There is a pattern I see across treatment center operators that shows up on the audit call before the operator ever finishes describing the situation. The marketing spend is up. The admits are flat. The billing data is muddled.
When the operator tries to get answers from the admissions team about specific inbound calls, the answers do not come. Or they come slowly. Or they come with defensiveness.
The operator has become hostage to their admissions team. And by the time they recognize it, they are usually five or six months into a revenue leak that has cost them hundreds of thousands of dollars, or millions in some cases.
I have walked into this situation more times than I can count across the admissions operations rebuilds we run at Webserv. It comes in two flavors. Both are recoverable.
Both take the same underlying fix: a system that does not depend on any single person or third party, and full transparency into every phone call and every dollar of marketing spend.
This article is written for the operator who suspects they are in this pattern and wants to know how to name it and how to get out.
Key Takeaways
- The hostage dynamic has two archetypes: an outsourced admissions team operating with zero transparency, and an internal admissions team that has siloed itself from ownership. Both share a transparency problem. Both are recoverable.
- The tell is usually a 5 to 6 month discovery timeline. It takes 120 days for the billing data to reveal that admits are not landing at the rate marketing spend should produce, and another month of internal investigation before the pattern crystallizes.
- The load-bearing variable in either archetype is account ownership. If your Google Ads account, your CRM, your call tracking, and your admissions team’s playbook all live outside your organization, you do not have a treatment center. You have a service contract that is monetizing your license.
- The fix is a system that does not rely on any one person or partner. Documented protocols, client-owned accounts, direct reporting cadence, and named accountability at every stage of the funnel. When the system is right, you can shut it down and turn it back on with any team you choose.
- Getting out of a hostage dynamic is possible but not free. Operators typically absorb another 60 to 90 days of transitional cost while the rebuild lands. That cost is measurable and finite. The cost of staying in the dynamic is not.
What “Hostage” Actually Means
DEFINITION
The Hostage Dynamic
An operational state in which a treatment center’s owner has lost direct control over the marketing-to-admissions funnel because a third party or an internal team holds all the authority: access to the accounts, ownership of the process, and information asymmetry that the owner cannot close on their own. The dynamic is not usually the result of malice. It is the result of an org chart that gave one party too much unchecked control over another party’s revenue.
I want to be careful about the framing here. Most third-party admissions services and most internal admissions teams are staffed by people trying to do the job well.
The hostage dynamic is not primarily about bad actors, though bad actors exist. It is about org-chart architecture that gives one party unchecked control over another party’s revenue.
When an owner outsources their admissions team to a third party that operates out of its own Google Ads accounts, its own CRM, and its own call tracking, the owner has structurally given up the ability to answer basic questions.
Which calls came in this week. What each caller said. Which VOBs were pulled. Which prospects converted to admits and which did not. Where the marketing spend went and what it produced.
Without those answers, the owner is dependent on the third party for every performance conversation. That dependence is the hostage. It is not always exploited. When it is exploited, the exploitation takes months to detect, because the operator has no independent data to compare against.
Archetype 1: The Outsourced Admissions Team
The most common version of the hostage dynamic is an outsourced admissions team operating as a black box. The owner pays a monthly fee, usually $30,000 to $80,000 depending on volume. The third party runs the phones, pulls VOBs, and reports monthly on admits.
The structural problem shows up when the third party is also running admissions for competing treatment centers. When a Cigna PPO call comes in, the third party is not just deciding whether this caller is a fit for your facility.
They are deciding which of their client facilities offers the best economics for that call.
If your facility pays the third party a certain rate per admit, and a competing facility pays double, the incentive is obvious. The Cigna PPO call goes to the competitor. You get the Medicaid callers.
Your admit rate drops. Your cost per admit rises. The third party’s monthly report shows fewer admits, and the explanation is always that the leads are the problem.
TRANSPARENCY IS THE LOAD-BEARING VARIABLE
If you cannot pull a call recording on demand, cannot audit your own Google Ads spend directly, cannot see every VOB pulled against your prospects, and cannot trace every admit back to its source campaign, you are not in a partnership with your admissions team. You are in a hostage dynamic. Get the transparency back before you decide whether to keep the relationship.
The behavior I described above is what patient-brokering law is designed to address at the federal level. The Eliminating Kickbacks in Recovery Act of 2018, codified at 18 U.S.C. § 220, established federal criminal penalties for payment-based referrals in behavioral health treatment.
The statute exists because the pattern is documented and widespread in the industry. Every operator working with an outsourced admissions team should understand it and should structure their contracts to require the transparency that surfaces the pattern early.
I am not accusing any specific third-party admissions team of unlawful behavior. What I am saying is that the operator has to design the relationship for transparency by default, because the operational structure otherwise creates the conditions for the pattern to develop.
Archetype 2: The Internal Team Gone Rogue
The second archetype is subtler and, in some ways, harder to detect. It happens inside the treatment center itself, when an internal admissions team develops a silo away from leadership.
The pattern usually has a leader and a small circle of allies. They control the phones, the CRM data entry, the call routing, and the coordinator training. Leadership does not have direct visibility into what is happening because the team resists any process change that would make their work legible.
The fear underneath the resistance is usually about replaceability. If leadership understands the exact protocol the team runs, if the CRM is properly configured, if the calls are recorded and reviewable, then the team members are no longer the sole holders of institutional knowledge.
They become replaceable. So the team resists the CRM. Resists the call recording. Resists the documented protocol. Resists the standardized reporting.
The result is the same as the outsourced version. The owner does not have the data to answer basic operational questions. The admits are what the team says they are. The cost per admit is opaque.
The relationship becomes adversarial when leadership pushes for accountability, because accountability threatens the team’s control.
I have seen this same dynamic play out in billing departments too. It is not unique to admissions. Any function that sits between marketing spend and revenue realization has the structural potential to develop a hostage dynamic when leadership gives it too much unchecked authority.
The Five to Six Month Discovery Timeline
~120 days
billing lag before the pattern shows up in the numbers
~30 days
typical internal investigation window after billing raises questions
Millions
typical revenue leakage during the discovery window at mid-size facilities
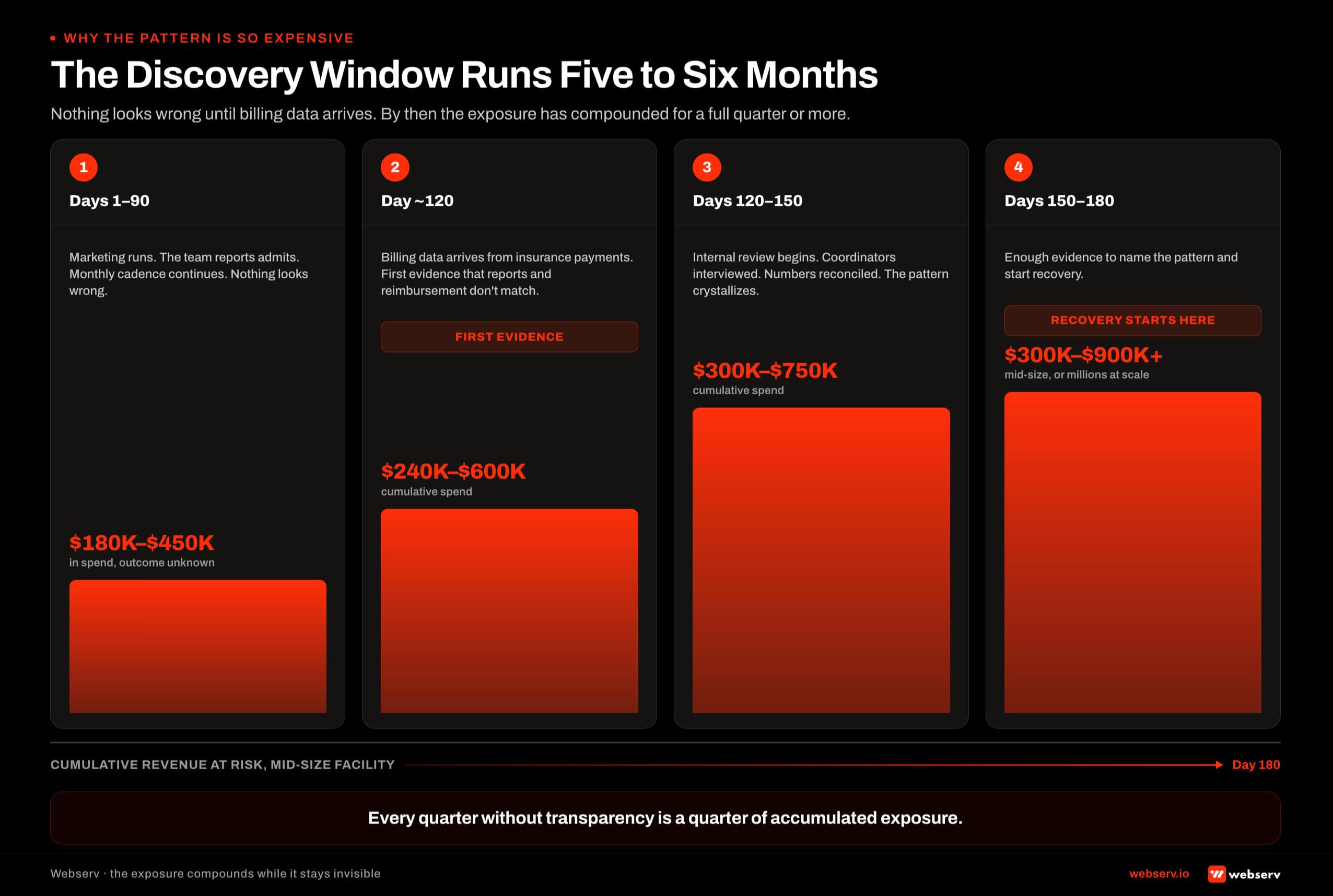 A four-phase timeline showing the 5 to 6 month discovery window before a treatment center owner can detect a hostage dynamic in their admissions team, with cumulative revenue at risk ranging from $180K in the first 90 days to $900K or more by day 180.
A four-phase timeline showing the 5 to 6 month discovery window before a treatment center owner can detect a hostage dynamic in their admissions team, with cumulative revenue at risk ranging from $180K in the first 90 days to $900K or more by day 180.The reason this pattern is so expensive is the discovery timeline. Nothing shows up immediately. The marketing runs. The admissions team reports admits. The monthly cadence continues.
The billing data starts to reveal the pattern about 120 days in, because that is the lag time between when treatment happens and when insurance actually pays.
When the payments come in and do not match the admissions team’s reported admit volume, the owner has the first evidence something is wrong.
Then it takes about another month of internal investigation before the pattern crystallizes. Questions get asked. Numbers get reconciled. Coordinators get interviewed. Eventually the owner has enough clarity to name what is happening.
By that point, five to six months have passed. On a mid-sized facility running $60,000 to $150,000 a month in paid media, that is anywhere from $300,000 to $900,000 of marketing spend that produced questionable admit outcomes.
On a larger operation, the number scales linearly with the spend. The revenue leak is often in the millions before the operator has enough evidence to act.
What Working Transparency Looks Like
WHAT SOVEREIGN ADMISSIONS OPERATIONS LOOK LIKE
- Google Ads, Meta Ads, GA4, and call tracking accounts are owned by the treatment center and administered by the agency
- CRM is owned and administered by the treatment center; the admissions team enters data but does not gate access
- Call recordings are accessible to operations leadership on demand, with 42 CFR Part 2 handling in place
- Weekly reporting reconciles marketing spend to specific admits by source, coordinator, and campaign
- Standard operating procedures for every stage of the admissions call are documented and version-controlled
WHAT HOSTAGE ADMISSIONS OPERATIONS LOOK LIKE
- Ad accounts are agency-owned or third-party-owned; the operator cannot access them directly
- CRM is opaque to leadership or exists outside the treatment center’s own systems
- Call recordings do not exist, or exist but are not accessible to leadership without asking
- Reporting is monthly, aggregated, and does not segment by coordinator or campaign
- Institutional knowledge lives in the heads of the current team; there is no written protocol
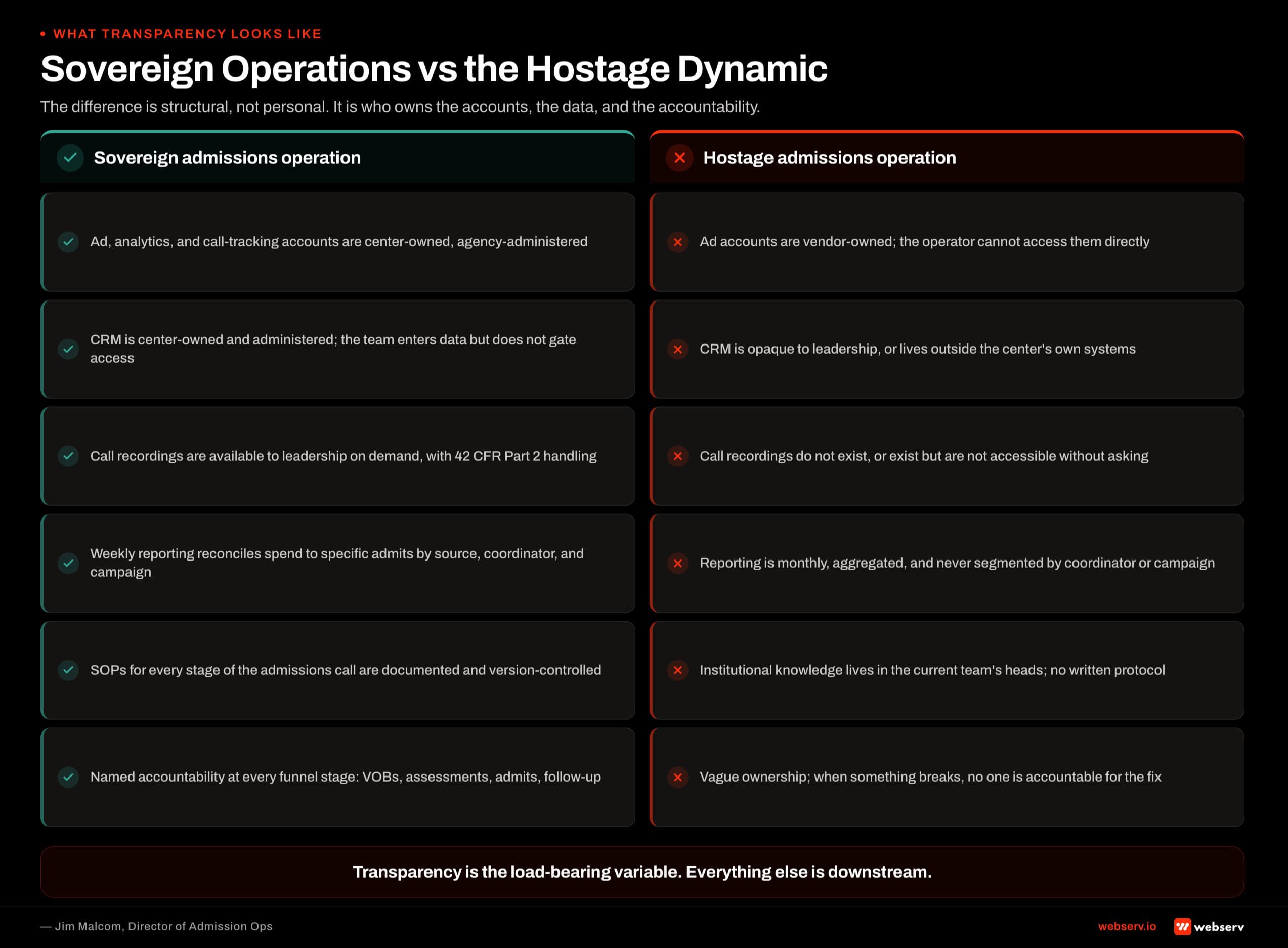 Six side-by-side comparisons showing what sovereign treatment center admissions operations look like versus what hostage admissions operations look like, account ownership, CRM access, call recording access, reporting depth, protocol documentation, and named accountability.
Six side-by-side comparisons showing what sovereign treatment center admissions operations look like versus what hostage admissions operations look like, account ownership, CRM access, call recording access, reporting depth, protocol documentation, and named accountability.The left column describes a treatment center that has structurally protected itself against the hostage dynamic. Even if a specific coordinator or vendor departs tomorrow, the operation continues.
The knowledge is in the documented process, not in the individuals. The data is in the client-owned systems, not in a third-party black box.
This is the state I try to move every engagement toward. It is what makes the treatment center sovereign over its own admissions function.
The Fix: A System, Not a Person
BUILD A SYSTEM THAT IS A MACHINE, NOT RELIANT ON ANY ONE PERSON OR VENDOR
You could shut it down and turn it back on with anybody. That is the goal of a properly-designed admissions operation. When the system carries the process, individual departures do not carry the process out the door with them.
The most successful admissions rebuild I have run involved a residential program that came to me in a hostile third-party admissions situation. They were down to a small handful of beds occupied, and the owner had been advised the facility was going to close.
In one week we hired a small internal team, brought the phones in-house under client-owned tracking, rebuilt the CRM configuration, documented the call protocol, and moved to weekly reporting reconciled against actual admits.
Over the following months, the facility grew from that near-closure state to substantially higher occupancy. The turnaround was not because of any one hire. It was because the structural transparency made the operation legible again.
The lesson from that engagement, and from every other successful admissions rebuild I have worked, is that the fix is not “find a better vendor” or “hire a better admissions director.” The fix is architectural.
Build the system so that no single vendor or director can hold the operation hostage. Then hire the right people to run the system.
The Five-Step Recovery Playbook
- Audit the Accounts. Who owns the Google Ads account? The Meta Ads account? The call tracking? The CRM? If the answer to any of these is “the agency” or “the admissions vendor,” start there. Client-owned accounts are non-negotiable before any other step happens.
- Access the Calls. Pull 90 days of call recordings. If they do not exist, that is the finding. If they exist but you cannot access them, that is also the finding. Listen to a random sample of 20 calls yourself. What you hear will tell you everything about the operation.
- Reconcile the Numbers. Compare what the admissions team reports for the last 90 days against what your billing shows. Same period. Same admits. If the numbers do not match, that gap is the leak. On a healthy operation the gap is under 5 percent, usually explained by insurance denials or accounting timing.
- Rebuild the Transparency. Move to client-owned accounts if you are not there already. Deploy the CRM with proper source-to-admit tracking. Move to weekly reporting reconciled to admits. Document the protocol. Every step of this is one you should own directly, not delegate.
- Rebuild the Team. Whether that is a new outsourced partner with better contractual transparency, or an in-house team, structure the relationship so the operation stays sovereign. Never sign a new contract that gives up account ownership or reporting transparency.
The recovery playbook takes 60 to 90 days to execute cleanly. It usually costs the treatment center an additional 60 to 90 days of transitional revenue impact while the rebuild lands. That cost is measurable and finite.
 The five sequential steps of the recovery playbook for treatment center owners in an admissions hostage dynamic: audit the accounts, access the calls, reconcile the numbers, rebuild the transparency, and rebuild the team.
The five sequential steps of the recovery playbook for treatment center owners in an admissions hostage dynamic: audit the accounts, access the calls, reconcile the numbers, rebuild the transparency, and rebuild the team.The cost of staying in the hostage dynamic is not. Operators who have been in it for a year at a mid-size facility are usually looking at $1 million to $3 million of foregone admit revenue. The rebuild pays back inside 60 to 120 days of stabilization.
What Not to Do
Getting out of a hostage dynamic is a delicate operation. There are several ways to do it wrong that make the situation worse.
Do not cut off the current team without a replacement running. The admits will stop entirely for as long as the transition takes. Overlap the current team and the new one for two to four weeks, even at higher cost, so you do not lose census during the transition.
Do not sign a new outsourced contract without transparency clauses. Client-owned accounts, on-demand call recording access, weekly reporting, and named accountability all belong in the contract. Any vendor unwilling to sign that language is telling you what the next 12 months will look like.
Do not rebuild the internal team without documented protocols first. Otherwise you are back in the same institutional-knowledge dependency, just with different individuals holding it. Write the protocol, then hire against the protocol.
Do not rush the account transfers. Google Ads account migration, CRM data migration, and call tracking transitions all have specific technical protocols. Rushing any of them can lose historical conversion data that took years to accumulate. Follow the migration protocols from each platform.
The industry-standard compliance frame for behavioral health provider transparency is worth understanding in this context. SAMHSA publishes guidance on ethical treatment operations and provides its own free National Helpline as a public reference point for standards of care. LegitScript’s certification requirements for treatment center advertisers also include transparency and disclosure standards.
When to Get Help
The hostage dynamic is one of the situations where an outside operator can accelerate the recovery. An outside partner brings the audit playbook, the transition protocols, and the transparency architecture that operators trying to do this alone often invent poorly.
It also gives the operator political cover with an internal team: the changes are being made because a third party recommended them, not because leadership is retaliating against specific individuals.
If you are reading this article and recognizing your own operation, the timeline for getting help matters. The sooner you start the rebuild, the smaller the revenue leak accumulates.
The longer you wait, the more the discovery timeline compounds. Book an intro meeting if you want to walk your current admissions setup with our team live.
Frequently Asked Questions
How can I tell if I am currently in a hostage dynamic?
The clearest single test is whether you can independently pull a call recording, an ad spend report, and a CRM extract for any 30-day period without asking your admissions team or your outsourced vendor for permission or delivery. If you can, you are in a healthy operational setup.
If you cannot, you are structurally exposed to the dynamic regardless of whether it is currently being exploited.
The secondary test is whether the last 90 days of billing revenue matches within 5 percent of what your admissions team reported for that same period. If the gap is larger, something is happening in the middle that you cannot see.
If both tests come back clean, you are likely operating in a sovereign structure. If either fails, start the audit playbook this week rather than next month.
Are outsourced admissions teams always risky?
No. Outsourced admissions teams can be a good fit for smaller treatment centers that do not have the volume to justify a full in-house team, or for operators who want to outsource the operational lift while retaining strategic oversight. What makes them risky is the contract structure and the transparency architecture.
An outsourced partner operating inside client-owned accounts, providing weekly reporting reconciled to admits, allowing on-demand call recording access, and providing named accountability at every funnel stage is a valid partnership. An outsourced partner operating outside all of that is a structural exposure regardless of their intentions.
The contract is the artifact. Get it right at the front of the relationship, or expect to be renegotiating it in six months from a position of weakness.
What if my current outsourced admissions vendor is a friend or long-time contact?
That relationship does not change the structural exposure. The hostage dynamic is architectural, not personal. Even a well-intentioned vendor operating without transparency infrastructure creates the conditions for revenue leakage over time.
The right move is to raise the transparency question directly. A vendor who has been operating in good faith will welcome the shift toward client-owned accounts and weekly reporting because it makes their good work legible to you. A vendor who resists the shift is telling you something about what they are protecting.
The conversation can be uncomfortable but is worth having early. Every quarter that passes without the transparency conversation is a quarter of accumulated exposure.
How much does a full admissions rebuild cost?
The direct cost typically runs $50,000 to $150,000 depending on facility size and the complexity of the transition. That covers audit, protocol design, CRM configuration, call tracking migration, admissions team hiring or retraining, and the 60 to 90 day stabilization window with an outside operator running the process.
The indirect cost is the transitional revenue impact. Most treatment centers see admits dip 15 to 25 percent for 60 days during the rebuild, then recover to a substantially higher run rate than the pre-rebuild baseline. The dip is real and needs to be planned for.
The math almost always works. Operators who complete the rebuild typically move from cost per admit in the $18,000 to $25,000 range to $10,000 to $14,000 within 120 days of stabilization. On a facility running 30 to 40 admits a month, that is $300,000 to $500,000 of monthly revenue improvement that pays back the rebuild several times over inside the first year.
Jim Malcom is the Director of Admission Ops at Webserv, a digital marketing agency for treatment centers.