Most behavioral health treatment centers run creative as an afterthought. The agency makes ads that look reasonable. The center approves them because they look like ads. Six months later the ads stop working and nobody can articulate why.
The reason is that the strategy was inherited from category convention rather than built on purpose. A working creative strategy for treatment center marketing is the layer that prevents this drift.
The behavioral health category is uniquely constrained. HIPAA, Meta’s self-harm classification, Google’s Healthcare and Medicines policy, FTC enforcement on outcome claims, and LegitScript certification combine into a creative space that is narrower than almost any other vertical.
The operators winning the category use each constraint as a creative forcing function instead of a creative ceiling.
This guide covers what creative strategy means in this category, the constraints that shape every decision, the audiences and voices that matter, the brand foundation, channel-specific creative principles, the testing discipline, the production pipeline, common mistakes, and the measurement framework that ties everything back to admits.
Creative strategy in this category is unusually difficult to do well because the constraint stack is unusually severe. HIPAA limits testimonials. The self-harm classification on Meta limits framing. The Healthcare and Medicines policy on Google limits headlines. The FTC limits outcome claims.
LegitScript limits who is allowed to advertise at all. Every operator faces the same constraints. Most operators respond to them with creative that looks identical to every other treatment center’s creative.
The centers that win in 2026 are the ones that built a creative strategy that treats those constraints as the starting line rather than the finish line. Family-member voice instead of patient voice. Real clinical leadership instead of stock professionals.
Specific positioning instead of “compassionate care.” Tested testimonials with consent and disclosure instead of unverified outcome claims. Each constraint is a forcing function that, handled correctly, becomes a competitive differentiator.
Most rehab creative is interchangeable because most rehab creative was made to be safe inside the constraint stack. The centers that win in this category make creative that is safe inside the constraints and unmistakable outside them. Same rules. Different outcome.
Trevor Gage, Director of Earned & Owned Media, Webserv
Key Takeaways
- Creative strategy is upstream of creative production. Production decides whether an ad gets made; strategy decides what to make, for whom, in what voice, with what visual treatment, in what channel mix. Most operators have implicit strategy inherited from category convention, which is why their creative looks like everyone else’s.
- Five constraints shape every creative decision in this category: HIPAA, Meta self-harm classification, Google Healthcare & Medicines policy, FTC enforcement on outcome claims, and LegitScript certification. Each one, taken seriously, becomes a competitive forcing function, not a creative ceiling.
- The audience framework matters more than the channel framework. Family members account for 60-70% of inbound treatment center inquiries. Patient voice (“Are you struggling with addiction?”) misses the audience and underconverts. Family-member voice (“When your son tells you he needs help, here is what to do next”) converts and sidesteps the self-harm policy flag.
- The four documents every treatment center needs: positioning statement (one paragraph), voice guide (two pages), visual identity guide, message architecture. Operators who maintain these four documents quarterly produce creative that compounds. Operators without them produce creative that resets every quarter.
- Cost per admit declines 2% to 4% month over month for the first six months in a well-run creative strategy program as testing finds winners and channel mix optimizes. After six months it stabilizes and the program scales by adding budget rather than improving efficiency. Operators whose cost per admit is rising are running a strategy that has stopped working. The fix is usually rebuilding the foundation, not adding channels.
This guide is the operator-facing version of how we think about creative strategy at Webserv.
It covers what creative strategy means in this category, the constraint stack you have to work inside, the audience framework that produces the right voice across channels, and the brand foundation work that most operators skip.
It then covers the channel-specific principles for paid social, paid search, organic content, landing pages, video, email, and local. The testing discipline that compounds creative performance over time. The production pipeline decisions that determine whether the strategy executes.
The most common creative strategy mistakes we audit and see repeated, and the measurement framework that tells you whether the strategy is working.
The audience for this guide is treatment center operators and the marketing leads who report to them. The depth is set for the buyer who has to make budget and direction decisions, not for the production team executing them. Specific tactical depth lives in the cluster spokes referenced throughout.
DEFINITION
Creative-to-Spend Ratio
The ratio of unique creative assets shipped per dollar of paid media spend. For behavioral health operators in 2026, the working range is one new creative per $1,500-$3,000 of monthly Meta and TikTok spend. Below that ratio, creative fatigue caps the program. Above it, production cost outruns the lift.
Part 1. What “creative strategy” means in this category
Creative strategy for behavioral health marketing is the layer underneath every ad, landing page, video, email, and organic asset a treatment center ships. The operators who run it explicitly produce work that compounds.
The operators who let category convention dictate the strategy ship work that looks technically correct and converts at category-average rates.
Creative strategy is the integrated set of decisions about voice, audience, visual identity, message architecture, and format mix that runs across every channel the operator uses to reach families.
It is upstream of creative production. Production decides whether a specific ad gets made. Strategy decides what to make, for whom, in what voice, with what visual treatment, in what channel mix.
For most operators, creative strategy is implicit rather than explicit. The agency makes ads that look reasonable. The center approves them because they look like ads. Six months later the ads stop working and nobody can articulate why.
The reason is that the strategy was inherited from category convention rather than built on purpose.
An explicit creative strategy answers six questions in advance:
| Question | What a working answer looks like |
|---|---|
| Who are we addressing on each channel? | Family member, patient, professional referrer, alumni, or general public. Each audience requires different voice and different message architecture. |
| What is our specific positioning? | The one or two things this facility does that no other facility in the relevant comparison set does as well. Not “compassionate care.” Specific: “Veteran-built residential program in Texas with VA CCN Region 1 contract and named medical director on every admission.” |
| What is our voice? | Tone, vocabulary, sentence structure, default emotional register. Clinical and direct, or warm and reassuring, or operator-blunt and unsentimental. Consistent across channels and recognizable. |
| What is our visual identity? | Color, typography, photography style, accreditation badges, founder portraiture. Reads consistently across paid ads, the website, email, and local print. |
| What channels are we creative-on, and what is the budget allocation? | Not every channel deserves equal investment. The right allocation depends on operator size, market position, payer mix, and admit goal. |
| What does success look like in 90 days, 6 months, 12 months? | Without success metrics defined in advance, the creative direction drifts to whatever the team feels good about producing rather than what produces admits. |
Operators who answer those six questions explicitly produce creative that compounds over time. Operators who do not produce creative that resets every quarter.
Part 2. The constraint stack
The five constraints that shape every creative decision in this category. Each one is non-negotiable. The strategy is built around them, not despite them.
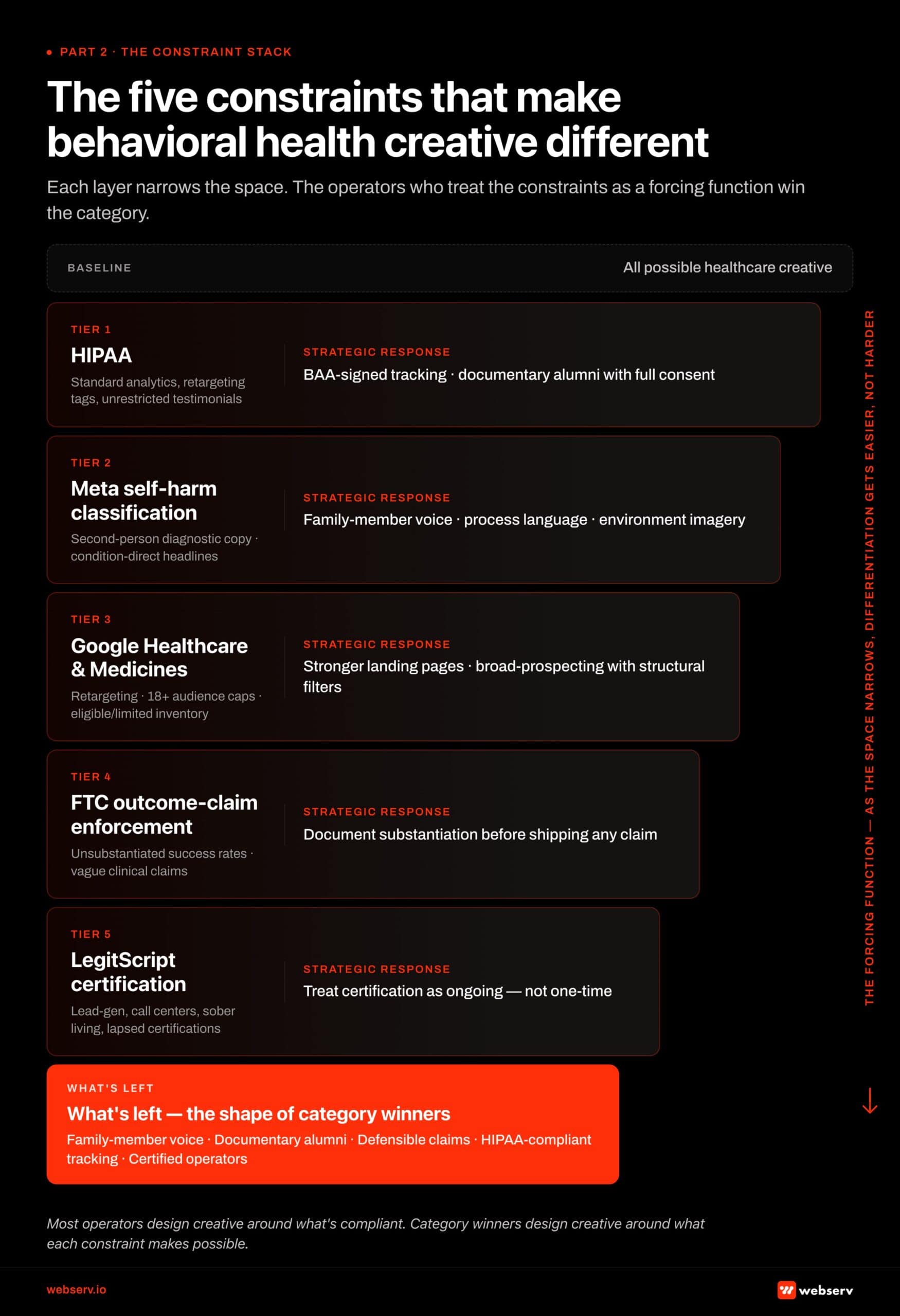 Infographic titled ‘The five constraints that make behavioral health creative different.’ Vertical five-tier stack showing each compliance constraint narrowing the creative space available to addiction treatment marketers. Tier 1 (widest) represents all possible healthcare creative. Tier 2 HIPAA narrows the space by restricting standard analytics, retargeting tags, and unrestricted patient testimonials; strategic response is BAA-signed tracking intermediaries and documentary alumni stories with full consent. Tier 3 Meta self-harm classification further narrows by restricting second-person diagnostic copy, condition-direct headlines, and before/after imagery; strategic response is family-member voice and process language. Tier 4 Google Healthcare and Medicines policy narrows by restricting retargeting, applying 18+ audience caps, and routing inventory through eligible/limited status; strategic response is stronger landing pages and broad-prospecting with structural filters. Tier 5 FTC enforcement narrows by restricting unsubstantiated success rates; strategic response is documenting substantiation before shipping any claim. Tier 6 LegitScript certification narrows by excluding lead-generators, call centers, sober living, and lapsed certifications; strategic response is treating certification as ongoing. Survivor band at the bottom: family-member voice, documentary alumni stories, defensible claims, HIPAA-compliant tracking, certified operators. Right-margin arrow labeled ‘The forcing function: as the space narrows, differentiation gets easier, not harder.’
Infographic titled ‘The five constraints that make behavioral health creative different.’ Vertical five-tier stack showing each compliance constraint narrowing the creative space available to addiction treatment marketers. Tier 1 (widest) represents all possible healthcare creative. Tier 2 HIPAA narrows the space by restricting standard analytics, retargeting tags, and unrestricted patient testimonials; strategic response is BAA-signed tracking intermediaries and documentary alumni stories with full consent. Tier 3 Meta self-harm classification further narrows by restricting second-person diagnostic copy, condition-direct headlines, and before/after imagery; strategic response is family-member voice and process language. Tier 4 Google Healthcare and Medicines policy narrows by restricting retargeting, applying 18+ audience caps, and routing inventory through eligible/limited status; strategic response is stronger landing pages and broad-prospecting with structural filters. Tier 5 FTC enforcement narrows by restricting unsubstantiated success rates; strategic response is documenting substantiation before shipping any claim. Tier 6 LegitScript certification narrows by excluding lead-generators, call centers, sober living, and lapsed certifications; strategic response is treating certification as ongoing. Survivor band at the bottom: family-member voice, documentary alumni stories, defensible claims, HIPAA-compliant tracking, certified operators. Right-margin arrow labeled ‘The forcing function: as the space narrows, differentiation gets easier, not harder.’| Constraint | What it limits | Strategic response |
|---|---|---|
| HIPAA | Patient testimonials require explicit consent, controlled clinical disclosure, and FTC-compliant attribution if compensation was involved. Standard analytics and retargeting tags that work on ecommerce sites are non-compliant on a treatment center site. | Tracking runs through a HIPAA-compliant intermediary with a signed BAA. Patient stories use documentary alumni testimonials with full consent. See our Meta CAPI HIPAA setup guide and the HIPAA marketing compliance glossary. |
| Meta self-harm classification | Substance use disorder is routed through Meta’s self-harm enforcement stack, operationally stricter than mental health. Second-person diagnostic language gets flagged. Direct condition references in headlines get flagged. Before-and-after imagery gets pulled. | Compliant creative defaults to family-member voice and process language. See our HIPAA-compliant Facebook ads playbook. |
| Google Healthcare and Medicines policy | Addiction treatment ads run as eligible/limited inventory with 18+ audience caps and no retargeting. The audience play is broad prospecting with structural filters (income tier, geography) layered on. | Creative has to work without retargeting nurture. Stronger landing page work, clearer trust signals, and search intent matched to landing page above the fold. |
| FTC enforcement on outcome claims | The FTC issued 30 warning letters to substance use treatment providers in March 2026 about advertising claims. “85% sobriety rate” without published methodology is a liability. | Make defensible claims or no claims at all. Document the substantiation for any clinical or quality claim before it ships. |
| LegitScript certification | Lead generators and call centers that resell admits are excluded. Sober living homes are excluded. Operators whose certification lapses are pulled from inventory immediately. | The certification is gating and ongoing, not one-time. The Meta-side certification is a separate workflow from the Google-side certification. |
The compound effect of the five constraints is that most operators default to creative that is technically compliant and competitively interchangeable. The centers winning the category use the constraints as a creative forcing function.
The HIPAA limit on testimonials becomes the case for documentary-style alumni storytelling produced with full consent. The self-harm classification becomes the case for family-member voice that converts higher anyway. The Healthcare and Medicines audience cap becomes the case for stronger landing page work and clearer trust signals.
Each constraint, taken seriously, becomes a competitive advantage.
Part 3. The audience framework
The most important strategic decision in creative for this category is who the creative is addressed to. Operators who get this wrong produce creative that misses both audiences. Operators who get it right produce creative that converts because the voice matches the listener.
 Infographic titled ‘Four audiences. Four voices. One brand spine.’ 2×2 grid of persona cards sized proportionally to share of inbound conversion volume in behavioral health marketing. The Family Member card is the largest at 60-70% of inbound, including spouses, parents, adult children, and siblings searching for treatment on behalf of someone else; converts on practical ‘what to do when’ framing in family-member voice; primary channels are paid social, ‘near me’ paid search, and organic search; flipped off by diagnostic second-person copy aimed at the patient. The Patient card at 10-20% covers self-referred patients who recognize their own need; responds to direct address used carefully without diagnostic second-person; primary channels are Reddit recovery communities, organic queries, and alumni-referred inbound; flipped off by clinical-distancing language. The Professional Referrer card at 5-15% covers EAP coordinators, PCPs, school counselors, courts, interventionists, and attorneys; responds to clinical and operational language about capacity, outcomes, and referral process; primary channels are LinkedIn outreach and referral-specific landing pages; flipped off by consumer-facing marketing tone. The Alumni card at 5-10% covers past patients in contact with the program; responds to community language about program updates and family events; primary channels are email and private community; flipped off by marketing-tone communication. Center divider separates high-volume audiences (Family, Patient) from high-leverage audiences (Referrer, Alumni). Footer: ‘These are not four separate creative tracks. They are four products of the same strategy.’
Infographic titled ‘Four audiences. Four voices. One brand spine.’ 2×2 grid of persona cards sized proportionally to share of inbound conversion volume in behavioral health marketing. The Family Member card is the largest at 60-70% of inbound, including spouses, parents, adult children, and siblings searching for treatment on behalf of someone else; converts on practical ‘what to do when’ framing in family-member voice; primary channels are paid social, ‘near me’ paid search, and organic search; flipped off by diagnostic second-person copy aimed at the patient. The Patient card at 10-20% covers self-referred patients who recognize their own need; responds to direct address used carefully without diagnostic second-person; primary channels are Reddit recovery communities, organic queries, and alumni-referred inbound; flipped off by clinical-distancing language. The Professional Referrer card at 5-15% covers EAP coordinators, PCPs, school counselors, courts, interventionists, and attorneys; responds to clinical and operational language about capacity, outcomes, and referral process; primary channels are LinkedIn outreach and referral-specific landing pages; flipped off by consumer-facing marketing tone. The Alumni card at 5-10% covers past patients in contact with the program; responds to community language about program updates and family events; primary channels are email and private community; flipped off by marketing-tone communication. Center divider separates high-volume audiences (Family, Patient) from high-leverage audiences (Referrer, Alumni). Footer: ‘These are not four separate creative tracks. They are four products of the same strategy.’The four audiences that matter, in order of typical conversion volume:
| Audience | When they convert | Voice they respond to |
|---|---|---|
| The family member | Spouse, parent, adult child, sibling. 60-70% of inbound treatment center inquiries. The person searching for treatment is usually not the patient. | Practical next-step information, framed as “what to do when…” rather than diagnostic. Family-member voice is the default for most rehab creative. |
| The patient | Self-referred patients who recognize their own need for treatment. A smaller share of inbound demand. | Direct address used carefully. Second-person diagnostic (“are you struggling”) triggers Meta’s self-harm enforcement. The right channels for patient voice are Reddit recovery communities, certain organic search queries, and alumni-referred inbound. |
| The professional referrer | EAP coordinator, primary care physician, school counselor, juvenile court system, interventionist, behavioral health attorney. Recommends facilities to patients and families who do call. | Clinical and operational language. Capacity, outcomes documentation, referral process, communication with the referring clinician. |
| The alumni | Past patients who have stayed in contact with the program. Source of word-of-mouth referrals, peer support traffic, and earned media through documentary storytelling. | Community language. Program updates, recovery resources, family events. Not marketing tone. |
The audience framework does not mean creating four separate creative tracks. It means knowing which audience each piece of creative is for, writing in the voice that audience responds to, and distributing each piece through the channels that audience uses.
A piece of paid social creative addressed to family members and a piece of LinkedIn outreach addressed to EAP coordinators are not slight variations of the same message. They are different products of the same strategy. The shared spine is the brand positioning.
The differentiated outputs are the voice, the message architecture, and the channel.
Part 4. Brand foundation
Brand foundation is the work most operators skip because it does not look urgent next to the paid media account. The shortcut is to skip the foundation and ship campaigns. The result is creative that drifts. Three months later the team is producing ads that contradict each other’s positioning.
Six months later the brand reads as generic.
The brand foundation work connects to the web design and web development surfaces. Operators who finalize brand positioning but never push it through the site experience produce work that reads as inconsistent. Brand consistency across blog, landing page, paid creative, and email is what makes the strategy compound.
A working brand foundation for a treatment center has four documents:
The positioning statement
One paragraph. What the facility does, for whom, against what alternative, with what specific differentiator. “We provide residential addiction treatment for veterans and first responders, who are underserved by generic treatment centers because they need clinical and peer environments built around the specific trauma stack their roles produce.
We are the only program in the country with [specific credential] and our medical director is [named person with credential].”
The voice guide
Two pages. The vocabulary the brand uses and the vocabulary it does not. Default emotional register. Examples of on-voice copy and off-voice copy. Tone calibration for different audiences and channels.
The visual identity guide
Color palette, typography, photography style, accreditation badge placement, founder and clinical leadership portraiture standards. Specific enough that an agency or a junior designer can produce on-brand assets without senior review.
The message architecture
The five to seven core message points the brand can defend and uses across channels. The differentiators, the trust signals, the proof points, the audience-specific framing, the call to action language.
The message architecture is what makes the creative recognizable as belonging to the same brand across paid social, paid search, organic content, the website, email, and local print.
Operators who maintain those four documents and update them quarterly produce creative that compounds. Operators without them produce creative that resets every quarter when a new agency or a new internal lead takes over.
Part 5. Channel-specific creative principles
The strategy lives at the brand level. The execution lives at the channel level. The channel-specific principles below are the working defaults for treatment center marketing in 2026.
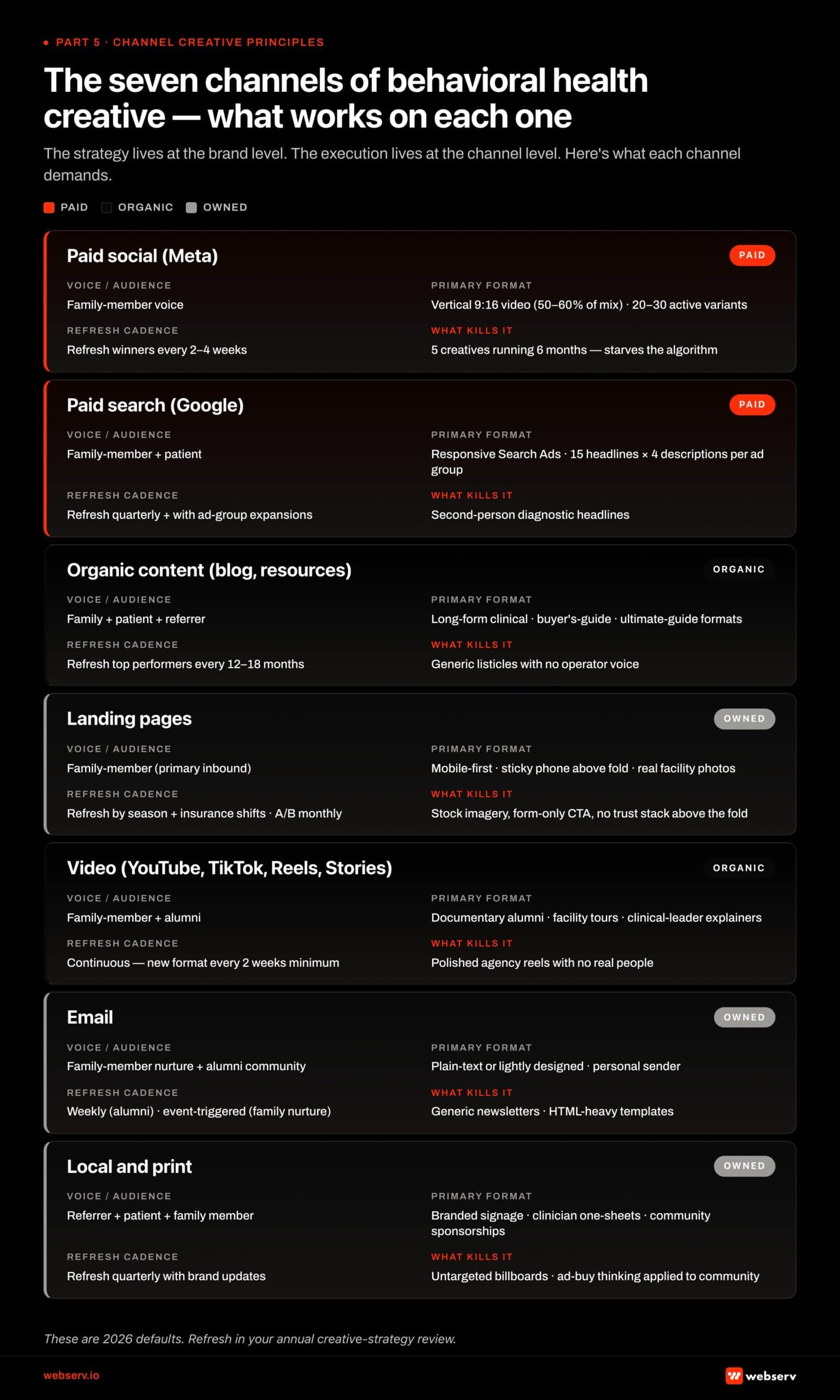 Infographic titled ‘The seven channels of behavioral health creative: what works on each one.’ Matrix grid showing seven marketing channels each evaluated across four creative dimensions: voice/audience, primary format, refresh cadence, and what kills it. Paid social (Meta) targets family-member voice with vertical 9:16 video at 50-60% of mix and 20-30 active variants, refreshed every 2-4 weeks, killed by 5 creatives running 6 months. Paid search (Google) targets family-member and patient voice with Responsive Search Ads (15 headlines x 4 descriptions per ad group), refreshed quarterly, killed by second-person diagnostic headlines. Organic content targets family-member, patient, and referrer with long-form clinical content, refreshed every 12-18 months, killed by generic listicles with no operator voice. Landing pages target family-member with mobile-first sticky-phone-above-the-fold design featuring real facility photos and specific USP, refreshed by season and tested monthly, killed by stock imagery and form-only CTAs. Video targets family-member and alumni with documentary alumni storytelling, facility tours, and clinical-leader explainers, refreshed continuously with new format every 2 weeks, killed by polished agency reels with no real people. Email targets family-member nurture and alumni community with plain-text personal sender, weekly to alumni and event-triggered for family nurture, killed by generic newsletters. Local and print target referrer, patient, and family member with branded signage and clinician-facing one-sheets, refreshed quarterly, killed by untargeted billboards. Channel families color-coded: red for paid, black for organic, grey for owned. Footer: ‘These are 2026 defaults. Refresh in your annual creative-strategy review.’
Infographic titled ‘The seven channels of behavioral health creative: what works on each one.’ Matrix grid showing seven marketing channels each evaluated across four creative dimensions: voice/audience, primary format, refresh cadence, and what kills it. Paid social (Meta) targets family-member voice with vertical 9:16 video at 50-60% of mix and 20-30 active variants, refreshed every 2-4 weeks, killed by 5 creatives running 6 months. Paid search (Google) targets family-member and patient voice with Responsive Search Ads (15 headlines x 4 descriptions per ad group), refreshed quarterly, killed by second-person diagnostic headlines. Organic content targets family-member, patient, and referrer with long-form clinical content, refreshed every 12-18 months, killed by generic listicles with no operator voice. Landing pages target family-member with mobile-first sticky-phone-above-the-fold design featuring real facility photos and specific USP, refreshed by season and tested monthly, killed by stock imagery and form-only CTAs. Video targets family-member and alumni with documentary alumni storytelling, facility tours, and clinical-leader explainers, refreshed continuously with new format every 2 weeks, killed by polished agency reels with no real people. Email targets family-member nurture and alumni community with plain-text personal sender, weekly to alumni and event-triggered for family nurture, killed by generic newsletters. Local and print target referrer, patient, and family member with branded signage and clinician-facing one-sheets, refreshed quarterly, killed by untargeted billboards. Channel families color-coded: red for paid, black for organic, grey for owned. Footer: ‘These are 2026 defaults. Refresh in your annual creative-strategy review.’Paid social (Meta)
Family-member voice. Vertical video as the primary format (9:16, 50% to 60% of the active mix). 20 to 30 active creative variants minimum per Advantage+ campaign. Refresh winners every 2 to 4 weeks. HIPAA-compliant CAPI through a BAA-signed intermediary.
The full mechanics are in our piece on under-investment in rehab Facebook creative and the 18 battle-tested Meta tactics for rehab.
The Meta creative principle that matters most: the algorithm needs volume and diversity to optimize. Five creatives running for six months starves the system. Twenty to thirty active variants with continuous refresh feeds it.
Paid search (Google Ads)
Responsive Search Ads with 15 headlines and 4 descriptions per ad group, tailored to the search intent of the ad group. “Near me” modifiers in the headlines for high-intent geographic queries. Insurance carrier names where the operator is in-network. Population specifics for population-targeted campaigns.
Avoid second-person diagnostic headlines. “Aetna-Covered Detox in Phoenix” works. “Are You Struggling With Addiction?” gets flagged and underperforms even when approved. The full headline-language pattern is in our compliant ad headlines guide.
The paid search creative principle that matters most: the headline has to match the search intent and the landing page has to match the headline. A search for “TRICARE rehab Texas” should land on a page that says “TRICARE Rehab in Texas” above the fold, not the generic homepage.
Organic content (blog, resources)
Family-member-first voice. Long-form explainers and process walkthroughs over short-form thought leadership. Named clinician authorship on YMYL content (Medical Reviewer credit, real bio with PhD/LMFT credentials). Schema markup as the structured signal Google needs. Topical concentration in the program’s actual specialization rather than broad health topics.
See our topical authority guide for treatment centers for the architecture work that makes organic creative compound.
The organic content creative principle that matters most: depth over breadth. Sixty long, authoritative articles on what the program treats outperform 600 shallow articles on adjacent topics.
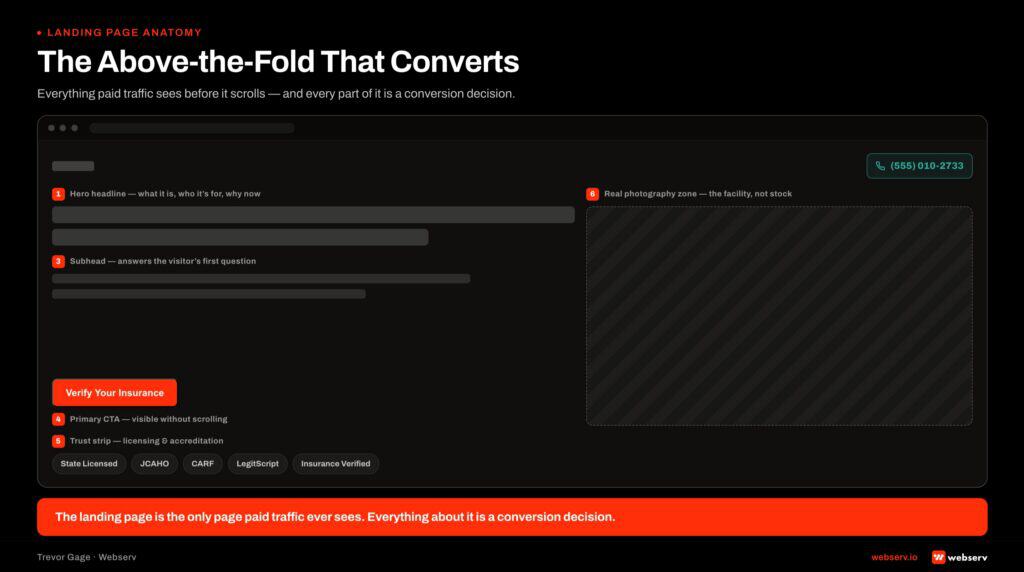
Landing pages
Mobile-first design. Call CTA primary, form CTA secondary. Confidentiality assurance above the fold. Joint Commission seal and named medical director visible without scrolling. Insurance verification prominently offered. Real facility imagery, not stock. Conversion rate target: 8% to 12% on paid search, 4% to 7% on paid social.
See our landing page conversion rate benchmarks for rehab.
The landing page creative principle that matters most: every element either earns the call or moves the visitor closer to making one.
Video (YouTube, TikTok, Reels, Stories)
YouTube long-form: 5 to 15 minute clinical explainers, founder stories, alumni documentaries (with consent and disclosure). Strong for SEO indirect traffic and brand searches. Cross-promotes Meta paid social Reels.
Reels and Stories: 15 to 60 seconds, audio-forward, native-style. Phone-shot facility tours and clinical team explainers outperform polished studio production.
TikTok: rarely productive for SUD-focused programs because of platform substance use restrictions. Sometimes productive for mental health and dual diagnosis programs with appropriate creative.
The video creative principle that matters most: authenticity outperforms polish. Real clinical leadership on camera outperforms stock professionals consistently.
Operator-direct copy. No marketing automation drip sequences that pretend to be personal. No “Dear [First Name]” personalization that feels manipulative.
Email works in this category for three audiences: alumni (program updates, recovery resources, family events), referral partners (clinical updates, capacity, partnership programs), and current admissions inquiries (process information, insurance verification, what-to-expect content). Email does not work for cold acquisition of patients or families.
The category is not search-substitutable through cold email.
The email creative principle that matters most: write like an admissions counselor would talk to a family member. Direct, specific, no marketing fluff.
Local and print
Print collateral, regional event sponsorships, local community materials. Lower volume than digital but high trust impact in regional markets. For multi-location operators or regional facilities, the local print stack matters more than national operators expect. EAP partner materials, sober living referral cards, hospital discharge planning brochures.
The local creative principle that matters most: consistency with the digital identity. The print materials should be recognizably the same brand as the website and the paid social.
A unified platform built for multiple locations, programs, and audiences without feeling fragmented
- Reorganized multi-service site architecture
- ADA compliant responsive design system
- Future-ready CMS with modular templates
- Optimized for SEO and lead capture
Part 6. The creative testing discipline
Creative strategy without a testing discipline is intuition. Creative testing without a strategy is randomness. The discipline that produces compounding creative performance is the integration of the two.
The testing framework we run inside Webserv accounts:
| Discipline | What it produces |
|---|---|
| The strategy hypothesis | Every creative variant tests a specific hypothesis about what produces admits. “Veteran-credential visual treatment outperforms generic clinical treatment on the veteran population campaign.” The hypothesis is what is being tested. The variant is the test artifact. |
| The variant volume target | 20 to 30 active variants in any tier 2 or tier 3 paid social account. 10 to 15 distinct concepts each in 2 to 3 format variants. The discipline is keeping the count high enough that the algorithm has options. |
| The evaluation window | 48 to 72 hours or $50 to $100 in spend for initial reads. 7 to 10 days or 100+ conversions for winner declaration. The discipline is not killing variants before they have signal and not promoting variants before they have proof. |
| The kill and promote criteria | Variants below median performance after 72 hours and $100 spend get killed. Variants above median for 7+ days get promoted to higher spend share. Winners run alongside the next concept generation until fatigue starts to show. |
| The refresh cadence | Winners get refreshed every 2 to 4 weeks even when still performing. Creative fatigue is real and compounds with frequency. |
| The naming convention | Every creative gets a structured name that makes performance pulls queryable by concept, format, and variant. Without naming discipline, the testing data is unreadable three weeks later. |
The testing discipline is the difference between operators whose creative compounds and operators whose creative resets every quarter.
Part 7. The production pipeline
The strategy does not execute itself. The production pipeline is the operational system that turns strategy decisions into creative assets at the volume the channel mix requires.
Production pipeline choices interact directly with the ad creative capability layer and with the operational realities of running treatment center landing pages at scale. Hybrid in-house plus agency models work for most operators because brand creative and operational creative have different production constraints and different optimal velocity.
Three pipeline models work in this category. Most operators settle on a hybrid of two of them.
| Model | Trade-offs | Best fit |
|---|---|---|
| In-house | Highest control over brand consistency. Slowest to ramp. Most expensive at the team level but cheapest per asset at scale. | Multi-location operators with budgets above $1M annual marketing spend. |
| Agency | Faster ramp than in-house. Lower fixed cost. The agency’s creative defaults tend to be category-typical, which makes differentiation harder unless the operator drives the strategy explicitly. | Tier 1 and early tier 2 operators with budgets under $500K annual marketing spend. |
| Hybrid | Agency runs paid media creative. Operator owns brand creative, founder portraiture, clinical leadership content, and alumni storytelling internally. Agency executes high-volume operational creative. Operator produces differentiating brand assets. | Most common pattern for tier 2 and tier 3 operators ($500K to $5M annual marketing budgets). |
The pipeline model is a budget decision. The pipeline output is a strategy decision. Operators who pick the model first and decide what to produce afterward end up with creative that the model can make, not creative that the strategy needs.
A simple rubric: list the 10 creative outputs the strategy requires for the next quarter. Estimate the cost to produce each one under the in-house, agency, and hybrid model. Pick the model that produces all 10 at the lowest total cost.
If no model produces all 10, the strategy is wrong or the budget is wrong.
Part 8. Common creative strategy mistakes
Eight patterns we audit across treatment center marketing programs.
The mistakes below pair with the diagnostic framework in our marketing agency review and the testing discipline in our conversion tracking work. Operators recognizing two or more of these patterns in their current engagement typically need to rebuild the strategy from the brand foundation outward, not patch individual campaigns.
| Mistake | Why it fails |
|---|---|
| 1. Brand foundation skipped | No positioning statement, no voice guide, no message architecture. The creative drifts because nothing anchors it. Six months in, the agency produces ads that contradict the website’s positioning. |
| 2. Patient voice instead of family-member voice | “Are you ready to get sober?” addressed to a person who would not be on the page if they were. The voice misses the actual audience and the conversion rate suffers. |
| 3. Compassionate-care positioning | “We provide compassionate, individualized addiction treatment.” Could be any treatment center. The visitor reads it and assumes interchangeability. |
| 4. Stock imagery shared with every competitor | Hands-in-a-circle on a beach, silhouette against a sunset, generic clinical setting. The visitor has seen the same imagery on every other rehab site this week. |
| 5. Inconsistent visual identity across channels | The website looks one way, the paid social looks another, the email looks like a third brand. Family members in research mode hit the inconsistency and read it as unreliability. |
| 6. Creative refresh treated as a quarterly project | Five ads at launch, then six months of silence. Meta’s algorithm starves. The CPL trends up. The operator concludes Meta is broken. |
| 7. Outcome claims without evidence | “85% sobriety rate” or “Most clients never use again.” The FTC will ask. The state regulator may ask. The competitor agency monitoring complaints will tip them off. |
| 8. Channel mix copy-pasted from a different category | SaaS retargeting funnels, ecommerce abandoned-cart sequences, B2B nurture drip emails. None of these work in BH because of the policy stack and audience behavior. |
The strategy that produces conversion in this category is built from the constraints up, not borrowed from adjacent verticals.
Part 9. Measurement framework
The right measurement framework for creative strategy tracks three layers: creative-level performance, channel-level performance, and program-level outcomes.
 Infographic titled ‘Three layers. One direction.’ Left half shows a three-tier measurement pyramid for creative strategy in behavioral health marketing. Base layer (widest): Creative-level performance with metrics hook rate, hold rate, completion rate on video, plus click-through rate, cost per click, and conversion rate by variant tells you which specific assets are doing the conversion work and is the input to creative iteration. Middle layer: Channel-level performance with metrics cost per lead, cost per private-policy verification of benefits, cost per admit by channel, and volume contribution by channel tells you whether the channel mix is right and is the input to budget allocation. Apex layer (narrowest): Program-level outcomes with metrics total admits per month, average payer mix, average length of stay, revenue per admit, and marketing cost per admit tells you whether the creative strategy is producing the business outcome the operator needs and is the input to strategic adjustment. Arrows on the pyramid sides labeled ‘Inputs flow up’ and ‘Decisions flow down.’ Right half shows a line chart of marketing cost per admit over 12 months: declining 2-4% month over month through month 6, then stabilizing through month 12. Dashed red line above the curve labeled ‘What it looks like when the strategy has stopped working: rising CPA.’ Bottom callout: ‘If your CPA is rising instead of declining, the fix is upstream. Rebuild the audience framework, voice, and message architecture from the strategy layer.’
Infographic titled ‘Three layers. One direction.’ Left half shows a three-tier measurement pyramid for creative strategy in behavioral health marketing. Base layer (widest): Creative-level performance with metrics hook rate, hold rate, completion rate on video, plus click-through rate, cost per click, and conversion rate by variant tells you which specific assets are doing the conversion work and is the input to creative iteration. Middle layer: Channel-level performance with metrics cost per lead, cost per private-policy verification of benefits, cost per admit by channel, and volume contribution by channel tells you whether the channel mix is right and is the input to budget allocation. Apex layer (narrowest): Program-level outcomes with metrics total admits per month, average payer mix, average length of stay, revenue per admit, and marketing cost per admit tells you whether the creative strategy is producing the business outcome the operator needs and is the input to strategic adjustment. Arrows on the pyramid sides labeled ‘Inputs flow up’ and ‘Decisions flow down.’ Right half shows a line chart of marketing cost per admit over 12 months: declining 2-4% month over month through month 6, then stabilizing through month 12. Dashed red line above the curve labeled ‘What it looks like when the strategy has stopped working: rising CPA.’ Bottom callout: ‘If your CPA is rising instead of declining, the fix is upstream. Rebuild the audience framework, voice, and message architecture from the strategy layer.’| Layer | Metrics | What it tells you |
|---|---|---|
| Creative-level performance | Hook rate, hold rate, completion rate on video. Click-through rate, cost per click, conversion rate on individual variants. | Which specific assets are working. Input to creative iteration. |
| Channel-level performance | Cost per lead, cost per private-policy VOB, and cost per admit by channel. Volume contribution by channel. | Whether the channel mix is right. Input to budget allocation decisions. |
| Program-level outcomes | Total admits per month, average payer mix, average length of stay, revenue per admit, marketing cost per admit. | Whether the creative strategy is producing the business outcome the operator needs. Input to strategic adjustment. |
Most operators report channel-level only. The creative-level metrics surface which assets are doing the conversion work, which is the input to creative iteration. The program-level metrics surface whether the channel mix and creative direction are producing actual admits, which is the input to strategic adjustment.
A working report has all three layers, refreshed monthly, trended over the last six months with year-over-year comparison where the data exists.
The benchmark we tell operators to expect: in a well-run creative strategy program, cost per admit declines 2% to 4% month over month for the first six months as the testing discipline finds winners and the channel mix optimizes.
After six months, cost per admit stabilizes and the program scales by adding budget rather than improving efficiency.
Operators whose cost per admit is rising are running a creative strategy that has stopped working. The fix is usually not new channels or more budget.
The fix is going back to the brand foundation and rebuilding the audience framework, voice, and message architecture from the strategy layer rather than the campaign layer.
Frequently asked questions about creative strategy for treatment center marketing
Should we run creative through an in-house team or an agency?
Most treatment centers under $30M in revenue do best with a specialist agency producing creative because the constraint stack (HIPAA, Meta, Google policy, FTC, LegitScript) makes in-house production expensive to staff for the volume an individual facility needs. Agencies producing creative across multiple BH clients see policy boundaries faster than any single facility can.
The exception is when in-house brand or marketing leadership has prior agency experience in the vertical. We have seen mid-size treatment centers run effective in-house creative teams when the creative lead came from a behavioral health agency and brought the constraint fluency in with them. Without that fluency, in-house creative tends to ship a higher percentage of disapproved or low-performing ads in the first 6 months.
The hybrid model is the option most operators miss. A specialist agency produces channel-level creative against compliance-cleared frameworks; an in-house designer or brand lead handles brand consistency, landing page production, and email creative against those frameworks. That split gives the operator control of the brand layer and offloads the constraint-heavy work.
How much should we invest in creative versus media spend?
Most well-run treatment center programs allocate 15 to 25 percent of paid media spend to creative production and testing, with the higher end of the range during launch or major repositioning. Below 10 percent, the program is running stale creative against changing platform behavior and watching CPL inflate quarter over quarter. Above 30 percent, the testing volume usually outruns the data the platform can produce against it.
The variable that matters more than the percentage is the production cadence. A program shipping 2 to 3 new creative concepts per week against a tested framework typically beats a program shipping 1 new concept per month, even at lower per-asset production cost. Meta and Google reward creative freshness; static creative loses CPM and CTR over 6 to 12 weeks regardless of how strong the initial concept was.
We size creative production budgets against the platform’s creative consumption rate, not against a generic percentage of media spend. A program running $40,000 monthly on Meta paid social needs more creative volume than a program running $40,000 monthly on Google paid search, because Meta’s algorithm burns through creative variants faster.
How do we test creative without burning budget on disapprovals?
Pre-submission review against the policy stack catches most of what would otherwise burn budget. Every new creative concept goes through a documented compliance checklist before it reaches the platform: HIPAA review for any patient-adjacent imagery, FTC review for outcome claims, Meta Health and Wellness review for substance use framing, Google Healthcare and Medicines review for headline patterns, FTC review for testimonial use.
The checklist catches roughly 80 percent of the disapprovals an unreviewed creative would trip. The remaining 20 percent comes from platform-level shifts the checklist has not caught yet, and those teach the agency or in-house team what to add to the next version of the checklist. The discipline compounds. Programs with 12 months of checklist iteration have disapproval rates around 5 percent versus the 30 to 50 percent disapproval rate typical for unprepared programs.
Once creative clears the checklist, structured A/B testing on the platform is the next layer. Two to three variants per concept, 7 to 14 days of data before drawing conclusions, statistical significance thresholds documented before the test launches. The goal is to find the winning concept, not to test every possible variant.
What is the biggest creative strategy mistake treatment centers make?
Treating the constraint stack as a creative limitation rather than a creative forcing function. The constraints (no patient testimonials on Meta, no outcome guarantees, no specific clinical claims) push lazy operators toward generic creative that looks identical to every other treatment center’s. The centers that win treat the constraints as a brief that forces sharper positioning rather than a limit that flattens it.
The second-biggest mistake is letting paid media run on the same creative for 6+ months. Platform algorithms reward fresh creative; stale creative loses CPM and CTR over time even when the initial concept was strong. A center running the same 3 ad creative variants in month 9 that it ran in month 3 is watching cost per admit climb without diagnosing why.
The third mistake is producing creative that markets to the patient when family members are the actual decision-maker in most BH purchases. Family-member voice clears Meta’s review queue more reliably than patient-first voice and converts higher because it matches the decision-making reality of how treatment center admissions actually happen.
How long does it take to see results from a creative strategy overhaul?
Most treatment centers see meaningful paid media performance lift within 30 to 60 days of shipping new creative against a coherent strategy. The first 30 days are diagnostic: which new concepts pass platform review, which audiences respond, which creative angles produce qualified leads versus form-fill volume. Days 30 to 60 see the algorithm calibrate to the new concepts and produce the first clean efficiency lift.
Bigger strategic shifts (brand voice repositioning, audience reframe from patient to family member, full channel-creative recalibration) take 60 to 120 days to show. The longer timeline is the algorithm relearning period plus the operational time to produce enough variants per concept to test cleanly. Programs that rush the overhaul tend to abandon a working strategy before the platform finishes calibrating.
The cleanest signal that the overhaul is working is the cost-per-admit comparison at day 90 against the trailing 90-day baseline. If cost-per-admit is at parity or better with the new creative producing the volume, the foundation is built for compounding gains in months 4 to 12 as the algorithm continues to calibrate.
What this means for treatment center operators
Creative strategy for rehab and addiction treatment marketing is a strategic discipline that produces creative outputs, not a creative discipline first. The constraint stack (HIPAA, self-harm classification, Healthcare and Medicines policy, FTC enforcement, LegitScript certification) is the starting line.
The audience framework, brand foundation, channel principles, testing discipline, production pipeline, and measurement framework are how the strategy executes inside those constraints.
Operators who treat creative as a series of campaigns produced by a series of agencies produce creative that resets every quarter. Operators who treat creative as a strategic discipline that compounds over years produce a marketing program that gets cheaper, more effective, and more defensible against competitors over time.
The center that runs this program correctly has a recognizable brand, a documented voice, a tested visual identity, a tuned channel mix, a continuous creative pipeline, and a measurement framework that surfaces both creative-level performance and program-level outcomes. The center that does not has campaigns. Campaigns end. Strategy compounds.
If you want to walk through where your current creative strategy sits against the framework above, book a discovery call. We will audit the brand foundation, the audience framework, the channel principles, and the production pipeline, and tell you honestly which parts are working and which parts need rebuilding.
The audit is free. The honest answer is the deliverable, not the pitch.
Most in-house teams hit a wall not because they lack knowledge, but because they lack bandwidth.
When you are ready to hand it off, Webserv has spent 9 years executing exactly this for treatment centers nationwide.