A treatment center marketing director forwarded me a proposal last month. The pitch was straightforward: $50,000 per quarter for “guaranteed DR70+ backlinks from established healthcare publications.” The deck included logos from Forbes, Inc., Healthline, and a few names I’d never heard of.
The proposal didn’t ask whether her facility could afford the program. It asked whether she could afford not to keep up with what competitors were buying.
I told her to throw it out. Not because $50,000 per quarter is unreasonable for a serious authority program. Because the program she was being pitched would have actively damaged her facility’s standing in 2026, not built it.
Two Google updates in March, a widening of SpamBrain’s link evaluation, a fundamental shift in how AI search platforms weight authority signals, and the YMYL standard applied to behavioral health have collectively rewritten the link-building playbook.
We work on the replacement playbook every day inside Webserv’s Digital PR program for treatment centers. The old “buy DR points by the dozen” approach is a liability now, not an asset.
This guide is the cluster hub for everything that replaces it, and it sits inside our broader drug rehab SEO strategy guide covering the on-page, technical, and content foundations earned links compound on top of.
Five organizing pillars covering why the old playbook broke, what authority actually means for behavioral health in 2026, the tactical earned-link plays that work, the compliance constraints that bound everything, and how the new authority stack feeds the AI citation layer that increasingly drives admissions.
Key Takeaways
- Google’s March 2026 spam and core updates landed within three days of each other. The spam update completed in under 20 hours and widened SpamBrain detection of link schemes. Expired-domain redirects, AI-content PBNs, and sponsored link structures with obscured attribution are now actively penalized.
- Behavioral health sits inside Google’s strictest evaluation category (YMYL). The penalty for low-quality or manipulative links on a rehab site is materially worse than the same tactics on a roofing or SaaS site.
- The 2026 authority stack for behavioral health is five layered components: brand entity recognition, topical authority, citation diversity, author entity strength, and AI citation share. None of these are produced by buying high-DR backlinks.
- The HARO playbook collapsed in 2024. The 2026 replacement is a stack of Qwoted, Featured, Source of Sources (Peter Shankman’s free replacement), and #JournoRequest on X. Used together they outperform legacy HARO at a fraction of the time investment.
- LegitScript Certification is the floor, not the ceiling. Compliance with HIPAA, EKRA, and ASAM-aligned positioning gates everything else. Programs that skip these constraints earn links faster and lose certifications faster.
- A 12-month earned-link program for a treatment center should produce 30-50 referring domain wins, 10-20 mid-DR vertical placements, 50+ author-authored LinkedIn long-form pieces, and a measurable lift in AI citation share across ChatGPT, Perplexity, and Google AI Mode.
Pillar 1: Why Link Buying Stopped Working for Rehabs in 2026
The structural backdrop matters because the new playbook only makes sense if you understand what changed.
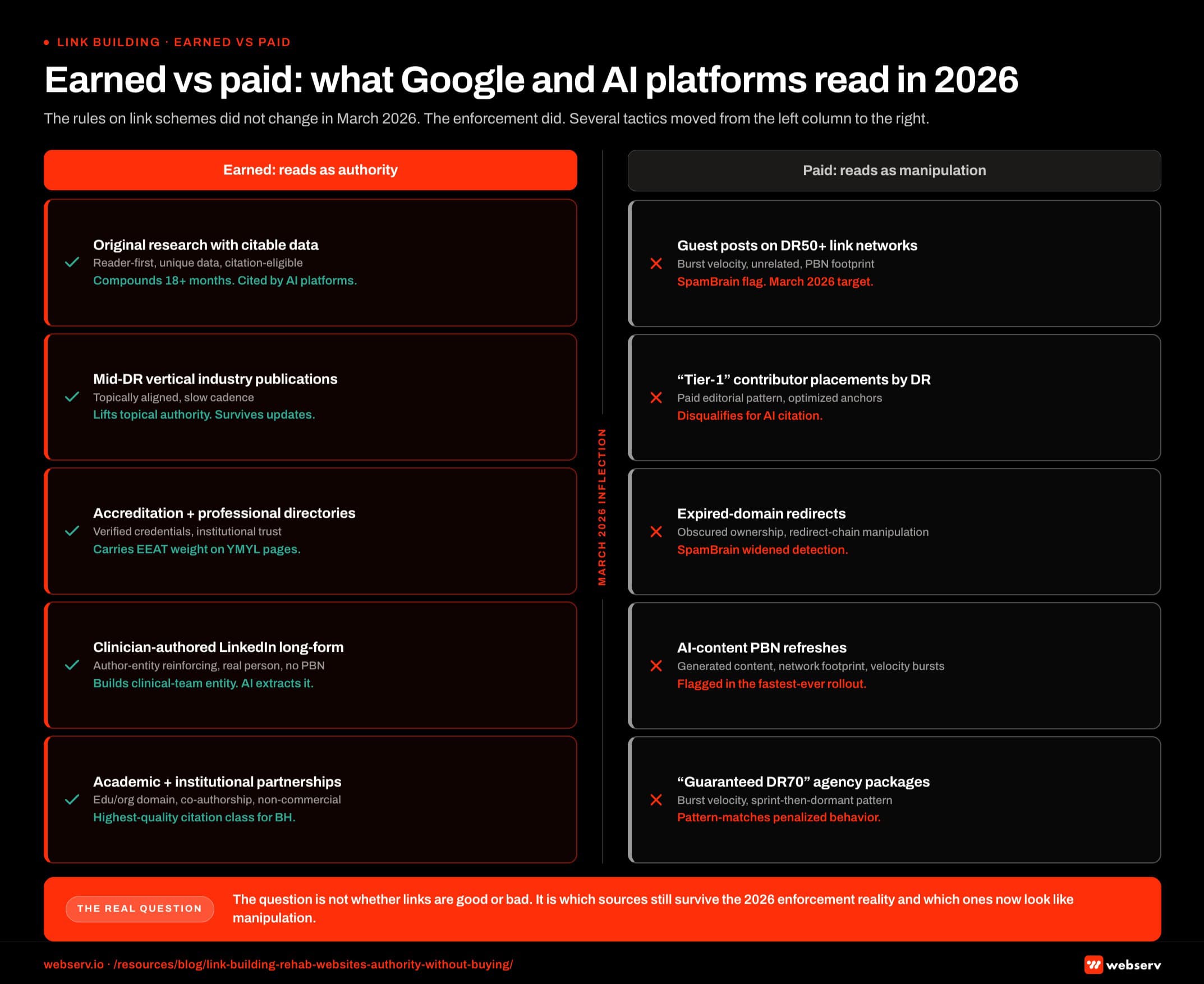 Infographic titled ‘Earned vs paid: what Google and AI platforms read in 2026’ showing a two-column comparison map. The left column carries earned signals Google and AI platforms read as authority. The right column carries paid signals Google now flags as manipulation. A center divider carries the March 2026 enforcement inflection date. The earned column contains five source cards. Original research with citable data: read as reader-first, unique, citation-eligible, brand-entity reinforcing; compounds over 18 or more months and is cited by AI platforms. Mid-DR vertical industry publications: topically aligned, slow-cadence; lift topical authority and survive algorithm updates. Accreditation and professional directories: verified credentials and institutional trust; carry EEAT weight on YMYL pages. Clinician-authored LinkedIn long-form: author-entity reinforcing with a real-person signature and no PBN footprint; builds clinical-team entity. Academic and institutional partnerships: edu and org domain class, research co-authorship; the highest-quality citation class for behavioral health. The paid column contains five source cards. Guest post placements on DR50 plus link networks: burst velocity, contextually unrelated, PBN footprint; SpamBrain flag, March 2026 enforcement target. Tier-1 contributor placements priced by domain rating: paid editorial pattern with optimized anchors; disqualify for AI citation. Expired-domain redirects: obscured ownership and redirect-chain manipulation; SpamBrain widened detection in March 2026. AI-content PBN refreshes: low-effort generated content with network footprint and link velocity bursts; SpamBrain flag in the fastest-ever rollout. Guaranteed DR70 agency packages: burst velocity, sprint pattern, dormant periods between bursts; pattern-match penalized behavior. Earned-column callout: the earned column compounds and each placement reinforces brand entity and topical authority. Paid-column callout: the paid column is now a risk-bearing asset class and burst velocity plus PBN footprints plus AI-content refreshes all trip the widened detection. Divider callout: March 2026 ran a core update and a spam update inside a three-day window, rules unchanged but enforcement widened, and the spam update completed in under 20 hours. Bottom strip callout: the question is not whether links are good or bad, the question is which sources survive the 2026 enforcement reality and which now look like manipulation.
Infographic titled ‘Earned vs paid: what Google and AI platforms read in 2026’ showing a two-column comparison map. The left column carries earned signals Google and AI platforms read as authority. The right column carries paid signals Google now flags as manipulation. A center divider carries the March 2026 enforcement inflection date. The earned column contains five source cards. Original research with citable data: read as reader-first, unique, citation-eligible, brand-entity reinforcing; compounds over 18 or more months and is cited by AI platforms. Mid-DR vertical industry publications: topically aligned, slow-cadence; lift topical authority and survive algorithm updates. Accreditation and professional directories: verified credentials and institutional trust; carry EEAT weight on YMYL pages. Clinician-authored LinkedIn long-form: author-entity reinforcing with a real-person signature and no PBN footprint; builds clinical-team entity. Academic and institutional partnerships: edu and org domain class, research co-authorship; the highest-quality citation class for behavioral health. The paid column contains five source cards. Guest post placements on DR50 plus link networks: burst velocity, contextually unrelated, PBN footprint; SpamBrain flag, March 2026 enforcement target. Tier-1 contributor placements priced by domain rating: paid editorial pattern with optimized anchors; disqualify for AI citation. Expired-domain redirects: obscured ownership and redirect-chain manipulation; SpamBrain widened detection in March 2026. AI-content PBN refreshes: low-effort generated content with network footprint and link velocity bursts; SpamBrain flag in the fastest-ever rollout. Guaranteed DR70 agency packages: burst velocity, sprint pattern, dormant periods between bursts; pattern-match penalized behavior. Earned-column callout: the earned column compounds and each placement reinforces brand entity and topical authority. Paid-column callout: the paid column is now a risk-bearing asset class and burst velocity plus PBN footprints plus AI-content refreshes all trip the widened detection. Divider callout: March 2026 ran a core update and a spam update inside a three-day window, rules unchanged but enforcement widened, and the spam update completed in under 20 hours. Bottom strip callout: the question is not whether links are good or bad, the question is which sources survive the 2026 enforcement reality and which now look like manipulation.For the better part of a decade, the dominant link-building strategy for treatment centers ran on three legs. Buy guest post placements on DR50+ sites. Pitch contributor placements at Tier-1 business publications. Layer in some HARO responses for variety.
The agencies selling those programs charged $5,000 to $25,000 per month, and the work produced enough referring domains to keep Ahrefs reports looking healthy.
The problem with that playbook was never that it didn’t work. It worked. The problem is that Google has spent two years systematically dismantling its inputs.
The March 2026 Double Update
In March 2026, Google rolled both a core update and a spam update within a three-day window. The spam update completed in under 20 hours, the fastest rollout ever recorded.
Per Google’s spam policies, the rules on link schemes didn’t change. The enforcement did.
SpamBrain’s detection widened to flag link velocity patterns that previously slipped through, expired-domain redirects that obscured original site ownership, and AI-content PBNs (private blog networks refreshed with low-effort AI-generated content).
The treatment centers that took the biggest hits in March 2026 were the ones running aggressive paid link campaigns. The sites that held steady had link profiles earned from genuinely relevant sources, with reader-first content backing each placement.
The technical foundation matters here too. Our walkthrough of technical SEO for behavioral health websites covers the indexation, schema, and crawl-quality work that has to be in place before any earned-link investment can compound.
Link Velocity Scrutiny Intensified
A specific behavior Google now flags is burst-style link velocity followed by dormant periods. The pattern matches what a paid campaign produces (sudden batch of placements over 30 days, then quiet for the next 90).
Legitimate earned-link programs produce steady-state growth (5-10 referring domains per month on average, sustained over 12 months) that looks structurally different from a paid sprint.
This means even agencies running technically defensible link campaigns now have to slow them down to avoid pattern-matching against penalized behavior.
YMYL Applied to Behavioral Health
Google’s Helpful Content guidelines apply the highest content-quality standard to Your Money or Your Life topics. Behavioral health hits all three components (health, financial stability, safety).
The practical consequence is that the penalty for low-quality or manipulative links on a rehab site is materially worse than the same tactics on a non-YMYL site.
A roofing company can take a small ranking hit from a sketchy link profile and recover quickly. A treatment center can lose 60 percent of its organic traffic for 12 months from the same tactics.
The risk-adjusted cost of buying links on a rehab site is multiple times what it is in other verticals. The expected value of paid link campaigns has gone meaningfully negative.
The Price-vs-Risk Math
The $50,000-per-quarter proposal I mentioned in the intro pencils out poorly when you do the actual risk math.
If the campaign produces 12 DR70+ links over the quarter and Google’s enforcement flags even three of them as part of a paid scheme, the resulting traffic drop wipes out 6 to 18 months of earned organic growth.
The recovery path is to disavow the bad links, rebuild trust signals over months, and absorb the admissions impact in the meantime.
The math gets worse if you also lose LegitScript Certification standing as part of the cleanup, which has happened to enough treatment centers in the last 24 months that compliance teams have started flagging Digital PR proposals as risk-elevated procurement.
This is why our earlier write-up on doorway pages and other anti-patterns is paired with this guide. The two anti-patterns share a root cause: agencies optimizing for tactics Google has clearly signaled it will penalize.
Pillar 2: The New Authority Stack for Behavioral Health
If buying links is dead, what replaces it. The answer is a five-layer stack that produces compounding authority over 6 to 18 months and survives algorithm updates because each component is the kind of signal Google and AI platforms have publicly stated they reward.
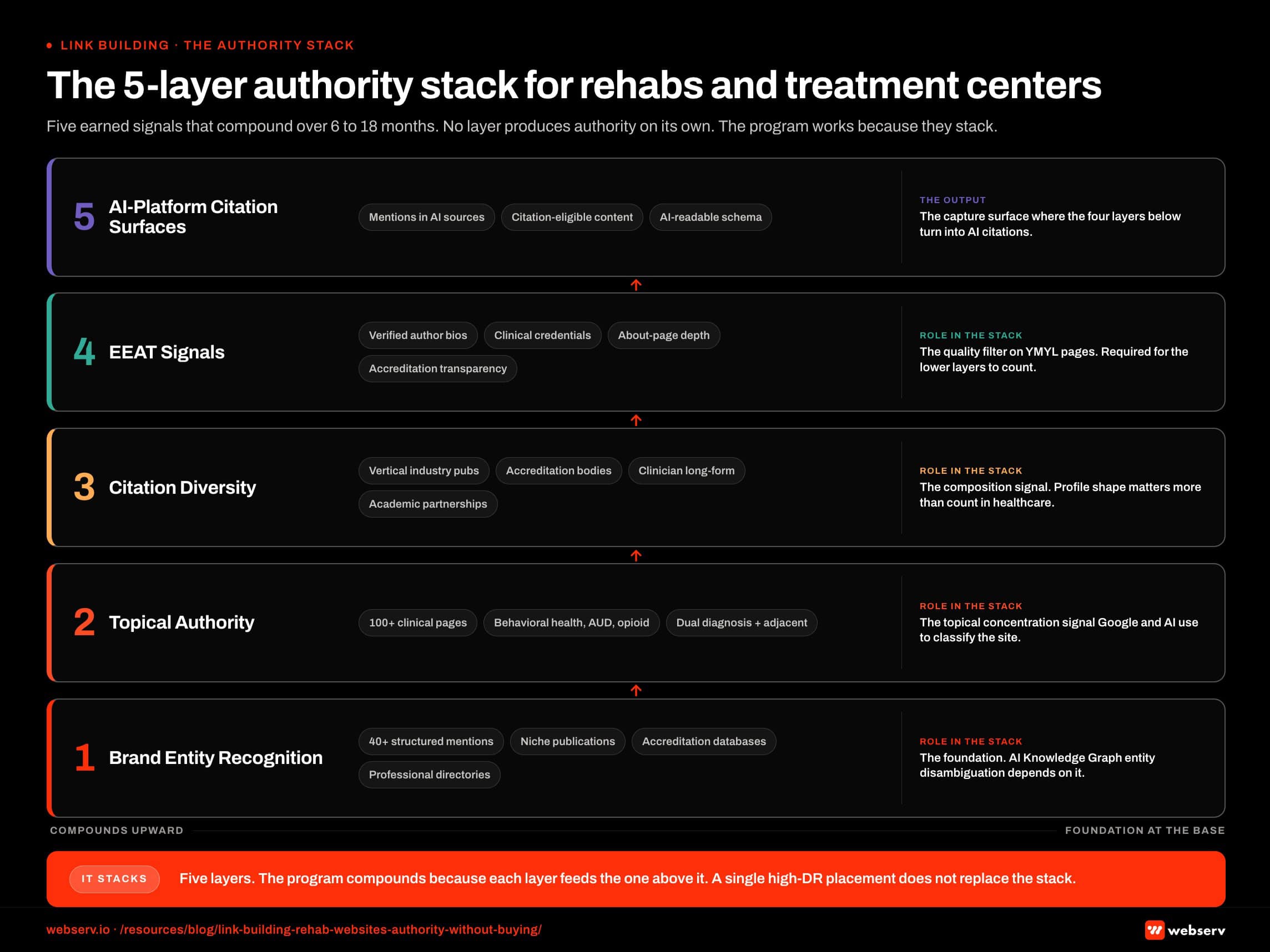 Infographic titled ‘The 5-layer authority stack for rehabs and treatment centers’ showing five earned signals that compound to produce defensible authority in 2026, structured as five horizontal layers stacked vertically with Brand Entity Recognition as the foundation and AI-Platform Citation Surfaces at the top. Layer 1, Brand Entity Recognition, is produced by 40 or more structured mentions across niche industry publications, accreditation databases, professional directories, and clinician-authored content; it is the foundation because AI Knowledge Graph entity disambiguation depends on it. Layer 2, Topical Authority, is produced by 100 or more well-built clinical pages on behavioral health, alcohol use disorder, opioid treatment, dual diagnosis, and adjacent topics; it is the topical concentration signal Google and AI platforms use to classify the site. Layer 3, Citation Diversity, is produced by links from four source categories covering vertical industry publications, accreditation bodies, clinician-authored long-form, and academic or institutional partnerships; it is the composition signal because profile shape matters more than raw count in healthcare. Layer 4, EEAT Signals, is produced by verified author bios, clinical credentials, About page depth, professional association memberships, and transparent ownership and accreditation; it is the quality filter Google applies to YMYL behavioral health pages and is required for the other layers to count. Layer 5, AI-Platform Citation Surfaces, is produced by brand mentions across the sources ChatGPT, Perplexity, Gemini, and Claude extract from plus citation-eligible content patterns and AI-readable schema; it is the capture surface where the other four layers turn into AI Mode and AI Overview citations. Layer 1 callout: brand search volume now predicts AI citation share better than backlink profile does, and forty mid-DR mentions outweigh three Forbes placements. Layer 3 callout: profile composition matters more than count and a profile that leans on one category is fragile. Layer 4 callout: EEAT is the quality filter on YMYL pages, and without it the other layers do not count. Layer 5 callout: AI platforms cite the sites the other four layers built. Bottom strip callout: five layers, the program compounds because each layer feeds the layer above it, and a single high-DR placement does not replace the stack.
Infographic titled ‘The 5-layer authority stack for rehabs and treatment centers’ showing five earned signals that compound to produce defensible authority in 2026, structured as five horizontal layers stacked vertically with Brand Entity Recognition as the foundation and AI-Platform Citation Surfaces at the top. Layer 1, Brand Entity Recognition, is produced by 40 or more structured mentions across niche industry publications, accreditation databases, professional directories, and clinician-authored content; it is the foundation because AI Knowledge Graph entity disambiguation depends on it. Layer 2, Topical Authority, is produced by 100 or more well-built clinical pages on behavioral health, alcohol use disorder, opioid treatment, dual diagnosis, and adjacent topics; it is the topical concentration signal Google and AI platforms use to classify the site. Layer 3, Citation Diversity, is produced by links from four source categories covering vertical industry publications, accreditation bodies, clinician-authored long-form, and academic or institutional partnerships; it is the composition signal because profile shape matters more than raw count in healthcare. Layer 4, EEAT Signals, is produced by verified author bios, clinical credentials, About page depth, professional association memberships, and transparent ownership and accreditation; it is the quality filter Google applies to YMYL behavioral health pages and is required for the other layers to count. Layer 5, AI-Platform Citation Surfaces, is produced by brand mentions across the sources ChatGPT, Perplexity, Gemini, and Claude extract from plus citation-eligible content patterns and AI-readable schema; it is the capture surface where the other four layers turn into AI Mode and AI Overview citations. Layer 1 callout: brand search volume now predicts AI citation share better than backlink profile does, and forty mid-DR mentions outweigh three Forbes placements. Layer 3 callout: profile composition matters more than count and a profile that leans on one category is fragile. Layer 4 callout: EEAT is the quality filter on YMYL pages, and without it the other layers do not count. Layer 5 callout: AI platforms cite the sites the other four layers built. Bottom strip callout: five layers, the program compounds because each layer feeds the layer above it, and a single high-DR placement does not replace the stack.Layer 1: Brand Entity Recognition
The most under-discussed shift in 2026 is that “authority” now incorporates brand entity recognition (the AI Knowledge Graph’s ability to map your facility to a coherent concept). Brand search volume now predicts AI citation share better than backlink profile does.
This means consistent, structured mentions of your brand across many sources (even mid-DR ones) outweigh a single high-DR placement. The mechanism is entity disambiguation. AI models triangulate which “Mountain View Recovery” or “Cascade Treatment” you are based on how consistently you appear across credible sources.
A facility with 40 mentions across niche industry publications, accreditation databases, professional association directories, and clinician-authored long-form content has a stronger brand entity than a facility with 3 Forbes placements and nothing else.
Layer 2: Topical Authority
Topical authority for treatment centers is the second layer. The principle is that Google and AI platforms classify sites by topical concentration, not just per-page relevance.
A site that publishes 100 well-built clinical pages on behavioral health, alcohol use disorder, opioid treatment, dual diagnosis, and adjacent topics builds topical authority that lifts every individual page it produces. A site with 12 thin pages on the same topic and 88 pages on unrelated subjects does not.
Topical authority compounds over time and produces ranking gains on terms you didn’t specifically target. It’s also one of the strongest signals AI platforms use when deciding which sites to extract citations from.
Layer 3: Citation Diversity
The third layer is citation diversity. The composition of your backlink profile matters more than the count, particularly in healthcare.
A healthy 2026 backlink profile for a treatment center has links from at least four source categories:
- Institutional research credibility: SAMHSA, NIH, NIDA, CMS, ASAM, JCAHO, CARF
- Mid-DR vertical industry publications: Behavioral Health News, Addiction Professional, Treatment Magazine, Recovery Today, The Fix, Filter Magazine (the full mid-DR thesis is covered in our companion piece on why mid-DR backlinks outperform DR70+ for LLM citations)
- Academic and university sources: research collaborations, faculty-authored content, citing studies
- Niche author profiles on aggregator platforms: LinkedIn long-form, Substack, podcast appearances
A profile concentrated in one category (even if all DR70+) signals less authority to both Google and AI platforms than a profile spread across all four.
Layer 4: Author Entity Strength
The fourth layer is the strength of the named clinical and operational entities associated with your facility. Google and AI platforms increasingly evaluate not just the site, but the people behind the content.
A treatment center with named clinical leadership who appear as quoted experts in industry publications, contribute to academic working groups, maintain active LinkedIn profiles with verifiable credentials, and author content under their own bylines produces stronger E-E-A-T signals.
A facility with anonymous content authored by a marketing team produces weaker E-E-A-T signals, regardless of how many backlinks the marketing team earns.
This is why our pre-launch SEO checklist for behavioral health websites treats clinical author bio rollout as a foundation requirement, not a polish item.
Layer 5: AI Citation Share
The fifth layer is the newest one. AI citation share (how often your brand and your owned content surface as cited sources in ChatGPT, Perplexity, Google AI Mode, and Claude answers) is now a top-line authority metric.
The mechanism is different from backlink-driven rankings. AI platforms use vector retrieval to score candidate documents by semantic relevance, then re-rank by a basket of trust signals. The output is a citation distribution that overlaps with traditional SEO authority but diverges sharply on which sources actually get pulled.
We dove deep on this in our analysis of how to get your rehab cited in AI Overviews and ChatGPT answers. The core takeaway: your Digital PR program should be designed to produce AI citation lift as a primary KPI, not as a side effect.
“The question for treatment center marketing teams in 2026 isn’t how to buy more authority. It’s how to earn the kind that algorithms haven’t learned to penalize and that AI platforms actively reward.
Those signals don’t come from DR points. They come from being a recognized entity across a diverse, credible citation graph.”
Preston Powell, Chief Executive Officer, Webserv
Pillar 3: The Tactical Earned-Link Playbook
Five plays produce the bulk of the earned-link wins for treatment centers in 2026. None of them require buying links. All of them have been pressure-tested on real BH portfolios.
Play 1: Original Research and Data Studies
The single most productive move is publishing original research. A treatment center has access to data that no journalist or generalist publication does: actual outcomes, length-of-stay patterns, payer-mix realities, demographic trends, modality effectiveness comparisons.
Packaging that data into a credible research report (12 to 30 pages, with chart visualizations and a clinical co-author) produces a content asset that earns links for years. Academic institutions cite it. Industry publications reference it. SAMHSA-adjacent policy work picks it up.
The investment is meaningful: $15,000 to $40,000 for a credible report, depending on data complexity and design quality. The output is typically 30 to 100 earned references over the following 12 to 24 months, with each reference carrying real topical authority weight.
Our portfolio data shows that one well-executed annual research study outperforms a year of contributor placement chasing on aggregate authority lift.
Play 2: The HARO Replacement Stack
HARO collapsed in 2024 when Cision restructured the platform into Connectively, which itself wound down by late 2024. Featured.com bought the HARO brand from Cision in April 2025 and revived it as a free daily newsletter.
The 2026 replacement is a stack, not a single platform:
- Qwoted: verification-gated, $99-$149/month, highest conversion rate of any HARO alternative. Healthcare is one of its strongest verticals.
- Featured.com: curated expert roundups for Fortune, Fast Company, Yahoo, and similar publications. Different model than classic HARO (roundup-style rather than direct journalist pitches).
- Source of Sources (SoS): Peter Shankman’s free replacement after the Connectively implosion. Honor-system based, lower noise.
- #JournoRequest on X: journalists post source requests directly. Fastest response window of any channel. Free.
The right cadence is daily monitoring across all four, with response pitches sent within 30 minutes of a relevant query going live. Real treatment center programs produce 3 to 8 placements per month through this stack alone.
The compliance constraint matters here. Every pitch needs to align with LegitScript-compliant messaging and ASAM-aligned positioning before it goes out, which slows response time slightly but eliminates the risk of an off-script quote producing a compliance issue downstream.
Play 3: Mid-DR Vertical Industry Publications
The mid-DR vertical pubs that dominate AI citation share are the most productive placement targets in 2026. The full thesis on why is covered in our companion analysis on why mid-DR backlinks now outperform DR70+ sites for LLM citations.
The target list for behavioral health includes Behavioral Health News, Addiction Professional, Treatment Magazine, Recovery Today, The Fix, Filter Magazine, and Recovery.com.
These sit in the DR 40-60 range and have small audiences relative to Forbes. They get cited by LLMs at rates that punch dramatically above their DR weight.
The pitch motion for these publications is different from Tier-1 pitching. Editors at industry trade pubs are looking for clinical depth, operational specifics, and named expert contributors.
A pitch that opens with “thought leadership piece on the future of behavioral health” gets deleted. A pitch that opens with “our Medical Director published a 14-month outcomes study on combined MAT and ACT therapy in our PHP program” gets a reply. We walk through the full pitch architecture in our guide to earning PR coverage for treatment centers, including subject-line patterns and the credibility cues editors actually screen for.
Cadence: 2 to 4 placements per quarter is realistic for a well-run program. Cost: typically $0 if the relationship is direct, $2,000-$5,000 if mediated through a PR firm with established editorial contacts.
Our existing playbook on specific Digital PR tactics for rehab centers covers the response cadence and pitch structure in operational detail.
Play 4: Expert Content Partnerships
The fourth play is partnership-driven. Co-authored pieces with academic researchers, clinicians outside your facility, or institutional figures produce credibility-rich placements that single-author pitches rarely match.
The motion: identify a researcher publishing in your modality space, propose a co-authored piece that combines your operational data with their academic framing, place it in a relevant journal or industry publication, and earn the citations and links that flow from both your network and theirs.
This works particularly well for facilities running specialized modalities (TMS, ketamine, EMDR, equine therapy) where the academic literature is still developing and operational data is genuinely useful for emerging research.
Cadence: 1 to 2 placements per quarter, but each one tends to compound for years.
Play 5: Author Entity Building
The fifth play is the longest-arc but produces the deepest moat. Building the named clinical and operational entities at your facility into recognized authorities in their own right shifts your link earning from “we need a placement” to “we have people journalists call when they need a source.”
The components:
- LinkedIn long-form posts authored by clinical leadership, published consistently (2-4 per month per author). Profound’s data shows LinkedIn rose from #11 to #5 most-cited source on ChatGPT between November 2025 and February 2026, the largest authority shift Profound recorded all year.
- Podcast appearances by named clinical leaders, particularly on shows hosted by clinicians or researchers.
- Substack newsletters from your Medical Director or Clinical Director, sustained over 12+ months.
- Guest lectures, conference presentations, and academic working group participation, all documented and linked from your author bio pages.
This isn’t a one-quarter motion. It’s a 12-to-36-month build that produces compounding citation share and protects your authority profile from algorithm volatility.
Pillar 4: Compliance and the Ethical Boundary
DEFINITION
Eliminating Kickbacks in Recovery Act (EKRA)
The 2018 federal anti-kickback law that prohibits paying or receiving remuneration for referrals to addiction treatment programs. EKRA exposure exists when any link, partnership, or referral arrangement could be construed as a paid referral mechanism. Most low-quality link schemes targeting addiction treatment programs create EKRA risk by default.
Every link-earning move for a treatment center sits inside a compliance frame. Skipping the frame produces faster wins and faster losses.
LegitScript Certification
LegitScript Certification is required to run addiction treatment ads on Google, Meta, Microsoft Ads, and Nextdoor. It’s also a signal that flows through your earned media work. Our broader guide to vetting top addiction treatment SEO agencies covers what credible vendor relationships look like in this compliance frame.
A facility that maintains LegitScript certification can pitch publications with that credential as part of its credibility profile. A facility that’s lost certification (or never had it) faces editor skepticism that closes pitch doors quickly.
The renewal cadence matters. LegitScript audits annually and the standards drift over time. Treatment centers that treat certification as a one-time achievement rather than an ongoing operational requirement run into placement problems mid-year that they didn’t expect.
HIPAA and Patient Privacy
Earned media work for treatment centers requires never using identifiable patient data without explicit, documented consent that meets HIPAA’s research-grade standard.
This is the constraint that shapes original research most directly. A study on “outcomes for our PHP program” can be published with aggregated, de-identified data.
The consent and aggregation work needs to happen up front. A research report that surfaces a privacy concern after publication is a worse outcome than no report at all. SAMHSA’s national treatment data is the public-domain benchmark facilities can reference without exposing patient-derived information.
Most facilities underspend on the compliance review layer of their content production. The right pattern is a documented review process where every piece of patient-derived content (research, case studies, clinical examples) goes through legal and compliance review before any external pitch.
EKRA and Patient Brokering
The Eliminating Kickbacks in Recovery Act (EKRA) is the legal floor for ethical operations. Any earned media or partnership that could be construed as a paid referral arrangement creates EKRA exposure.
This affects link earning in two specific ways:
- Affiliate-style arrangements: paying a partner publication for placements that include referral mechanics (call-tracking attribution to an affiliate, revenue share on resulting admissions) is EKRA-exposed.
- Referral source recognition placements: thanking referral sources publicly in ways that could be construed as compensation is EKRA-exposed.
The clean pattern is full separation. Earned media is earned on the basis of credibility and content. Referral relationships are managed entirely separately, in compliance frameworks reviewed by legal counsel.
ASAM-Aligned Positioning
ASAM (American Society of Addiction Medicine) provides the clinical standard most editors and journalists use as a credibility filter. Content that aligns with ASAM’s framework on substance use disorder treatment, the disease model of addiction, and evidence-based practice clears editorial review faster.
This means the language you use in earned media pitches matters. “Patient” rather than “client” in clinical contexts. “Substance use disorder” rather than “addiction” in formal writing. “Medication-assisted treatment” or “medications for opioid use disorder” rather than colloquial terms.
Editors who cover behavioral health are increasingly trained in this language. Pitches that don’t reflect it signal a facility that hasn’t done the clinical foundation work, which closes pitch doors.
The Ethical Messaging Multiplier
Beyond the legal floor, ethical messaging is a measurable performance lever. Research consistently shows transparent, evidence-based content produces 40-60 percent higher qualified inquiry rates than urgency-driven or manipulative tactics.
Earned media pitches that lead with operational specifics, clinical outcomes, and named contributor credentials outperform pitches that lead with brand claims or facility marketing. The first category gets placed. The second category gets archived.
Pillar 5: The AEO and LLM Citation Layer
The newest dimension of authority is how earned-link strategy translates into AI citation share. This is where the 2026 playbook diverges most sharply from the 2022 one.
How Earned Authority Translates to AI Citations
AI platforms (ChatGPT, Perplexity, Google AI Mode, Claude) use vector retrieval to select citation sources for each query. The retrieval step rewards semantic relevance and topical authority. The re-ranker layer rewards brand entity recognition, structured content formatting, and author credential signals.
Traditional backlinks influence AI citation share, but through different mechanisms than they influence Google rankings. A backlink from SAMHSA passes research credibility that AI re-rankers weight heavily. A backlink from Forbes passes domain authority that AI re-rankers weight weakly (or in some cases not at all).
This is why the shift from DR-chasing to entity-building matters operationally. Earned links from sources that contribute to your topical authority profile produce AI citation lift. Earned links that primarily exist to pass DR don’t.
Building Your Brand Entity in the AI Knowledge Graph
The AI Knowledge Graph is the conceptual map AI platforms use to disambiguate entities. Your facility is an entity. The question is whether you’re a clearly recognized one.
Building a strong brand entity in 2026 requires:
- Consistent NAP and brand information across institutional databases (Google Business Profile, Bing Places, Apple Maps, Yelp, healthcare-specific directories like Psychology Today). Our local SEO playbook for rehab centers covers the directory work that builds this layer
- sameAs schema on your site connecting to authoritative profiles (LegitScript listing, professional association memberships, key staff LinkedIn profiles)
- Wikipedia or Wikidata presence for facilities large enough to warrant a credible entry (this isn’t a vanity move, it’s a Knowledge Graph anchor)
- Mentions across diverse credible sources with consistent brand attribution
Page-Level Structure for Citation Eligibility
Beyond brand-level signals, page-level structure determines whether individual pages get extracted as citations. Pages built for fan-out query mechanics and semantic triple patterns get cited at substantially higher rates than long-form magazine prose, regardless of where it’s published.
This means the work you do on your owned content interacts with the link-earning work in a multiplier pattern.
A well-structured page on your site that earns a backlink from a credible source produces compounding citation lift. A poorly-structured page earning the same backlink produces single-event lift only.
Measurement Infrastructure
You can’t manage what you can’t measure. The 2026 measurement stack for AI citation share includes:
- Profound: continuous prompt monitoring across ChatGPT, Perplexity, AI Mode, Claude. Enterprise-grade with $96M Series C funding.
- AthenaHQ: growth-stage focused, deeper analytics, lower price point than Profound.
- Otterly and Peec: budget-tier options with adequate coverage for smaller programs.
The baseline metric is AI citation share (percentage of relevant prompts that produce an answer citing your brand or owned content). Track monthly against a defined competitive set. Programs that produce mid-DR vertical placements and original research consistently show measurable citation share gains within 90 to 180 days. Our companion piece on measuring citation share across ChatGPT, Perplexity, Claude, and Google AI Overviews covers the prompt set design and competitive baselining inside the tools above.
The New KPI Hierarchy
The KPI structure for a treatment center earned-link program in 2026 looks different from the 2022 version. The new hierarchy:
- AI citation share (primary metric)
- Referring domains from diverse source categories (with category breakdown, not aggregate count)
- Branded search volume growth (proxy for entity recognition strength)
- Author entity engagement metrics (LinkedIn follower growth, podcast appearances, conference invitations)
- Traditional referring domain count (still tracked, no longer the headline)
The shift from #5 being the headline to #1 being the headline is the entire point of this guide.
How SoCal Sunrise generated 85 admissions and 2,297% ROI from SEO in 6 months
A ground-up SEO rebuild using the Pathfinder Parents Methodology turned an invisible online presence into a top-ranking admissions engine.
Read the case study →85 admits and 3,152 leads attributed to organic
What a 12-Month Earned-Link Program Looks Like
Foundation (Q1)
Author bios deployed, clinical leadership LinkedIn polished, original research scoped with IRB and legal review. The credentialing and asset work that the rest of the year compounds on.
Earn + Amplify (Q2-Q3)
Research published, 6-10 industry publication pitches sent, derivative content scheduled (op-eds, podcasts, conference proposals). The active earned-media phase.
Rebase (Q4)
AI citation share measured against the baseline, topical authority signals assessed, underperforming tactics pruned, the following year’s research scope drafted.
A real earned-link program for a treatment center, structured to operate inside the 2026 reality, has the following shape.
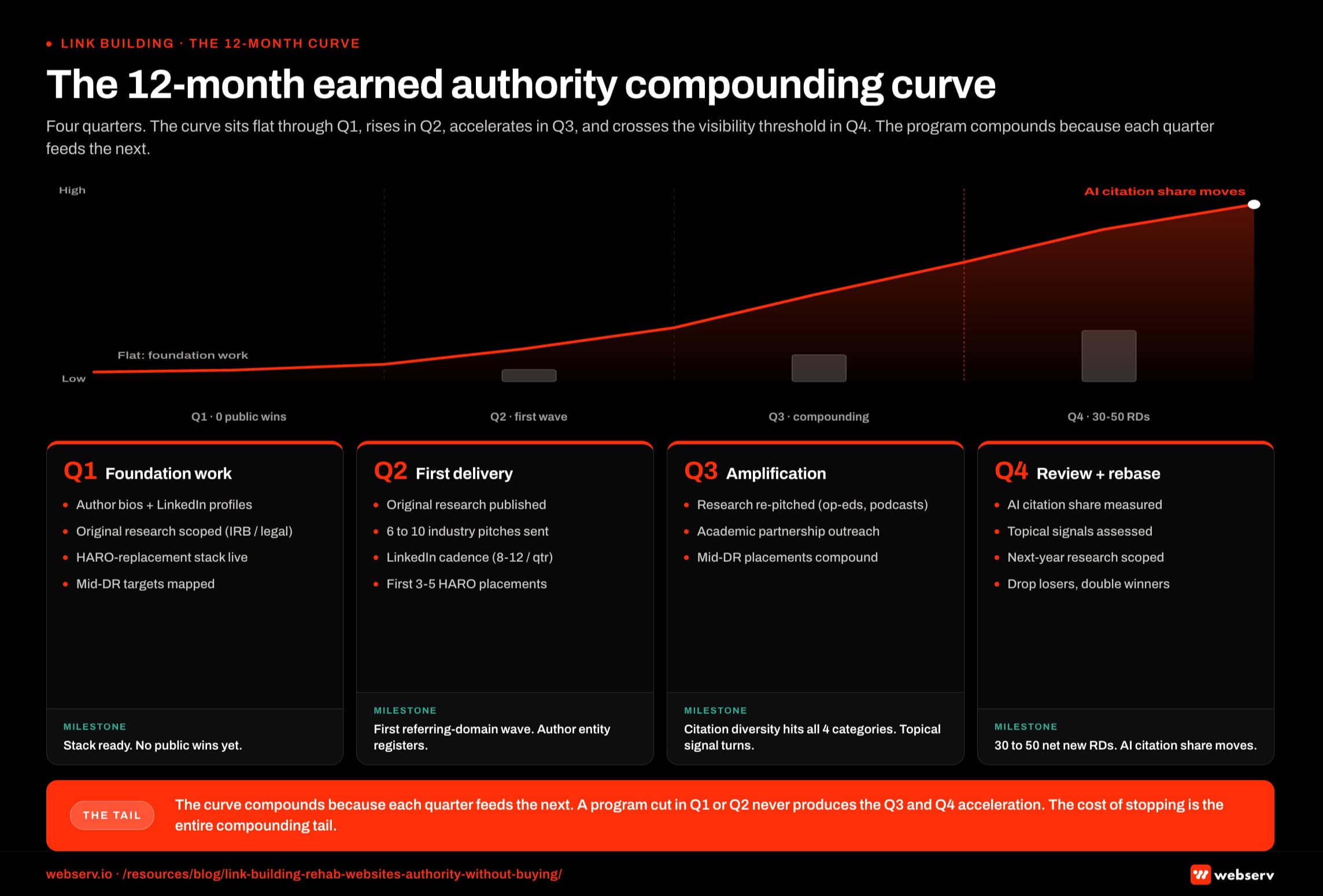 Infographic titled ‘The 12-month earned authority compounding curve’ showing how earned authority accumulates across the four quarters of a 12-month program for a rehab or treatment center, rendered as a line chart spanning four quarter columns Q1 through Q4 with a stepped bar layer underneath showing deliverable counts per quarter. The curve sits flat through Q1 (foundation work, no public wins), rises modestly across Q2 as the first deliverables land, accelerates across Q3 as the layers compound, and continues climbing into Q4 where the program crosses the visibility threshold and AI citation share begins to move. Q1 is the foundation quarter: author bios rolled out, clinical LinkedIn profiles built, original research scoped with IRB and legal review initiated, HARO-replacement stack subscriptions activated, mid-DR target publication relationships mapped; quarter-end milestone is the stack ready with no public wins yet. Q2 is the first delivery quarter: original research published, industry publication pitches sent (target 6 to 10 placements), LinkedIn long-form cadence established (target 8 to 12 posts per quarter per featured author), first 3 to 5 HARO-stack placements logged; milestone is the first referring domain wave and the author entity starting to register. Q3 is the amplification quarter: research re-pitched as op-eds, podcast appearances, and conference proposals; partnership outreach to academic institutions; mid-DR placement count compounding; milestone is citation diversity hitting all four source categories and the topical authority signal turning. Q4 is the review and rebase quarter: AI citation share measured against baseline, topical authority signals assessed, next year’s research scoped, underperforming tactics dropped, overperforming ones doubled; milestone is 30 to 50 net new referring domains across the four diversity categories and AI citation share moving. Q1 callout: Q1 produces no public wins, the quarter most programs get killed because leadership cannot see foundation work. Q2 callout: the first referring domain wave lands in Q2 and the curve starts to bend. Q3 callout: Q3 is where the layers compound and the curve steepens fastest. Q4 callout: by Q4 AI citation share moves and cost per admit on organic becomes defensible. Bottom strip callout: the curve compounds because each quarter feeds the next, a program cut in Q1 or Q2 never produces Q3 and Q4 acceleration, and the cost of stopping is the entire compounding tail.
Infographic titled ‘The 12-month earned authority compounding curve’ showing how earned authority accumulates across the four quarters of a 12-month program for a rehab or treatment center, rendered as a line chart spanning four quarter columns Q1 through Q4 with a stepped bar layer underneath showing deliverable counts per quarter. The curve sits flat through Q1 (foundation work, no public wins), rises modestly across Q2 as the first deliverables land, accelerates across Q3 as the layers compound, and continues climbing into Q4 where the program crosses the visibility threshold and AI citation share begins to move. Q1 is the foundation quarter: author bios rolled out, clinical LinkedIn profiles built, original research scoped with IRB and legal review initiated, HARO-replacement stack subscriptions activated, mid-DR target publication relationships mapped; quarter-end milestone is the stack ready with no public wins yet. Q2 is the first delivery quarter: original research published, industry publication pitches sent (target 6 to 10 placements), LinkedIn long-form cadence established (target 8 to 12 posts per quarter per featured author), first 3 to 5 HARO-stack placements logged; milestone is the first referring domain wave and the author entity starting to register. Q3 is the amplification quarter: research re-pitched as op-eds, podcast appearances, and conference proposals; partnership outreach to academic institutions; mid-DR placement count compounding; milestone is citation diversity hitting all four source categories and the topical authority signal turning. Q4 is the review and rebase quarter: AI citation share measured against baseline, topical authority signals assessed, next year’s research scoped, underperforming tactics dropped, overperforming ones doubled; milestone is 30 to 50 net new referring domains across the four diversity categories and AI citation share moving. Q1 callout: Q1 produces no public wins, the quarter most programs get killed because leadership cannot see foundation work. Q2 callout: the first referring domain wave lands in Q2 and the curve starts to bend. Q3 callout: Q3 is where the layers compound and the curve steepens fastest. Q4 callout: by Q4 AI citation share moves and cost per admit on organic becomes defensible. Bottom strip callout: the curve compounds because each quarter feeds the next, a program cut in Q1 or Q2 never produces Q3 and Q4 acceleration, and the cost of stopping is the entire compounding tail.Quarterly Cadence
Q1: foundation work. Author bios rolled out, clinical leadership LinkedIn profiles built or polished, original research scoped and IRB/legal review initiated, HARO-replacement stack subscriptions activated, mid-DR target publication relationships mapped.
Q2: original research delivered. Industry publication pitches sent (target: 6-10 placements). LinkedIn long-form cadence established (target: 8-12 posts per quarter per featured author). First 3-5 HARO-stack placements logged.
Q3: amplification phase. Research findings re-pitched as derivative content (op-eds, podcast appearances, conference proposals). Partnership outreach to academic institutions. Mid-DR placement count compounds.
Q4: review and rebase. AI citation share measured against baseline. Topical authority signals assessed. Following year’s research scoped. Underperforming tactics dropped, overperforming ones doubled.
Deliverable Counts
A well-run program in 2026 produces approximately:
- 30-50 net new referring domains over 12 months, across the four diversity categories
- 10-20 mid-DR vertical industry publication placements
- 1-2 original research reports published
- 50-100 author-authored LinkedIn long-form pieces across the clinical team
- 6-12 podcast appearances logged
- 3-6 academic or institutional partnerships initiated
Budget Allocation
Total program cost for a regional treatment center group typically lands in the $120,000-$240,000 per year range for an in-house operating model, or $96,000-$180,000 per year as an agency-managed retainer.
The retainer model is cheaper because the fixed staff costs amortize across multiple clients.
The allocation inside the budget looks like:
- 30-40% to original research (production cost + design + clinical co-authoring)
- 25-30% to outreach and pitching labor (HARO stack, mid-DR pubs, podcast)
- 20-25% to compliance and legal review (the layer most programs underfund)
- 10-15% to measurement infrastructure (Profound or AthenaHQ subscription)
- 5-10% to author entity building support (LinkedIn editor, podcast booking)
Compared to the $50,000-per-quarter “guaranteed DR70 links” program in my intro, this looks similar on top-line spend and dramatically different on risk-adjusted outcome.
The deeper economics, including the relationship between SEO investment level and market competitiveness, depend on facility size and competitive context.
Most in-house teams hit a wall not because they lack knowledge, but because they lack bandwidth.
When you are ready to hand it off, Webserv has spent 9 years executing exactly this for treatment centers nationwide.
Frequently Asked Questions
Are backlinks still important for rehab SEO in 2026?
Yes, but the way backlinks matter has shifted meaningfully. Traditional Google rankings still respond to backlink profile, particularly for commercial-intent head terms where domain authority remains a meaningful signal. A treatment center with a credible link profile still outranks a thin one on most competitive keywords.
The change is that the value of backlinks now compounds with brand entity recognition, topical authority, and citation diversity in ways it didn’t five years ago. A backlink from a topically aligned mid-DR vertical publication produces more aggregate authority lift than a backlink from a high-DR generalist site that’s topically misaligned.
For treatment centers planning a 2026 earned-link program, the right framing isn’t “should we still build links.” It’s “what’s the right composition of our citation profile across the four diversity categories, and how do we earn placements that compound across both Google rankings and AI citation share.”
Is it ever okay to pay for a backlink in 2026?
Sponsored content is permissible under Google’s guidelines when it’s clearly disclosed with appropriate rel attributes (rel=”sponsored” or rel=”nofollow”). The placements that get penalized are paid arrangements that obscure the paid nature, link schemes that disguise commercial intent, and bulk paid placements designed to manipulate ranking signals.
For treatment centers specifically, paid placements come with additional compliance risk. EKRA exposure exists if the arrangement could be construed as a referral mechanism. LegitScript Certification can be jeopardized by certain affiliate-style arrangements. The risk profile is higher in behavioral health than in most other verticals.
The cleanest framework is: never pay for placements that pass link equity (nofollow or sponsored attribution is the floor), and avoid even sponsored placements if the publication cannot articulate its editorial separation from the commercial relationship. If a placement requires obscured disclosure to look credible, the placement is not worth doing.
How long does an earned-link program take to show meaningful results?
Most treatment center earned-link programs show leading indicator movement (referring domain growth, mid-DR vertical placements logged, AI citation share lifts) within 3 to 6 months of program launch. Meaningful Google ranking impact from the link earning typically expresses between months 6 and 12. Compounding effects on AI citation share and topical authority continue for years after the initial program work.
The timeline is longer than buying links, which can produce ranking lifts in 60 to 90 days for the placements that don’t get caught by enforcement updates. The total cost of ownership over 24-36 months meaningfully favors the earned approach once you adjust for risk and recovery costs.
Programs that try to compress the timeline by mixing earned and paid tactics tend to produce ambiguous results: hard to tell which placements drove which lifts, hard to disavow problem links cleanly when enforcement updates land. Clean separation is operationally better.
What’s the difference between earned media and paid placements?
Earned media is content placement that happens because an editor decided the content was worth publishing on its own merit. The treatment center provided source material, expert commentary, original data, or a credible pitch. The publication assessed editorial value and made an independent decision to publish.
Paid placements include sponsored content, paid contributor arrangements, guest post payments to publication editors or webmasters, and any arrangement where money changes hands in exchange for placement. The placement may still be high-quality content, but the publication decision was influenced by the payment.
The signals these produce differ. Earned media carries editorial endorsement, which translates to higher reader trust, stronger algorithmic credibility, and resilience against enforcement updates. Paid placements pass weaker signals at best and create penalty exposure at worst. The cost difference is real but the risk-adjusted value of earned media is meaningfully higher.
How do I measure if my earned-link program is working?
Five metrics cover the working surface of an earned-link program. AI citation share growth against a defined competitive set, tracked monthly through Profound or AthenaHQ. Referring domain growth, broken out by source category.
Branded search volume growth as a proxy for entity recognition strength. Author entity engagement metrics including LinkedIn follower growth and podcast appearances. And traditional ranking and organic traffic metrics for the commercial keywords that drive admissions.
The mistake most operators make is over-weighting the last metric early in a program. Rankings and traffic lag the leading indicators by 90 to 180 days. A program that’s producing strong leading indicator movement at month 4 but flat traffic is on track, not behind. The decision point at month 6 is whether AI citation share and referring domain growth are tracking against baseline expectations.
Can a small or mid-size treatment center afford a credible earned-link program?
A single-location facility with a $5,000-$8,000 per month marketing budget can run a meaningful earned-link program if the allocation is correct. The components that scale down well are the HARO-replacement stack (Qwoted subscription, manual pitching by the marketing lead, free Source of Sources access) and the LinkedIn long-form author cadence (founder or clinical director publishing 2-4 times per month).
The components that don’t scale down well are original research (which has a credibility floor below which it doesn’t earn placements) and the institutional partnership work (which requires a senior outreach lead’s time commitment).
For sub-$5,000 per month budgets, the right pattern is to concentrate everything on author entity building and HARO-stack response. Skip the research and partnerships until the budget supports doing them well. Trying to do credibility-light versions of the higher-investment tactics produces no placements, just wasted hours.
What’s the role of HARO and HARO alternatives in 2026?
The HARO category collapsed in 2024 when Cision restructured the original HARO into Connectively, which itself wound down by late 2024. The 2026 replacement isn’t a single platform but a stack. Qwoted ($99-$149/month, highest conversion rate, healthcare is a strong vertical). Featured.com, which bought the HARO brand back from Cision in April 2025 and revived it as a free daily newsletter.
Source of Sources from Peter Shankman (free, honor-system, lower noise). And #JournoRequest on X (fastest response window, no platform overhead).
The right cadence for treatment centers is daily monitoring across all four channels, with response pitches sent within 30 minutes of a relevant query. Real programs produce 3 to 8 placements per month through this stack alone, with mid-DR vertical publications and quote-driven roundups being the most reliable categories. Every response needs to pass LegitScript-compliant messaging and ASAM-aligned positioning before it leaves the inbox.
How does Webserv think about Digital PR for behavioral health clients?
Our Digital PR practice operates inside the framework this guide describes. We treat earned-link programs as authority engines that produce AI citation lift, brand entity recognition, and topical authority compounding, with traditional referring domain count as a downstream indicator rather than a headline metric.
Programs are structured around quarterly cadence: foundation work, original research production, amplification, and rebase. We integrate tightly with our SEO program for treatment centers so that on-page authority signals and off-page citation signals compound together rather than operating in silos.
We don’t sell guaranteed-placement contracts, because the placements that get guaranteed in writing are almost always the ones with the highest compliance and enforcement risk. We commit to processes (research production, pitching cadence, author entity work) and report against the KPI hierarchy outlined above.
Build a Citation-First Digital PR Program
The treatment center earned-link playbook for 2026 looks meaningfully different from the playbook five years ago. The components that worked then are now liability-creating. The components that work now require longer time horizons, deeper compliance integration, and clearer alignment between earned media and AI citation share.
We build citation-first Digital PR programs for behavioral health brands that produce authority compounding across Google rankings, AI Mode citations, ChatGPT and Perplexity surface area, and brand entity recognition.
The work integrates with our broader SEO and content program for treatment centers so authority lift on the link earning side reinforces the on-page authority signals downstream.
Schedule a Digital PR audit to see where your current program stands against the new authority benchmarks, where the gaps are in your citation diversity profile, and what a reallocated budget could produce for your facility over the next 12 months.
For the wider picture of how Digital PR fits inside a full treatment center marketing program, see our ultimate guide to behavioral health marketing.
Trevor Gage is Director of SEO at Webserv, where he leads organic strategy, Digital PR, and AEO programs for behavioral health and addiction treatment centers across the U.S. He writes about treatment-center SEO economics, AI search citation, and the operational realities of marketing high-acuity healthcare.