Running a Google Ads program for a behavioral health treatment center in 2026 is structurally different from running paid search in any other vertical. The category is gated by LegitScript certification, governed by Google’s Healthcare and Medicines policy, and classified alongside self-harm in Google’s enforcement stack. Most operators discover the constraints only after their first account gets disabled.
The fundamentals that follow are the ones that decide whether a Google Ads program produces admits or burns budget: who can advertise, in-network versus out-of-network economics, campaign architecture, bidding strategy and conversion values, HIPAA-safe tracking, budget tiers, the 90-day timeline, and the platform changes through 2025 and 2026.
Here is what an operator needs to know before signing on a paid search agency or auditing their current one.
Key Takeaways
- The gate to entry is LegitScript certification, not a credit card. No certification, no Google Ads. Lead generators, call centers reselling admits, and sober living homes are not eligible.
- In-network and out-of-network are two different products, not variations of the same play. OON optimizes against verified policy data with full-funnel tracking and $60K+ monthly minimum. INN optimizes for volume within geography at $10K+ monthly minimum.
- The bidding strategy is Max Conversion Value with weighted signals. $200 per lead, $2,000 per private-policy VOB, $5,000 per approved VOB. The algorithm needs 15 conversions of the target type within 21 days to optimize, which is the mathematical reason underfunded campaigns rarely work.
- Search impression share ceilings at roughly 35%. Past that threshold, additional spend in the same geography inflates CPC without adding admits. The growth lever is geographic expansion, not budget expansion.
- Full-funnel conversion tracking is the difference between a working campaign and a broken one. Standard tracking optimizes for cheap leads from low-converting populations. Full-funnel tracking optimizes for verified private-policy outcomes and shifts spend toward the right traffic within 60 days.
Google Ads for an addiction treatment center is a different sport than Google Ads for any other vertical. The gate to entry is LegitScript certification, not a credit card.
The conversion that funds the facility is a verified policy, not a form fill. The audience filter that matters most is income tier, not interest segmentation.
Roughly half the time a center says “our paid media isn’t working,” the ads themselves are not the problem.
This guide is the full-funnel version of how we run paid search for treatment centers at Webserv. It covers the entry requirements, the campaign architecture, the bidding strategy, the conversion tracking infrastructure, the budget tiers, the timeline, the landing page mechanics, the common mistakes, and the platform changes that matter in 2026.
It is written for operators, not for paid media specialists. The technical depth is in the cluster spokes if you want to go deeper.
Most rehab paid search accounts get fired for not generating enough leads. Most of them should be fired for generating the wrong ones. Lead volume is theater. Cost per private-policy VOB is the business.
Mitch Marowitz, Director of Paid Media, Webserv
A reader’s note before we start. Webserv has been running paid search for behavioral health and addiction treatment for nearly a decade. We manage roughly 40 active behavioral health accounts at any time and have run paid search across more than 200 treatment center brands. The numbers in this guide are what we see in our portfolio, not what we read in industry reports. For a worked example, our 3-brand behavioral health case study walks through the exact reallocation moves across a detox, a residential, and a mental health brand.
The industry reports tend to underestimate the cost of running paid search for out-of-network residential and overestimate the cost for in-network local outpatient. We will show our numbers in the right tier so you can size the spend against your facility correctly.
Part 1. Before you run a single ad
The behavioral health paid search environment is shaped by three constraints that do not apply to almost any other vertical. LegitScript certification, the Healthcare and Medicines policy on Google, and the substance use disorder classification that Google maps to the same enforcement stack as self-harm.
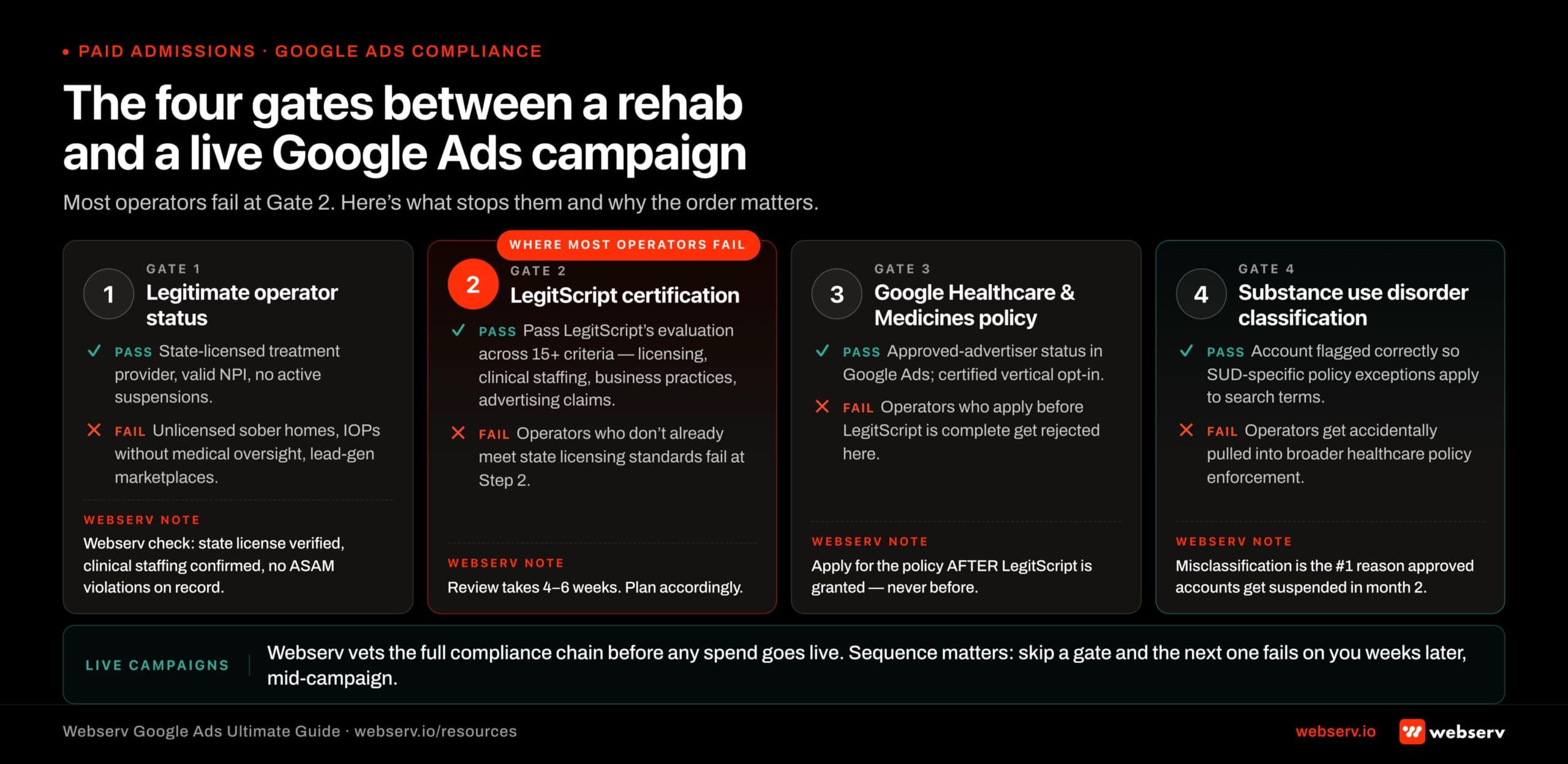 Infographic titled ‘The four gates between a rehab and a live Google Ads campaign.’ Visual sequence showing the four sequential compliance gates a treatment center operator must pass to run paid search ads. Gate 1 Legitimate operator status: requires state-licensed treatment provider, valid NPI, no active suspensions; unlicensed sober homes, IOPs without medical oversight, and lead-gen marketplaces fail here. Gate 2 LegitScript certification: requires passing 15+ criteria across licensing, clinical staffing, business practices, and advertising claims with a 4-6 week review window; this is where most operators fail. Gate 3 Google’s Healthcare and Medicines policy: requires approved advertiser status applied for AFTER LegitScript is granted, not before; operators who apply prematurely get rejected. Gate 4 Substance use disorder classification: requires correct account flagging so policy exceptions apply to SUD-specific search terms; misclassification is the number one reason approved accounts get suspended in month 2. Footer: ‘Most operators fail at Gate 2. Webserv vets the full chain before any spend goes live.’
Infographic titled ‘The four gates between a rehab and a live Google Ads campaign.’ Visual sequence showing the four sequential compliance gates a treatment center operator must pass to run paid search ads. Gate 1 Legitimate operator status: requires state-licensed treatment provider, valid NPI, no active suspensions; unlicensed sober homes, IOPs without medical oversight, and lead-gen marketplaces fail here. Gate 2 LegitScript certification: requires passing 15+ criteria across licensing, clinical staffing, business practices, and advertising claims with a 4-6 week review window; this is where most operators fail. Gate 3 Google’s Healthcare and Medicines policy: requires approved advertiser status applied for AFTER LegitScript is granted, not before; operators who apply prematurely get rejected. Gate 4 Substance use disorder classification: requires correct account flagging so policy exceptions apply to SUD-specific search terms; misclassification is the number one reason approved accounts get suspended in month 2. Footer: ‘Most operators fail at Gate 2. Webserv vets the full chain before any spend goes live.’Google’s own Healthcare and Medicines policy gates substance use disorder treatment advertising to LegitScript-certified providers. The policy explicitly requires certification before Google Ads approval is granted, which is why operators applying through Google first trigger automatic rejection at the Healthcare and Medicines review stage. The order matters: LegitScript first, Google policy approval second.
LegitScript certification
LegitScript is the third-party certification that gates paid advertising for addiction treatment on Google, Microsoft, and Meta. No certification, no ads. Period. The certification verifies the operator’s clinical licensing, regulatory compliance, treatment practices, and advertising disclosures. The application takes 30 to 60 days. Renewal is annual.
Two important exclusions: lead generators and call centers that resell admits are not eligible for LegitScript certification. Neither are sober living homes. If your facility model is admissions referral aggregation, the LegitScript path is not available and Google paid search is not available.
The renewal process is not automatic. Operators who let certification lapse get pulled from ad eligibility immediately. We recommend setting a recurring quarterly review of the certification status and a 90-day pre-expiration renewal protocol.
Google’s Healthcare and Medicines policy
Once certification is in place, Google routes addiction treatment ads through the Healthcare and Medicines policy. This policy controls eligibility, audience reach, and creative restrictions. Three rules matter most.
No retargeting. Customer data from health and medical information cannot be used for audience matching on addiction treatment campaigns. The retargeting playbook that works for ecommerce and SaaS does not exist here. The strategy compensates with broader prospecting audiences and stronger landing page work, not with creative workarounds.
Audience eligibility caps at 18+. Addiction treatment ads are limited to 18-and-up audiences. This is non-negotiable. It removes a portion of family members searching on behalf of an adolescent patient and shapes how adolescent-focused programs need to structure their paid social and SEO mix.
Restricted reach. Google labels addiction advertisers as eligible/limited. Audience expansion features, broad demographic targeting, and certain ad formats are constrained. Operators with sophisticated agencies are aware of every restriction in advance.
The substance use disorder classification
Google’s enforcement stack treats substance use disorder advertising similarly to suicide and self-injury content. This is operationally different from mental health advertising, which faces fewer restrictions.
Two specific implications: second-person ad copy gets flagged more aggressively in SUD campaigns than in mental health campaigns, and direct medical-condition references in headlines have lower approval rates. Compliant creative defaults to indirect language and outcome framing.
Who cannot advertise
Lead generators. Call centers reselling admits. Sober living homes. Operators with active DEA or state regulatory issues. Operators outside the United States targeting US audiences without a US clinical license. Operators whose LegitScript certification has lapsed. Operators in active dispute with Google’s policy team for prior violations.
The first six rule out a meaningful share of the BH advertising market. That fact is what makes the remaining market more competitive than the surface CPC numbers suggest.
Part 2. In-network versus out-of-network: two different playbooks
The biggest strategic decision in BH paid search is whether the facility is in-network with major payers or out-of-network, not what creative or bidding strategy you run. The strategies for those two models are not minor variations of the same play. They are fundamentally different products.
 Infographic titled ‘Two playbooks. Same platform. Wildly different economics.’ Side-by-side comparison of out-of-network versus in-network Google Ads playbooks for behavioral health. Out-of-network playbook targets self-pay and PPO-out-of-network patients with brand-plus-condition keywords like ‘inpatient rehab’ and ‘drug detox’ at $35 to $120 CPC, prioritizes calls over forms with $400 to $800 weighted call values, uses target CPA bidding, runs $25K to $80K monthly budgets, and converts at 4 to 9 percent. In-network playbook targets in-network commercial insured plus Medicare and Medicaid patients with insurance-specific location keywords like ‘Aetna rehab near me’ and ‘BCBS treatment’ at $8 to $30 CPC, prioritizes forms over calls with $80 to $150 weighted form values, uses target ROAS bidding, runs $5K to $25K monthly budgets, and converts at 12 to 22 percent. Out-of-network footer: higher CPC, fewer leads, much higher LTV per admit. In-network footer: lower CPC, more leads, lower LTV per admit but scalable volume. Bottom strip: hybrid facilities run both playbooks in separate ad groups, never blend.” class=”wp-image-23985″/>
Infographic titled ‘Two playbooks. Same platform. Wildly different economics.’ Side-by-side comparison of out-of-network versus in-network Google Ads playbooks for behavioral health. Out-of-network playbook targets self-pay and PPO-out-of-network patients with brand-plus-condition keywords like ‘inpatient rehab’ and ‘drug detox’ at $35 to $120 CPC, prioritizes calls over forms with $400 to $800 weighted call values, uses target CPA bidding, runs $25K to $80K monthly budgets, and converts at 4 to 9 percent. In-network playbook targets in-network commercial insured plus Medicare and Medicaid patients with insurance-specific location keywords like ‘Aetna rehab near me’ and ‘BCBS treatment’ at $8 to $30 CPC, prioritizes forms over calls with $80 to $150 weighted form values, uses target ROAS bidding, runs $5K to $25K monthly budgets, and converts at 12 to 22 percent. Out-of-network footer: higher CPC, fewer leads, much higher LTV per admit. In-network footer: lower CPC, more leads, lower LTV per admit but scalable volume. Bottom strip: hybrid facilities run both playbooks in separate ad groups, never blend.” class=”wp-image-23985″/>Out-of-network playbook
Out-of-network facilities have higher revenue potential per admit and higher cost per admit. They are competing for a smaller pool: roughly 23% of leads carry private (non-Medicaid) insurance. The strategy is built around finding and converting that 23%.
Out-of-network search campaigns optimize against verified policy data, not lead volume. The campaigns need full-funnel tracking that passes VOB outcomes back to Google Ads. The bidding strategy is Max Conversion Value with weighted signals. The audience targeting excludes the bottom 50% of income because that bracket is unlikely to carry a PPO policy that pays out.
Minimum recommended monthly spend for an OON detox or residential facility is $60,000. Below that, search impression share is too low to produce the conversion volume Google’s algorithm needs to optimize against private-policy outcomes.
Benchmarks we see in our OON portfolio:
| Metric | Range |
|---|---|
| Cost per lead (high intent) | $350 to $550 |
| Cost per private-policy VOB | ~$2,000 |
| Cost per approved VOB | ~$5,000 |
| % of leads with private insurance | ~23% |
| Search impression share ceiling | ~35% |
In-network playbook
In-network facilities have lower revenue per admit and lower CPA. They are competing for higher-volume covered admits within contracted payer networks. The strategy is built around volume within geography.
In-network campaigns can survive on standard form fill and call conversion tracking, though full-funnel tracking still helps. Bidding can be Max Conversions or Max Conversion Value depending on volume. The audience targeting is less aggressive on income segmentation because the payer mix is more predictable.
Minimum recommended monthly spend for an in-network local outpatient program is $10,000. The campaign covers a smaller geography (one local market), uses tighter match types, and operates with a flatter conversion value structure.
Benchmarks for in-network local outpatient:
| Metric | Range |
|---|---|
| Cost per lead | ~$350 |
| Cost per admit | Varies by contracted carrier rates |
| Search impression share ceiling | ~35% (same as OON) |
| Minimum monthly spend | $10,000 |
Which playbook applies to your facility
If your facility takes out-of-network insurance and your goal is to maximize the percentage of admits with PPO coverage, run the OON playbook.
If your facility is contracted with a network of payers and your goal is to fill beds at the contracted rate, run the INN playbook.
Facilities that take both should run separate campaigns for each, with separate conversion tracking and separate bidding logic.
The most expensive mistake in this category is running an OON playbook on an INN budget or an INN playbook on an OON budget. We see both routinely.
Part 3. Campaign architecture
Once the playbook is selected, the campaign architecture follows a consistent pattern. Search is the primary channel because it captures intent at the moment a patient or family member is searching for help.
Search campaign structure
Ad groups are organized by level of care and search theme, not by keyword. The structure looks like this:
| Campaign | Ad groups |
|---|---|
| Detox | “Detox near me”, “Alcohol detox”, “Drug detox”, “Medical detox” |
| Residential | “Residential rehab”, “Inpatient rehab”, “30 day rehab” |
| PHP / IOP | “Partial hospitalization”, “Intensive outpatient”, “Day program rehab” |
| Outpatient | “Outpatient rehab”, “Sober living outpatient”, “Aftercare” |
| Population-specific | “Veteran rehab”, “Adolescent rehab”, “Executive rehab” |
| Insurance-specific (optional) | “Aetna rehab”, “BCBS rehab”, “TRICARE rehab” |
Each ad group runs a tightly themed keyword set with matched headlines and landing pages. “Near me” modifiers are the highest-priority targets because they capture the highest-intent traffic.
Match types
Exact and phrase match are the defaults. Broad match is used cautiously and only after a clean negative keyword list is in place. Search terms in BH go off-topic faster than in most verticals. A “drug rehab” broad query will pull traffic from physical rehabilitation searches, marijuana legalization searches, and search terms generated by users in active intoxication who do not convert to admits.
The negative keyword list for a mature BH account typically runs 800 to 2,000 negatives. Common categories: physical rehab terms, legal terms, drug name slang, recreational use queries, “near me” queries pulling from low-conversion geographies, and competitor brand terms (depending on strategy).
Geographic targeting
OON detox and residential campaigns can run nationally with state-by-state bid modifiers. The bid modifiers reflect the policy mix variation by state. States with higher PPO penetration get higher bids.
In-network campaigns run within a defined service radius around the facility. For local outpatient, the radius is typically 15 to 30 miles. For regional residential, the radius extends to 100 to 200 miles. Patients drive for the right program. They do not drive for outpatient IOP.
A geographic mistake we see regularly: campaigns targeting markets where the facility does not have a meaningful referral pipeline or admissions team capacity. The ad reaches the searcher. The admissions team cannot close the lead because the geography does not work. The campaign wastes budget while looking like it is performing.
Part 4. Bidding strategy and conversion values
The bidding strategy is where OON and INN start to diverge most sharply. The same campaign architecture can produce two different commercial outcomes depending on the bidding setup.
Why bidding strategy matters
Google’s automated bidding optimizes against the conversion signal you feed it. If the conversion signal is a form fill, the algorithm optimizes for cheap form fills. If the conversion signal is a verified private-policy VOB, the algorithm optimizes for verified private-policy VOBs. The same campaign run against those two signals produces different admit mixes within 60 days. The underlying Quality Score mechanics compound with whichever signal the campaign is feeding.
For most BH operators, the right bidding strategy is Maximize Conversion Value with weighted conversion signals. This is not the default Google recommends in account setup. The setup requires custom configuration and ongoing maintenance.
Weighted conversion values
A weighted conversion structure assigns a dollar value to each downstream event in the funnel. Webserv’s default structure:
| Event | Conversion value | Logic |
|---|---|---|
| New lead (form fill or call) | $200 | Initial touchpoint signal |
| VOB on any private (non-Medicaid) policy | $2,000 | 10x lead value; the primary optimization target |
| Approved VOB (policy clears client criteria) | $5,000 | Highest-weight signal; usually a subset of VOBs |
| Admit | Tracked separately | Low volume; high-value reporting signal |
The algorithm uses these values to bid more aggressively on queries and audience segments that historically produce higher-weighted conversions. The result is that the campaign learns to favor traffic that converts to private-policy VOBs over traffic that converts to form fills only.
The 15-conversion threshold
Google’s smart bidding algorithms need roughly 15 conversions of the target type within a 21-day window to optimize effectively. A 30-day window is acceptable but suboptimal.
For a BH operator running Max Conversion Value bidding optimized for VOBs, this means the account needs to produce at least 15 VOBs in three weeks for the bidding to work as designed. At a ~$2,000 cost per VOB, that requires roughly $30,000 in monthly spend on a campaign that is operating at the standard 23% policy mix.
Below that threshold, the algorithm is essentially guessing. This is the mathematical reason underfunded campaigns rarely optimize well. Not because the operator is doing something wrong. Because the data volume is below the threshold the bidding system needs to function.
When to override the default
There are two situations where Max Conversions is preferable to Max Conversion Value:
Early launch (Month 1). New accounts need volume to give the algorithm enough conversions to learn from. Running Max Conversions for the first 30 to 45 days while the campaign builds data, then switching to Max Conversion Value, is a defensible sequence.
Below the volume threshold. If the account cannot produce 15 VOBs in 21 days at any budget level the operator will fund, Max Conversion Value optimization breaks. Max Conversions at least keeps the algorithm functioning while the operator either scales the budget or expands the geographic footprint.
Part 5. Conversion tracking infrastructure
Conversion tracking is where most BH paid search accounts fail. The campaign looks fine in Google Ads because Google sees what the account configured it to see. The account configuration is the problem.
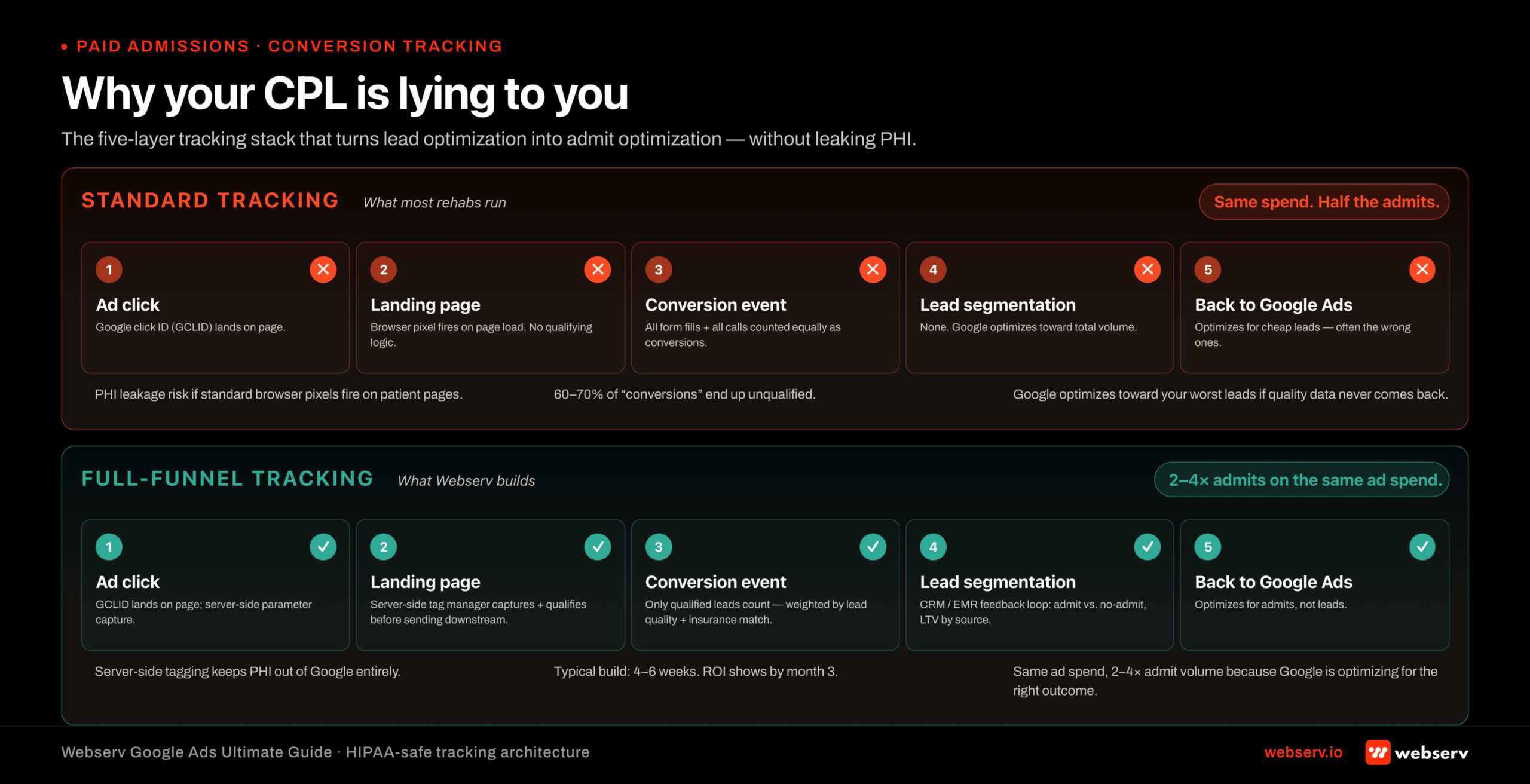 Infographic titled ‘Why your CPL is lying to you’ showing two horizontal tracking architectures stacked for comparison. Top stack labeled ‘Standard tracking (broken)’ shows the five-layer flow most rehab accounts run: Google click ID lands on landing page, browser pixel fires on page load with no qualifying logic, all form fills and calls counted equally as conversions, no lead segmentation feeds back to Google, and Google ends up optimizing for cheap unqualified leads. Risk callouts: PHI leakage from standard browser pixels firing on patient data pages, 60 to 70 percent of conversions unqualified, optimization aimed at bad leads. Bottom stack labeled ‘Full-funnel tracking (Webserv)’ shows the same five layers rebuilt for HIPAA safety: server-side tag manager captures and qualifies leads before they hit Google, only qualified weighted conversions counted with lead quality and insurance match factored in, CRM and EMR admit data flows back to Google, and optimization aims at admits not leads. Result on the same ad spend: 2 to 4x admit volume because Google is optimizing for the right outcome. Annotation: server-side tagging keeps PHI out of Google entirely, typical setup 4 to 6 weeks to implement, ROI shows by month 3.
Infographic titled ‘Why your CPL is lying to you’ showing two horizontal tracking architectures stacked for comparison. Top stack labeled ‘Standard tracking (broken)’ shows the five-layer flow most rehab accounts run: Google click ID lands on landing page, browser pixel fires on page load with no qualifying logic, all form fills and calls counted equally as conversions, no lead segmentation feeds back to Google, and Google ends up optimizing for cheap unqualified leads. Risk callouts: PHI leakage from standard browser pixels firing on patient data pages, 60 to 70 percent of conversions unqualified, optimization aimed at bad leads. Bottom stack labeled ‘Full-funnel tracking (Webserv)’ shows the same five layers rebuilt for HIPAA safety: server-side tag manager captures and qualifies leads before they hit Google, only qualified weighted conversions counted with lead quality and insurance match factored in, CRM and EMR admit data flows back to Google, and optimization aims at admits not leads. Result on the same ad spend: 2 to 4x admit volume because Google is optimizing for the right outcome. Annotation: server-side tagging keeps PHI out of Google entirely, typical setup 4 to 6 weeks to implement, ROI shows by month 3.Guidance from the HHS Office for Civil Rights on online tracking technologies confirms that IP addresses combined with health information constitute PHI under HIPAA. Standard Google Ads conversion pixels firing on a treatment center’s insurance verification page or symptom-assessment page create direct exposure: the URL paths reference health conditions, and the IP traveling with them is regulated data. That is why the right tracking pattern routes through a server-side intermediary, not a browser-side pixel.
Standard tracking versus full-funnel tracking
Standard conversion tracking captures the initial form fill or call. Full-funnel tracking captures the verified policy outcome on the back of that form fill. The two systems produce very different optimization behavior.
A standard-tracking account optimizing for form fills will eventually find traffic that produces cheap form fills from low-converting populations. The cost per lead looks great. The admit rate is awful. The operator concludes that paid search “is not generating quality leads” when the paid search system is doing exactly what it was configured to do.
A full-funnel-tracking account passes the VOB and admit outcomes back into Google Ads as offline conversions. The algorithm learns which lead sources produce private-policy VOBs and which do not. Within 60 days, the campaign shifts spend toward the higher-converting traffic without any manual intervention.
What the full-funnel stack looks like
A working stack typically includes:
A CRM or admissions platform (Salesforce Health Cloud, KipuHealth, Sigmund, or similar) that captures every inbound lead, the outcome of the verification call, and the admit decision.
An offline conversion import from the CRM into Google Ads. The import sends a record for each lead with the gclid (Google Click ID), the timestamp, and the conversion value. The conversion value is the weighted dollar amount: $200 for a lead, $2,000 for a VOB, $5,000 for an approved VOB.
A consent and HIPAA layer. Even on Google Ads (which has fewer HIPAA-adjacent restrictions than Meta), the way lead data is passed back to the platform needs to be reviewed by counsel. The setup matters for compliance even where Google’s own policies do not explicitly require it.
A reporting layer that exposes the funnel outcomes to the operator. The admissions team needs to see how their close rate on paid leads compares to their close rate on organic and referred leads. The marketing team needs to see cost per private-policy VOB, not just cost per lead. Most of this flows through CallRail or equivalent call tracking for the call side of the funnel.
HIPAA considerations on Google Ads
Google does not gate addiction treatment advertising through a Business Associate Agreement the way Meta does. The standard Google Ads tag is not HIPAA-compliant by default. The conversion data passed back through offline conversion imports needs to avoid transmitting protected health information.
The compliant pattern: pass the gclid, timestamp, conversion type, and conversion value. Do not pass the patient name, diagnosis, or any identifier that would let Google associate the conversion with a specific person. The conversion value approach above stays within those guardrails.
Operators with sophisticated legal counsel sometimes add a BAA-style intermediary layer to the data flow even where Google does not require it. The cost is modest. The risk reduction is meaningful for facilities operating under tight compliance scrutiny.
How Profound Treatment drove 31 admits and a 42% drop in cost per viable in one quarter
Broad match pivot, negative keyword management, and intake-level conversion tracking turned a fragmented paid strategy into a predictable admissions engine.
Read the case study →68 viable VOBs at $4,529 cost per viable
Part 6. Budget tiers and benchmarks
$10K-$20K
Tier 1: in-network local outpatient, single market, single LOC
$20K-$60K
Tier 2: regional in-network or smaller out-of-network, multi-LOC
$60K+
Tier 3: out-of-network detox and residential, multi-state
Most operators size their paid media budget based on what they can afford rather than what the campaign needs to function. The result is underfunded campaigns that never reach the optimization threshold.
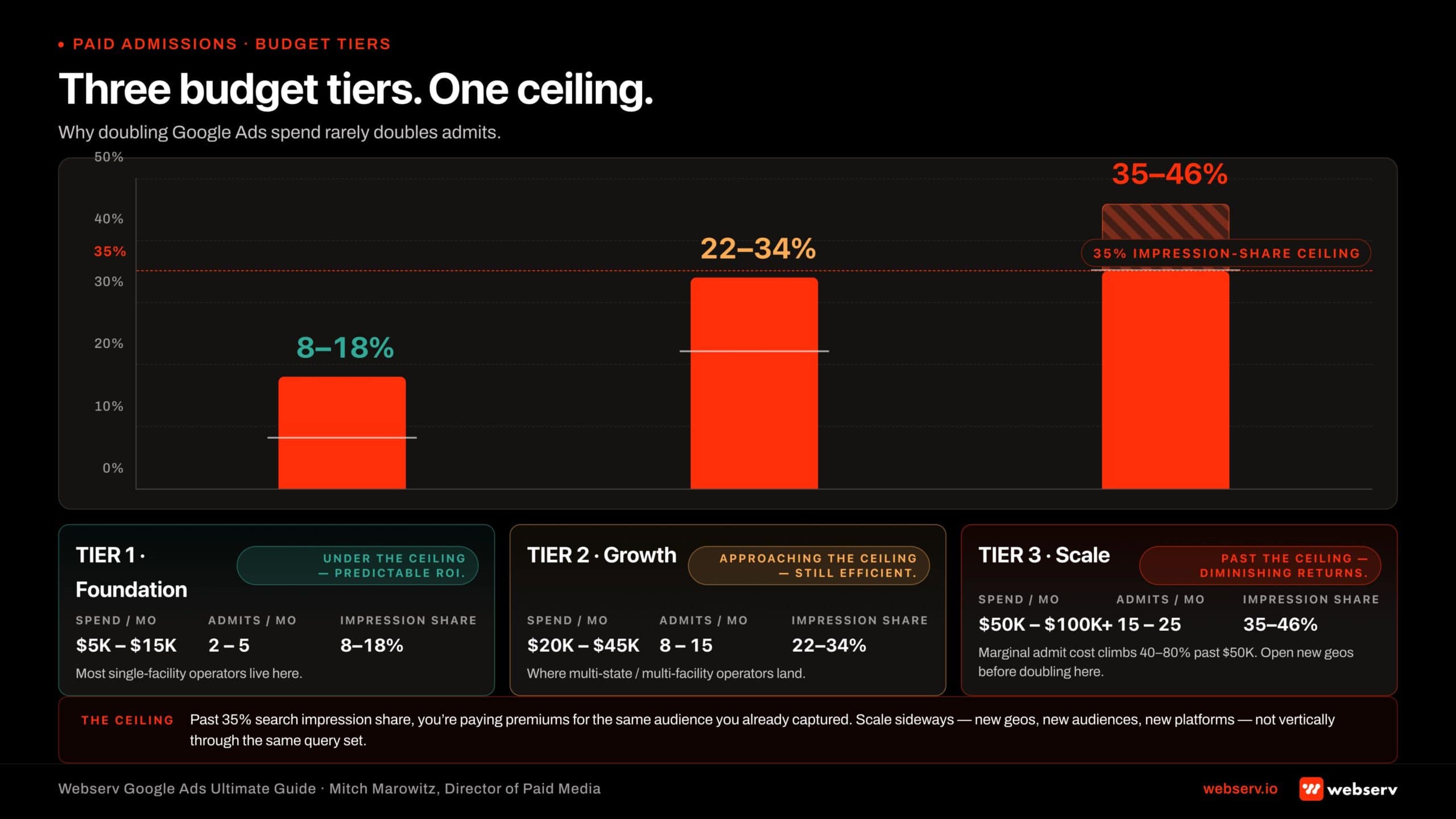 Infographic titled ‘Three budget tiers. One ceiling.’ Bar chart showing three Google Ads budget tiers for rehab operators with a horizontal red dashed line at 35 percent search impression share labeled ‘The ceiling.’ Tier 1 Foundation: $5K to $15K monthly spend producing 2 to 5 admits per month at 8 to 18 percent impression share, sitting under the ceiling, predictable ROI, where most single-facility operators live. Tier 2 Growth: $20K to $45K monthly producing 8 to 15 admits at 22 to 34 percent impression share, approaching the ceiling, still efficient, where multi-state and multi-facility operators land. Tier 3 Scale: $50K to $100K plus monthly producing 15 to 25 admits at 35 percent plus impression share, past the ceiling, marginal admit cost climbs 40 to 80 percent. Ceiling annotation: 35 percent search impression share marks the point where the operator is paying premiums for the same audience already captured. Webserv recommendation: scale sideways with new geographies, new audiences, and new platforms before doubling vertically past Tier 2.
Infographic titled ‘Three budget tiers. One ceiling.’ Bar chart showing three Google Ads budget tiers for rehab operators with a horizontal red dashed line at 35 percent search impression share labeled ‘The ceiling.’ Tier 1 Foundation: $5K to $15K monthly spend producing 2 to 5 admits per month at 8 to 18 percent impression share, sitting under the ceiling, predictable ROI, where most single-facility operators live. Tier 2 Growth: $20K to $45K monthly producing 8 to 15 admits at 22 to 34 percent impression share, approaching the ceiling, still efficient, where multi-state and multi-facility operators land. Tier 3 Scale: $50K to $100K plus monthly producing 15 to 25 admits at 35 percent plus impression share, past the ceiling, marginal admit cost climbs 40 to 80 percent. Ceiling annotation: 35 percent search impression share marks the point where the operator is paying premiums for the same audience already captured. Webserv recommendation: scale sideways with new geographies, new audiences, and new platforms before doubling vertically past Tier 2.The three tiers
Tier 1: $10,000 to $20,000 per month. In-network local outpatient. One market. One level of care. Standard conversion tracking. Max Conversions bidding. Geographic radius of 15 to 30 miles. CPL benchmark around $350. Admit rate dependent on contracted payer mix.
Tier 2: $20,000 to $60,000 per month. Regional in-network or smaller out-of-network. Multiple levels of care. Full-funnel tracking starts to make sense in this tier. Max Conversion Value bidding becomes viable at the upper end of this range. Mixed search and remarketing-substitute prospecting.
Tier 3: $60,000 and up per month. Out-of-network detox and residential, national or multi-state. Full-funnel tracking is mandatory. Max Conversion Value bidding with weighted VOB signals is the default. CPL $350 to $550. Cost per private-policy VOB ~$2,000. The campaign reaches the optimization threshold reliably.
The 35% search impression share ceiling
Search results begin to diminish past roughly 35% search impression share in BH paid search. The reason is the insurance policy filter. Above that ceiling, the campaign is reaching searchers who do not carry the right policy mix to convert.
When a campaign approaches the 35% ceiling, the correct response is geographic expansion, not budget expansion. Adding more spend in the same geography inflates CPCs and pulls the cost per VOB up without adding viable admits. Expanding to an adjacent state or metro keeps the impression share below the ceiling and maintains optimization quality.
This is one of the most counterintuitive facts in BH paid search. The growth lever past a certain budget is geographic, not financial.
Industry data versus operator reality
Public industry data tends to underestimate BH paid search costs. The most-cited 2026 benchmark for “addiction recovery” CPL is $120.30, drawn from LocaliQ’s healthcare benchmarks data. That number averages across mental health, outpatient counseling, and small-program campaigns where the OON dynamics do not apply.
For an OON detox or residential facility specifically, $120 CPL is not achievable. The $350 to $550 range we publish is what real campaigns produce when measured honestly. Operators who are quoted $120 CPL on an OON campaign are being quoted a benchmark that does not apply to their operating model.
The same dynamic applies to addiction recovery’s reported 77% YoY CPL increase. The number is real for the aggregate. For specific operator tiers it under- or over-states the change. Webserv’s portfolio data shows OON CPL roughly stable year-over-year and INN CPL up 12% to 18% in the same window, with the increase concentrated in markets where weight-loss drug advertising has driven up healthcare CPCs broadly.
Part 7. Timeline: what to expect
Treatment center operators new to paid search consistently expect faster results than the campaign can produce. The data threshold is the constraint. Below the volume needed to optimize, the campaign produces inconsistent results that look like underperformance.
Month 1: setup and launch
The campaign typically launches three weeks after engagement. The first week is account audit, LegitScript verification, conversion setup, and ad creative development. The second week is landing page review and tag implementation. The third week is launch and the first live optimization pass.
Month 1 is data collection, not optimization. CPL is volatile. Lead quality is mixed. The algorithm is learning. Operators who judge performance by Month 1 numbers will make the wrong call. Operators who quit after Month 1 leave before the system can deliver what they paid for.
Month 2: first optimization
A full month of data enables real pivots. CPL begins declining week over week. Policy mix data flows through to bidding adjustments. Negative keyword lists tighten. Ad copy variants are A/B tested against real volume.
Most clients see a noticeably better month in Month 2. Lead volume stabilizes. Lead quality improves. The cost per VOB starts to trend toward the operator’s target.
Month 3 and beyond: optimized campaign
If the campaign was set up correctly and Months 1 and 2 went as expected, Month 3 should represent a well-optimized, scalable campaign. CPL within target range. Policy mix near 23% for OON or near contracted rates for INN. Conversion volume reliable enough that Max Conversion Value bidding is working as designed.
This is when scaling decisions are made. Increase budget. Expand geographically. Add a paid social layer. Test PMAX. The campaign is the platform the rest of the marketing stack now compounds on. Operators ready to add the Meta layer can start from our scored ranking of paid social ad agencies for the Meta-side of the budget, which applies the same operational discipline this guide demands from a paid search partner.
Part 8. Search versus PMAX: when and how
Performance Max adoption grew from 60% of advertisers in 2024 to 71% in 2025 across all verticals. BH paid search adoption tracks slightly behind that curve because the data thresholds for PMAX are higher.
When pure search is the right move
For OON facilities below $120,000 monthly spend, pure search outperforms PMAX. The search inventory is the highest-intent traffic and the bidding system can optimize against it efficiently at moderate volumes. PMAX layered on top before the operator has saturated search wastes budget on lower-intent inventory.
For in-network local outpatient, pure search is the default at every budget tier. PMAX requires national or regional reach to perform. Local outpatient with a 30-mile radius does not produce enough PMAX volume.
When PMAX makes sense
For OON facilities above $120,000 monthly spend, pure search starts to hit diminishing returns. The 35% impression share ceiling is the proximate cause. PMAX opens additional inventory (YouTube, Discover, Display) that can pick up traffic the search-only campaign cannot reach.
Local PMAX (single market) becomes viable at $10,000 to $15,000 monthly spend. National PMAX requires $60,000 to $65,000 monthly minimum to generate the data PMAX needs to optimize.
Between $50,000 and $120,000 monthly, the right search/PMAX mix is a judgment call based on the operator’s goals. Higher private-policy mix targets favor more search. Higher total admit volume targets favor more PMAX.
Demand Gen as the awareness layer
Demand Gen campaigns sit upstream of search. They build awareness on YouTube, Discover, and Gmail. They are appropriate for established BH brands with a recognized name that want to reach families before the crisis search begins.
For most operators, Demand Gen is a Tier 3 spend ($60,000+/month accounts) and a Year 2+ initiative. The campaign does not directly produce admits. It produces brand awareness that compounds with the search campaign over time.
Part 9. Landing pages and creative
The campaign delivers the click. The landing page converts the click. Most operators underinvest in landing pages relative to ad spend, which is a costly mistake.
The landing page work pairs with our landing page optimization guide for treatment centers and our coverage of compliant ad headlines for rehab and addiction treatment. Operators investing in paid search without strong landing pages typically see CPLs that look acceptable in Google Ads and admit rates that look terrible at the facility level.
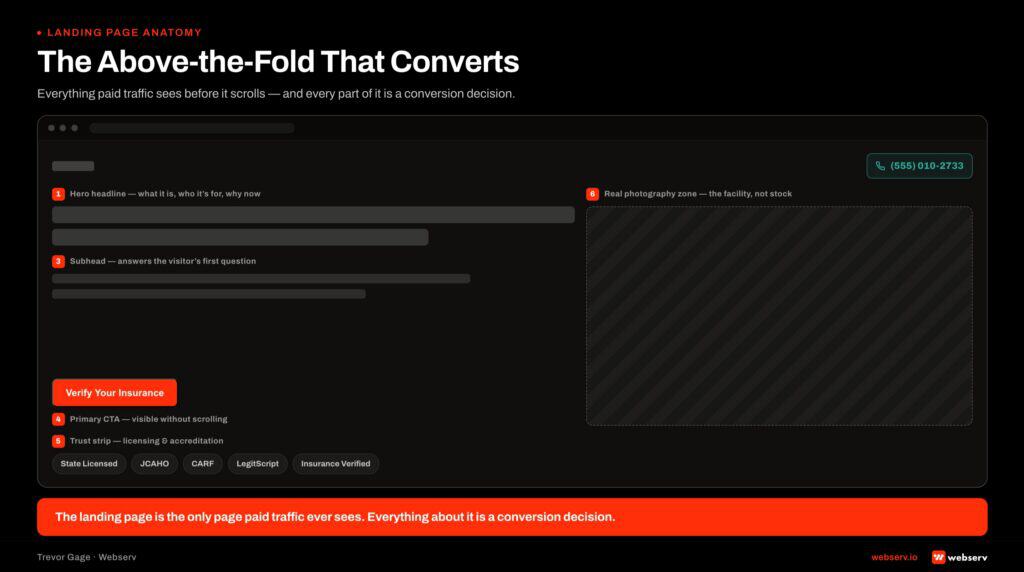
What belongs above the fold
Clear unique selling proposition. What makes this facility different. Not “compassionate care” or “individualized treatment.” Specific: “Only adolescent-focused residential program in California with on-site academic credit.” “Joint Commission accredited, in-network with Aetna and Cigna.” “Veteran-built program with VA CCN Region 1 contract.”
Strong call to action. Static call button visible at all times. Family members in crisis do not click through to a contact form. They call. The call button stays on screen during scroll.
Trust builders above the fold. Joint Commission seal. Accreditations. Named medical director with credentials. Insurance accepted (when honest). A family member deciding whether to call needs to see the trust signals before they scroll.
Confidentiality assurance. Unique to addiction treatment. Many callers need explicit reassurance that the call is confidential before they will reach out. The confidentiality language belongs above the fold or in the hero callout.
What works on mobile
Webserv runs mobile-first or mobile-only on most BH campaigns. Mobile users searching “detox near me” close at materially higher rates than desktop researchers because mobile traffic is more often in active crisis. Desktop traffic skews toward research mode, which has a slower path to admission.
Mobile-only campaign exceptions: national OON detox/residential where desktop sometimes performs comparably, and B2B referral programs targeting professional referrers on LinkedIn.
What to avoid on Google Ads search
Call extensions on search. Call extensions tend to generate competitor calls (other operators researching the market) and low-quality contacts. They perform better on Performance Max than on standard search.
Location extensions on search. Location extensions expose the facility’s address. This undercuts the “near me” strategy and tends to attract Medicaid callers searching for the nearest treatment center rather than the right one.
Aggressive demographic exclusions at low budgets. Excluding the lower 50% income bracket removes ~30% of total searchers. Excluding “unknowns” removes ~50%. These exclusions only make sense at budget tiers where impression share can afford the narrowing.
Part 10. Common mistakes
LEGITSCRIPT REJECTION TRIGGERS
The five patterns that get behavioral health Google Ads accounts suspended or LegitScript certification revoked: unverified location addresses on landing pages, claims of “guaranteed sobriety” or specific outcome rates, missing physician-supervised language on medical detox pages, insurance logos used without written carrier permission, and cost-per-lead affiliate schemes routed through the ad account. All five are surfaced in policy reviews and account audits before campaigns launch — not after.
Five patterns we audit and see repeated across BH paid search accounts that are underperforming. The full compliance mistakes framework covers the policy side of these failures.
- Optimizing for lead volume instead of policy quality. The campaign produces a high volume of cheap leads that the admissions team cannot close. The operator interprets this as “paid search is generating quality leads” until the close rate data shows otherwise. The fix is full-funnel tracking and Max Conversion Value bidding against VOB signals.
- Quitting after Month 1. The data threshold for optimization is roughly 15 conversions in 21 days. Month 1 is data collection. Operators who quit before Month 2 leave before the system can perform. The campaign is not broken. The clock has not finished.
- Treating in-network and out-of-network the same. Running an OON playbook on an INN budget produces an underfunded campaign that never reaches optimization threshold. Running an INN playbook on an OON budget produces high lead volume with the wrong policy mix. Each playbook is its own product.
- Broad match without disciplined negative keywords. Broad match in BH pulls traffic from physical rehab, recreational drug, legal, and crisis-line queries that do not convert. The negative keyword list has to be 800 to 2,000 entries deep before broad match performs.
- Adding spend in a saturated market. Past 35% search impression share, additional spend inflates CPC without adding admits. Operators who keep adding budget in their primary market when they should be expanding geography pay more for the same volume.
WHAT WORKING REHAB GOOGLE ADS DO
- Optimize against verified policy quality (VOB signals)
- Hold for at least 2 months of data before campaign changes
- Run separate INN and OON campaigns with separate bidding
- Tighten match types as the data set matures
- Pair Search with PMAX or Demand Gen, not as a substitute
WHAT BROKEN REHAB GOOGLE ADS SKIP
- Optimize for raw lead volume the admissions team cannot close
- Quit after Month 1 because “the campaign is not performing”
- Run one campaign covering both in-network and out-of-network
- Leave broad match running with no negative keyword discipline
- Replace Search with PMAX and lose conversion attribution clarity
Part 11. Measurement and reporting
The standard agency report focuses on lead volume, CPL, and click-through rate. Those metrics describe activity. They do not describe whether the activity produced admissions.
Measurement on the paid search side is incomplete without the back-of-funnel data covered in our revenue cycle management guide. Cost per lead and cost per admit only become defensible numbers when the billing operation reliably collects on the leads paid search produces.
The metrics that predict whether a BH paid search account is healthy are:
Cost per private-policy VOB. The primary metric for OON. Target range $1,500 to $2,500. Anything above $2,500 should trigger a campaign review.
Cost per approved VOB. The closer-to-revenue version of cost per VOB. Target range $4,000 to $6,000. Higher than $6,000 usually means the admissions team is screening out leads that look qualified to Google but are not.
Policy mix percentage. The percentage of leads carrying private (non-Medicaid) insurance. OON target is 23% to 30%. INN target depends on contracted payer mix; usually 60% to 80%.
Search impression share by market. Track impression share at the geographic unit you bid on. State, metro, or DMA. The 35% ceiling is the constraint to watch.
Cost per admit. The downstream truth. OON target range varies widely by program ($8,000 to $20,000 cost per admit is the working band). INN target depends on contracted rates.
Mobile versus desktop close rate. Track separately. Mobile should close higher. If desktop is closing higher, the mobile landing page or call workflow needs review.
A monthly operator-facing report should include all six metrics, trended over the last six months, with the year-over-year comparison where the data exists. Most agency reports show none of these. That is a signal worth acting on.
Part 12. What changed in 2025 and 2026
A short list of platform changes worth knowing.
PMAX adoption growth. Performance Max usage grew from 60% of advertisers in 2024 to 71% in 2025. For BH operators, this matters most at Tier 3 spend levels where PMAX is increasingly the default scale lever past search saturation.
Demand Gen reaching maturity. Google’s Demand Gen format has matured into the awareness-layer counterpart to PMAX. For BH brands with the budget to operate at scale, Demand Gen is the upper-funnel investment that compounds with search over 12 to 24 months.
AI Max for Search. Google’s AI-assisted Search campaign format extends Smart Bidding into broader query coverage. The implications for BH are mixed. AI Max picks up tangential queries that have to be policed with negative keywords. We are running it cautiously in our portfolio with stricter negative list maintenance.
Healthcare CPC inflation. Healthcare CPCs rose roughly 18% year-over-year in 2025, driven largely by competition from weight-loss drug advertisers and telehealth platforms. BH operators not running aggressive bidding strategies are getting outbid in shared auctions.
FDA scrutiny on substance use treatment advertising. The FDA issued 30 warning letters in March 2026 to substance use treatment providers, focused on advertising claims about outcomes and treatment success rates. Operators making any kind of outcome claim in paid creative should review the claim against current FDA guidance. The same scrutiny applies to AI-citable content per our AEO Ultimate Guide. The risk is real and rising.
Frequently asked questions about Google Ads for addiction treatment centers
What is a realistic monthly budget for residential versus outpatient Google Ads?
Most residential treatment centers running disciplined Google Ads spend between $30,000 and $80,000 per month, scaling with bed count and target market. Outpatient programs typically run smaller budgets, $10,000 to $25,000 per month, because the geographic radius is tighter and the cost-per-click on outpatient-specific terms is lower than on residential terms.
Below $15,000 per month on residential paid search, the program does not generate enough conversion data for Smart Bidding to calibrate against verified VOBs. The algorithm runs on noise rather than signal. Programs in that range tend to see inconsistent admit volume month to month, not because the strategy is wrong but because the data volume is below the calibration threshold.
The budget conversation should always be downstream of the conversion tracking conversation. A program without HIPAA-compliant tracking and weighted conversion values configured cannot defensibly size budget regardless of the number. Fix the measurement layer first, then size against what the data shows is working.
Should we hire an agency or run Google Ads in-house?
Most treatment centers under $30M in revenue do best with a specialist agency rather than in-house Google Ads management. The vertical-specific knowledge (LegitScript, HIPAA-aware tracking, OCR enforcement reality, behavioral health policy patterns) takes years to build, and the cost of bringing an in-house team up to that bar is generally higher than agency fees once you account for full-loaded headcount.
Larger programs (above $30M in revenue or running multi-location operations across multiple states) sometimes run hybrid models: in-house marketing leadership manages strategy and reporting, with specialist agency execution at the channel level. The right split depends on whether the in-house leader has prior agency experience in BH or is learning the vertical on the job.
The model that fails consistently is hiring a generalist in-house Google Ads manager without specialist agency support. The cost of the learning curve in the BH vertical (account suspensions, HIPAA violations, miscalibrated conversion tracking) typically erases any savings from the in-house arrangement inside the first year.
How does the 2024 OCR HIPAA guidance affect our Google Ads tracking?
The 2024 OCR online tracking guidance treats the standard Google Ads conversion tag and the Google Analytics tag as HIPAA-non-compliant when they fire on pages that touch PHI (treatment-specific pages, intake forms, insurance verification forms). The standard pixel transmits browsing behavior to Google in a way that the guidance considers a HIPAA violation when the underlying pages are patient-adjacent.
The fix is a HIPAA-aware analytics intermediary with a signed BAA that strips or hashes PHI before forwarding conversion events to Google Ads. The compliant pattern involves three layers: BAA-protected event collection on-page, server-side event forwarding, and audience strategy built from non-PHI signals. The full pattern is in our conversion tracking guide for addiction treatment Google Ads.
Treatment centers running standard Google tracking on patient-adjacent pages carry exposure that compounds. OCR penalties for tracking-related violations have run into seven figures for healthcare systems since the guidance landed. The cost of building the compliant tracking layer is substantially smaller than the cost of an enforcement action.
How do we know if our current agency is doing real behavioral health Google Ads work?
Three diagnostic questions surface most of the gap. First: what is our primary conversion event, and is it weighted by policy type? A specialist agency answers with a specific value structure (e.g., $200 for a new lead, $2,000 for a private-policy VOB, $5,000 for an approved VOB). A generalist agency answers in generic terms or defaults to raw form-fill volume.
Second: what is our LegitScript certification status and renewal cycle? A specialist agency owns this proactively and can tell you the next renewal date and the documentation pipeline. A generalist agency refers you to a third-party compliance vendor and stays out of the certification process, which is a flag.
Third: what is our HIPAA-compliant tracking architecture? A specialist agency can name the analytics intermediary, show you the BAA, and walk you through which conversion events flow through it. A generalist agency says the standard Google tag plus Google Analytics is fine, which is the answer that creates OCR exposure.
How long from launching paid search to consistent admit volume?
Most treatment centers see first admits from a new paid search account within 7 to 21 days of launch, with consistent admit volume building between days 30 and 90. The first 30 days are typically the algorithm calibration window: enough conversion data accumulates for Smart Bidding to identify which keywords, audiences, and creative variants produce qualified leads versus form-fill noise.
Programs starting from zero (new facilities, no prior paid search) take longer to reach consistent admit volume than programs adding paid search to an existing organic presence. The branded search query volume that compounds paid search performance is small or nonexistent at launch, and Google’s algorithm has less authority signal to work with.
The cleanest signal that paid search is working is the cost-per-admit comparison at day 90 against forecasted budget. A program hitting the forecasted cost-per-admit at day 90 with consistent admit volume in the prior 30-day window is in a position to scale spend confidently. A program missing the forecast at day 90 needs a diagnostic conversation, not more budget.
What this means for treatment center operators
Google Ads remains the most important admissions acquisition channel for treatment centers because it captures intent at the moment a patient or family is searching for help. Nothing else in the channel mix does that. The trade-off is that it is also the most technical, most regulated, and most expensive channel to run badly.
The operators winning at Google Ads in 2026 are running it as an operational discipline, not as a media buy. Full-funnel conversion tracking. Weighted conversion values. Geographic expansion at impression share ceilings. Mobile-first creative. Quality over quantity on lead optimization. Trust signals on the landing page. A monthly report that shows cost per private-policy VOB and admit attribution.
The operators losing at Google Ads are running it as a generic paid search campaign with healthcare-shaped creative on top. Optimization for lead volume. Standard conversion tracking. PMAX layered on before search is saturated. Broad match without disciplined negatives. Reports built around CPL and click-through rate.
The gap between those two operating modes is widening, not narrowing. Google’s algorithms reward the operational version more than they did three years ago. The technical depth required to run paid search well in BH has compounded. The agencies that built infrastructure for the right way are pulling away from the ones that did not.
If you want to walk through whether your current paid search setup is the first version or the second, book a discovery call. We will pull your account, look at the tracking stack, the bidding strategy, the negative keyword list, and the conversion value setup, and tell you honestly what we see. Discovery is free. The honest answer is the deliverable, not the pitch.
The perspective in this article comes from 9 years working exclusively inside behavioral health.
We are a team built by people in recovery who understand that behind every admission is someone asking for help. If that resonates, get to know us.
Mitch Marowitz is the Director of Paid Media at Webserv, a digital marketing agency for treatment centers.