be a $100K monthly Tier 2 program produces Tier 1 outputs at Tier 2 cost. The right way to evaluate whether the program is sized correctly is to compare current cost per admit against the appropriate tier benchmark and adjust either the spend or the allocation pattern.
Timeline at 3, 6, 12, and 24 months
The single most common reason treatment center marketing programs fail is timeline expectation mismatch. Operators expect organic results on paid-media-speed timelines, conclude organic is not working at month 6, and cut the investment. Twelve months later, the operators who maintained organic investment are capturing inbound traffic that the operators who cut it cannot replace at paid spend levels.
The realistic timeline for an integrated five-pillar program looks like this.
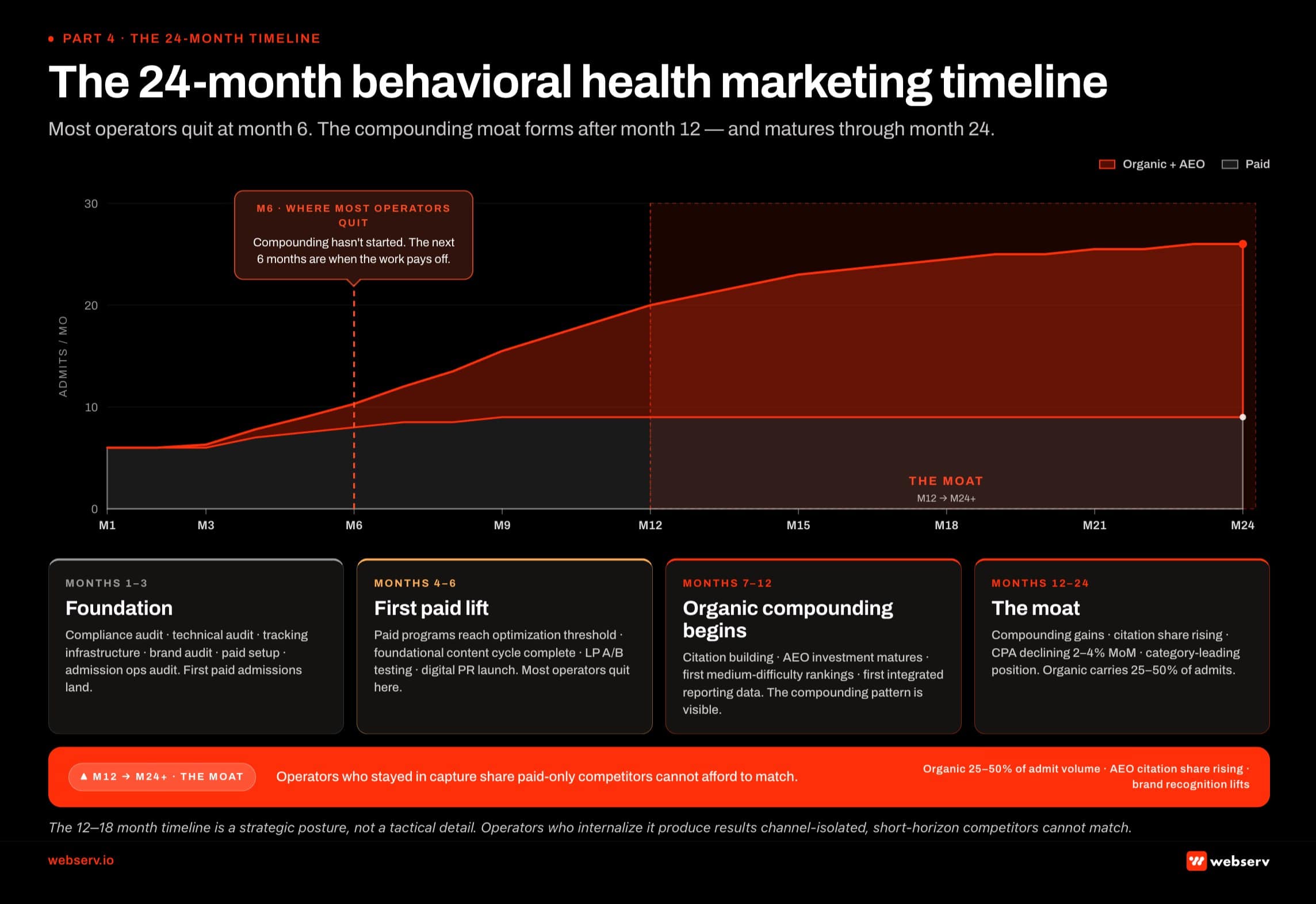 Infographic titled ‘The 24-month behavioral health marketing timeline’ showing what compounds when across two years of an integrated 5-pillar marketing program for treatment centers. Phase 1 Foundation (Months 1 to 3): compliance audit including LegitScript and HIPAA tracking, technical audit, content audit, brand audit, paid program setup, and admission ops audit; first paid admissions land but organic is still building. Phase 2 First paid lift (Months 4 to 6): paid programs reach optimization threshold with cost per admit improving 15 to 30 percent vs month 1, foundational content cycle completes, landing pages mature, digital PR placements begin; organic still pre-compounding. Red dashed warning band at Month 6: where most operators quit, but the compounding pattern starts here. Phase 3 Organic compounding begins (Months 7 to 12): citation building accelerates, AEO investment matures, first medium-difficulty rankings appear, AEO citation share visible across ChatGPT, Perplexity, Claude, and Google AI Overviews, first integrated reporting shows multi-channel compounding. Phase 4 The moat (Months 12 to 24 plus): cost per admit declines 2 to 4 percent month over month, organic carries 25 to 50 percent of admit volume by tier, brand recognition lifts in service geographies, operator now defends category position rather than building it.
Infographic titled ‘The 24-month behavioral health marketing timeline’ showing what compounds when across two years of an integrated 5-pillar marketing program for treatment centers. Phase 1 Foundation (Months 1 to 3): compliance audit including LegitScript and HIPAA tracking, technical audit, content audit, brand audit, paid program setup, and admission ops audit; first paid admissions land but organic is still building. Phase 2 First paid lift (Months 4 to 6): paid programs reach optimization threshold with cost per admit improving 15 to 30 percent vs month 1, foundational content cycle completes, landing pages mature, digital PR placements begin; organic still pre-compounding. Red dashed warning band at Month 6: where most operators quit, but the compounding pattern starts here. Phase 3 Organic compounding begins (Months 7 to 12): citation building accelerates, AEO investment matures, first medium-difficulty rankings appear, AEO citation share visible across ChatGPT, Perplexity, Claude, and Google AI Overviews, first integrated reporting shows multi-channel compounding. Phase 4 The moat (Months 12 to 24 plus): cost per admit declines 2 to 4 percent month over month, organic carries 25 to 50 percent of admit volume by tier, brand recognition lifts in service geographies, operator now defends category position rather than building it.Month 1 to 3: foundation
Compliance audit (LegitScript status, HIPAA tracking, FTC creative review). Technical audit (mobile-first, schema, Core Web Vitals, site architecture). Content audit (E-E-A-T status of existing content, clinical-review workflow audit). Brand audit (positioning clarity, voice consistency, message architecture).
Paid program setup or restructure (campaign architecture, conversion tracking, creative refresh). Admission ops audit (CRM, attribution, lead routing). First paid admissions typically land in this window, but the organic work has not yet produced measurable results.
Month 4 to 6: first paid lift and foundational content cycle
Paid programs reach optimization threshold and produce cost per admit improvements of 15 to 30% vs month 1. First content publishing cycle delivers initial SEO ranking lift on long-tail queries. Landing pages reach mature conversion rates. First A/B testing cycle on paid creative completes. Digital PR placements begin. Operators who quit the program in this window do so right before compounding starts and produce nothing.
Month 7 to 12: organic compounding begins
SEO content cluster reaches critical mass and starts ranking for medium-difficulty commercial queries. AEO citation share visible across ChatGPT, Perplexity, Claude, and Google AI Overviews. First measurable organic admission volume reported. Paid program runs efficiently with mature optimization. First integrated reporting data shows the five-pillar program’s compounding effect.
Cost per admit starts to decline 2 to 4% month over month as organic carries an increasing share of admission volume.
Month 12 to 24: the moat
Organic admission volume reaches a sizable percentage of total admissions (typically 25 to 50% depending on tier). AEO citation share continues to rise. Brand recognition lifts in service geographies. Cost per admit stabilizes at the integrated-program benchmark for the tier, with the operator now defending market position against new entrants rather than building it.
The moat from year 1 to year 2 is what separates operators who treated marketing as compounding investment from operators who treated it as expense.
Operators expecting paid-media-speed results from the full five-pillar program quit at month 6. Operators who internalize the 12-to-18-month compounding timeline produce admit volume that paid-only competitors cannot afford to match. The timeline is a strategic posture, not a tactical detail.
How SoCal Sunrise generated 85 admissions and 2,297% ROI from SEO in 6 months
A ground-up SEO rebuild using the Pathfinder Parents Methodology turned an invisible online presence into a top-ranking admissions engine.
Read the case study →85 admits and 3,152 leads attributed to organic
Agency vs. in-house: when to build, when to hire
Every treatment center operator at some point evaluates whether to run marketing in-house, hire an agency, or build a hybrid model. The right answer depends on operator scale, in-house capacity, and the specific pillar in question.
The in-house model works for operators with annual marketing budgets above $1M, in-house content production capacity, and a CMO or marketing director with the strategic depth to coordinate across the five pillars. Tier 4 national operators frequently run in-house brand, clinical leadership content, and alumni community work while agency partners run technical execution.
The cost is highest at the team level but lowest per asset at scale. The risk is that institutional knowledge concentrates in a small number of internal team members and walks out the door when they leave.
The agency model works for most Tier 1 and Tier 2 operators. The ramp is faster, the fixed cost is lower, and the specialized expertise across SEO, paid media, creative, and reporting is available without hiring a five-person internal team. For the operator-side ranking of behavioral health SEO agencies specifically, see our scored shortlist.
The risk is that agency creative defaults tend to be category-typical, which makes differentiation harder unless the operator drives the strategy explicitly. Agency selection becomes the single most consequential decision in this model.
The hybrid model is the most common pattern for Tier 2 and Tier 3 operators. The agency runs paid media execution, technical SEO, AEO, content production at volume, and reporting infrastructure. The operator owns brand creative, founder portraiture, clinical leadership content, alumni community storytelling, and the executive-level strategic decisions.
The hybrid model captures the speed advantage of agency execution while preserving the differentiation advantage of operator-owned brand work. The breakdown of responsibility has to be explicit; ambiguity in the hybrid model produces work that falls through gaps.
For operators evaluating agency partners specifically, our coverage of the best marketing agencies for rehabs documents the working framework. The framework an agency runs matters more than any specific tactic, because the framework is what makes the work compound across engagements and across team turnover. Operators who want a head-start on the diligence can also work from our paid social ad agency shortlist, which scores the firms already running 2026-grade stacks against this same framework.
The reporting framework operators actually need
The reporting framework is the layer that makes the integrated five-pillar program defensible at the budget meeting. Programs that report on rankings, traffic, and cost per lead cannot answer the C-suite question “what did we get for the marketing investment?” Programs that report on cost per admit by channel, AEO citation share, and integrated five-pillar performance can.
The reporting stack has three layers. Each compounds the others.
Layer 1: Creative and asset-level performance
Per-asset metrics like hook rate, hold rate, completion rate on video, click-through rate, cost per click, and conversion rate by variant. The input to creative iteration. Tells you which specific assets are doing the conversion work. Updated continuously in the ad platforms and reviewed weekly.
Layer 2: Channel-level performance
Per-channel metrics like cost per lead, cost per verified-policy VOB, and cost per admit by channel. Volume contribution by channel. AEO citation share by query set. The input to budget allocation decisions. Tells you whether the channel mix is right. Reported monthly with trend lines over the prior 6 to 12 months.
Layer 3: Program-level outcomes
Total admits per month, average payer mix, average length of stay, revenue per admit, and marketing cost per admit. The C-suite reporting layer. Tells you whether the marketing program is producing the business outcome the operator needs. Reported monthly to the executive team and quarterly to the board.
The benchmark for a working integrated program is that marketing cost per admit declines 2 to 4% month over month for the first 12 months, then stabilizes at a tier-appropriate level. The program scales by adding budget rather than by improving efficiency once it reaches that stabilization point.
Operators whose cost per admit is rising are running a marketing program that has stopped working, and the fix is usually upstream of the campaign layer. The fix is in the strategy, brand, audience framework, or message architecture.
Common behavioral health marketing mistakes
Eight patterns show up consistently in treatment center marketing programs that underperform.
Treating BH like general marketing. The seven-layer constraint stack disqualifies most general marketing playbooks. Operators who apply ecommerce, SaaS, or even general healthcare playbooks to behavioral health produce programs that look reasonable and underperform structurally. Recognize the category as structurally different from day one.
Underfunding the compliance and tracking layer. LegitScript certification, HIPAA-compliant server-side tracking, FTC-defensible creative review, and state advertising compliance are all preconditions to running marketing programs at scale. Operators who skip this layer produce above-category CPAs regardless of channel mix.
Quitting organic at month 6. The organic compounding pattern starts at month 9 to 12. Operators who quit at month 6 do so right before the work starts producing measurable results. The next 12 months of competitive position is determined by whether the operator stays in or quits in this window.
Stock creative that signals interchangeability. Treatment center creative that uses stock photography, stock language (“compassionate, evidence-based”), and generic clinical imagery signals to family members that this facility is interchangeable with every other facility. The cost is not just lower conversion. It is brand-level commodity positioning that takes years to climb out of.
Channel-isolated reporting without admit attribution. Programs that report cost per lead by channel cannot answer the C-suite question about cost per admit. Reports that do not tie to admissions cannot defend the budget. Building the marketing-to-admissions attribution layer is upstream of every other reporting improvement.
Picking an agency without the operating system underneath. The Client Brain framework documents the 8 components every working agency runs as an operating system. Agencies without this system ship category-typical content. Operators who pick on price or on relationship without diligence on the system frequently sign with agencies that cannot scale with the operator’s growth.
Building paid programs before the compliance and landing page foundation is solid. Paid traffic to a landing page that fails Core Web Vitals, lacks HIPAA-compliant tracking, or runs FTC-vulnerable claims produces ad account disables and wasted budget. The foundation has to come first.
Ignoring AEO because “AI search is still emerging.” AI search is no longer emerging. It is a primary discovery surface for treatment center queries in 2026. Operators not investing in AEO are losing citation share on a metric most marketing teams are not measuring. The 12-month window for getting ahead is closing as more operators recognize the compounding pattern.
WHAT INTEGRATED PROGRAMS DO
- Run all five pillars as one integrated program
- Hold paid through the 12-to-18-month organic compounding window
- Single internal owner for marketing-to-admissions attribution
- Brand positioning that survives across every creative asset
- Documentary alumni storytelling in the production calendar
WHAT BROKEN PROGRAMS SKIP
- Run paid as if organic does not exist
- Cut organic at month 6 because “it is not working yet”
- No one internally owns the funnel-to-admission report
- Different brand voice on every campaign and creative
- Stock library imagery that fits every other rehab site
What changed in 2025 and 2026
Six structural shifts changed behavioral health marketing in the last 18 months. Programs that have not adjusted to these shifts are running 2022 playbooks against a 2026 reality.
First, AI search engines became primary discovery surfaces. ChatGPT, Perplexity, Claude, and Google AI Overviews now intermediate a sizable percentage of treatment center search demand. The operators who invested in AEO through 2024 and 2025 are capturing citation share that paid-only competitors cannot match.
Second, Meta moved healthcare advertisers into a sensitive category framework in early 2025. Substance use disorder ads now route through Meta’s self-harm enforcement stack, with tighter audience targeting restrictions, optimization signal restrictions, and creative policy enforcement.
Third, the FTC issued 30 warning letters to substance use disorder treatment providers in March 2026 about advertising claims. The federal regulatory layer on outcome claims is now actively enforced, and the cost of unsubstantiated claims has moved from theoretical to actionable.
Fourth, HHS-OCR enforcement on online tracking technologies escalated through 2025 and 2026. Civil enforcement actions on healthcare tracking technologies more than doubled year over year, and the HIPAA-restricted tracking layer is now an active operator-level compliance concern, not a theoretical one.
Fifth, LegitScript audit patterns shifted toward more frequent re-certification reviews and stricter material-change reporting requirements. Operators who treated LegitScript certification as a one-time setup are now finding themselves under continuous-audit obligations they had not budgeted for operationally.
Sixth, Google’s May 2026 I/O announcements moved Search from keyword-matching to compound-prompt-matching. Gemini 3.5 Flash powers AI Mode globally. The new Intelligent Search Box trains users to write longer prompts. Information agents and agentic booking start intermediating the action layer this summer.
The compound-prompt shift means position 2 to 5 in traditional rankings is no longer a click-capture band. It is the citation pool Gemini 3.5 Flash picks from when generating AI Mode answers. Operators chasing clicks at that position miss the citation share that now drives the demand.
The compound effect of these six shifts is that the 2022 marketing playbook does not produce 2026 results. Operators running 2022 programs are losing share to operators running 2026 programs. The gap between the two is the work covered across this guide.
Frequently asked questions about behavioral health marketing
What does behavioral health marketing actually include?
Behavioral health marketing is the integrated discipline that produces admitted patients for treatment centers. It includes five operational pillars: organic admissions (SEO, AEO, content marketing, digital PR), paid admissions (paid search, paid social, conversion rate optimization), admission operations (lead management, billing and RCM, attribution, admissions process), creative (brand foundation, web design and development, ad creative, landing pages, documentary storytelling), and general marketing strategy (budget allocation, agency selection, reporting). The pillars compound on each other.
Operators arriving from general marketing frequently treat behavioral health marketing as a collection of tactics. The framework above treats it as a system. The difference matters operationally because channel-isolated execution produces fragmented results that do not compound, and integrated execution produces a compounding admission funnel over 12 to 18 months.
The work each pillar covers is substantial in its own right. Each has its own constraint stack (HIPAA, LegitScript, FTC, Google policy, state regulations), its own measurement framework, its own cost benchmarks, and its own timeline. The integrated guide above covers the strategic frame across all five; the subservice cluster hubs we publish go deeper on each individual pillar.
How much should a treatment center budget for marketing?
The right marketing budget is a function of operator scale and current performance. Tier 1 (foundational) programs land at $25K to $50K monthly. Tier 2 (growth) programs at $75K to $150K monthly. Tier 3 (scale) programs at $200K to $500K monthly. Tier 4 (national) programs at $500K and above monthly. Each tier requires a specific pillar allocation pattern to produce its expected results.
Operators who underfund a tier produce sub-tier results. A center spending $40K monthly on what should be a $100K Tier 2 program produces Tier 1 outputs at Tier 2 expectations, then gets frustrated that the program is not compounding. The right diagnostic is to compare your current cost per admit against the benchmark for your tier and identify whether the gap is in spend level, pillar allocation, or execution quality.
Most operators we work with discover they are either underfunding the compounding pillars (organic and creative) or overfunding the short-term pillars (paid) relative to their tier’s compounding potential. The reallocation conversation is more impactful than the budget-increase conversation in most cases.
How long before marketing produces measurable admits?
First paid admissions typically land in month 1 to 3 once the campaign architecture, compliance stack, and conversion tracking are in place. Organic admissions start appearing in volume at month 9 to 12 as content clusters mature and AEO citation share builds. The integrated program reaches a stable cost-per-admit benchmark at month 12 to 18, where the work becomes a defensible category-leading position.
The single most common reason marketing programs fail is timeline expectation mismatch. Operators who expect organic results on paid-media timelines quit at month 6, right before the compounding pattern starts producing measurable lift. The 12-to-18-month timeline is a strategic posture, not a tactical detail, and operators who internalize it produce results that channel-isolated, short-horizon competitors cannot match.
The realistic timeline for a Tier 2 or Tier 3 operator running the full five-pillar discipline: 30 to 90 days for first paid admissions, 6 to 9 months for foundational organic ranking lift, 12 months for AEO citation share to become a leading indicator of organic growth, and 18 to 24 months for the integrated program to produce a stable cost-per-admit benchmark and a defensible market position.
Should we run marketing in-house or hire an agency?
The in-house model works for operators with annual marketing budgets above $1M and in-house content production capacity. The agency model works for most Tier 1 and Tier 2 operators where the agency’s specialized expertise across SEO, paid media, creative, and reporting is faster to access than building it internally. The hybrid model (agency runs technical execution; operator owns brand and clinical leadership content) is the most common pattern for Tier 2 and Tier 3 operators.
The agency selection decision matters more than the in-house-versus-agency decision in most cases. Agencies without an operating system (the 8-component framework that covers positioning, clinical leadership, audience documentation, voice, trust signals, topic and content gap maps, performance history, and operator-stated constraints) ship category-typical content regardless of how much the operator spends. Agencies with a strong operating system produce work that compounds. The diligence questions to ask before signing with any agency partner separate the two.
For operators evaluating partners, our coverage of the best marketing agencies for rehabs documents the working evaluation criteria.
What is the difference between BH marketing and general healthcare marketing?
Behavioral health marketing operates inside a seven-layer constraint stack that general healthcare marketing does not face. YMYL ranking standards, HIPAA-restricted tracking, LegitScript certification gates, FTC enforcement on outcome claims, Google’s Healthcare and Medicines policy, Meta’s self-harm classification, and state-by-state advertising regulations all combine to narrow the creative and operational space available in ways no other healthcare vertical faces.
The compound effect: most general healthcare marketing playbooks are technically permissible in behavioral health but commercially ineffective. Stock testimonials do not work because HIPAA restricts patient stories without consent. Direct-response copy does not work because Meta’s self-harm classification flags it. Outcome claims do not work because the FTC actively enforces against them. Standard tracking pixels do not work because they create HIPAA exposure.
Treatment centers that internalize the constraint stack as a creative forcing function produce documentary alumni storytelling, family-member-voice creative, defensibly-claimed messaging, and HIPAA-safe tracking architectures that outperform general healthcare playbooks. The constraints, taken seriously, become the competitive advantage.
What is the most consequential layer of behavioral health marketing?
The single most consequential layer over an 18-month horizon is Organic Admissions, specifically the combination of SEO, AEO, content marketing, and digital PR running together as one integrated discipline. Organic compounds in a way no other pillar does, and operators who invest in it from month 1 produce admission volume in months 12 through 24 that paid-only competitors cannot afford to match.
The reason organic carries the most weight: every admission generated by an organic search query or AI citation costs the operator nothing in incremental media spend after the initial content production cost. The compounding pattern means month 24’s organic admission volume is materially larger than month 12’s, while paid spend produces the same admission output every month for the same spend. The math compounds in organic’s favor as the program ages.
The catch is the timeline. Organic does not produce material results inside 6 months. Operators who do not have the capital or strategic patience to invest for 12 to 18 months before measurable compounding starts will not produce organic’s results regardless of how strong the execution is. For operators with that timeline, organic is the most consequential investment available.
How do AI search and AEO affect treatment center marketing?
AI search engines (ChatGPT, Perplexity, Claude, and Google AI Overviews) became primary discovery surfaces for treatment center queries through 2024 and 2025. By 2026, a sizable percentage of high-intent operator-research-stage search demand for treatment centers is intermediated by AI engines rather than traditional blue-link search. Operators not measuring AI citation share are operating without visibility into one of their primary discovery surfaces.
The work that produces AI citation share is structurally adjacent to but distinct from traditional SEO. Named clinical authorship, structured citations, schema markup, digital PR and earned media, Reddit and community presence, video content, and site architecture all contribute. AEO is not a separate discipline from SEO; it is the layer that sits on top of SEO and produces the multiplier effect.
Treatment centers that started investing in AEO through 2024 and 2025 are now capturing citation share that paid-only competitors cannot match. The 12-month window for getting ahead is closing as more operators recognize the compounding pattern, but it remains the most consequential organic investment available for centers with the 12-to-18-month strategic patience to invest in it. Our AEO playbook for treatment centers covers the seven-layer operational frame.
What is the most common reason treatment center marketing fails?
Channel-isolated execution without admit attribution is the most common failure pattern. Marketing teams run paid social, paid search, SEO, and content as four separate disciplines that never connect to admission ops, never share data across channels, and never report at the cost-per-admit level. The result is a marketing program that produces leads but cannot defend the budget at the C-suite level when admissions are below target.
The fix is upstream of any specific tactic. The reporting framework has to tie marketing spend to admitted-patient revenue. The five-pillar program has to run as one integrated discipline, not five separate budgets. The agency selection has to prioritize a partner with an operating system that compounds, not a partner with cheap deliverables. The strategic posture has to support 12-to-18-month timelines on organic, not paid-media-speed expectations across the whole program.
Treatment centers that internalize these strategic decisions produce compounding programs that outperform the category. Treatment centers that do not internalize them run programs that look reasonable and underperform structurally regardless of how much budget they spend. If you want a second opinion on whether your current program is producing the integrated five-pillar compounding effect, reach out for a strategy session and we can walk through where the gaps are.
Where to start: the 90-day operator playbook
Days 1-30 · Diagnose
Audit pillar allocation, verify compliance status (LegitScript, HIPAA tracking, FTC review), and pull the current cost-per-admit by channel.
Days 31-60 · Decide
Confirm tier fit, pick the operating model (in-house, agency, hybrid), and name the single internal owner for marketing-to-admissions reporting.
Days 61-90 · Deploy
Stand up the compliance and tracking foundation, restart paid programs against the new architecture, and begin the content cadence the 12-18 month compounding rides on.
Behavioral health marketing in 2026 rewards operators who treat it as one integrated five-pillar program with strategic patience for the 12-to-18-month compounding timeline. The first 90 days set whether the program ever reaches that compounding effect.
The sequence below is the diagnostic-to-deployment path we run with new treatment center operator engagements. Most operators find the most consequential gap inside the first 30 days, and the next 60 days are about closing it without breaking the rest of the program.
Days 1 to 30: diagnose what is actually running
Audit the current pillar allocation against the framework in this guide. Where are the gaps? Which pillars are running on auto-pilot? Which are not running at all?
Check compliance status: LegitScript certification active and current, HIPAA-safe tracking in place, FTC-defensible creative across all paid surfaces, state advertising compliance verified for each service geography.
Pull the current cost-per-admit number by channel. If marketing reports stop at cost-per-lead and do not tie to admissions, that gap is the most consequential one to close first. Reporting is upstream of every other improvement.
Days 31 to 60: decide the strategic shape
Confirm the right tier for the program based on facility scale, payer mix, and category position. Adjust spend level and pillar allocation against that tier’s benchmark.
Decide the operating model: in-house, agency, or hybrid. If agency or hybrid, evaluate current partners against the Client Brain operating system standard. Most operators find agency selection is the single most consequential move available.
Name the owner of the reporting framework. Marketing-to-admissions attribution is what makes the program defensible at the C-suite level, and it has to have a single internal accountable owner.
Days 61 to 90: deploy the foundation
Stand up the compliance and tracking foundation if it is not already in place. Restart paid programs against the new campaign architecture. Begin the content publishing cadence that produces SEO and AEO compounding over the next 12 to 18 months.
Lock the brand positioning into a one-paragraph articulation every downstream creative asset reflects. Pull documentary alumni storytelling into the production calendar. That single production becomes 12 downstream creative assets.
By day 90 the program is running against the framework. First paid admissions land. First content publishing cycle completes. The 12-to-18-month compounding timeline starts from here.
The cluster hubs underneath this guide go deeper into each pillar at operator-decision depth. The AEO guide documents the seven-layer playbook for AI citation share. The RCM guide documents the six levers of a functioning billing operation. The Client Brain framework documents what to look for in an agency partner.
Behavioral health marketing rewards operators who do the work the category structurally demands. The operators running integrated five-pillar programs in 2026 produce admission volume that paid-only competitors cannot afford to match. The 90-day sequence above is where that work starts.
Most in-house teams hit a wall not because they lack knowledge, but because they lack bandwidth.
When you are ready to hand it off, Webserv has spent 9 years executing exactly this for treatment centers nationwide.
Preston Powell is the CEO of Webserv, a digital marketing agency for behavioral health treatment centers.