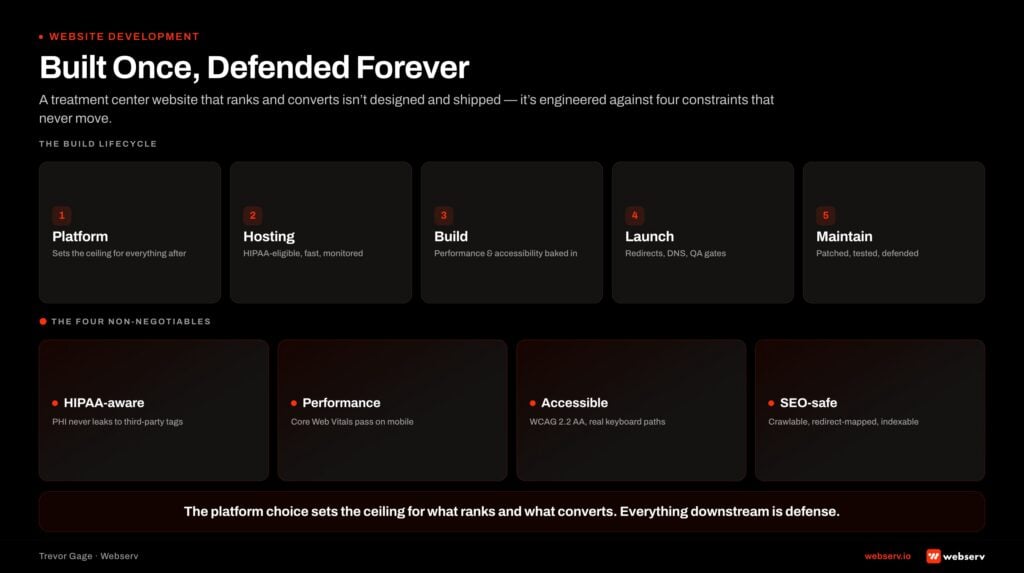
The biggest single lever on the cost-per-admission of a paid acquisition program for behavioral health is the landing page the traffic lands on. A high-converting page can take the same media spend and produce 3 to 6 times the admission calls of a generic page. Most rehab operators are running generic pages.
The pattern is consistent across the operators we audit: brand-team-built pages designed for a clinical director, not a family member in crisis. Phone numbers below the fold. Forms as the primary CTA. Stock photography. Generic compassionate-care copy. Each of these is a quiet conversion tax that the agency spreadsheets never quite explain.
This guide covers the architecture, creative, copy, trust signals, technical scaffolding, and tracking layers that separate a high-converting rehab landing page from a generic one. Here is what changes.
Key Takeaways
- The landing page is the single highest-ROI improvement available to most rehab paid media accounts. A 2x conversion rate lift cuts the cost per admit in half without changing a single line of bidding strategy or creative production.
- 70 to 85% of treatment center landing-page traffic is mobile. The page has to be designed mobile-first, with a sticky call button, sub-2-second LCP, and a hero that fits an iPhone screen before it fits a desktop browser.
- The phone call is the primary conversion event, not the form fill. Phone-primary landing pages in this category convert at 2 to 3 times the rate of form-primary pages on paid social traffic. The form is a backup for visitors who cannot call.
- Confidentiality assurance above the fold is the single most underused conversion lever. Five sentences explaining that the call is private, the facility does not contact employers or insurance carriers without permission, and admissions counselors are clinicians, not salespeople.
- HIPAA-compliant tracking is non-negotiable. Standard Meta pixel, standard GA gtag, and third-party retargeting tags without BAAs transmit data patterns that have triggered HHS OCR investigations. The tracking stack runs through a HIPAA-compliant intermediary with a signed BAA.
The landing page is where most rehab paid media spend gets wasted. The campaign delivers the click. The page burns it. Most treatment center landing pages were built for the brand team, not the family member in crisis. They look polished. They convert at 2%.
A landing page built for the actual visitor (a family member, on mobile, in a moment of decision, with no patience for marketing copy) converts at 6% to 12%. Same media spend. Three times the admissions calls. The math is not subtle.
The landing page is the single highest-ROI improvement available to most rehab paid media accounts. A 2x conversion rate lift cuts the cost per admit in half without changing a single line of bidding strategy or creative production.
Mitch Marowitz, Director of Paid Media, Webserv
This guide is the operator-facing version of how we build and audit landing pages for treatment center clients at Webserv. It is written from the paid media seat, which means the orientation is conversion outcomes over design aesthetics. A landing page in this vertical is a conversion machine that happens to be a webpage. The job is to convert. Everything else is constraint.
The 14 sections below cover what makes rehab landing pages different from any other category, the mobile-first reality the data demands, the architecture, what belongs above the fold, the trust signal stack, and the confidentiality framing operators consistently underuse.
Then: call versus form versus hybrid CTAs, form design when forms are necessary, insurance verification widgets, copy approach, below-the-fold trust builders, page speed and Core Web Vitals, the HIPAA tracking layer that lives on the page itself, the common mistakes we audit and see repeated, and the measurement framework that tells you whether the page is actually working.
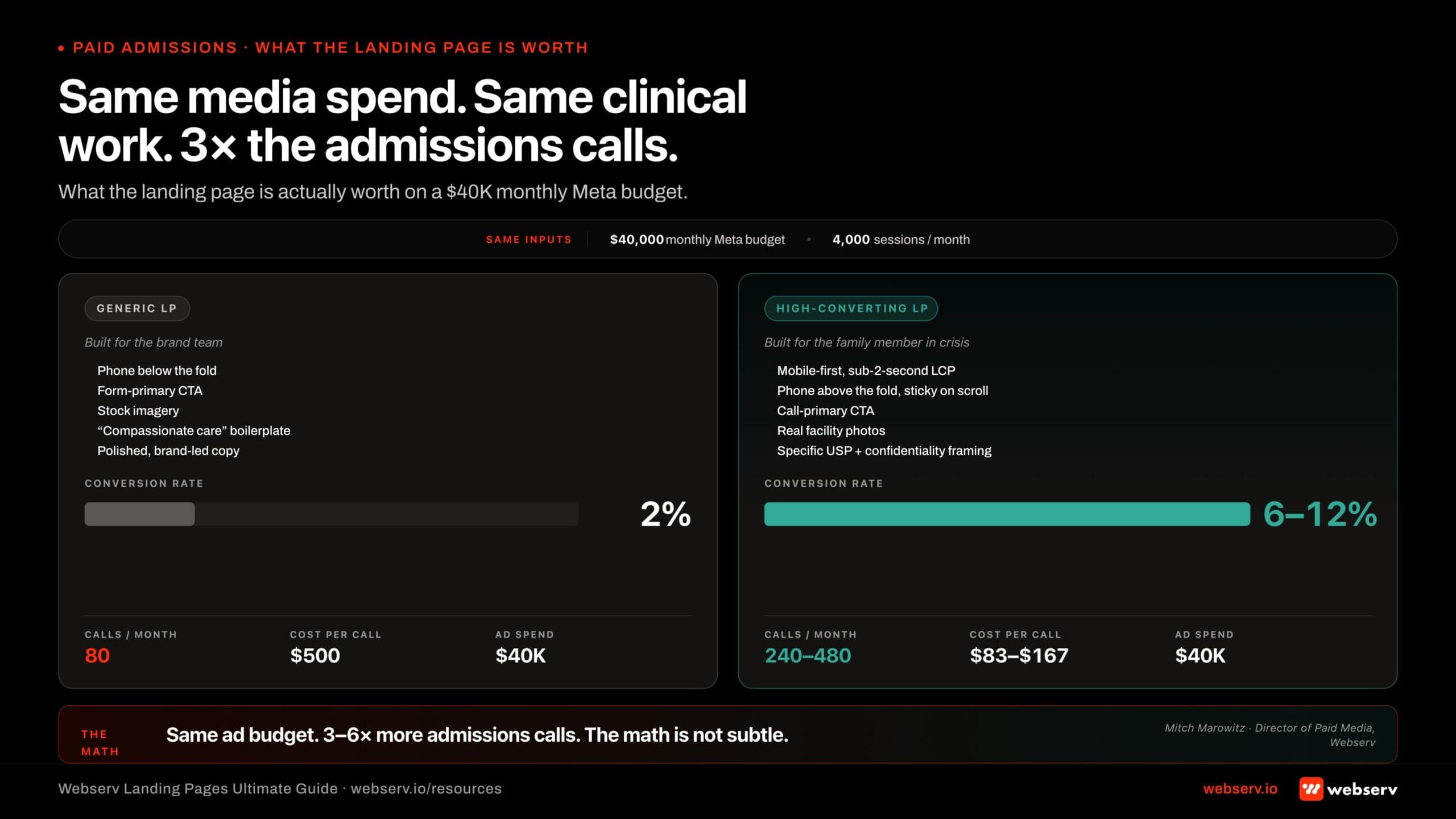 Infographic titled ‘Same media spend. Same clinical work. 3x the admissions calls.’ Side-by-side comparison of a generic rehab landing page converting at 2% versus a high-converting page at 6-12% on the same $40,000 monthly paid media spend. The generic page (built for the brand team, polished, phone below the fold, form-primary CTA, stock imagery, generic ‘compassionate’ copy) produces 80 calls per month at $500 cost-per-call. The high-converting page (built for the family member in crisis, mobile-first, sticky phone above the fold, call-primary CTA, real facility photos, specific USP with confidentiality framing) produces 240-480 calls at $83-$167 cost-per-call. Visual headline: 3-6x more admissions calls on the same ad budget.
Infographic titled ‘Same media spend. Same clinical work. 3x the admissions calls.’ Side-by-side comparison of a generic rehab landing page converting at 2% versus a high-converting page at 6-12% on the same $40,000 monthly paid media spend. The generic page (built for the brand team, polished, phone below the fold, form-primary CTA, stock imagery, generic ‘compassionate’ copy) produces 80 calls per month at $500 cost-per-call. The high-converting page (built for the family member in crisis, mobile-first, sticky phone above the fold, call-primary CTA, real facility photos, specific USP with confidentiality framing) produces 240-480 calls at $83-$167 cost-per-call. Visual headline: 3-6x more admissions calls on the same ad budget.Part 1. Why rehab landing pages are different
A high-converting treatment center landing page is not a brand exercise. It is a specific operational layer of the paid acquisition program: a single screen, on a phone, viewed by a family member in crisis, designed to produce a phone call within 90 seconds. Every choice in the design either shortens that path or lengthens it.
Three constraints shape rehab landing page design in ways that do not apply to other categories.
The visitor is in crisis. The family member arriving on the page just searched “alcohol rehab near me” because their spouse is in the next room and the situation has gotten worse. The visitor has zero patience for clever copy, brand storytelling, or three-screen scrolls before the call button appears. Every element on the page either serves the next call or gets in the way of it.
The conversion is a phone call, not a form fill. Treatment center traffic skews toward calling, not filling out forms. The family member wants to talk to a person, not click through a contact form. Landing pages designed around form-fill primacy underconvert in this category. The phone number is the primary CTA. The form is the backup for visitors who cannot call from where they are sitting.
HIPAA-adjacent constraints govern the tracking. Standard analytics pixels, retargeting tags, and CRM integrations that would be fine on an ecommerce landing page are non-compliant on a rehab landing page. The tracking stack has to be built around a HIPAA-compliant intermediary with a signed BAA, which constrains what data flows where. Operators who skip this expose the facility to HIPAA liability.
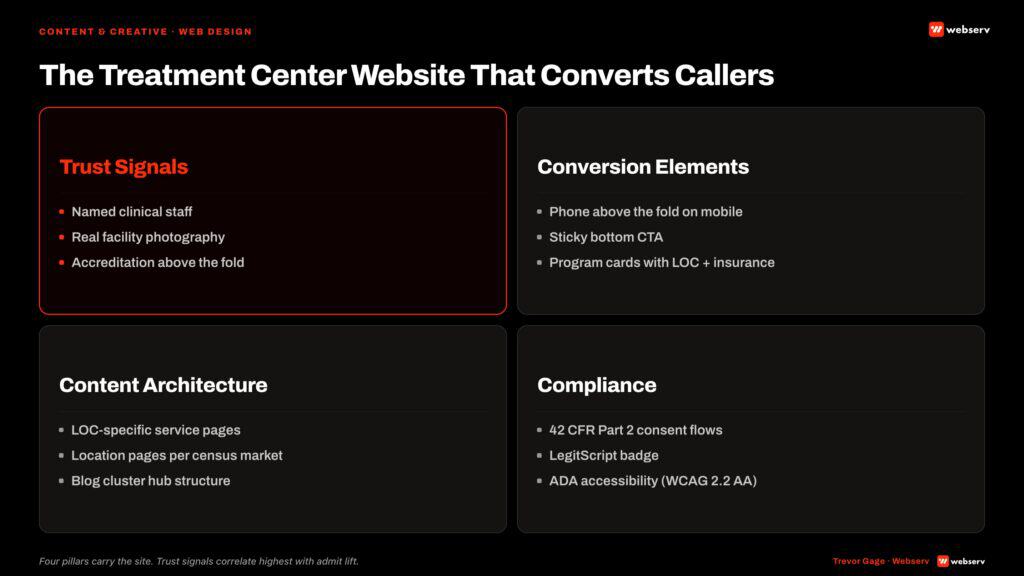
Those three constraints produce a landing page that looks fundamentally different from a typical SaaS or ecommerce LP. Phone number above the fold. Confidentiality language above the fold. Insurance verification prominently offered. Trust signals (Joint Commission seal, named medical director, payer contracts) before the visitor scrolls. Form fields stripped down to the minimum necessary to qualify and route the lead. Tracking architecture that does not transmit PHI to ad platforms.
Part 2. The mobile-first reality
Mobile traffic is roughly 65% of all website visits in 2026 and is consistently higher on rehab paid media because Meta paid social pushes 98% mobile and Google paid search skews mobile in this vertical. For most treatment center landing pages, 70% to 85% of incoming traffic is on a phone.
The mobile-first design constraints connect directly to the broader treatment center web design discipline and the conversion mechanics covered in our conversion tracking guide. Landing pages live inside the broader website system; design choices that work in isolation can fail when the site’s navigation, header treatment, or trust signals are inconsistent with the landing page itself.
The conversion gap is widening. Mobile traffic converts at 1.82% across categories in 2026. Desktop converts at 3.14%. The mobile-desktop gap was 38% in 2024 and is now 42%. For treatment centers, the mobile underconversion is usually a landing-page-design problem rather than a traffic-quality problem. The desktop version of the page works. The mobile version has the same content rendered worse on a small screen with slower load times.
The fix is to design mobile-first and let desktop be the secondary surface. Concrete implications:
The call button stays visible during scroll on mobile. A floating call button (or a sticky header with the phone number) keeps the conversion path one tap away no matter where the visitor is on the page.
The hero block has to render at the right size on a phone before it is allowed to look right on desktop. Most rehab landing pages are designed in a desktop browser and squeezed onto mobile. The result is a hero that fits on desktop and pushes the call button below the fold on iPhone 14.
The form, if there is one, has to be thumb-navigable. Five fields stacked vertically with autofill-friendly inputs. Not 12 fields in a multi-column layout that requires pinch-and-zoom on mobile.
Page weight has to stay low. Mobile carriers and patchy WiFi connections in family-member homes are not delivering the same load speeds as office desktops. A 4-second LCP on mobile loses 25% to 40% of family-member traffic before the page renders.
Part 3. Page architecture
The standing architecture for a treatment center landing page is six sections in order. The order is not flexible. The family member’s questions answer in a specific sequence.
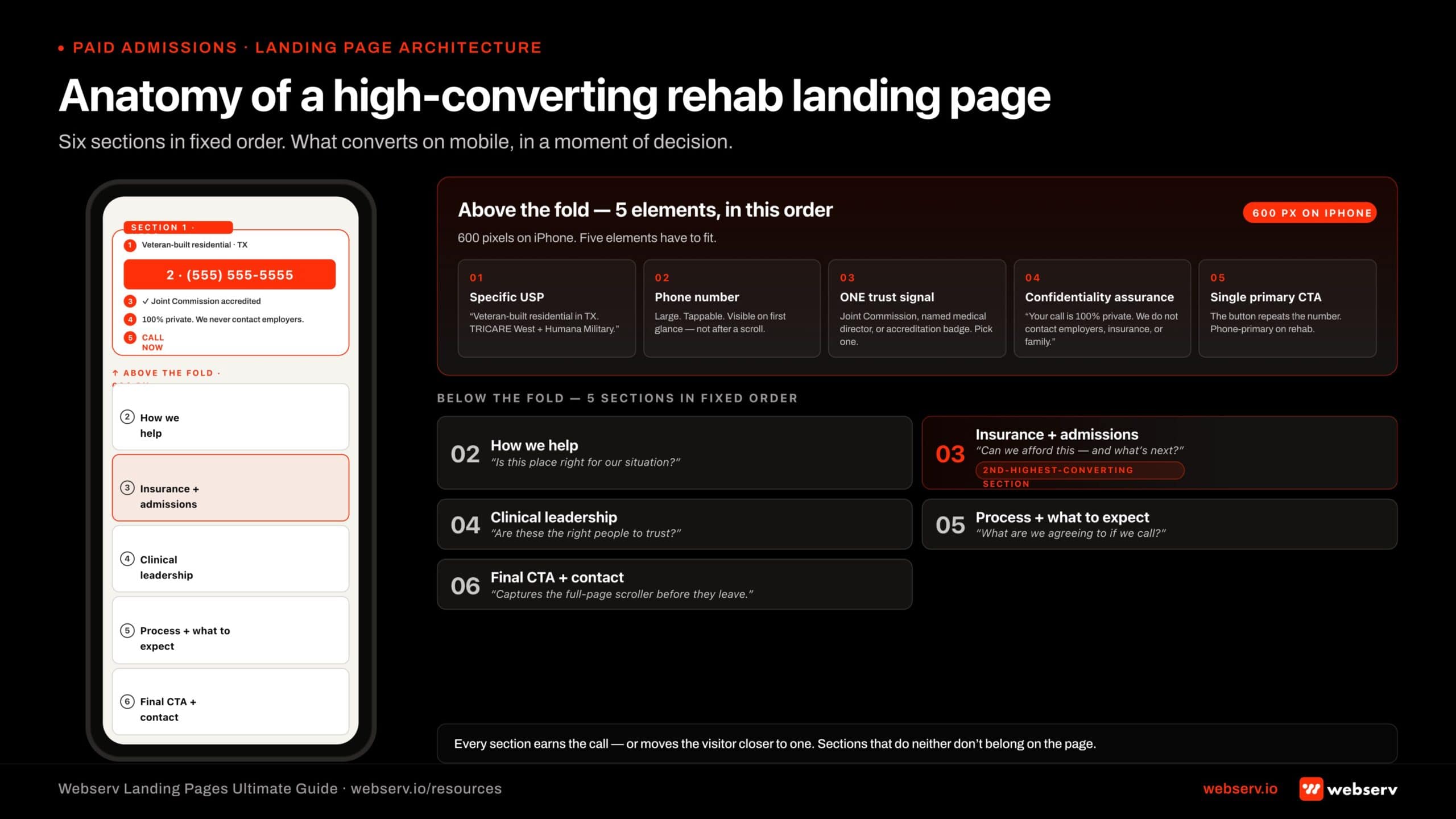 Infographic titled ‘Anatomy of a high-converting rehab landing page.’ Annotated mobile mockup showing the six-section architecture of a treatment center landing page. The above-the-fold zone (sized to approximately 600 pixels on iPhone) shows the five required elements: a specific unique selling proposition (example: ‘Veteran-built residential in TX with TRICARE West, Humana Military, VA CCN Region 1 coverage’), a large tappable phone number, one trust signal (Joint Commission seal, named medical director, or accreditation badge), a one-sentence confidentiality assurance, and a single primary CTA. Below-the-fold sections in order: Section 2 ‘How we help’ (answers ‘Is this place right for our situation?’); Section 3 ‘Insurance and admissions’ (the second-most-converting section, answers ‘Can we afford this and what is next?’); Section 4 ‘Clinical leadership’ (answers ‘Are these the right people to trust?’); Section 5 ‘Process and what to expect’ (answers ‘What are we agreeing to if we call?’); Section 6 ‘Final CTA’ (captures the full-page scroller). Footer pull-quote: ‘Every section earns the call or moves the visitor closer to one. Sections that do neither do not belong on the page.’
Infographic titled ‘Anatomy of a high-converting rehab landing page.’ Annotated mobile mockup showing the six-section architecture of a treatment center landing page. The above-the-fold zone (sized to approximately 600 pixels on iPhone) shows the five required elements: a specific unique selling proposition (example: ‘Veteran-built residential in TX with TRICARE West, Humana Military, VA CCN Region 1 coverage’), a large tappable phone number, one trust signal (Joint Commission seal, named medical director, or accreditation badge), a one-sentence confidentiality assurance, and a single primary CTA. Below-the-fold sections in order: Section 2 ‘How we help’ (answers ‘Is this place right for our situation?’); Section 3 ‘Insurance and admissions’ (the second-most-converting section, answers ‘Can we afford this and what is next?’); Section 4 ‘Clinical leadership’ (answers ‘Are these the right people to trust?’); Section 5 ‘Process and what to expect’ (answers ‘What are we agreeing to if we call?’); Section 6 ‘Final CTA’ (captures the full-page scroller). Footer pull-quote: ‘Every section earns the call or moves the visitor closer to one. Sections that do neither do not belong on the page.’Section 1: Hero. Unique selling proposition. Trust signal stack. Phone number. Confidentiality assurance. The hero does most of the conversion work. Visitors who do not call from the hero either fall off or scroll for more information before calling.
Section 2: How we help. Plain-language summary of what the program does. Levels of care, populations served, key differentiators. This section answers “is this place right for our situation?”
Section 3: Insurance and admissions. Insurance verification widget, accepted payers, admissions process explanation. This section answers “can we afford this and what happens next?” It is the second-most-converting section after the hero.
Section 4: Clinical leadership and credentials. Named medical director with credentials. Clinical team overview. Accreditations (Joint Commission, state license, CARF if applicable). This section answers “are these the right people to trust with our family member?”
Section 5: Process and what to expect. Step-by-step admissions walkthrough. What happens on the first call. What the first 24 hours look like. This section answers “what are we agreeing to if we call?”
Section 6: Final CTA and contact. Phone number repeated. Backup form. Address (if appropriate). 24/7 admissions assurance. This section captures the visitor who scrolled the full page before deciding to act.
Every section either earns the call or moves the visitor closer to making one. Sections that do neither do not belong on the page.
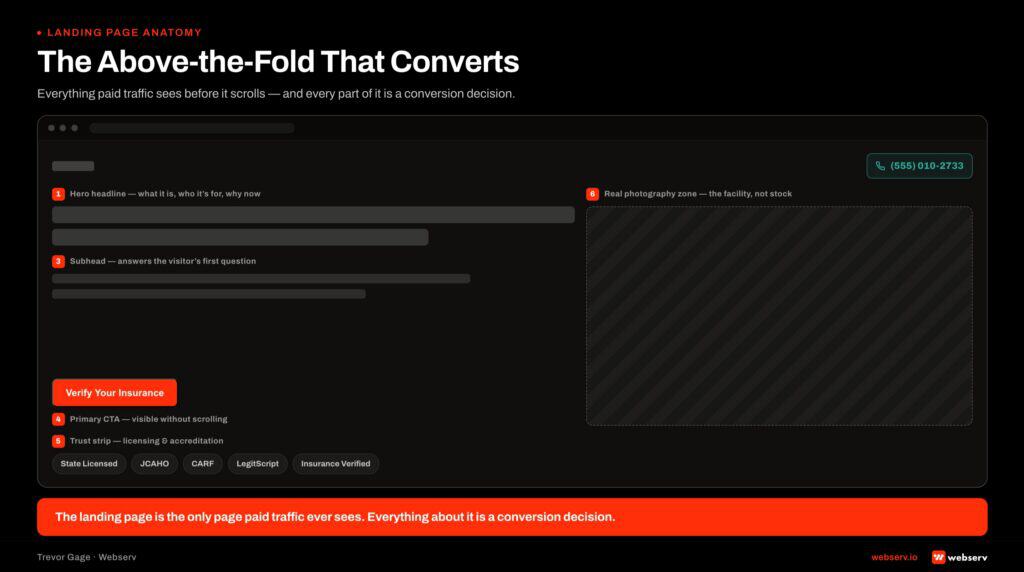
Part 4. What belongs above the fold
Above the fold on mobile is roughly 600 pixels of vertical space on a standard iPhone. Five elements have to fit:
The unique selling proposition. What makes this facility different. Specific, not generic. “Veteran-built residential program in Texas with TRICARE West, Humana Military, and VA CCN Region 1 coverage.” Not “Compassionate, individualized addiction treatment.” The specific UVP gives the family member the right reason to keep reading. The generic UVP fails the visitor’s first scan.
The phone number. Visible, large, and tappable. Most treatment center mobile traffic converts on a call. Burying the phone number below the hero is the most common conversion-rate killer we audit.
A trust signal. One. Not five. The Joint Commission seal, OR the named medical director with credentials, OR an accreditation badge. The trust signal that fits in the space available, picked for the audience. For a clinical-anxious family member, the medical director credential lands strongest. For an insurance-anxious caller, the payer list lands strongest. Test both.
The confidentiality assurance. A short, one-sentence statement that calls are private and the facility does not contact employers, family members, or insurance carriers without permission. This is the single most underused conversion element on rehab landing pages. Family members hesitate to call because they assume confidentiality is uncertain. Saying so removes the hesitation.
The primary CTA. A “Call Now” or “Verify Insurance” button. Single CTA, not three. Multiple CTAs above the fold dilute the next action. Pick one and run it.
Below the fold is the rest of the architecture. Above the fold is the conversion event happening or not happening within 3 seconds of page load.
Part 5. The trust signal stack
Trust signals do more conversion work on a rehab landing page than on almost any other category page. The visitor is making a decision about clinical care for a family member in crisis. Trust is the gating question.
Trust signal placement is the highest-leverage decision below the fold on a rehab landing page. The patterns below build on our healthcare advertising compliance overview and on the marketing agency rankings we publish — operators who fail at trust signal stacking typically have the underlying credentials and just have not made them visible on the conversion surface.
 Infographic titled ‘6 trust signals ranked by conversion impact for rehab landing pages.’ Vertical ranked stack of six trust signals on a treatment center landing page, ordered by conversion impact rather than by what looks good. Rank 1 (highest impact): Joint Commission accreditation, the most recognized seal in healthcare, belongs above the fold. Rank 2: Named medical director with credentials such as Dr. Jane Smith, PhD, LMFT, with bio, photo, and one-sentence positioning. Rank 3: Payer contracts and insurance acceptance (example: ‘In-network with Aetna, BCBS, Cigna, United, Humana’), answers the second-most-asked question after ‘is this the right place’. Rank 4: State license number, family members rarely verify but presence signals the facility is willing to be checked. Rank 5: Years in operation, tenure correlates with trust, newer facilities should emphasize clinical leadership instead. Rank 6: Outcome data only if defensible, with the FDA’s 30 warning letters in March 2026 and FTC enforcement making outcome claims expensive to get wrong. Bottom callout: ‘Above the fold, pick ONE. Multiple trust signals above the fold dilute each other.’
Infographic titled ‘6 trust signals ranked by conversion impact for rehab landing pages.’ Vertical ranked stack of six trust signals on a treatment center landing page, ordered by conversion impact rather than by what looks good. Rank 1 (highest impact): Joint Commission accreditation, the most recognized seal in healthcare, belongs above the fold. Rank 2: Named medical director with credentials such as Dr. Jane Smith, PhD, LMFT, with bio, photo, and one-sentence positioning. Rank 3: Payer contracts and insurance acceptance (example: ‘In-network with Aetna, BCBS, Cigna, United, Humana’), answers the second-most-asked question after ‘is this the right place’. Rank 4: State license number, family members rarely verify but presence signals the facility is willing to be checked. Rank 5: Years in operation, tenure correlates with trust, newer facilities should emphasize clinical leadership instead. Rank 6: Outcome data only if defensible, with the FDA’s 30 warning letters in March 2026 and FTC enforcement making outcome claims expensive to get wrong. Bottom callout: ‘Above the fold, pick ONE. Multiple trust signals above the fold dilute each other.’The trust signals that actually move conversion rate, in order of impact:
Joint Commission accreditation. The single most recognized accreditation in healthcare. Family members may not understand what it means technically, but they recognize the seal and read it as institutional legitimacy. The seal belongs above the fold or in the first visible section below it.
Named medical director with credentials. A real person with real letters after their name. Dr. Jane Smith, PhD, LMFT. The named professional creates accountability and clinical credibility in a way that “our team of experts” never does. The bio with photo, credentials, and a one-sentence positioning statement.
State license number. The state-issued treatment provider license number, displayed in the trust section. Family members rarely verify it independently, but its presence signals the facility is willing to be checked.
Payer contracts and insurance acceptance. “In-network with Aetna, BCBS, Cigna, United, and Humana.” For out-of-network programs: “Out-of-network coverage accepted. Most PPO plans cover treatment at our facility.” The insurance signal answers the second-most-asked question after “is this the right place” and shapes whether the family member calls at all.
Years in operation. “Treating families since 2008.” Tenure correlates with trust. Newer facilities should not invent tenure but should emphasize the credentials of the clinical leadership instead.
Outcome data, if defensible. This category gets sensitive after the FDA’s 30 warning letters to substance use treatment providers in March 2026. Outcome claims have to be evidence-backed and FTC-compliant. “85% of alumni report sustained sobriety at one-year follow-up based on internal survey data, N=200, conducted Q1 2025” works. “85% sobriety rate” without evidence does not.
The order matters. Joint Commission first because the visual recognition is highest. Medical director second because the named professional creates the strongest trust handshake. Insurance signal third because it gates whether the call happens at all.
Part 6. The confidentiality framing operators underuse
Confidentiality is the single most underleveraged conversion lever on rehab landing pages. We audit dozens of treatment center sites where confidentiality is mentioned in a footer paragraph nobody reads, if it is mentioned at all.
The family members who hesitate to call hesitate for one of three reasons. They assume the facility will contact the patient’s employer. They assume the facility will tell the insurance carrier and the rate will go up. They assume the family member’s name or the patient’s name will end up on a list somewhere.
All three concerns are addressable with one paragraph of clear language. Operators who put that paragraph above the fold pick up family-member calls that would not have happened otherwise.
The framing we recommend:
Your call is 100% confidential. We do not contact your employer, your insurance company, or any family member without your explicit permission. Our admissions counselors are clinicians, not salespeople. The conversation is private and at no obligation.
Five sentences. Above the fold or in the first section. The paragraph is short enough to read in three seconds and direct enough to remove the specific hesitations the visitor is carrying.
Test the confidentiality framing across populations. Family-member-focused programs may benefit from emphasizing the patient’s privacy. Adolescent-focused programs may benefit from emphasizing the parent’s discretion. The base framing is the same. The emphasis adjusts by audience.
Part 7. Call versus form versus hybrid CTAs
The biggest CTA decision is whether the primary action is a phone call, a form fill, or a hybrid. The right answer in treatment center marketing is overwhelmingly the phone call, with form fills as a backup channel for visitors who cannot call.
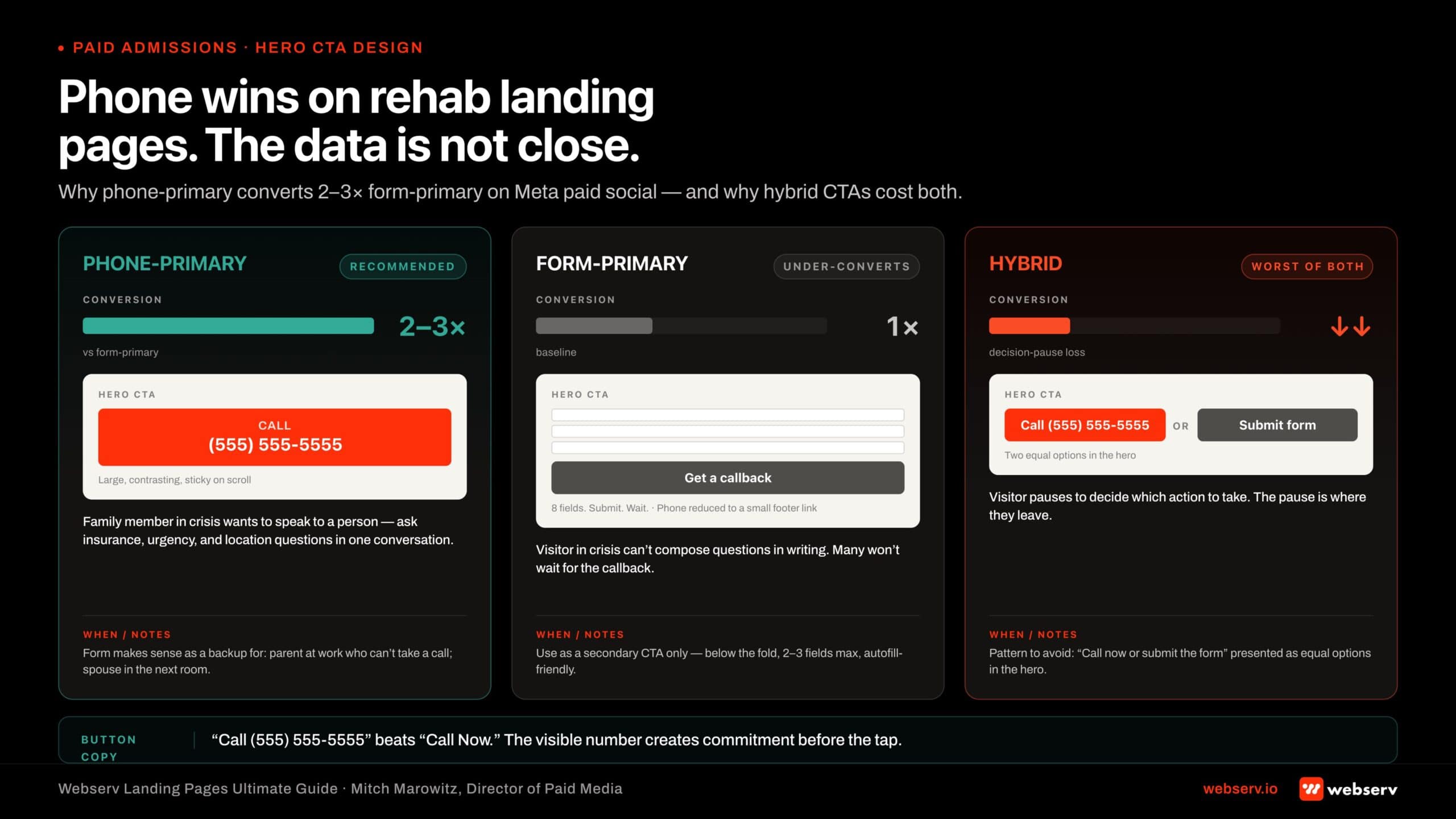 Infographic titled ‘Phone wins on rehab landing pages. The data is not close.’ Three-column comparison of CTA strategies for treatment center landing pages: phone-primary (recommended), form-primary (under-converts), and hybrid (worst of both). Phone-primary column shows a large click-to-call button design with the actual phone number visible (Call 555-555-5555), large, contrasting color, sticky on scroll, and converts at 2 to 3 times form-primary on Meta paid social traffic. The form-primary column shows an 8-field form as the hero CTA, which fails because visitors in crisis cannot compose questions in writing and many will not wait for callbacks. The hybrid column shows ‘Call OR Submit form’ presented as equal options, which fails because visitors pause to decide which action to take and the pause is where conversion drops. Notes when the form makes sense as backup: a parent at work who cannot take a private call, a spouse with the patient in the adjacent room. Bottom callout: ‘Button design: Call (555) 555-5555 beats Call Now. The visible number creates commitment before the tap.’
Infographic titled ‘Phone wins on rehab landing pages. The data is not close.’ Three-column comparison of CTA strategies for treatment center landing pages: phone-primary (recommended), form-primary (under-converts), and hybrid (worst of both). Phone-primary column shows a large click-to-call button design with the actual phone number visible (Call 555-555-5555), large, contrasting color, sticky on scroll, and converts at 2 to 3 times form-primary on Meta paid social traffic. The form-primary column shows an 8-field form as the hero CTA, which fails because visitors in crisis cannot compose questions in writing and many will not wait for callbacks. The hybrid column shows ‘Call OR Submit form’ presented as equal options, which fails because visitors pause to decide which action to take and the pause is where conversion drops. Notes when the form makes sense as backup: a parent at work who cannot take a private call, a spouse with the patient in the adjacent room. Bottom callout: ‘Button design: Call (555) 555-5555 beats Call Now. The visible number creates commitment before the tap.’Why calls outperform forms in this category. The family member is in crisis. They want to speak to a person. They want to ask insurance questions, urgency questions, location questions, and clinical questions in one conversation. A form requires them to compose their questions in writing, wait for a callback, and stay available when the callback comes. Many will not.
The conversion data is unambiguous. Phone-primary landing pages in treatment center marketing convert at 2 to 3 times the rate of form-primary landing pages on Meta paid social traffic.
When the form makes sense as a backup. Visitors who cannot call from where they are sitting (a parent at work who cannot make a private call from their desk, a spouse with the patient in the next room). The form should be one or two fields (name, phone number) with no qualifying questions. The faster the form, the more it captures.
Why hybrid CTAs underperform. “Call Now or Fill Out the Form” presented as equal options dilutes the primary action. The visitor pauses to decide. The pause is where the conversion drops. The right pattern is the phone number as the primary CTA with a smaller secondary form below the fold for the visitors who scroll past the call.
The call button design. Large, contrasting color, sticky on scroll, and the button text is “Call (555) 555-5555” with the actual number visible. “Call Now” as a button label is weaker than “Call (555) 555-5555” because the visible number creates commitment before the tap.
The phone number tracking. Every landing page needs a unique tracking number routed through CallRail or CallTrackingMetrics. The tracking number lets you attribute calls back to source, campaign, ad set, and creative. Without it, the entire upstream measurement stack is blind to half of conversion events.
How Profound Treatment drove 31 admits and a 42% drop in cost per viable in one quarter
Broad match pivot, negative keyword management, and intake-level conversion tracking turned a fragmented paid strategy into a predictable admissions engine.
Read the case study →68 viable VOBs at $4,529 cost per viable
Part 8. Form design when forms are necessary
The form is the secondary CTA on a rehab landing page, but it still has to be designed correctly because the visitors who use it tend to be the ones who could not call. The form has to capture them in one shot.
Field count. The minimum number of fields that lets the admissions team route the lead. For most operators, that is three fields: name, phone number, and preferred contact time. Email is optional because most admissions teams call rather than email. Insurance, location, and condition are all post-form qualifying questions handled on the callback.
Multi-step versus single-step. Multi-step forms convert higher than single-step forms in this category when the first step is the lightest possible commitment. Step 1: name and phone. Step 2: a single qualifying question (insurance carrier or location). Step 3: submit. The visitor commits to step 1 and rarely abandons before step 3.
Autofill. Every form field needs to be configured for browser autofill. Family members on mobile do not want to type. They want to tap autofill and submit. The autofill configuration is a 10-minute tag setup that materially improves mobile form conversion.
Submit button language. “Get Help Now” or “Speak With an Admissions Counselor” outperforms generic “Submit” or “Send.” The submit button language reinforces the conversion outcome, which lowers last-second abandonment.
Trust signals near the form. A short confidentiality line directly under the form button. “Your information is private. We will call you within 1 hour, never contact your employer, and never share your data.” The same content that lives in the hero needs to be reinforced at the form because the visitor’s anxiety is highest at the moment of submission.
Error handling. Field validation that catches mistakes in real time and helps the visitor fix them. Hard error states that block submission without explaining the issue lose visitors at the last possible moment.
Part 9. Insurance verification widgets
The insurance question is the single most-asked question family members have when calling a treatment center. Addressing it directly on the landing page converts visitors who would otherwise call competitors to compare.
VOB widgets connect to the billing operation downstream — operators running this widget without alignment to their VOB workflow typically generate friction at the admissions handoff. The widget is a marketing surface, not a billing tool; the data flow into intake has to be wired before the widget goes live.
The simple version: insurance list and verification CTA. A short list of accepted payers with a “Verify Your Insurance” button that opens a form or initiates a call routing flow. Works for most operators.
The widget version: real-time insurance verification. Integrations with vendors like InsuranceAble, Verisys, or built-in admissions software widgets that let the visitor enter their insurance information and get a real-time pre-verification response. Higher conversion rate but requires technical infrastructure, HIPAA-compliant data handling, and a clear consent flow.
The widget version converts at 2 to 3 times the call-based insurance verification path because it gives the visitor an immediate answer to their primary question without requiring them to call. The conversion happens before the family member ever speaks to admissions.
HIPAA considerations on insurance verification widgets. Insurance information is PHI. The widget cannot transmit member IDs, dates of birth, or insurance details through standard analytics tags. The data flow has to run through a HIPAA-compliant intermediary with a signed BAA. The vendors named above are HIPAA-compliant by default, but the implementation has to be reviewed by counsel.
What to avoid on insurance verification. Asking for insurance information before the visitor knows what they are getting. The widget should appear after the visitor has read the hero and the trust signals, not as the entry point. Visitors who land on an insurance question before they know who the facility is bounce at high rates.
Part 10. Copy approach
The copy on a rehab landing page does as much work as the design. The right copy speaks to the family member, in plain language, about the specific question they have at each point in the page.
Family-member voice, not patient voice. The family member arrived on the page. Address them. “When your husband told you he needed help, you were not sure what to do next. We are.” beats “Are you struggling with addiction?” The second-person diagnostic frame is also a Meta self-harm classification trigger, which makes it bad for both the platform and the visitor. Our compliant ad headlines work covers the same pattern on the Meta and Google ad copy side.
Process explainer language. The most-asked question after “what is the cost” is “what happens next.” Spell out the process. “When you call, an admissions counselor will speak with you for 15 to 20 minutes about your situation. We will run a free insurance verification while we are on the call. If we are the right fit, we can have your family member admitted within 24 hours.” Specific, sequential, low-anxiety.
Plain language, not clinical jargon. “Residential treatment” beats “inpatient milieu therapy.” “Detox” beats “medically supervised acute withdrawal management.” The family member does not have the vocabulary the clinical team has. The landing page should not require them to learn it.
Short sentences. Crisis readers do not parse long sentences well. Shorter is better. Two-line paragraphs. Sentence fragments where they read naturally.
Trust language without overpromising. “Most insurance accepted” is defensible. “100% acceptance rate” is not. “Most clients complete treatment” is defensible if you have the data. “85% success rate” is not without published evidence. The FTC enforcement environment in 2026 makes outcome claims expensive to get wrong.
Avoidance list. Inspirational stock language (“Hope is here,” “Begin your journey”). Aggressive sales language (“Don’t wait another day”). Pity language (“You don’t have to suffer alone”). Each of these reads as marketing copy to the family member and produces immediate skepticism. The replacement is operator-direct, plain, and specific.
Part 11. Below-the-fold trust builders
The visitor who scrolls past the hero is asking a deeper version of the trust question. The below-the-fold trust builders are designed for that visitor.
Clinical team page section. Bios of the medical director, the clinical director, and one or two named clinicians. Photo, credentials, one-sentence positioning. Family members reading this section are doing due diligence on whether the clinical team is real and qualified.
Facility imagery. Real photos of the actual facility, not stock imagery. Family members can usually tell the difference, and the real facility imagery produces a meaningful conversion lift over generic clinical stock. Show the bedrooms, the common areas, the outdoor space, the dining area. Show the clinical team in real settings.
Accreditation and licensing detail. A section that explains what Joint Commission accreditation means, what the state license covers, and any additional accreditations (CARF, ASAM affiliation, AAAP membership). Family members who scroll this far want to understand the credentials beyond the seal in the hero.
Process walkthrough with timing. “Within 24 hours of your call: insurance verified, bed reserved, intake coordinated.” This section reduces the visitor’s uncertainty about timeline, which is a frequent source of last-mile hesitation.
Alumni stories or family testimonials. HIPAA-compliant and FTC-compliant. The alumni story has to be produced with full consent and disclosed if any compensation was involved. Done correctly, alumni stories produce strong below-the-fold conversion lift.
FAQ section. The 10 to 15 questions family members consistently ask, answered in two to three sentences each. Insurance coverage. Length of stay. Family involvement. Confidentiality. What to bring. What happens after. The FAQ section catches visitors with specific remaining objections.
Part 12. Page speed and Core Web Vitals
Page speed is a conversion problem before it is an SEO problem. A 1-second delay in page load reduces conversions by 7%. Sites that pass all three Core Web Vitals thresholds see roughly 24% lower abandonment than sites that do not.
Page speed work pairs with the technical SEO foundations covered in our technical SEO fixes for rehab admissions guide and our web development capability. A landing page that loads fast on a marketing test can still fail in production when the parent site’s render-blocking resources or theme weight drag the actual page render past the Core Web Vitals thresholds.
DEFINITION
Core Web Vitals (CWV)
Google’s three real-world performance metrics measured at the 75th percentile on mobile: Largest Contentful Paint (LCP, load speed), Interaction to Next Paint (INP, responsiveness), and Cumulative Layout Shift (CLS, visual stability). A treatment center landing page that fails any one of the three competes at a structural disadvantage in both classic and AI search.
The 2026 Core Web Vitals thresholds have tightened. Google lowered the “Good” Largest Contentful Paint threshold from 2.5 seconds to 2.0 seconds. Interaction to Next Paint (INP) moved from a supplementary metric to an equal ranking signal alongside LCP and Cumulative Layout Shift.
LCP under 2.0 seconds on mobile. The largest visible element on the page (usually the hero image or hero text) needs to render within 2 seconds. The standard fixes: image optimization (WebP format, lazy-loaded everything below the fold, properly sized images), CDN delivery, font preloading, and removing render-blocking JavaScript from the critical path.
INP under 200 milliseconds. Interaction to Next Paint measures responsiveness to user input. For rehab landing pages, the critical interactions are the call button tap and the form field tap. Both have to respond within 200ms. The fix is keeping JavaScript execution off the main thread, especially for analytics and tag manager scripts.
CLS under 0.1. Cumulative Layout Shift measures how much the page shifts during load. A page that shifts as ads or trust badges load loses visitors who tap the wrong element. The fix is reserving space for every asynchronously loaded element and avoiding above-the-fold content that depends on dynamic insertion.
Only 42% of mobile sites pass all three Core Web Vitals in 2026. The 58% that do not are paying conversion-rate penalties on every paid visit. The fix is an annual technical audit of the landing pages and a budget line for ongoing performance maintenance.
Part 13. The HIPAA tracking layer on landing pages
The tracking architecture on a rehab landing page has to be HIPAA-aware. Standard analytics, retargeting, and CRM tags transmit data patterns that can be associated with health-related behavior, which makes them non-compliant on a treatment center page.
What is required. Conversion events route through a HIPAA-compliant intermediary (Freshpaint, Liveramp Health, or similar). The intermediary has a signed BAA with the operator. PHI never reaches Meta, Google, or third-party analytics platforms directly. De-identified conversion events get passed via Conversions API (for Meta) or offline conversion imports (for Google).
What is not required but recommended. A HIPAA-compliant call tracking solution (CallRail Healthcare, CallTrackingMetrics with BAA). HIPAA-compliant heatmap and session recording tools (Microsoft Clarity with PHI masking, FullStory with healthcare configuration). HIPAA-compliant form tools (the form vendor signs a BAA).
What needs counsel review. The full tracking stack on a rehab landing page needs to be reviewed by counsel familiar with HIPAA at least annually. Standards change. New vendors enter the space. The Health and Human Services Office for Civil Rights has issued updated guidance on online tracking technologies that affects how analytics tools can be configured. Counsel review is the operator’s protection against compliance drift.
What gets operators in trouble. Standard Meta pixel on the page. Standard Google Analytics gtag on the page without configured exclusions. Third-party retargeting tags from vendors without BAAs. Form tools that store PHI without BAAs. CRM integrations that transmit insurance information through unencrypted pixels. Each of these has triggered HHS OCR investigations in the last two years and overlaps with the broader Google Ads compliance mistakes framework on the paid side.
Part 14. Common mistakes operators repeat
Eight patterns we audit and see across treatment center landing pages.
Pattern 1: Call button below the fold. The phone number is buried in the navigation or appears two scrolls down. Family members in crisis tap the first call button they see. If none is above the fold, they leave.
MOST EXPENSIVE MISTAKE
Call button buried below the fold on mobile. Family members in crisis tap the first call button they see — if that button is two scrolls down, they bounce before reaching it. Treatment center conversion happens primarily on phone calls; this single placement decision drives more lost admits than any other pattern on this list.
Pattern 2: Generic “compassionate care” copy. The hero says nothing specific. Could be any treatment center. The visitor reads it and assumes the facility is interchangeable with the next one.
Pattern 3: Stock imagery that looks like every other rehab ad. Hands holding hands in a circle. Silhouette on a beach. Generic clinical setting. The stock library is shared across the entire category. Real facility imagery is a differentiator most operators decline to invest in.
Pattern 4: Form-primary CTA. “Fill Out the Form” as the hero action. The form has 8+ fields. The phone number is small and secondary. Most treatment center visitors call. The form-primary page misreads the conversion behavior of the audience.
Pattern 5: No confidentiality assurance above the fold. The visitor’s primary hesitation (assumed lack of privacy) is not addressed before they decide whether to call. The conversion event that would have happened does not.
Pattern 6: Slow page on mobile. LCP above 4 seconds. Family members on mobile leave before the hero renders.
Pattern 7: HIPAA-non-compliant tracking. Standard Meta pixel, standard GA tag, third-party retargeting pixels with no BAAs. The operator does not know the exposure exists until an audit surfaces it.
Pattern 8: One landing page for everything. The same page used for all campaigns, all populations, all levels of care. The visitor from “veteran rehab Virginia” lands on the same generic page as the visitor from “adolescent drug treatment California.” Both convert at a lower rate than population-specific landing pages would.
Part 15. Measurement
8–12%
Paid-search conversion rate benchmark on a well-built rehab landing page. Below this range, the page is the bottleneck, not the traffic.
4–7%
Paid-social conversion rate benchmark on a well-built rehab landing page. Same floor logic applies.
Cost per VOB
The right north-star metric per landing page. Cheapest CPL is not the same as cheapest cost per private-policy VOB, and only the latter funds census.
8–12%
Paid-search conversion rate benchmark on a well-built rehab landing page. Below this range, the page is the bottleneck — not the traffic.
4–7%
Paid-social conversion rate benchmark on a well-built rehab landing page. Same rule applies below the floor.
Cost per VOB
The right north-star metric per landing page. Cheapest CPL is not the same as cheapest cost per private-policy VOB — and only the latter funds census.
The right measurement framework for treatment center landing pages tracks four things, in order of priority.
Conversion rate by traffic source. Paid search, paid social, organic, direct. Each source has different visitor intent and different baseline conversion expectations. Paid search visitors convert higher than paid social visitors. Organic visitors convert higher than paid visitors. The benchmark for paid search on a well-built rehab landing page is 8% to 12%. For paid social, 4% to 7%. Below those, the page is the bottleneck.
Conversion rate by population segment. If the operator runs population-specific campaigns (veteran, adolescent, executive), the conversion rate by segment reveals whether the landing pages are correctly targeting each audience. Mismatched targeting shows up as flat conversion across segments that should be performing differently.
Cost per private-policy VOB by landing page. The downstream metric. The landing page that produces the lowest cost per private-policy VOB is the landing page that should be receiving more traffic. Most operators measure CPL by landing page but not cost per VOB by landing page. The former optimizes for cheap leads. The latter optimizes for admits, which is the measurement framework we describe in our Google Ads strategy guide.
Mobile versus desktop conversion gap. Track separately. A mobile gap of 30% to 40% is normal. A gap of 60%+ indicates a mobile-specific design or speed problem.
The metrics most operators report but should not. Bounce rate. Time on page. Pages per session. These are activity metrics, not conversion metrics. They describe what visitors did, not whether they called. A 75% bounce rate on a single-page conversion-focused landing page is fine if the 25% who did not bounce called at 30%.
WHAT WORKING REHAB LANDING PAGES DO
- Above-the-fold tap-to-call phone number, large and contrasted
- Specific, facility-distinct hero copy that names the program
- Real facility photography (clinical team, building, treatment areas)
- LCP under 2.5 seconds on mobile, ideally under 2.0
- HIPAA-compliant tracking with signed BAAs on every vendor
WHAT BROKEN REHAB LANDING PAGES SKIP
- Phone number buried in nav or two scrolls down
- Generic “compassionate care” boilerplate that fits any rehab
- Stock images shared across every other rehab site
- Slow page on mobile (LCP above 4 seconds)
- Standard Meta pixel, GA tag, retargeting without BAAs
Most in-house teams hit a wall not because they lack knowledge, but because they lack bandwidth.
When you are ready to hand it off, Webserv has spent 9 years executing exactly this for treatment centers nationwide.
Frequently asked questions about rehab landing page optimization
What conversion rate is realistic for a treatment center landing page?
A well-built treatment center landing page typically converts mobile paid traffic between 6 and 12 percent into calls or qualified form fills, with the highest-intent pages converting at 10 to 15 percent. Most generic treatment center landing pages convert at 1 to 3 percent. The difference is rarely traffic quality. It is how the page treats the family member arriving on mobile in a moment of decision.
The 6 to 12 percent range assumes the page hits the structural requirements: mobile-first design, above-the-fold trust signals, click-to-call prominent, confidentiality framing visible, page speed under 2.5 seconds Largest Contentful Paint, and HIPAA-compliant tracking that does not interfere with the user experience.
Programs converting below 4 percent typically have a structural problem rather than a creative one. The fix is usually addressed in the first 30 days of CRO work and produces a 2x to 4x conversion lift on the same paid traffic. The math justifies the work in almost every case.
Should we build one landing page or dedicated pages per campaign?
Most treatment centers running paid search should build at minimum 3 to 5 dedicated landing pages: one for branded traffic, one for non-branded detox, one for non-branded residential, one for PHP/IOP, and one for insurance-led traffic. Single-page setups force the page copy to compromise across audiences that have meaningfully different needs.
Family-member traffic responds to different language than patient-direct traffic. Insurance-led searches respond to verification-prominent design. Out-of-network and in-network audiences need different framing on policy acceptance. A single landing page trying to serve all of these converts worse than even modestly segmented pages.
The ceiling on segmentation is operational. More pages means more A/B testing surface, more tracking complexity, and more creative production. For most operators the right number is 3 to 8 pages, segmented by audience or campaign type, not by individual keyword.
How do we A/B test landing pages without breaking HIPAA compliance?
A/B testing on treatment center landing pages works the same as any conversion-rate optimization program, with one constraint: the testing tool cannot transmit PHI or PHI-adjacent signals to a non-BAA platform. Google Optimize is sunset; the modern HIPAA-compliant pattern uses a tool with a signed BAA (VWO Enterprise, Optimizely with BAA, Convert with BAA) that handles patient-adjacent traffic correctly.
Most operators do not need page-level testing tools at all in the first 90 days of a CRO program. Server-side A/B testing using campaign-level UTM splits and reporting against verified VOB conversions captures most of the lift available without adding a third-party testing tool to the HIPAA stack.
When a testing tool is needed, the BAA is the gate. Tools without behavioral health customer references should be assumed non-compliant until proven otherwise. The cost of an OCR violation from a non-BAA testing tool exceeds the cost of the BAA-enabled enterprise tier by orders of magnitude.
How long does it take to see results from landing page work?
Most treatment centers see meaningful conversion-rate lift within 30 to 60 days of shipping a new landing page. The first 14 days are diagnostic: enough paid traffic to validate the new page is not regressing performance. Days 15 to 30 see the algorithm calibrate to the new conversion event volume. Days 30 to 60 produce the cleanest before-and-after comparison against the prior baseline.
The fastest wins come from fixing the most expensive single friction point first. A mobile page-speed fix can lift conversion 30 to 50 percent in the first week. A click-to-call placement fix can lift call volume 20 to 40 percent in the same window. Compounded across the trust signal stack, the cumulative lift typically reaches 2x to 4x in 90 days.
Programs that take 90 days or more to see lift usually have a structural problem the optimization did not address. The fix is to diagnose the bottleneck (page speed, mobile UX, trust signal gap, friction in the conversion flow) and address it specifically rather than running broad creative changes hoping the conversion rate improves.
What is the single most common landing page mistake that costs admissions?
Building the page for the brand team rather than the family member arriving on mobile in a moment of decision. The brand-team page looks polished, leads with the facility’s mission, and routes the visitor through a multi-step journey toward a soft inquiry. The family-member-arriving-in-crisis page leads with the trust signal, makes the phone number prominent, and answers the three questions the visitor actually has within the first scroll.
The second-most-common mistake is treating the form as the primary conversion. Most family members making BH treatment decisions prefer phone over form by 2:1 or 3:1 ratios. A page that buries the phone number below the fold while emphasizing a 6-field form is leaving phone-based admits unrealized. The right pattern is click-to-call prominent above the fold, with the form as a secondary conversion path for visitors who prefer text.
The third mistake is missing the confidentiality framing entirely. Family members in crisis are worried about privacy. A landing page that addresses confidentiality explicitly above the fold (HIPAA-protected intake, anonymous insurance verification, named clinical leadership) converts higher than a page that does not address it at all.
What this means for treatment center operators
The landing page is the most under-invested asset in most treatment center paid media programs. Operators spend $40,000 to $80,000 a month on media and route it to a landing page they have not touched since 2022.
The 14-section playbook above describes what a 2026 treatment center landing page should be. Mobile-first design. Above-the-fold call button. Confidentiality assurance in the hero. Joint Commission and named medical director as trust anchors. Insurance verification offered prominently. Page speed under 2.0 seconds LCP on mobile. HIPAA-compliant tracking. Population-specific variants for population-specific campaigns. Cost per VOB measured at the landing page level.
Operators who audit their landing pages against this list will usually find 3 to 5 fixes that compound. Adding a sticky call button. Moving the confidentiality assurance above the fold. Replacing stock imagery with real facility photos. Compressing the form from 8 fields to 3. Each fix produces a measurable conversion lift. Together they often produce a 2x to 3x improvement in cost per admit without changing the media spend.
The work is unglamorous post-click discipline most agencies skip because clients do not see it on the dashboard. The agencies that build the landing page infrastructure correctly are the agencies whose clients consistently outperform their benchmarks year after year.
If you want to walk through whether your current landing pages are doing the conversion work the paid media spend is paying for, book a discovery call. We will audit the landing pages, run the mobile speed test, check the HIPAA tracking stack, and tell you honestly where the conversion leaks are. The audit is free. The honest answer is the deliverable, not the pitch.
The perspective in this article comes from 9 years working exclusively inside behavioral health.
We are a team built by people in recovery who understand that behind every admission is someone asking for help. If that resonates, get to know us.
Mitch Marowitz is the Director of Paid Media at Webserv, a digital marketing agency for treatment centers.