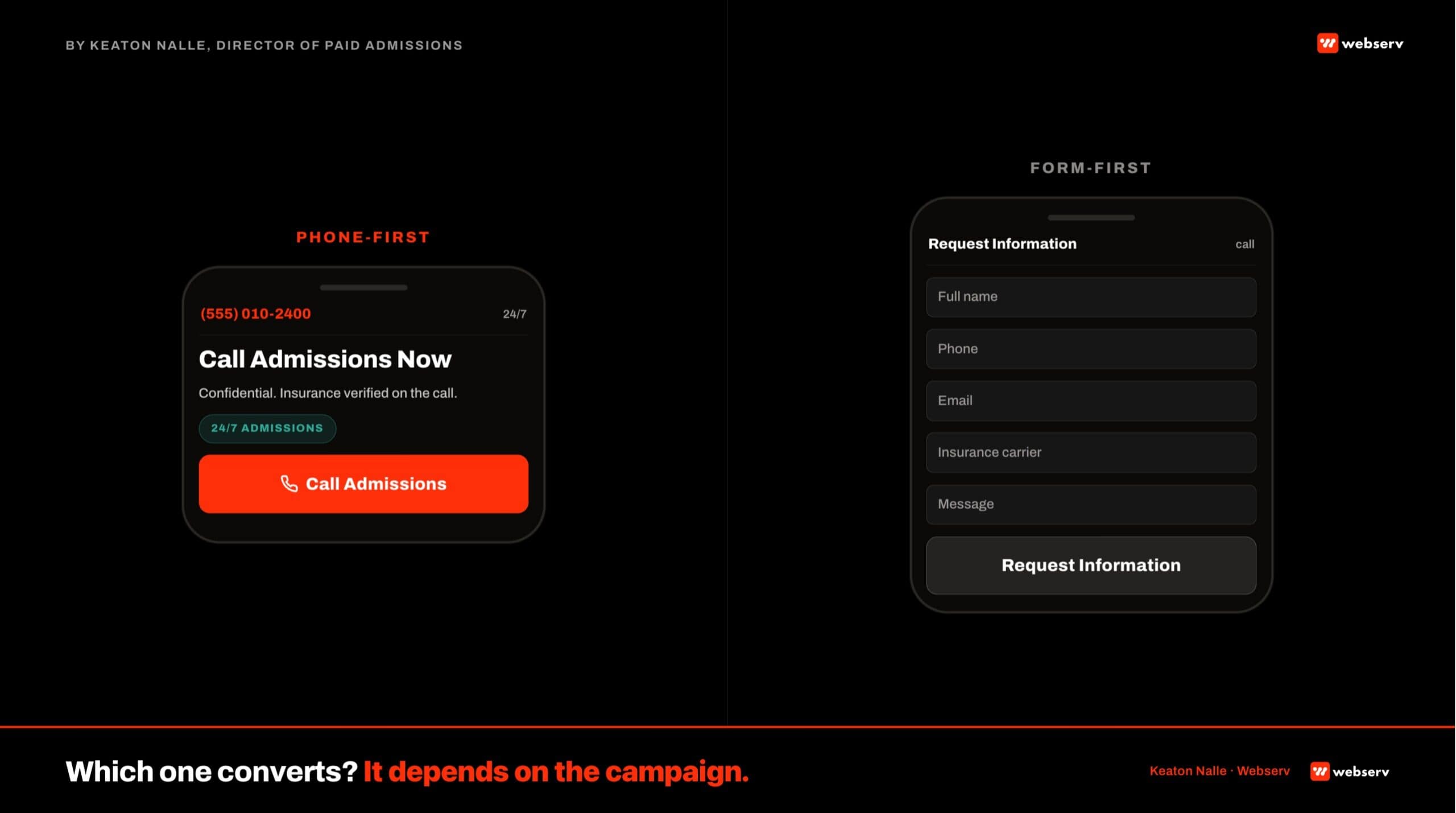
Most treatment center paid landing pages ship form-first by default. The form sits above the fold, four to six fields, phone number tucked into the header as a secondary option.
This is the pattern the marketing team inherits from B2B SaaS, from the paid CRO agency they used before, from the LP builder templates that ship with form-first defaults.
For behavioral health, that default is often wrong. Prospects and families calling a treatment center are not filling out a demo request form.
They are in an urgent moment, they want to hear a voice, and they will choose the facility that answered over the facility that made them wait for a callback.
Our team manages $1M+ per month in paid media across behavioral health accounts. The phone-first versus form-first decision on the landing page turns out to be one of the biggest conversion inputs we adjust, campaign by campaign, inside our paid CRO program at Webserv.
This article walks the framework we use to decide phone-first, form-first, or a hybrid pattern on paid conversion rate optimization landing pages for treatment centers.
It also covers how the noindex-for-paid-LP standard changes what you can put on the page and how aggressive the CTA can be without hurting the main site’s organic signal.
Key Takeaways
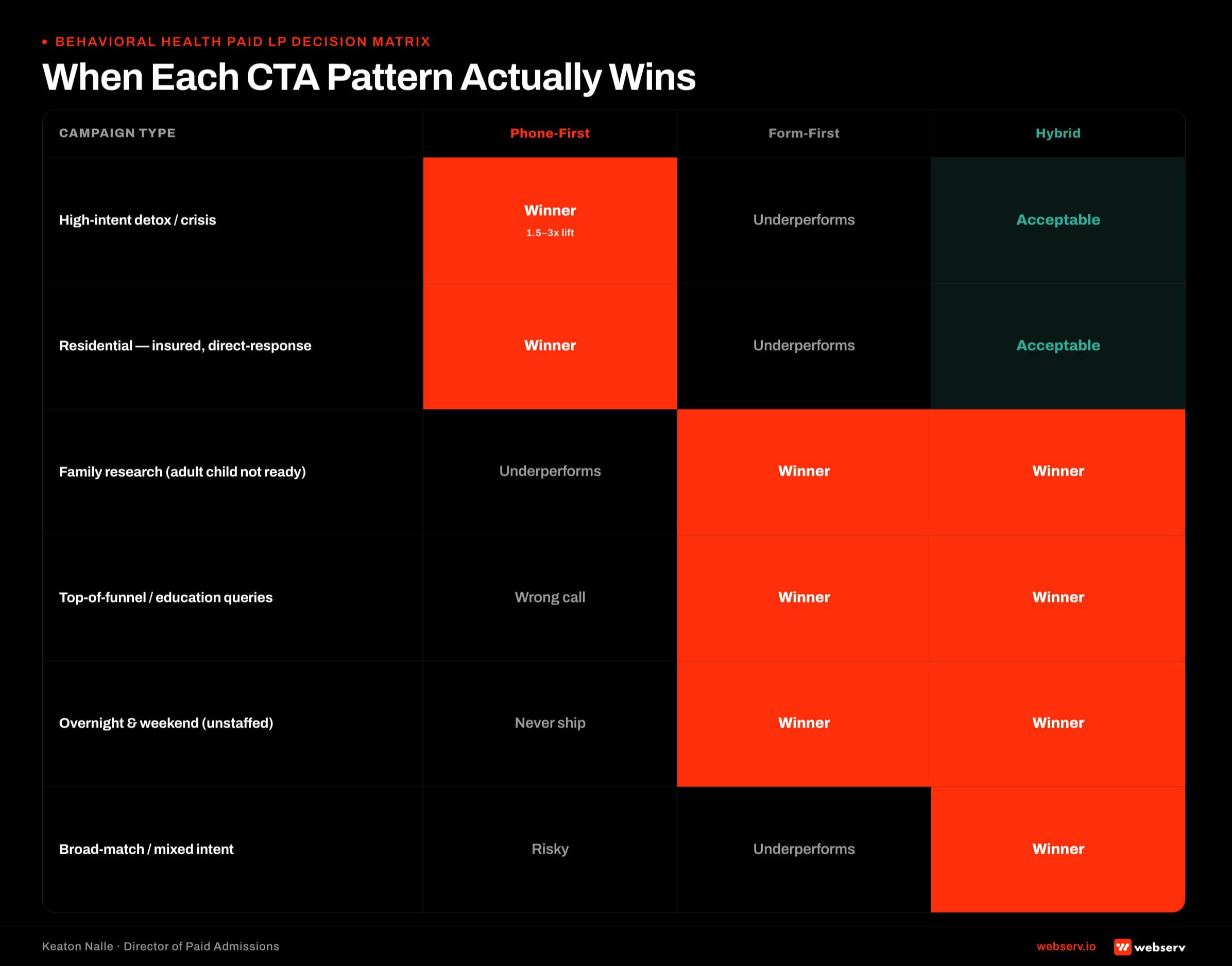
- Most treatment center paid landing pages ship form-first because that is the default in LP builder templates and in B2B CRO practice. For behavioral health specifically, form-first is often the wrong call. Phone-first converts better on high-intent detox, residential, and crisis campaigns because the caller wants to hear a voice inside 30 seconds, not fill out a form.
- Phone-first only works if the admissions team is actually staffed to answer inside 30 seconds during the campaign’s traffic windows. Phone-first with a voicemail catch is worse than form-first with an automated confirmation. Coverage is the load-bearing variable.
- Form-first wins on family-research campaigns, on overnight and weekend traffic when phone coverage is limited, and on lower-intent top-of-funnel campaigns where the prospect wants materials before a live conversation.
- The hybrid pattern outperforms both defaults for most treatment centers. Phone number always visible in the header and a fixed footer bar, secondary form for prospects who prefer not to call. This captures both intent types without forcing the wrong CTA on either.
- Paid landing pages for treatment centers are typically noindexed so the main site’s E-E-A-T signal is not diluted by aggressive paid CRO tactics. That noindex changes what you can put on the page (more aggressive CTAs, less clinical depth, tighter compliance-adjacent messaging) without hurting the organic footprint.
- Measurement discipline is where phone versus form gets decided honestly. Not lead volume. Viable VOB rate, cost per admit, and downstream conversion by CTA type. A phone-first LP that produces 30 percent fewer leads but a viable VOB rate two-and-a-half times higher is the better LP.
The Default: Why Most Treatment Centers Ship Form-First
DEFINITION
Form-First Landing Page
A paid landing page where the primary conversion CTA is a lead-capture form, typically 3 to 8 fields, placed above the fold. The phone number appears secondary, either in the header or in a click-to-call element on mobile. Most B2B SaaS landing pages, most consumer lead-gen templates, and most default LP builder templates ship form-first. The pattern reflects sales-industry inheritance more than behavioral health-specific evidence.
Form-first is the default for three reasons that have nothing to do with what actually converts for treatment centers.
The first is inheritance. Marketing teams and agencies use the same landing page frameworks across categories, and the B2B SaaS category (where form-first is correct) trained an entire generation of marketers to treat the form as the primary conversion.
That training carries into behavioral health engagements even though the prospect behavior is different.
The second is trackability. Forms produce clean structured data (name, email, phone, insurance) that fills a CRM record automatically. Phone calls produce recordings and duration metrics but require call-tracking integration to populate the CRM at the same clean level. Google Ads documents the offline conversion pipeline that connects call data to admit attribution.
Marketing teams pick the option that produces cleaner analytics, not the option that produces more admits.
The third is fear of missed calls. Operators who have seen their admissions team miss inbound calls in the past worry that phone-first landing pages will overwhelm the team and produce miss rates that undermine the campaign.
This concern is legitimate. It also has a solution (real staffing coverage) that is cheaper than the alternative of accepting lower conversion.
When Phone-First Actually Wins
DEFINITION
Phone-First Landing Page
A paid landing page where the primary conversion CTA is a click-to-call phone number, displayed prominently above the fold with a clear supporting benefit statement. Secondary elements (form, chat, informational content) sit below the primary CTA. Requires admissions team coverage during the campaign’s traffic windows and clean call tracking integration for attribution. In behavioral health, phone-first often outperforms form-first on high-intent detox, residential, and crisis campaigns.
Phone-first landing pages produce materially higher conversion on specific campaign types.
1.5-3x
typical conversion lift on phone-first LPs for high-intent detox and crisis campaigns
30 sec
answer-time threshold for phone-first LPs to work
60-80%
share of BH admissions inquiries that come from family members, not the patient
High-intent detox campaigns. A prospect searching “detox help today” or “medical detox now” is in a moment where a form fill feels like the wrong friction. They want to hear a professional voice inside 30 seconds.
Phone-first LPs on these campaigns often convert 1.5 to 3 times the equivalent form-first LP.
Crisis-adjacent campaigns. Same dynamic. When the query language signals urgency, phone-first wins.
Family caller research. A family member calling on behalf of a loved one usually wants to hear a voice more than fill out a form. Families make roughly 60 to 80 percent of behavioral health admissions inquiries, so the family-caller preference is a majority use case for many treatment centers.
Small treatment centers with dedicated admissions coverage. A center running one or two admissions coordinators who answer every call inside 30 seconds gets more out of phone-first than a larger operation whose call routing is more complex.
PHONE-FIRST ONLY WORKS IF YOU ACTUALLY ANSWER THE PHONE
A phone-first landing page that routes to voicemail during peak paid traffic hours is worse than a form-first LP with an automated confirmation. The math flips completely: missed calls at $200-$400 cost per click are pure waste, while an automated form confirmation at least gives you the chance to follow up. If your admissions team is not staffed for the campaign’s traffic pattern, do not ship phone-first. Fix the staffing first.
When Form-First Actually Wins
Form-first is the right call in specific scenarios.
Overnight and weekend traffic without staffed phone coverage. If the admissions team is not answering the phone at 2 AM on a Sunday, phone-first is a losing pattern for that traffic window. Form-first with an automated confirmation catches the lead for callback during staffed hours.
Family research campaigns. Some family caller segments actually prefer to submit a form. Parents researching for adult children who are not yet ready to accept treatment often want to fill out an information request first, then evaluate materials before calling. Form-first LPs converting family research campaigns land at reasonable rates.
Lower-intent top-of-funnel campaigns. A prospect searching “signs of alcoholism” or “what is IOP” is in a research phase. Phone-first on these campaigns is premature. Form-first with an educational nurture sequence often works better.
High-volume broad-match campaigns. When targeting is looser and lead quality is more variable, form-first lets the admissions team filter before a phone conversation, protecting coordinator time.
The Hybrid: Progressive Disclosure
THE PATTERN THAT OUTPERFORMS BOTH DEFAULTS FOR MOST TREATMENT CENTERS IS A HYBRID
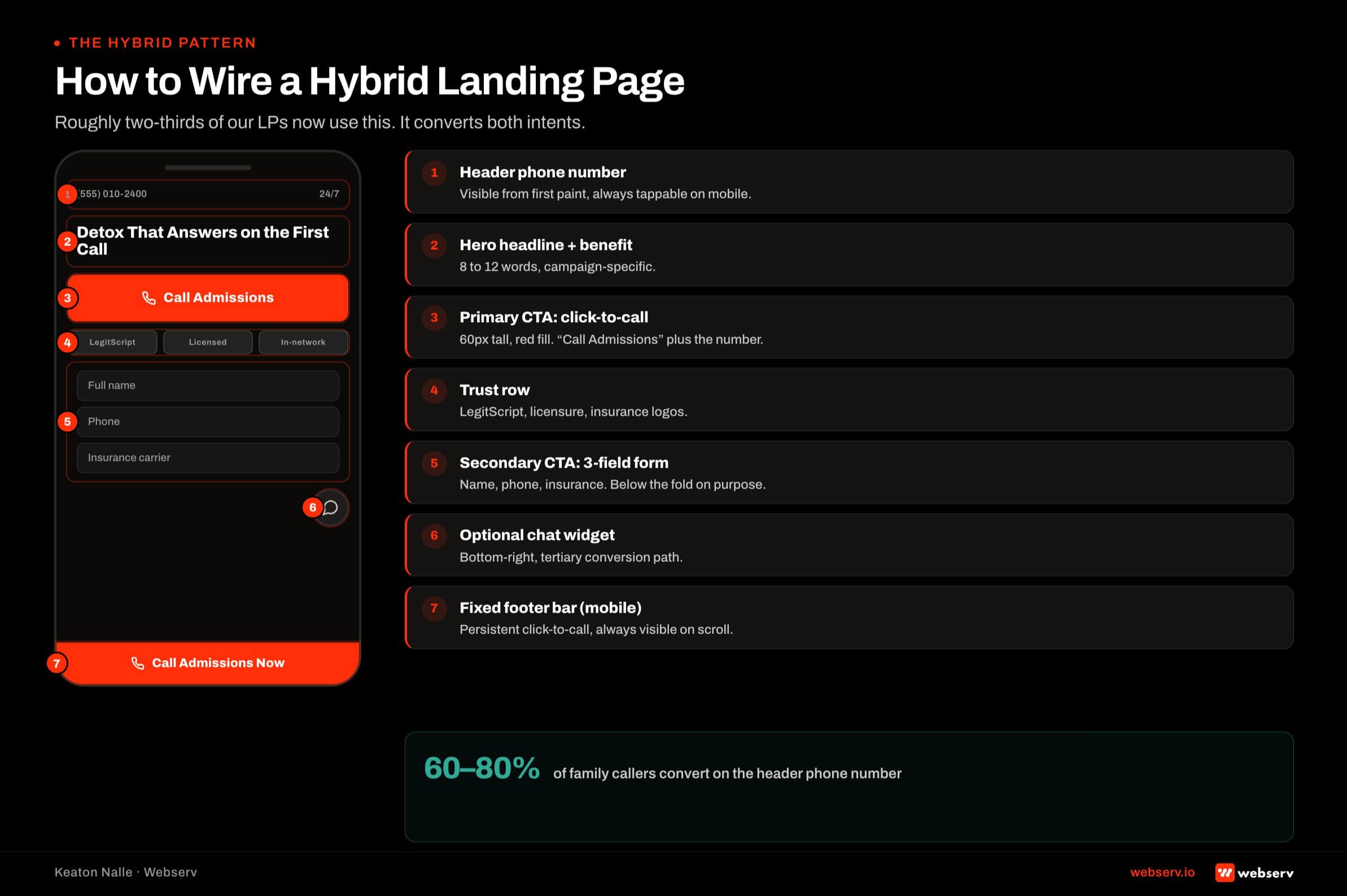
Phone number visible in the header and a fixed footer bar on mobile, always available for the prospect who wants to call. Form present as a secondary conversion for prospects who prefer not to call. Optional chat as a tertiary. This captures both the phone-inclined and the form-inclined prospects without forcing the wrong CTA on either. Roughly two-thirds of treatment center paid LPs we manage now use this hybrid pattern.
The hybrid math looks like this. High-intent, urgent prospects call. Lower-intent, research-mode prospects fill out the form. The LP does not pick one CTA to enforce; it offers both, and the prospect self-selects based on their state.
The measurement side matters. Track conversions by CTA type. On a well-designed hybrid, phone conversions typically outnumber form conversions on high-intent campaigns by 2 to 4x, and form conversions typically outnumber phone conversions on family-research campaigns by similar margins.
If your hybrid is not producing that intent-based split, the LP is not doing the work.
The Noindex Reality
DEFINITION
Noindex Paid Landing Page
A landing page that is deployed to serve paid traffic only, tagged with a noindex meta directive that prevents Google from indexing the page for organic search results. The noindex standard is common practice for treatment center paid media because it keeps the main site’s E-E-A-T signal clean while allowing more aggressive paid CRO tactics (stronger CTAs, tighter compliance-adjacent messaging, single-page focus) that would not fit the treatment center’s organic content strategy.
Webserv’s default posture on paid landing pages for treatment centers is noindex. The main site handles the organic experience with clinical depth, named authorship, E-E-A-T signaling, and full compliance-reviewed content.
The paid landing pages handle the paid experience with tighter focus, direct conversion, and creative that would not fit the organic site’s editorial standard.
This split matters for the phone versus form conversation in three ways:
First, the paid LP can use aggressive urgency framing (visible phone number, immediate-availability messaging, direct-response calls to action) that would not sit well on the main site’s clinical education content. Noindex lets that aggressive framing exist without polluting the organic footprint.
Second, the paid LP is optimized for one thing: converting a paid click into a lead or call.
It does not need to serve organic search intent, does not need to rank for queries, and does not need to compete with the main site’s SEO content. Focus is tighter, structure is simpler.
Third, the paid LP can iterate faster than the main site. A/B testing on a noindexed paid LP does not risk the main site’s ranking signal. New versions can ship weekly. Winners can be scaled aggressively. Losers can be killed.
The compliance layer still applies. LegitScript certification for addiction treatment advertisers, Meta family-first standards, 42 CFR Part 2, and FTC endorsement guidelines all constrain what can appear on the paid LP, exactly the same way they constrain the main site. Noindex is a search-visibility choice, not a compliance choice.
The 5-Step Decision Framework
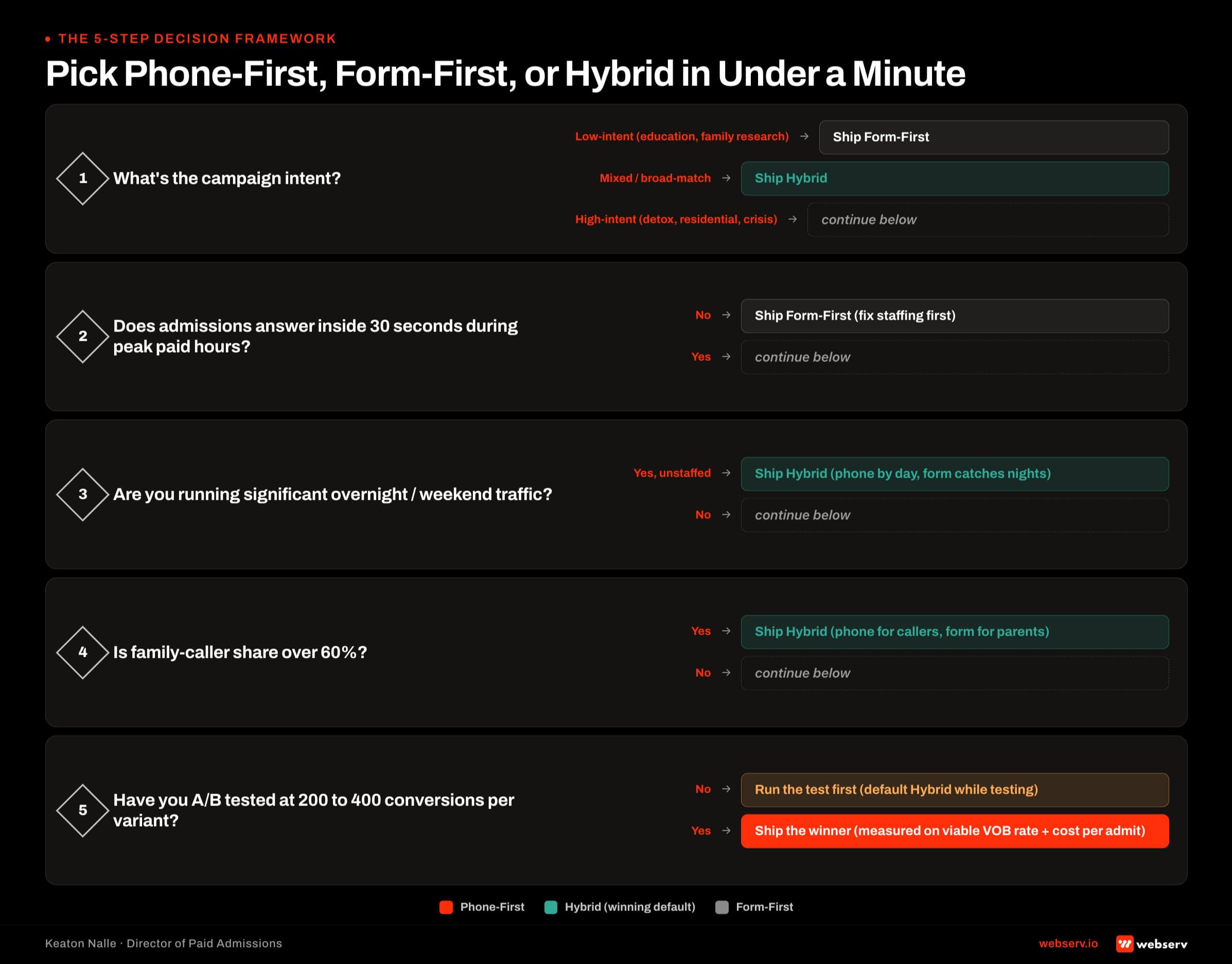
- Segment by Intent Level. Look at the query set the campaign is targeting. High-intent detox, residential, and crisis queries lean phone-first. Family research, condition education, and top-of-funnel queries lean form-first. Broad-match campaigns should almost always use the hybrid pattern.
- Check Admissions Coverage. Map the campaign’s traffic patterns against your admissions team’s actual answer-inside-30-seconds capacity. If you cannot answer during peak paid hours, phone-first is a losing pattern regardless of intent. Fix the staffing first or ship form-first.
- Test Both Against Real Traffic. Run a real A/B test. Split traffic 50/50 for at least 200-400 conversions per variant so the results are statistically defensible. Do not decide based on opinion or on what the LP builder template defaulted to.
- Measure Downstream (Not Lead Volume). The metric that decides phone versus form is viable VOB rate, not lead volume. A phone-first LP producing 30 percent fewer leads at a 2.5x viable VOB rate is a better LP than the form-first winner on volume. Cost per admit is the answer, cost per lead is the noise.
- Segment by Device. Mobile behaves differently than desktop for behavioral health paid traffic. Mobile users are more likely to tap a phone number than fill out a form. Desktop users are more likely to fill out a form. Consider device-specific LP variants when the split is material.
The framework is intentionally simple. Most operators who commit to running it produce measurable conversion improvements inside 60 to 90 days. The failure pattern is skipping steps 3 and 4 (real A/B testing and downstream measurement) and picking based on assumption.
Measurement That Matters
The measurement discipline that separates working paid CRO from opinion-based CRO:
Viable VOB rate by CTA type. For each landing page variant, track what percentage of leads converted to a viable VOB. This is the metric that reveals whether the CTA is producing quality or noise.
Cost per admit by CTA type. The full downstream number. Phone-first and form-first LPs sometimes tie on cost per lead but diverge substantially on cost per admit. The admit is what matters.
Time-to-first-touch. Median time between form submission or missed call and the admissions team making contact. Below 10 minutes is healthy. Above 60 minutes is a leaky funnel that the LP variant cannot fix.
Conversion by device. Mobile-versus-desktop split on each CTA type. Reveals whether one variant is winning on aggregate but losing on a specific device.
Conversion by day-part. Which hours produce phone conversions vs form conversions. Reveals coverage gaps in the admissions team’s staffing pattern.
Every metric above is trackable in a properly configured Google Ads plus call tracking plus CRM stack. Treatment centers that do not have this stack configured cannot honestly answer the phone-versus-form question because the data does not exist to answer it.
What Not to Do
WORKING PAID CRO PATTERNS FOR LP CTA DECISIONS
- A/B test with real traffic for statistically defensible sample sizes (200-400 conversions per variant)
- Measure downstream through viable VOB rate and cost per admit, not just cost per lead
- Ship phone-first only when admissions coverage matches the campaign’s traffic windows
- Ship form-first with 3-5 fields maximum for behavioral health traffic
- Deploy paid LPs as noindexed pages separate from the main organic site
PATTERNS THAT PRODUCE BAD DECISIONS AND WASTED SPEND
- Pick CTA type based on ‘what feels right’ or on last quarter’s opinion
- Optimize for lead volume, then wonder why cost per admit rose
- Ship phone-first LPs that route to voicemail during peak traffic hours
- Ship form-first with 8+ field forms that reduce conversion without adding value
- Compete your paid LPs against your organic content for the same keywords
The most expensive mistake I see across the paid CRO audits our team runs is treatment centers making the phone-versus-form decision once, at the start of the campaign, based on an LP template default.
The decision should be revisited every campaign, based on data, and revisited again when the admissions team’s coverage or the campaign’s target audience changes.
The second most expensive mistake is treating cost per lead as the KPI. Cost per lead is directional; cost per admit is the number that pays for the campaign.
A phone-first LP that produces fewer leads at a higher viable VOB rate is the better LP for the business, even if the marketing dashboard says the form-first variant “won” on lead volume. Our Complete Guide to Conversion Rate Optimization for Rehab Marketing walks the full paid CRO framework that this decision sits inside.
Book an intro meeting if you want to walk your current paid LP setup with our team.
Frequently Asked Questions
Should we use the same phone number for paid LPs as our main site?
No. Paid campaigns should use dedicated tracked numbers so you can attribute admits back to the specific campaign, keyword, or LP variant that produced them. Call tracking platforms like CallRail and CTM provide dynamic number insertion that swaps in the tracked number based on the source of the visitor.
Using the main site’s phone number on paid LPs breaks attribution. Admits get counted as “direct” or “organic” when they actually came from paid. Budget decisions made on that muddled data are usually wrong.
The tracked number should route to the same admissions team as the main site number. The prospect experience does not change. What changes is that the marketing team can see which campaigns produced which admits, which lets them scale winners and cut losers based on real data.
How aggressive can we get with CTA copy on a noindexed paid LP?
Noindex removes the search-visibility constraint but not the compliance constraint. LegitScript, Meta family-first standards, 42 CFR Part 2, and FTC endorsement guidelines apply the same way on paid LPs as on the organic site.
Within those constraints, paid LPs can use more direct-response framing than the organic site typically uses. “Get help now” as a phone-first CTA is fine on a paid LP but would sit awkwardly on the main site’s clinical education content. “Verify your insurance” as a form-first CTA is fine on both.
What is not fine anywhere: outcome guarantees, sensationalized recovery imagery, patient-in-crisis staging, or language that reads as sales pitch about treatment. The compliance floor is the same regardless of index status.
What is the right length for a treatment center paid LP?
Depends on the CTA type. Phone-first LPs are typically shorter (300 to 600 words above the fold, phone number and 3 to 5 trust signals) because the goal is to trigger the call fast. Form-first LPs are typically longer (600 to 1,200 words) because the prospect needs more context before submitting.
The hybrid pattern lands in the middle. Enough content to establish the treatment center’s credibility, not so much that the prospect scrolls past the CTA.
The metric that decides length is not word count. It is scroll depth versus conversion. If most conversions happen before the fold, the below-the-fold content is not doing enough work. If most conversions happen after significant scroll, longer content is working. Track and adjust.
How does the phone-first LP connect to our admissions team’s first 60 seconds?
Directly. The phone-first LP produces the call. What happens in the first 60 seconds of that call determines whether the call becomes an admit. The two decisions (LP CTA and call-handling protocol) work as a system, not as separate levers.
An excellent phone-first LP feeding into a broken first-60-seconds workflow produces high call volume with low viable VOB rate. An excellent first-60-seconds workflow with a form-first LP that produces few calls produces high conversion on the calls that come in but leaves paid budget on the table.
The right combined pattern is a phone-first LP that produces high call volume paired with a trained admissions team running the standardized first-60-seconds protocol. That combination produces the closing rates that turn paid media into admits at benchmark cost per admit.
Keaton Nalle is the Director of Paid Admissions at Webserv, a digital marketing agency for treatment centers.