A 60-bed residential treatment center asked me to evaluate why their content program had stalled after producing 200 blog posts over two years. The agency had been writing on whatever topic came up in the weekly meeting.
The keyword strategy was a one-line Google Sheet from 2023 that nobody had revisited. There was no map of which queries the cluster covered and which it did not.
I ran a gap analysis and surfaced 47 specific high-priority queries the site should have been ranking for but had no content addressing. Some were commercial gaps (no page on “MAT in [city]” despite the facility offering it).
Some were informational gaps (no pillar on dual diagnosis even though half the admissions involved co-occurring disorders). Some were AEO gaps (existing content too vague to get cited inside AI Mode for specific clinical sub-queries).
The remediation took 6 months. Of the 47 gaps, the team built content for 28 of them, expanded 12 existing pages to close partial gaps, and intentionally skipped 7 as not worth the investment.
Organic admission inquiries grew 41 percent year over year, with most of the lift attributable to the gap closures rather than to broader site optimization. The 200 existing posts continued to underperform. The 28 new pieces produced 60 percent of the new admissions from organic.
The content strategy had been working harder than it needed to because it was working without a map. That pattern is the norm in behavioral health authority content programs.
Most treatment centers publish without a systematic view of what the cluster should cover, which means most operators have 30 to 60 percent of their potential admission-producing content unbuilt. A real content gap analysis surfaces the missing pieces and prioritizes them by admission-economics impact.
This piece covers how to run one for a treatment center site in 2026. The framework is what our authority content practice applies on every new client engagement, and the structure scales from single-location residential operators to multi-location systems.
Key Takeaways
- A content gap analysis maps what your cluster should cover against what your cluster currently covers. For most BH operators, the gap is 30 to 60 percent of the addressable content space.
- Five dimensions of gap matter for behavioral health: commercial intent, informational intent, clinical specialty, geographic, and AEO/passage-level. Most operators only analyze one or two.
- Gap sourcing comes from five places: keyword research tools, competitor content analysis, AI citation prompt audits, intake CRM data, and the FAQ stream from admissions and clinical teams.
- Prioritization should weight admission-economics impact above traffic or ranking metrics. A 200-monthly-search query that produces 6 admissions a year matters more than a 5,000-search query that produces none.
- The right output is a prioritized 90-day to 12-month roadmap with each gap mapped to a specific content type (pillar, micro, service page, FAQ block, expansion of existing content) and a clinician contributor.
What a content gap analysis actually is
The conventional framing of “content gap analysis” is “look at the topics you have not covered yet.” That framing is too narrow to produce a useful output for behavioral health.
A real content gap analysis maps the cluster’s addressable space against what the site currently covers, and identifies where the gaps cluster. The addressable space includes every commercial query, every informational query, every clinical specialty, every geography, and every AEO sub-query the operator could rank or be cited for.
Google Search Central’s guidance on creating helpful, reliable, people-first content explicitly frames topical coverage as a primary input to ranking and citation eligibility, which is why the gap-mapping work matters in 2026.
The output is a prioritized list with admission-economics impact estimates, not just a list of missing topics.
The five dimensions of gap that matter for BH:

Commercial intent gap. Queries with direct admission-purchase intent that the site does not cover. “[City] residential rehab,” “[insurance] PHP near me,” “alcohol detox accepting Aetna” type queries. These are the highest-economics gaps because the buyer is already in the funnel.
Informational intent gap. Educational and research-stage queries the buyer asks before commercial queries. “Difference between PHP and IOP,” “what to expect in residential treatment,” “how to support a family member in recovery.” These feed the commercial layer through internal linking and brand authority.
Clinical specialty gap. Topical authority gaps tied to the facility’s actual clinical offerings. A facility that treats dual diagnosis but has no dual-diagnosis content has a clinical specialty gap. The retrieval layer cannot recognize the facility as a topical authority on a service they actually offer.
Geographic gap. Location pages, modality pages, and geographic informational content for the markets the facility serves. A multi-location operator with 5 facilities and 2 location pages has a geographic gap. The local SEO work depends on closing these.
AEO/passage gap. Sub-queries inside AI Mode fan-out that the existing content does not answer at the passage level. The page may rank organically on the head query but get fragmented citation (or no citation) inside AI answers because specific passages are missing. This is the newest gap dimension and the least frequently analyzed.
Most BH operators only analyze one or two of these dimensions (usually commercial and informational). The full five-dimension analysis surfaces gaps the partial analyses miss.
How to source the gaps
Gap sourcing comes from five places. The right analysis pulls from all five and triangulates.
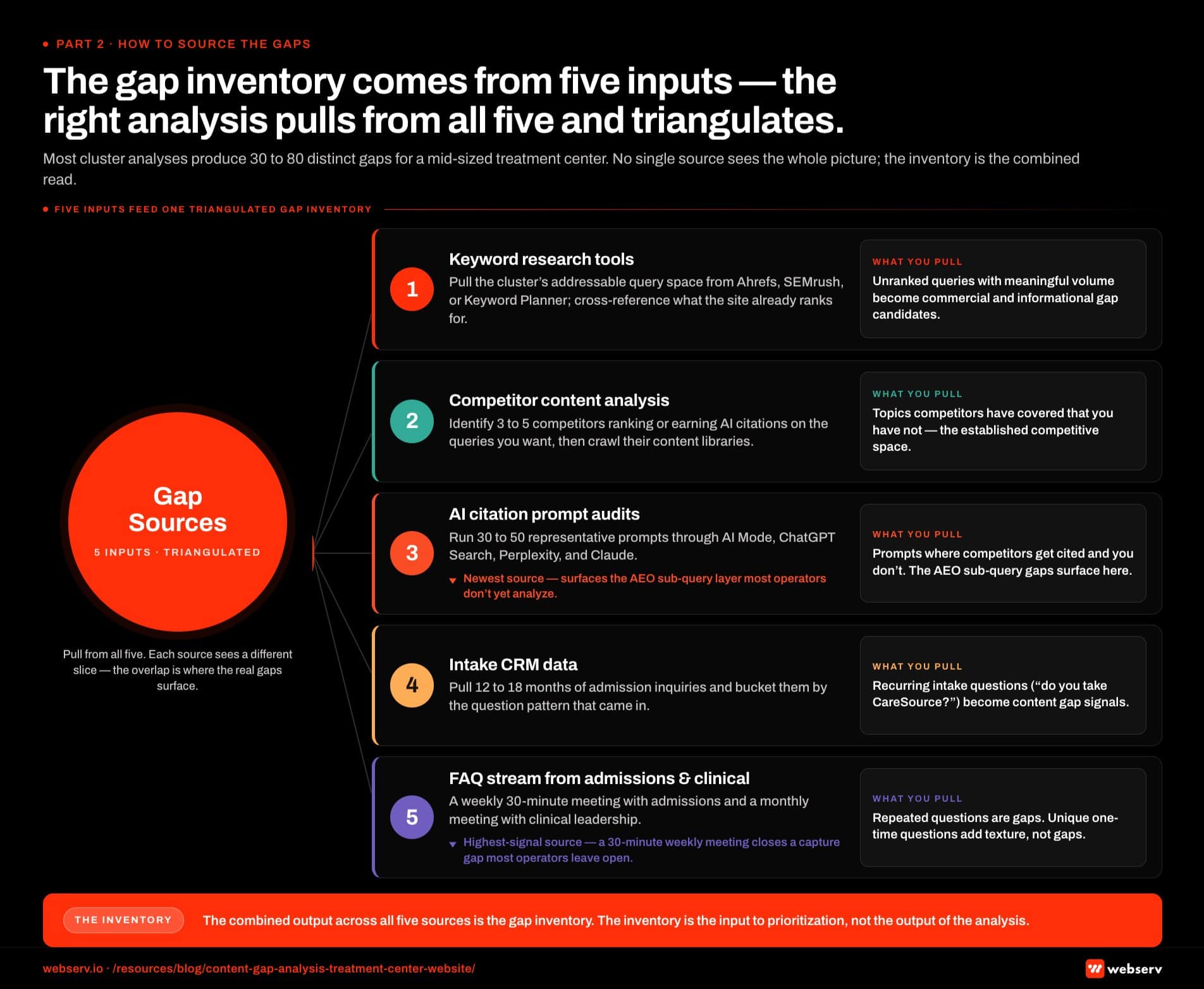
Keyword research tools. Pull the cluster’s addressable query space from Ahrefs, SEMrush, or Google Keyword Planner. Filter by relevance to the facility’s actual offerings. Cross-reference against what the site already ranks for. The unranked queries with meaningful volume are commercial and informational gap candidates.
The keyword strategy work for behavioral health covers the specific filters that work for this category.
Competitor content analysis. Identify 3 to 5 competitor sites that rank or earn AI citations on queries you want to compete for. Crawl their content libraries. Identify topics they have covered that you have not. The competitors’ coverage maps to gaps in your coverage because the competitive content space is already established.
AI citation prompt audits. Pull 30 to 50 representative prompts in the cluster and check AI Mode, ChatGPT Search, Perplexity, and Claude responses. Identify which competitors get cited and on which prompts your content does not appear. The gap surfaces as “competitors cited on prompt X where we have no content that could answer the sub-queries the prompt generates.”
Intake CRM data. Pull 12 to 18 months of admission inquiries and bucket them by the question pattern that came in. The intake team is hearing questions like “do you take CareSource?” or “do you treat methadone-assisted patients?” or “is your facility veteran-friendly?” Each recurring question is a content gap signal because the buyer is asking it before they could find an answer on the site.
The FAQ stream from clinical and admissions teams. A weekly 30-minute meeting with the admissions team and a monthly meeting with clinical leadership surfaces the questions families are actually asking. The recurring questions that get repeated answers are content gaps. The unique questions that come up once are not gaps but provide texture for existing content.
The combined output across all five sources is the gap inventory. Most cluster analyses produce 30 to 80 distinct gaps for a mid-sized treatment center. The inventory is the input to prioritization, not the output of the analysis.
How to score and prioritize the gaps
Not every gap is worth closing. The right prioritization weights admission-economics impact above ranking or traffic potential, with three specific scoring inputs.

Admission-economics estimate. For each gap, estimate the realistic admission count per year the content could produce. A commercial-intent gap on “[city] residential rehab” where the facility’s residential program runs $30,000 in revenue per admission and the search volume supports 2 to 4 admissions a year scores higher than an informational gap with 5,000 searches but no admission attribution.
The math is conservative: assume 0.5 to 2 percent of organic traffic converts to inquiry and 10 to 20 percent of inquiries convert to admission. The product is the annual admission estimate.
Production cost. Pillar content with clinician quotes runs 8 to 15 hours per piece. Service page or location page work runs 6 to 12 hours. FAQ block expansions run 1 to 3 hours. Cost-per-piece varies by content type. The prioritization should account for which gaps are cheap to close and which require deeper production.
Strategic fit. Some gaps fit cleanly into the cluster’s strategic direction (the facility is expanding into a new modality, the operator is preparing for a regulatory shift, the program is repositioning toward a different payer mix). Strategic-fit gaps deserve weighting beyond pure admission-economics math.
The combined score (admission economics × strategic fit ÷ production cost) ranks the gaps. The top 15 to 25 gaps in the ranking become the 90-day to 12-month roadmap. The bottom 30 to 50 gaps get archived or scheduled for later cycles.
The mistake most operators make is treating all gaps as equal. The right framing is that 80 percent of the admission lift comes from closing 20 percent of the gaps. Finding the right 20 percent is what the prioritization does.
“A 200-monthly-search query that produces 6 admissions a year matters more than a 5,000-search query that produces none.”
Preston Powell, Chief Executive Officer, Webserv
Turning the gap into a roadmap
A prioritized gap list is not yet a roadmap. The roadmap maps each gap to a specific content type, a specific clinician contributor, a specific publication window, and a specific success metric.
Content type mapping. Each gap should resolve to one of five content types:
- Pillar piece (3,000 to 5,000 words, cluster authority anchor)
- Micro thought leadership (1,800 to 3,000 words, supporting depth on a sub-topic)
- Service page or location page (1,200 to 2,500 words, commercial conversion surface)
- FAQ block expansion (4 to 6 question-answer pairs added to existing pages)
- Existing-piece expansion (extending an underperforming existing piece to cover the gap)
The mapping matters because different content types have different production economics and different cluster roles. A gap that maps to a pillar costs more to close than a gap that maps to a FAQ expansion.
Clinician assignment. Each gap should map to a credentialed clinical contributor who will provide the quotes, review the draft, and carry the byline. The author bio infrastructure work means each clinical contributor has an established E-E-A-T profile. The gap assignment uses that infrastructure.
A clinician with 3 published bylines on dual diagnosis content is the right assignee for the dual-diagnosis pillar gap.
Publication window. Gaps should be sequenced across the roadmap in batches. The first 90 days should close 6 to 10 of the highest-economics gaps. The 90 to 180 day window closes another 6 to 10. The 180 to 365 day window closes 8 to 15 more. The full roadmap usually runs 12 to 18 months to close the top 25 to 35 gaps from the inventory.
Success metrics. Each gap should have an attached success metric tied to admission economics, not just traffic or ranking. A pillar gap might have “10 admission inquiries attributable to the page within 9 months” as its success metric. A FAQ expansion might have “AI Mode citation rate on the parent topic prompts up 25 percent in 90 days.” The metric makes the gap closure measurable.
How SoCal Sunrise generated 85 admissions and 2,297% ROI from SEO in 6 months
A ground-up SEO rebuild using the Pathfinder Parents Methodology turned an invisible online presence into a top-ranking admissions engine.
Read the case study →85 admits and 3,152 leads attributed to organic
Common mistakes in BH content gap analyses
MOST COMMON MISUNDERSTANDING
Conflating traffic potential with admission potential. A gap at 8,000 monthly searches that produces one admit a year is a worse gap to close than a gap at 200 searches that produces four. Most agencies prioritize on traffic because it is the easier axis to sell. The right axis is verified admits. Second failure: skipping the clinical-specialty dimension. Gap analyses that only look at commercial and informational queries miss the topical authority work the facility's actual clinical offerings demand — dual diagnosis, co-occurring trauma, MAT-eligible populations.
Six mistakes account for most of the underperformance I see when operators have attempted gap analyses on their own.
Conflating traffic potential with admission potential. A gap with 8,000 monthly searches that produces 1 admission a year is a worse gap to close than a gap with 200 monthly searches that produces 4 admissions a year. Most agencies prioritize on traffic. The right prioritization is on admissions.
Skipping the clinical specialty dimension. Gap analyses that only look at commercial and informational queries miss the topical authority work the facility’s actual clinical offerings demand. A facility treating dual diagnosis without dual-diagnosis pillar content is leaving authority on the table even on queries the facility already ranks for.
Missing the AEO sub-query layer. The fan-out query architecture in AI search creates sub-query gaps inside existing content. A page that ranks organically for “what is residential treatment” may get fragmented citation in AI Mode because specific clinical sub-queries (admission criteria, length of stay norms, family involvement protocols) are not answered at the passage level. The gap analysis has to look inside the content, not just at the topic level.
Treating the analysis as a one-time exercise. Gaps emerge continuously as Google updates the algorithm, AI search models shift the citation patterns, the facility expands services, and the competitive set evolves. The right cadence is a full re-analysis every 6 months with monthly adjustments to the active roadmap.
Ignoring the geographic dimension for residential. Multi-location operators with 5 facilities and 2 location pages are losing geographic visibility on 3 markets. Even single-location residential operators benefit from market-specific content (the surrounding metro, the regional treatment market, the local recovery community) that produces local trust signals.
Closing gaps without the clinician layer. Gaps closed with anonymous bylines or AI-generated content produce the same authority problem that drove the gap analysis in the first place. The closure has to include credentialed clinical attribution and the Person schema deployment that powers AI citation eligibility.
The cumulative cost of these six mistakes is usually 40 to 60 percent of the lift the analysis could have produced. Operators who run the analysis correctly and close the gaps systematically produce the kind of admission growth the opening case study showed.
How the analysis fits into the broader content program
A content gap analysis is one input to the broader content strategy and architecture. The gap inventory drives the roadmap. The roadmap drives production scheduling. The production produces the pieces that close the gaps.
The adjacent layers that matter:
Editorial calendar. The gap roadmap maps to specific publication windows. The editorial calendar manages the production sequence, the clinician availability, the healthcare blog and article writing standards, and the publishing cadence.
Refresh cycle. Existing pieces flagged for expansion (rather than archival) feed back into the refresh cadence. Pieces being expanded to close adjacent gaps need updated dates, updated clinician sign-offs, and updated entity schema. Underperforming farm-content pieces or templated city pages that are not worth saving should be 301-redirected to the closest relevant new piece, the same logic that governs doorway pages cleanup.
Cluster linking. Every closed gap should fit into the existing cluster’s internal linking architecture. A new pillar piece needs the supporting micros that reference it. The existing micros need to link to the new pillar. The healthcare content creation framework covers the linking discipline.
Measurement. The success metrics attached to each closed gap roll up into program-level measurement. The aggregate admission impact across all closed gaps over 12 months is the program’s ROI metric.
The combined view treats the gap analysis as an input to a working content program, not as a standalone exercise. Operators who run the analysis but do not integrate it into the broader behavioral health marketing program produce a list of gaps that never get closed.
Frequently Asked Questions
How long does a content gap analysis take?
For a single-location treatment center with 100 to 300 published pieces, a full gap analysis takes 20 to 40 hours of analyst work spread over 2 to 4 weeks. The analyst time covers keyword research, competitor content audit, AI prompt testing, CRM data pulls, and prioritization scoring. Multi-location operators or operators with multiple service lines take 40 to 80 hours.
The output is the gap inventory plus the prioritized 12-month roadmap. The roadmap is then handed to the content team for production, which runs separately from the analysis time.
Most operators benefit from a full re-analysis every 6 months and lighter monthly check-ins on the active roadmap. Continuous monitoring is overkill for most BH operators because the gaps do not shift fast enough to justify weekly attention.
What tools do we need to run this analysis?
The minimum tool stack is a keyword research platform (Ahrefs, SEMrush, or Moz at the small-budget end), a competitor crawler (Screaming Frog or equivalent), and a CRM that captures inquiry source attribution. Most BH operators already have these tools or can subscribe for $300 to $800 a month.
The optional additions for the AEO dimension are AI citation tracking tools, which are still maturing in 2026. Platforms like Otterly, Profound, or LLM Tracker provide partial visibility into AI Mode and ChatGPT Search citations. The data is imperfect but better than guessing.
The most underused tool in this analysis is direct conversation with the admissions and clinical teams. The recurring questions they hear are the highest-signal gaps available, and most operators do not have a systematic way to capture them.
How do we know if a gap is worth closing?
The economics test is the most reliable filter. If the gap can realistically produce 3 to 6 admission inquiries a year (at the facility’s specific intake-to-admission rate), and the production cost is 8 to 20 hours of content team time plus 2 to 4 hours of clinician time, the gap is worth closing. The payback on a single admission usually justifies the production investment many times over.
Gaps that produce less than 1 to 2 admission inquiries a year are usually not worth closing even if the search volume looks reasonable, because the unit economics do not support the production cost. These gaps should be archived or grouped with adjacent gaps to produce a single piece that addresses multiple low-volume queries.
The exception is strategic-fit gaps. A facility expanding into a new clinical specialty or a new market may need to close the content gaps in that space even if the immediate admission economics are weak, because the strategic positioning depends on the topical authority being established before the admissions volume develops.
Can we use AI tools to run this analysis?
Partially. AI tools (ChatGPT, Claude, Perplexity) are useful for surfacing competitor content, summarizing competitor coverage, generating initial keyword expansion lists, and helping draft the gap inventory documentation. They are less useful for the admission-economics scoring and the strategic-fit weighting because those require operator-specific judgment.
The right pattern is to use AI tools for the high-volume, low-judgment parts of the analysis (keyword expansion, competitor content scanning, basic gap identification) and reserve the operator-specific judgment work for the human analyst. Running the entire analysis through AI tools produces gap lists that look reasonable but miss the strategic context that makes the prioritization work.
The AI citation prompt audit specifically is a place where AI tools are essential, since you are testing how the AI engines themselves respond to representative prompts. Use them as the test instrument, not as the analyst.
How does the gap analysis interact with our existing keyword strategy?
The keyword strategy provides the input to the commercial and informational gap dimensions. The keyword strategy framework for treatment centers covers the cluster taxonomy and the search-intent mapping that feeds into the gap analysis. Operators with mature keyword strategy work in place can run the gap analysis as a focused next step. Operators without it should run the keyword strategy first and the gap analysis after.
The relationship is that the keyword strategy defines the addressable space and the gap analysis maps coverage against it. The two artifacts are complementary. Neither substitutes for the other.
The long-tail keyword work within the keyword strategy also matters for the AEO sub-query dimension of the gap analysis. AI search rewards content that answers long-tail sub-queries cleanly, and the gap analysis surfaces the long-tail patterns the existing content does not yet cover.
What is the first step we should take after reading this?
Pull 12 months of admission inquiries from the CRM and bucket them by source query (organic search, paid search, direct, social). Look at the organic admissions and the URLs they landed on. This baseline tells you which existing content is actually producing admissions, which is the input to the rest of the analysis.
The next step is to map the facility’s actual service lines, levels of care, clinical specialties, payer relationships, and geographic markets. Each combination represents a cluster element. The gap analysis then maps the cluster elements against existing content coverage and surfaces the gaps systematically.
The first full analysis usually takes 3 to 5 weeks for a treatment center starting from scratch. By month 2, the roadmap is ready and production can start. By month 6, the first batch of closed gaps starts producing measurable admission contribution. The compound effect builds through month 18 and continues if the analysis is refreshed on cadence.
The perspective in this article comes from 9 years working exclusively inside behavioral health.
We are a team built by people in recovery who understand that behind every admission is someone asking for help. If that resonates, get to know us.
Trevor Gage is the Director of Earned & Owned Media at Webserv, where he leads SEO, content strategy, and organic acquisition for behavioral health treatment centers. He has overseen audits of more than 200 behavioral health sites and writes about the technical and editorial SEO standards Webserv applies to client work.