
A treatment center operator called us last quarter with the question every behavioral health owner asks eventually.
“We spent $180,000 on a website redesign, we publish four blog posts a month, we have 87 Google reviews at 4.7 stars, and we are still not ranking. What is wrong with our SEO?”
Two things were wrong. Neither was the website redesign or the publishing cadence.
The first was that the operator’s site had been quietly hit by a Core Update six months earlier and the team had not noticed because traffic was still flowing from paid ads.
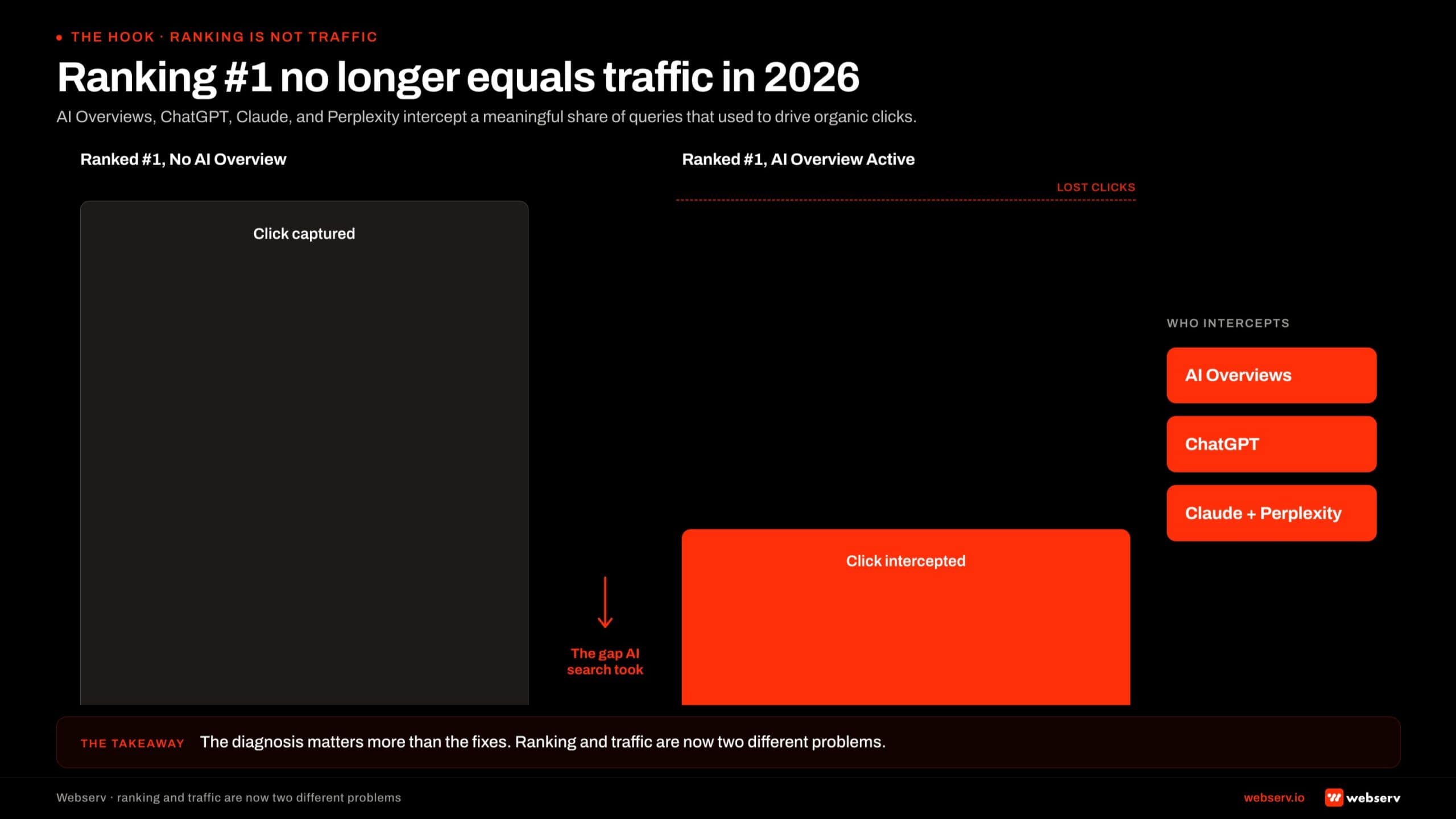
The second was that the operator was measuring “ranking” against keyword positions from a 2022 mental model, while ChatGPT and Google AI Overviews had been intercepting roughly 40 percent of the queries that used to drive organic clicks for behavioral health.
The diagnostic playbook for “why isn’t my rehab website ranking on Google” looks different in 2026 than it did three years ago. The questions are still familiar (technical SEO, E-E-A-T, topical authority, backlinks, local signals).
The order in which you investigate them matters more now, and there is a 2026-specific layer on top of all of them that most operators have not adjusted for yet.
This piece is the diagnostic playbook we walk treatment center operators through when they call. It is the long-form version of what we cover in our SEO capability for treatment centers.
Seven categories of failure mode, the diagnostic sequence to figure out which two or three apply to your site, and the 90-day fix order that produces the cleanest ranking and citation recovery.
Key Takeaways
- Ranking on Google has decoupled from getting traffic in 2026. AI Overviews, ChatGPT, Claude, and Perplexity intercept a meaningful share of the queries that used to drive organic clicks. “We are not ranking” might actually mean “we rank but AI search ate the click.” The diagnosis is different in each case.
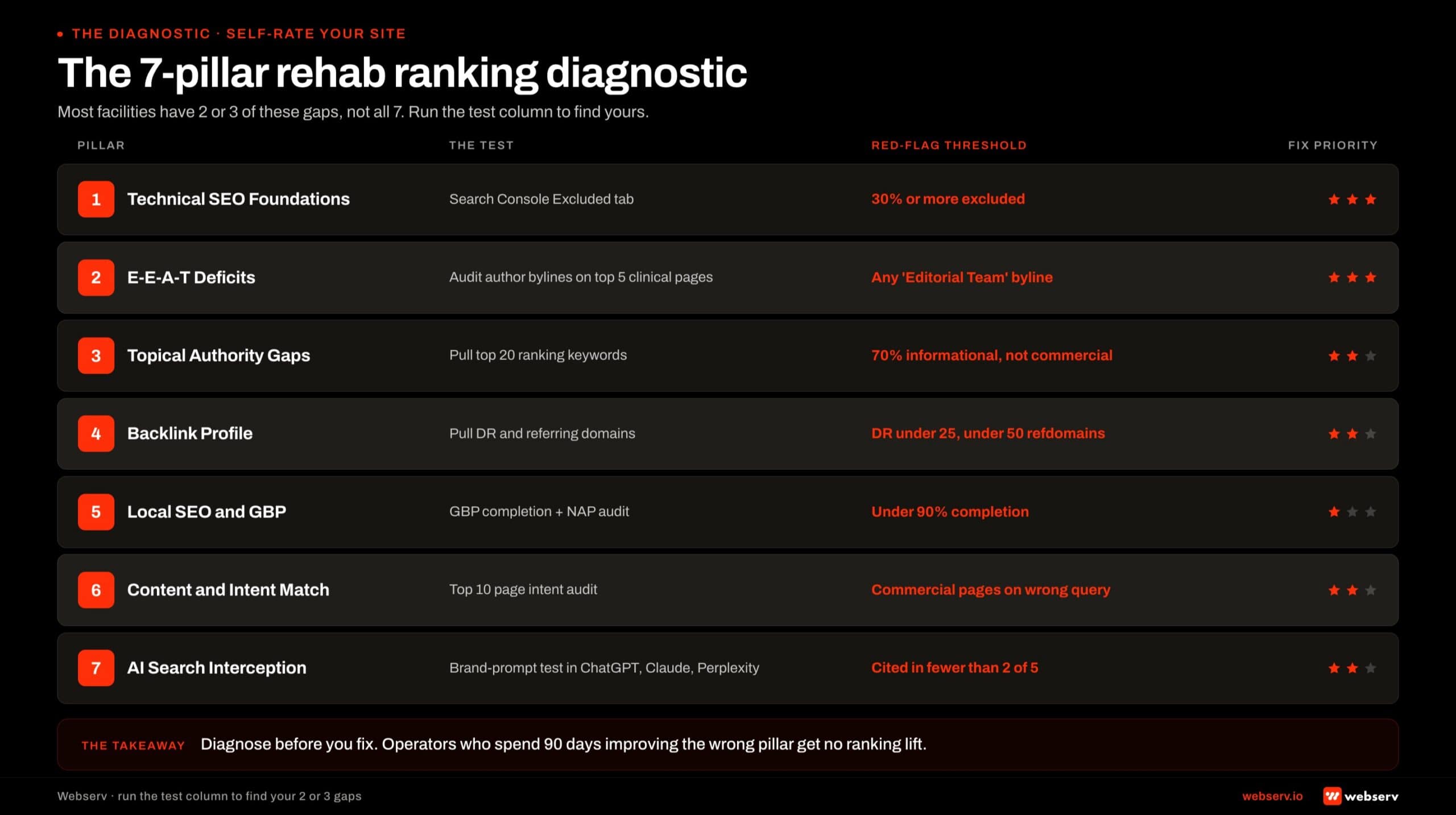
- Seven categories cover almost every reason a rehab site is not ranking: technical SEO, E-E-A-T deficits, topical authority gaps, backlink profile, local SEO, content and intent mismatch, and the 2026 AI search interception layer. Most facilities have 2 to 3 of these gaps, not all 7.
- Healthcare YMYL is evaluated against the strictest E-E-A-T threshold of any vertical Google tracks. Named clinical authorship, reviewer credit, and peer-reviewed citation discipline are not stylistic choices; they are the load-bearing infrastructure that determines whether a treatment center site is treated as authoritative.
- The diagnosis matters more than the fixes. Operators who spend 90 days improving the wrong thing get no ranking lift. Operators who spend 60 days fixing the right 2 or 3 things move from ranking nowhere to ranking on commercial-intent terms in the same cluster.
- The fix order is foundations first (technical and E-E-A-T), then topical authority, then off-site signals. Reversing the order is the most common mistake in rehab SEO and the reason most facilities pay for backlinks before they have the on-site infrastructure to make those links work.
Pillar 1: The First Question Isn’t “Why Aren’t We Ranking”: It’s “Are You Actually Not Ranking?”
The 2026 reality changes the first question. Before the diagnostic, the operator and the SEO team need to agree on what “not ranking” actually means.
Four scenarios produce the same complaint. Each requires a different response.
Scenario A: The site is not indexed. Crawl issues, robots.txt misconfiguration, accidental noindex tags, JavaScript-rendered content that Googlebot cannot parse. The pages do not appear in Google at all.
Diagnostic: type site:yourdomain.com into Google. If the count is substantively lower than the number of pages on the site, the gap is indexation, not ranking.
Scenario B: The site is indexed but not ranking on commercial-intent terms. Pages appear in Google but live on page 3 or worse for “alcohol rehab,” “drug treatment center,” “PHP near me,” and the high-intent queries that actually produce admits.
This is the classic SEO ranking problem and what most operators mean by “we are not ranking.”
Scenario C: The site ranks but is not getting clicks. Pages sit in position 1 to 5 for target terms, but organic sessions are flat or declining. AI Overviews are eating the click.
ChatGPT and Perplexity citation share for the queries is not landing on the facility. This is the 2026-specific failure mode that did not exist three years ago.
Scenario D: The site ranks for the wrong queries. Traffic looks healthy in Google Search Console, but the queries driving it are informational rather than commercial. The site ranks for “what is rehab” instead of “rehab near me.” Sessions are high; admit-attributed conversions are low.
The diagnostic sequence is different for each scenario. Indexation issues get fixed in days. Ranking gaps take 60 to 180 days.
AI search interception requires a separate strategy that overlaps with but is distinct from traditional SEO, which is why our AEO capability sits as a separate service line. Intent mismatch requires content re-targeting, not more content.
Most operators conflate these four scenarios into “we are not ranking” and ask the SEO team for a single fix. The SEO team that delivers a single fix without diagnosing which scenario the operator is actually in produces 90 days of effort with no measurable result.
Pillar 2: Technical SEO Foundations
The technical layer is where most diagnostic sequences should start, because technical gaps invalidate every fix downstream. A facility with perfect content, perfect authorship, and a great backlink profile still does not rank if Googlebot cannot crawl the site or render the pages.
The technical foundations Google itself documents in the Search Essentials are not optional in healthcare YMYL. Four categories of technical gaps account for most of the technical-side failures in treatment center sites.
Crawl and indexation. Robots.txt accidentally blocking important paths. Noindex tags left over from staging. XML sitemap stale or missing. Canonical tags pointing at the wrong URLs. Internal linking too shallow for Googlebot to find the deep pages on the site.
Diagnostic: pull the site into Google Search Console, run the Coverage report, and look at the “Excluded” tab. If 30 percent or more of the site is excluded, the technical layer is the load-bearing issue.
The deeper read on entity SEO for treatment centers in AI search covers how the schema and entity layer compounds on top of clean indexation.
Core Web Vitals and mobile performance. Google’s Core Web Vitals framework measures Largest Contentful Paint, Interaction to Next Paint, and Cumulative Layout Shift. Treatment center sites built on Elementor or other heavy page builders frequently fail Core Web Vitals on mobile, particularly LCP and CLS.
Mobile is where the load-bearing audience lives. Family members researching at 11 PM are on their phones. A page that takes 4.5 seconds to load on mobile loses ranking position and conversion against an equivalent page that loads in 1.8 seconds, regardless of content quality.
Schema and structured data. Organization schema, MedicalOrganization schema, LocalBusiness schema, FAQPage schema, BreadcrumbList, and (for facilities running clinical content) Article schema with named author markup. Google’s structured data guidelines document the shape; the implementation is where most facilities fall short.
Schema gaps are particularly costly in healthcare YMYL because schema is one of the load-bearing signals AI systems use to disambiguate entities and verify authority claims. A clean schema stack is the technical infrastructure that makes the rest of the E-E-A-T work readable to AI search.
JavaScript and rendering. Treatment center sites built on heavy JavaScript frameworks sometimes serve content that Googlebot cannot render. The page looks fine to humans; the bot sees an empty shell.
Diagnostic: use the URL Inspection tool in Search Console and look at the “Rendered HTML” output. If the rendered HTML does not contain the page content, you have a rendering problem.
Most facilities can fix the four technical categories in 30 to 60 days with a focused engineering pass. The technical gap is rarely the single reason a site is not ranking, but technical gaps invalidate the fixes downstream, which is why this layer goes first.
Pillar 3: YMYL E-E-A-T Deficits Are the Single Most Common Behavioral Health Failure Mode
If the technical layer is the floor, the E-E-A-T layer is the load-bearing structure of YMYL ranking.
Google’s healthcare-specific Quality Rater Guidelines make the Experience, Expertise, Authoritativeness, and Trustworthiness threshold materially higher for healthcare content than for almost any other category, and the September 2025 QRG update extended the framework to AI Overviews citation eligibility.
Five sub-gaps account for almost every E-E-A-T failure we see in treatment center sites.
Editorial team bylines. Articles bylined “Editorial Team” or “[Facility Name] Staff” do not carry E-E-A-T weight in YMYL evaluation. Google’s quality raters explicitly look for named, credentialed authors on healthcare content.
The absence of an attributable human author is a negative signal at scale, and we cover the broader frame in the case against generic healthcare content farms in addiction treatment.
Missing or hidden author bios. When clinical content does have a named author, the author bio page is often missing, thin, or hidden in the footer. The bio page is itself a YMYL signal that Google evaluates.
Bio pages without credentials, licensing, sameAs links to professional registries, or a structured authored-article list are functionally invisible. Our deeper read on author bios that build E-E-A-T for behavioral health blogs covers the bio anatomy that actually carries weight.
Missing clinical reviewer credit. Even named-author content underperforms without a second credentialed reviewer signing off on clinical accuracy. The “Clinically Reviewed by [Name, Credentials] on [Date]” line is a small visible signal that produces outsized ranking effect. Most treatment center blogs do not include it.
Citation discipline. Clinical claims that cite peer-reviewed sources (SAMHSA, NIDA, NIMH, JAMA Psychiatry, ASAM publications) carry materially more E-E-A-T weight than claims that cite other blog posts or undocumented industry statistics.
Citation format also matters: inline hyperlinks beat reference lists, and direct quotes from named researchers beat paraphrased citations.
Entity-level credibility signals. Accreditation badges (JCAHO, CARF, LegitScript), licensure references, and clinical leadership bios in or near the page hero. These small signals combine to produce the “trust gestalt” Google’s evaluation framework rewards in YMYL.
The E-E-A-T layer is the load-bearing fix for most BH sites we audit. A treatment center with strong technical SEO and no named clinical authorship still does not rank for commercial-intent healthcare queries.
A treatment center with average technical SEO and a strong E-E-A-T system ranks ahead of competitors with the inverse profile.
This is the gap operators consistently underestimate. The fix is not glamorous (it is bio pages, reviewer credit lines, and citation discipline), but it produces more ranking lift per dollar than almost any other intervention in YMYL.
Pillar 4: Topical Authority Gaps and Doorway Page Risk
Beyond individual page quality, Google evaluates whether the site has topical authority across the category. A facility with five great pages on addiction treatment ranks worse than a facility with twenty connected pages covering the condition, the modalities, the levels of care, and the patient and family questions.
The topical authority framework for treatment centers is the deep read. The short version is that topical authority compounds across pages in a cluster. The site that publishes 23 connected pages produces more ranking and AI citation share than the site that publishes 200 disconnected pages.
Three topical authority gaps account for most of the failures we see.
Thin cluster coverage. A facility publishes a service page for “Alcohol Use Disorder Treatment” and three blog posts that vaguely mention alcohol. The cluster is too thin to signal topical authority. Google treats the site as a competitor in the category but not as an authority.
The fix is sequenced pillar and cluster building. Condition pillar pages (alcohol use disorder, opioid use disorder, anxiety, depression) anchor the architecture. Modality cluster pages (CBT, DBT, EMDR, MAT) sit one level below.
Level-of-care pages (detox, residential, PHP, IOP) anchor the operational layer. The content gap analysis methodology is the diagnostic input that surfaces which cluster gaps are blocking ranking.
Doorway pages. Treatment center sites that built location-specific landing pages with near-identical content (the “alcohol rehab in [city]” pattern across 50 cities) trip Google’s doorway pages penalty.
The pages were intended to capture local intent. Google reads them as an attempt to manipulate ranking through thin, duplicated content.
The cost of doorway pages on a behavioral health site covers the measurable ranking drag. The fix is consolidation rather than de-publication: collapse the 50 doorway pages into 5 to 10 substantive geographic pages tied to real facility presence and real content depth.
Internal linking density. Even good content underperforms when the internal linking architecture does not pass authority across the cluster. The condition pillar page should link to every modality and level-of-care page in the cluster.
The modality pages should link to relevant condition pillars and case-study or outcome content. Sites with weak internal linking density behave as if they have no cluster at all from Google’s perspective.
A 90-day topical authority audit and rebuild is the second most common fix we deploy for treatment center sites stuck in mid-page ranking ranges. The compounding effect across a 12-month horizon is large.
The most expensive mistake in rehab SEO is paying for backlinks before the on-site E-E-A-T infrastructure is in place to make those links matter.
Operators who fix the order produce ranking and citation lift in 90 days. Operators who skip the foundation and chase off-site signals spend a year buying authority they cannot hold.
Preston Powell, CEO of Webserv
Pillar 5: Backlink Profile Issues
Off-site signals come third in the diagnostic sequence, not first. Backlinks are a load-bearing ranking signal in healthcare YMYL, but they are downstream of on-site quality.
A facility with weak on-site E-E-A-T and great backlinks ranks worse than a facility with strong on-site E-E-A-T and average backlinks.
Three backlink profile issues account for most of the off-site failure modes we audit.
Low domain authority baseline. Facilities with Domain Rating below 25 (per Ahrefs) and fewer than 50 referring domains struggle to rank in any competitive healthcare category.
The fix is a sustained 12 to 24 month link-building program, not a single PR push. Our link building methodology for rehab websites covers the approach we use.
Toxic or unnatural anchor profiles. Sites that bought links in 2018 to 2020 often have anchor profiles dominated by “alcohol rehab,” “drug treatment,” and other exact-match commercial anchors. The anchor profile pattern itself triggers algorithmic suspicion.
Diagnostic: pull the anchor profile from Ahrefs or SEMRush and look at the top 20 anchors. If exact-match commercial anchors dominate, the profile is unnatural by current standards.
The fix is dilution rather than disavowal: build branded and natural anchors fast enough that the exact-match anchors decline as a percentage of the profile. Full disavowal is rarely the right move for treatment center sites with mixed-quality back catalog links.
Mid-DR backlinks for AI citation. A 2026-specific frame. Mid-DR backlinks now outperform DR70+ sites for LLM citations in many AI search contexts.
LLM citation models weight topical fit and source diversity differently than traditional ranking algorithms weight raw authority. A facility chasing only high-DR links is leaving AI citation share on the table.
The backlink layer is the slowest fix in the diagnostic sequence. Twelve to twenty-four months from a standing start to a real Domain Rating lift.
Longer if the underlying E-E-A-T infrastructure is not in place to make the new links work, which is the argument for fixing the on-site work first.
Pillar 6: Local SEO and GBP Signals
For most treatment centers, local search is a meaningful share of admit-attributed conversion. Google Business Profile, NAP (Name, Address, Phone) consistency across local citation sites, and review velocity all feed into Map Pack visibility and local-intent SERP performance.
Google’s documentation on Business Profile optimization is the technical reference. The diagnostic sequence for local SEO failure usually surfaces three issues.
GBP incomplete or stale. Service categories not populated. Hours not updated. Photos not refreshed. Q&A section left untouched. Google Posts cadence at zero. A GBP at 30 percent completion ranks below an otherwise-equivalent facility at 90 percent completion.
NAP inconsistency across citations. The facility’s address on the website, the GBP, Healthgrades, Psychology Today, Yelp, and twenty other directories does not match. The variation triggers entity disambiguation issues. Google is less confident which listing represents the real facility, which suppresses local ranking.
Review velocity and response rate. Facilities at 4.5+ stars with 100+ reviews and a response rate above 80 percent on negative reviews materially outrank facilities at the same star average with thin review volume or no review responses.
Review velocity (the rate of new reviews over time) matters as much as the static count.
Local SEO is one of the faster diagnostic fixes. Most facilities can close the GBP and NAP gaps in 30 to 60 days. Review velocity is a longer-term operational fix tied to the admissions and alumni workflows, not the marketing team alone.
Pillar 7: Content Quality, Intent Match, and the 2026 AI Search Interception Layer
The last category is the most modern. Two related failure modes that operators frequently confuse with each other.
Content quality and intent mismatch. A facility publishes 184 blog posts averaging 850 words, bylined “Editorial Team,” targeting informational queries the operator’s actual audience does not search for.
The site ranks for “what is alcohol use disorder” (informational, low admit-attributed conversion) and not for “best alcohol rehab in Arizona” (commercial intent, real conversion).
The fix is content re-targeting and quality consolidation. Cut the thin posts. Build deeper pillar pages that target both clinical and patient-vocabulary queries.
The clinicians-as-AEO-moat framing is the closest read on what that looks like in behavioral health. Address the family member as a reader, not only the patient.
Most behavioral health operators we audit have at least 30 percent of their content library producing zero admit-attributed conversion and could improve cluster authority by un-publishing it.
The 2026 AI search interception layer. Even when content is good and rankings are healthy, Google AI Overviews and the ChatGPT-Perplexity-Claude citation ecosystem intercept a meaningful share of clicks.
The facility ranks in position 2 for the target query but gets 40 percent less traffic than the same position produced two years ago.
This is the 2026-specific failure mode that did not exist in traditional SEO thinking. The fix is AEO and AI search infrastructure work, not more traditional SEO.
Schema deepening, AI Information pages, llms.txt, MCP servers, and OKF bundles like the Open Knowledge Format bundle Webserv published in June 2026 all sit in this layer.
Operators investigating “why we are not ranking” sometimes find that they actually are ranking, but the AI search layer is intercepting the traffic. The diagnosis matters because the fix for ranking gaps is different from the fix for AI citation gaps.
The treatment center sites that win in 2026 are the ones where the operator stopped asking “why are we not ranking” and started asking “which two or three things are actually broken.” The diagnosis is the work. The fixes are downstream.
Preston Powell, CEO of Webserv
The Diagnostic Sequence: How to Figure Out Which 2 or 3 Categories Apply to Your Site
MOST COMMON MISUNDERSTANDING
Operators default to “we need more content” or “we need more links” before running the diagnostic. Both are usually wrong. The diagnostic sequence exists because 90 percent of ranking problems trace to two or three specific pillars, not all seven. Skipping the diagnostic and funding a broad content or link program is how treatment centers spend $60K on SEO retainers without moving a single commercial keyword. Run the pillar-by-pillar field test first. Fund the fix only for the two or three that flag red.
Eight steps, in order, run end-to-end in a single afternoon. The output is a ranked list of which 2 to 3 of the 7 pillars are actually broken on the site, which is the input to the 90-day fix order below.
Step 1: Indexation count. Type site:yourdomain.com into Google. Compare the result count to the total pages on the site. A gap above 20 percent points to Pillar 2 (technical) as a starting place.
Step 2: Search Console Coverage report. Pull the Coverage report. Read the “Excluded” tab. If 30 percent or more of the site is in Excluded, the technical layer is the load-bearing constraint and goes to the top of the fix list.
Step 3: Core Web Vitals on mobile. Run PageSpeed Insights on the homepage, top 3 service pages, and a representative blog post. If LCP is above 2.5 seconds or CLS is above 0.1 on any of them, technical performance is a contributor.
Step 4: Author bio audit. Open the most-trafficked 5 clinical content pages on the site. Note the byline on each. If any read “Editorial Team,” “Staff,” or a marketing-team name, Pillar 3 (E-E-A-T) is broken and goes high on the fix list.
Step 5: Topical authority pulse. Open Ahrefs or SEMRush. Pull the top 20 keywords the site ranks for.
If 70 percent or more are informational (“what is,” “symptoms of”) rather than commercial (“rehab near me,” “best treatment center for”), Pillar 4 (topical authority) or Pillar 7 (intent mismatch) is the gap.
Step 6: Backlink baseline. Pull the Domain Rating and referring domain count from Ahrefs. DR below 25 with fewer than 50 referring domains points to Pillar 5 (backlinks) as a long-cycle fix that needs to start now even if other pillars come first.
Step 7: Local SEO sweep. Check GBP completion (aim for 90 percent), NAP consistency across the top 10 directory listings, and review velocity over the last 12 months. Gaps here flag Pillar 6 as a fast-fix opportunity.
Step 8: AI interception check. Pick 10 commercial-intent queries the site should rank for. Run each through ChatGPT, Perplexity, and Google AI Overviews.
If the facility appears in fewer than 3 of the 30 AI responses, Pillar 7 (AI search interception) is a real and growing leak that traditional ranking work will not fix.
Most facilities finish the 8-step sequence with 2 to 3 pillars flagged as broken and 4 to 5 pillars healthy. The fix order below sequences the 2 to 3 broken ones in the right order.
The 90-Day Fix Order
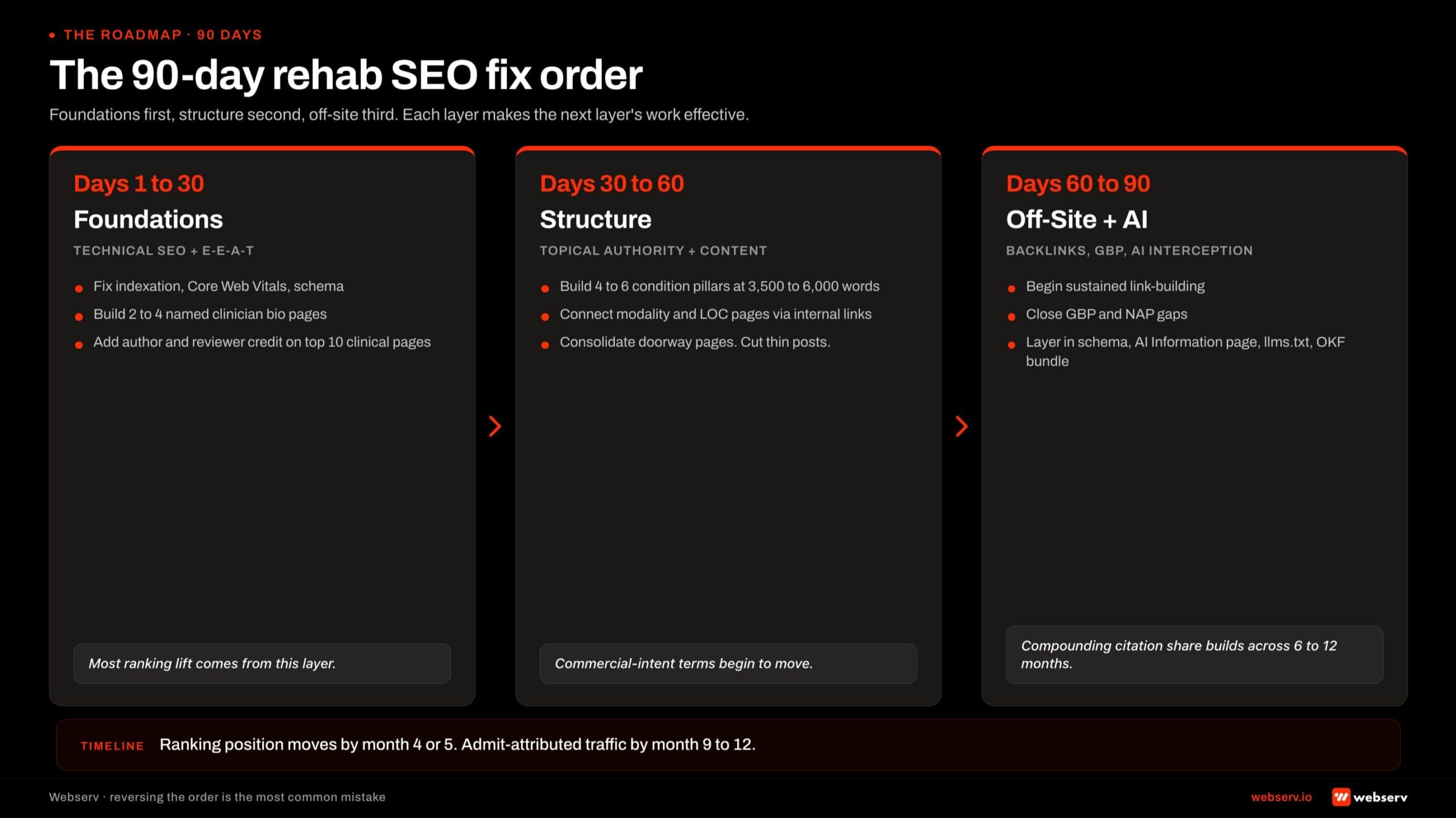
Foundations first, structure second, off-site third. The sequencing matters because each layer makes the next layer’s work effective.
Days 1-30: Foundations. Technical SEO and E-E-A-T. Fix the technical issues (indexation, Core Web Vitals, schema) and stand up the named-author and reviewer-credit system on the top 10 to 20 clinical pages. Build out 2 to 4 structured clinician bio pages with credentials, sameAs links, and headshots.
Most ranking lift in the first 90 days comes from this layer. Skipping it to chase content or backlinks is the most common mistake in rehab SEO.
Days 30-60: Structure. Topical authority and content. Build out the missing condition pillar pages (3,500 to 6,000 words each, named clinician author, full citation discipline). Connect the existing modality and level-of-care pages back to the pillars with strong internal linking.
Consolidate any doorway pages flagged in the audit. Cut the thin informational posts that are not earning admit-attributed conversion. Re-target the remaining content for both clinical and patient-vocabulary queries.
Days 60-90: Off-site and AI interception. Backlinks, local SEO, and the AI search interception layer. Begin the sustained link-building program (digital PR, data-driven campaigns, named-clinician thought leadership). Close GBP and NAP gaps.
Layer in the AEO infrastructure: schema deepening, AI Information page, llms.txt, and an OKF bundle. These produce no immediate ranking lift but begin the citation share compounding that pays back over 6 to 12 months.
The 90-day window does not finish the work. It produces the first measurable ranking signal, validates the diagnosis, and sets up the 12-to-18-month compounding that turns SEO into a primary admit channel.
Operators who run the sequence cleanly see ranking position moving by month 4 or 5 and admit-attributed traffic by month 9 to 12.
Frequently Asked Questions
How long does it take to fix rehab SEO and start ranking again?
Six to nine months for ranking to move materially. Twelve to 18 months for organic traffic to compound. Eighteen to 24 months for admit-attributed conversions from organic search to show up as a primary admit channel. The timeline runs longer than most operators expect because behavioral health is a stricter YMYL category than most.
The fix order matters more than the total time. Operators who fix technical and E-E-A-T foundations in the first 30 to 60 days see ranking signal moving by month 4 or 5. Operators who skip foundations and try to backfill them later add 6 to 9 months to the recovery curve.
Our deeper read on how long SEO takes to work for a rehab website covers the cycle in more detail. Operators planning on a 6-month ROI horizon are setting up for disappointment; operators planning on an 18-to-24-month compounding horizon produce SEO that pays back for years.
Do we need a new website to fix our rankings?
Rarely. Most ranking problems we audit are content, authorship, and architecture issues that can be fixed on the existing site at a fraction of the cost of a rebuild. A $180,000 redesign that addresses no E-E-A-T gaps and no topical authority gaps produces no ranking lift.
The exception is when the existing site has fundamental technical problems (a heavy JavaScript framework that Googlebot cannot render, Core Web Vitals failures that an existing platform cannot fix, a CMS that does not support proper schema or named-author bio architecture). In those cases the rebuild is a prerequisite for the SEO fixes, not the fix itself.
The right diagnostic question is: can the existing site support the authority content infrastructure (named author bio pages, reviewer credit, schema, FAQ blocks) the SEO fixes require? If yes, fix in place. If no, rebuild scoped to enable the SEO work, not to chase a redesign refresh.
Is publishing more content the fix?
Almost never on its own. The 184-vs-23 case framing holds: a facility publishing 184 posts under “Editorial Team” bylines typically ranks worse than a facility publishing 23 posts under named clinicians with peer-reviewed citations and connected cluster architecture. Volume without the E-E-A-T system underneath produces no ranking lift.
The exception is content gap closure inside a strong existing system. If a facility already has named authorship, reviewer credit, schema, and connected cluster architecture but is missing key condition or modality pillar pages, additional content closes the gap. If the foundation is not in place, additional content adds drag rather than lift.
Run a content gap analysis before deciding whether to scale up publishing. Most facilities discover the answer is “less, better, and architecturally connected” rather than “more.”
Should we hire a new agency if our current one isn’t getting us ranking?
Run the diagnostic first. Agencies sometimes underperform because the strategy is wrong; agencies sometimes underperform because the operator’s constraints (no clinician time for authorship, no engineering bandwidth for technical fixes, no budget for the link-building program the strategy requires) make the strategy unworkable. The cause matters for the decision.
Before switching agencies, audit which of the 7 pillars in this article the current agency has actually addressed. If the agency has shipped strong technical work, named author bio architecture, condition cluster pages, and topical authority compounding but ranking is still flat, the issue may be a backlink or AI search interception gap that takes longer to surface.
If the agency has shipped none of those, the issue is execution and a new agency may help.
The mistake to avoid is switching agencies every 6 to 12 months. SEO and AEO work compounds over 18 to 24 months; resetting the program every year guarantees no compounding ever happens. Switch when you have to; do not switch reflexively.
How do we know if Google has manually penalized our site?
Check Google Search Console under Security & Manual Actions. Manual actions show up in this report explicitly. If the report shows “No issues detected,” the site has not been manually penalized; the ranking problem is algorithmic, structural, or competitive.
The more common scenario is an algorithmic adjustment from a Core Update rather than a manual penalty. The September 2025 Quality Rater Guidelines update and the December 2025 Core Update both produced sizable ranking shifts on health-related websites. Facilities that lost ranking position in those windows usually lost it to E-E-A-T evaluation changes rather than to a manual penalty.
The diagnostic for algorithmic drops is to compare the affected URLs against the QRG criteria: named authorship, reviewer credit, citation quality, schema implementation, and overall trust signals. Pages that miss multiple E-E-A-T elements are the ones that lost position. The fix is the E-E-A-T system, not a penalty appeal.
Will AI search replace traditional SEO for treatment centers?
Not in the next 24 to 36 months. The two surfaces are co-existing rather than replacing each other. Traditional Google rankings still drive a substantial share of organic admit-attributed conversion for behavioral health, even as AI Overviews and ChatGPT citation share grows.
The strategic frame is that AI search is an additional surface to optimize for, not a replacement for the traditional SEO work. The two surfaces share substantial infrastructure: named clinical authorship, schema, content quality, and topical authority feed both organic ranking and AI citation eligibility.
For most operators, the right read is to keep the SEO program running at full cadence and add AEO work (schema deepening, AI Information page, llms.txt, MCP server, OKF bundle) as an additive layer. Our framing on how AI Overviews and ChatGPT citations work for rehab covers the additive layer in depth.
Diagnose Your Site Against the 8-Step Sequence Before Buying More SEO Work
The most expensive SEO decisions in behavioral health are made by operators who skip the diagnosis. Ninety days of content production, an agency switch, or a six-figure backlink campaign that addresses the wrong 2 to 3 pillars produces no ranking lift and a year of lost time.
The 8-step diagnostic sequence in this article runs in an afternoon. The output is a ranked list of which 2 or 3 of the 7 pillars are actually broken on your site, which is the input to the 90-day fix order. The diagnosis is the work; the fixes are downstream.
We help treatment center operators run the diagnostic, sequence the fix order against facility-specific constraints, and execute the 12-to-18-month compounding work that turns SEO into a primary admit channel.
The work spans technical SEO, E-E-A-T architecture, topical authority cluster building, link-building programs, local SEO, and the AEO and AI citation infrastructure that pairs with the traditional ranking work.
Book an intro meeting to walk through your current ranking profile, where the 2 or 3 broken pillars likely sit, and what the 90-day fix order would produce for your facility.
For the broader picture of how SEO fits inside a full treatment center marketing program, see our ultimate guide to behavioral health marketing.
Trevor Gage is the Director of Marketing at Webserv. Webserv works with behavioral health and addiction treatment centers on SEO, paid media, and full-funnel admissions strategy.





