A treatment center we work with had been running pure direct response creative on Meta for 18 months. Hard headlines. Insurance-callout copy. Urgent CTAs. Phone numbers on every frame.
The early returns were strong, cost per inquiry sat in the low double digits, and the operator wrote the playbook around it.
Eighteen months later, cost per inquiry had doubled. Lead quality was dropping. The admissions team was complaining about the volume of low-intent callers. The creative team was running out of new angles for the same direct-response template.
The operator’s question to us was the wrong one: “Do we need new direct response creative?” The actual answer was that the program had hit the ceiling of what pure direct response could deliver.
Inside our paid media program for treatment centers, this is one of the most common diagnostic moments we walk operators through.
The audience was fatigued. The brand had no resonance outside the immediate-need moment. Every inquiry had to be acquired from cold, because nobody knew the facility existed two weeks before they called.
The fix was not new DR creative. The fix was rebalancing the mix toward brand-awareness work that would warm the audience, build category authority, and give the existing direct response creative more lift per dollar.
This piece is the operator-facing read on the brand versus direct response question we get from treatment center operators almost every week. What each type of creative actually does. When you need more brand.
When you need more DR. The hybrid model that works for most behavioral health facilities. And the channel-by-channel and stage-by-stage decisions that determine the right mix for your facility right now.
The broader frame lives inside our paid media program for treatment centers, and the creative capability is where the production side of this work sits. This article is the strategic decision frame that sits one level above both.
Key Takeaways
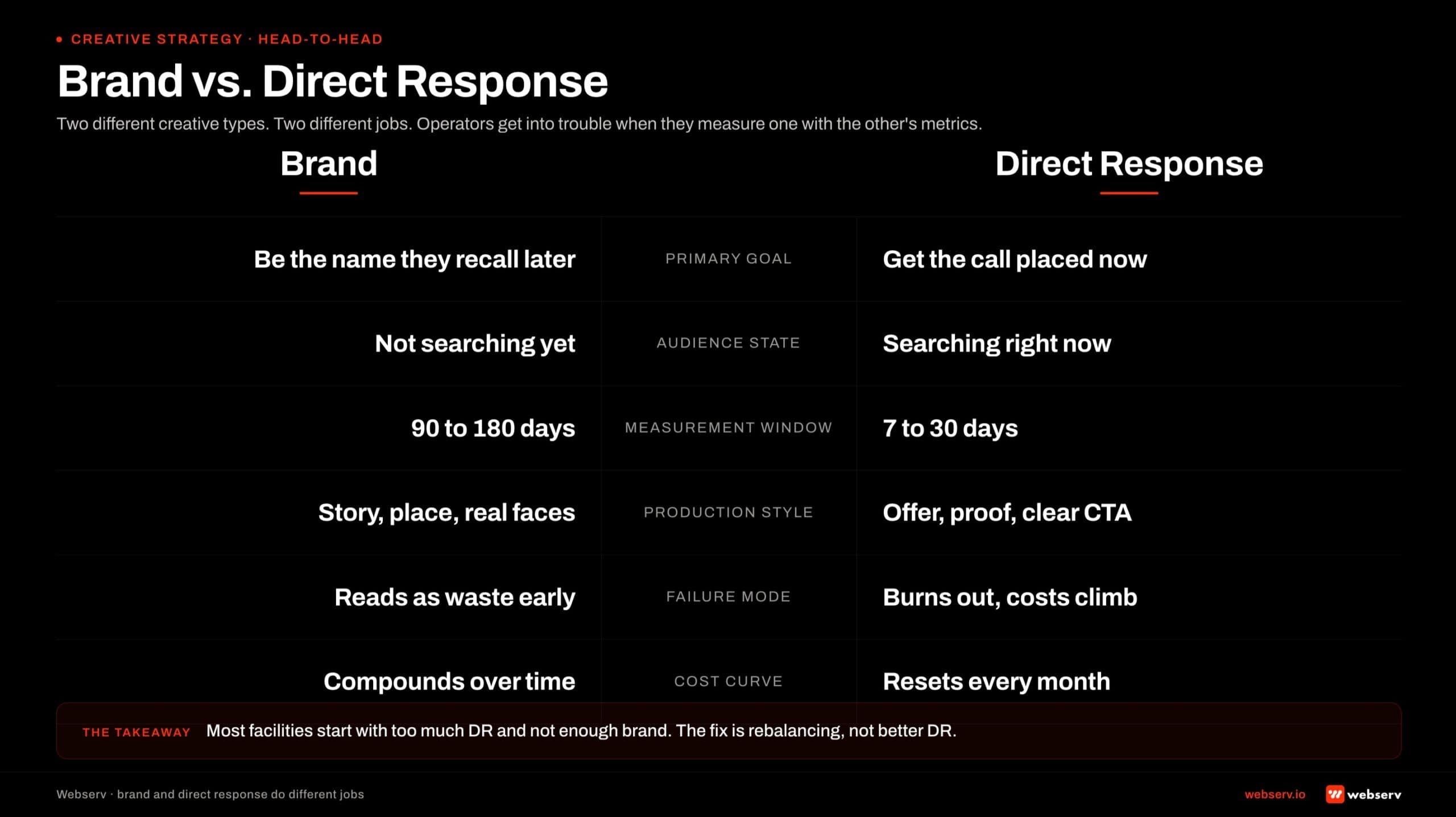
- Brand awareness creative and direct response creative are not interchangeable, and the choice between them is not a stylistic preference. They produce different conversion patterns, on different timelines, with different measurement requirements, and they fail in different ways when over-used in isolation.
- Most treatment center operators start with too much DR and not enough brand. Pure DR creative produces strong early returns and hits a ceiling at 12 to 18 months as audience fatigue and category saturation drive up cost per inquiry. The fix is rebalancing, not better DR.
- The behavioral health audience has a 30 to 120 day evaluation window between first awareness and inquiry call. Pure DR creative misses everyone outside the immediate-need moment. Brand creative compounds inside that window and lowers the cost of every DR inquiry the campaign produces.
- The right mix depends on channel, facility stage, and audience segment. Search-intent traffic on Google Ads wants DR. Meta and YouTube benefit from brand. Mature facilities benefit from heavier brand allocation; new facilities benefit from heavier DR. Family-member targeting wants different creative than patient targeting.
- Compliance constraints push BH creative toward brand-adjacent DR. LegitScript and Google healthcare policy limit how aggressive pure DR can be on outcome promises. The hybrid model (brand-informed DR) is often the highest-performing and lowest-compliance-risk format in the BH category.
The Conventional Wisdom (and Why It’s Partially Wrong)
The standard advice for treatment center marketing has been direct response everything.
The thinking is that the conversion event is an inquiry call, the audience is in active crisis or supporting someone in active crisis, and the time-pressure of the decision means the audience does not want or need brand-building advertising.
The conventional wisdom is half right. The conversion event is in fact the inquiry call. The audience is in crisis or family-member crisis. The time pressure is real. Pure DR creative does produce strong early performance against these conditions.
The half that the conventional wisdom misses is the audience timeline. The behavioral health prospect does not move from “I have a problem” to “I am calling a facility” in a single session.
The journey runs 30 to 120 days for residential treatment in most cases, longer for outpatient and ongoing care.
During that window, the prospect (and the family member) is searching, researching, evaluating, talking to friends, weighing options, finding insurance information, and slowly converging on the facility they will eventually call.
Pure DR creative serves the audience at the inquiry moment and ignores everything that happens upstream of the inquiry.
Brand awareness creative serves the audience during the 30 to 120 day evaluation, builds recall, and ensures that when the inquiry moment arrives, the facility is on the consideration list rather than absent from it.
A facility running pure DR creative is essentially trying to win the inquiry-moment auction every time, against competitors who are also running pure DR creative against the same auction.
The mathematics of the auction punish the facility with the worst-known brand against the facility with the best-known brand at the same bid level.
Brand creative is what changes the brand-known variable that the auction implicitly weights.
What Each Creative Type Actually Does
Before the mix conversation makes sense, the operator and the agency need to agree on what each type of creative actually accomplishes.
Direct response creative is built to drive a specific, measurable action inside a defined window. In behavioral health, that action is an inquiry call, a VOB form submission, or a click through to a high-intent landing page.
The creative typically includes a hard CTA, an urgency element, social proof or credibility signal, and a price or insurance-coverage hook. The audience for DR creative is in or near the decision window.
The measurement frame for DR creative is clean. Cost per lead, cost per inquiry, cost per admit, attributed conversion rate by ad set, ROAS at the campaign level. Every metric the operator cares about is observable inside a 30 to 60 day window after the creative goes live.
Brand awareness creative is built to produce recall, category association, and trust signal in audiences that are not yet in the decision window. The creative typically emphasizes the facility’s clinical philosophy, named clinical leadership, alumni outcomes (anonymized), facility environment, and the institution-level trust signals (accreditation, licensure, founding story).
The audience for brand creative is upstream of the decision window.
The measurement frame for brand creative is harder and longer. Aided and unaided brand recall, brand search volume in Google Trends, direct traffic to the facility’s domain, branded query click-through rate, and the lift in DR creative performance over time.
The window is 90 to 180 days minimum before the brand work shows up in DR metrics.
The two creative types are not in competition with each other. They serve different funnel stages. Pure DR without brand serves the bottom 10 to 20 percent of the audience that is in immediate decision mode.
Pure brand without DR builds recall but produces no measurable admit-attributed conversion. The right read is that they compound when run in the right ratio against the right audiences.
Pure DR creative serves the bottom 10 to 20 percent of the audience that is in immediate decision mode. The other 80 percent are inside the 30 to 120 day evaluation window. Brand creative is what makes the facility a real option when those evaluators convert.
The math compounds in the direction of whichever facility shows up across the full window, not the auction moment alone.
Preston Powell, CEO of Webserv
The BH-Specific Consideration: The Long Evaluation Window
The behavioral health audience moves through a longer consideration window than almost any other consumer category. The reasons are clinical, financial, and emotional in roughly that order.
The clinical reason: treatment is a major life decision. The patient or family member is choosing a clinical program that will affect 30 to 90 days of life trajectory, recovery probability, and family dynamics.
Nobody picks a residential facility the same way they pick a restaurant. The decision deserves the time.
The financial reason: residential treatment is expensive. Insurance verification takes days. Out-of-pocket cost analysis takes longer. The prospect needs time to figure out the financial dimension of the decision before they call.
The emotional reason: admitting that treatment is necessary is itself a hard step. The family member needs time to come to terms with the situation. The patient often needs more time. The decision window has a built-in emotional latency that no creative can shortcut.
This means the behavioral health marketing complete guide consistently shows that audience touches across the 30 to 120 day window correlate with inquiry rate at the end of the window.
Facilities that touch the audience three to seven times during that window inquire at materially higher rates than facilities that only show up at the inquiry-moment auction.
Brand awareness creative is what populates those upstream touches. Pure DR creative shows up only at the bottom of the funnel. The math compounds toward whichever facility is doing both.
When Brand Awareness Creative Earns Its Keep
Five conditions where brand creative is the highest-lever investment.
Mature facility, plateaued lead volume. A facility that has been running paid media for 12 to 24 months and is no longer seeing volume growth at the same cost per inquiry is hitting the saturation ceiling on its DR audience.
Adding more DR budget produces diminishing returns. Adding brand budget refreshes the upstream audience and re-opens the DR funnel.
Saturated geographic market. Facilities in markets with 8 to 12 well-funded competitors all running similar DR creative pay an auction tax on every click. Brand creative differentiates the facility outside the auction moment so that when the auction does come, the facility’s bid is weighted by audience preference.
Premium positioning. Facilities competing on clinical quality, specialty programming, or premium experience benefit from brand creative because the differentiation does not fit inside a 6-second DR ad. The clinical philosophy, named clinical leadership, and outcome reporting take longer-form creative to communicate.
Family-member targeting. Family members are the load-bearing decision-makers in residential admissions, and they evaluate facilities over a longer window than active-crisis patients. Family-focused brand creative (parent stories, caregiver resources, family program content) produces compounding consideration lift that pure DR creative does not.
Channel-specific lift. Meta and YouTube reward brand creative with lower CPMs and better engagement signal than Google Search does. For facilities running heavy Meta and YouTube spend, brand creative produces better cost-per-thousand-impression math than DR creative even before the audience lift compounds.
The 14 paid social strategies for treatment centers under $20K doc covers the under-budget version of this dynamic.
When Direct Response Creative Wins
Five conditions where DR creative is the right primary investment.
New facility, building from zero. A new facility with no brand history needs lead volume now. Brand creative does not produce measurable inquiry lift inside the first 90 days. DR creative produces inquiry volume the operator can measure week by week.
The right read for new facilities is DR-heavy in months 1 to 6, with brand budget layered in starting month 6 to 9.
Search-intent traffic. Google Search traffic arriving on commercial-intent queries (“alcohol rehab near me,” “rehab covered by Aetna”) is already inside the decision window. The audience does not need brand introduction; they need clear answers and a clear call-to-action.
DR creative on search converts better than brand-style creative on search by 2 to 4 times in most behavioral health paid programs.
Budget under $20,000 per month. At smaller budgets, brand creative produces fewer touches per audience member than the minimum required for recall lift. The math on brand spend below a certain threshold does not work.
Operators at this budget level should run DR-heavy until volume justifies expanding into brand work.
Active-crisis audience segments. The patient in active crisis or the family member at 11 PM searching for emergency treatment is not in the consideration window. They are in the inquiry moment. DR creative serves this audience cleanly. Brand creative is wasted spend against them.
Operator with weak admissions follow-up. Brand work compounds across months. If the facility’s admissions team cannot keep up with the lead volume DR creative is already producing, adding brand budget is throwing more pre-warm leads at a broken bottom-of-funnel.
Fix the admissions side first, then layer in brand.
The operators who treat the creative mix as a quarterly decision outperform the operators who pick a side and run it for 18 months. Brand vs DR is not a brand identity question.
It is a quarterly portfolio allocation that should shift with channel, facility stage, audience segment, and the cost-per-inquiry trend the program is actually producing.
Preston Powell, CEO of Webserv
The Hybrid Model: Brand-Informed Direct Response
The cleanest model we run for most treatment center operators is neither pure DR nor pure brand.
It is brand-informed direct response: DR creative that uses brand-quality storytelling, named clinical leadership, real facility footage, and authentic family-member voice while still containing a hard CTA and a measurable conversion path.
The brand-informed DR model has four properties.
Brand-quality production values. Real people, real settings, real stories. Not stock footage, not paid actors, not generic “diverse smiling people” b-roll. Production quality should match what a premium brand would put out, even though the creative is functionally DR.
Named clinical leadership and credibility signals. Featuring the clinical director, the chief medical officer, a named clinician explaining the program. The signals that brand creative usually carries (credibility, authority, trust) layered into a piece that still has DR structure.
A clear CTA and conversion path. Phone number visible, landing page tied to a specific campaign, conversion attribution wired through to admit-attributed measurement. The creative is producing measurable inquiry volume in the 30 to 60 day window of standard DR creative.
Compliance discipline that respects LegitScript and Google healthcare policy. No outcome promises, no statistical claims without substantiation, no testimonial language that exceeds 42 CFR Part 2 limits.
Brand-informed DR is naturally less aggressive on compliance edge cases because the brand-quality storytelling does the persuasion work that hard-DR creative tries to do with outcome promises.
The hybrid model is what most of the best-performing behavioral health paid programs we audit are running, even when the operator describes it as “DR.” The brand-quality production, named clinical leadership, and trust signal are doing as much work as the CTA, and the math reflects it.
Cost per inquiry is competitive with hard DR. Cost per admit is materially better. Long-term audience fatigue is lower because the creative does not feel transactional.
Channel-by-Channel: Where Each Type Wins
The right mix is channel-specific, not facility-wide. The same facility should be running different creative mixes on different platforms.
Google Search. Heavy DR. Audience is at the bottom of the funnel by definition. Brand creative on search wastes the high-intent moment.
The exception is branded search defense, where the facility is bidding on its own brand name to defend against competitor encroachment; that traffic is already brand-warm and needs less creative effort.
Our Google Ads strategy guide for behavioral health providers covers the search-specific creative pattern.
Meta (Facebook and Instagram). Mixed, leaning brand. The audience is in scroll-mode, not search-mode. Brand creative produces better engagement and lower CPMs.
DR creative still needs to be in the mix for conversion-attribution, but the ratio should run 60 brand / 40 DR or 50/50 for most behavioral health facilities.
The deeper read is in Facebook Ads vs Google Ads for addiction treatment.
YouTube and CTV. Heavy brand. Long-form video is the medium where brand creative produces the most lift, per Think with Google’s video marketing research. DR-style short cuts work on YouTube Shorts and pre-roll, but the platform rewards storytelling.
Facilities running YouTube and CTV should default to brand-quality creative with DR elements layered in rather than the opposite.
Programmatic display. Heavy brand. Display creative is functionally an awareness medium even when the operator buys it on DR metrics. The CPM is too low and the click-through rate too volatile to make DR display creative work for behavioral health in most cases.
Brand-quality display that reinforces the message from Meta and YouTube produces compounding recall lift.
OOH (out-of-home) and broadcast. Pure brand. The format does not support DR creative; the audience cannot click. Operators investing in OOH or broadcast for residential treatment are buying brand recall, not direct response. The measurement frame should match.
Reddit and community platforms. Mixed, leaning brand-adjacent. The audience is research-mode, evaluating options, talking to peers. DR-style creative reads as intrusive and produces backlash. Brand-quality content that respects the platform norm produces engagement and consideration lift.
The Reddit strategy for AEO citations in behavioral health covers the organic-side companion to this paid frame.
Compliance and the Brand vs DR Decision
The behavioral health compliance frame shapes the brand versus DR decision in ways that operators outside the category do not always appreciate. Three constraints matter.
LegitScript certification limits aggressive DR. Treatment center facilities running Google Ads must be LegitScript-certified, and the certification carries specific landing-page and creative requirements.
Outcome promises, statistical claims without substantiation, and aggressive urgency tactics that would work in other DR categories trigger LegitScript review and potentially loss of ad eligibility.
Google Ads healthcare policy adds another layer. Google’s ad policy framework layers healthcare-specific restrictions on top of LegitScript. The restrictions favor brand-quality creative that earns trust through credibility signals over DR creative that pushes urgency or coverage promises.
42 CFR Part 2 governs testimonial and alumni content. Federal SUD patient confidentiality law shapes what can appear in either brand or DR creative when patient stories are involved.
The constraint applies to both types but tends to favor brand creative because brand pieces typically use anonymized alumni stories with proper consent rather than testimonial-style content that crosses compliance lines.
The net effect of the compliance frame is that brand-quality and brand-informed DR creative are often more compliance-defensible than pure DR creative. The constraints push behavioral health advertisers toward production quality, named clinical leadership, and authentic storytelling, all of which are brand-creative features.
This is one of the underappreciated reasons that the hybrid brand-informed DR model is the highest-performing format in the behavioral health paid category.
Measurement: How to Tell What’s Working
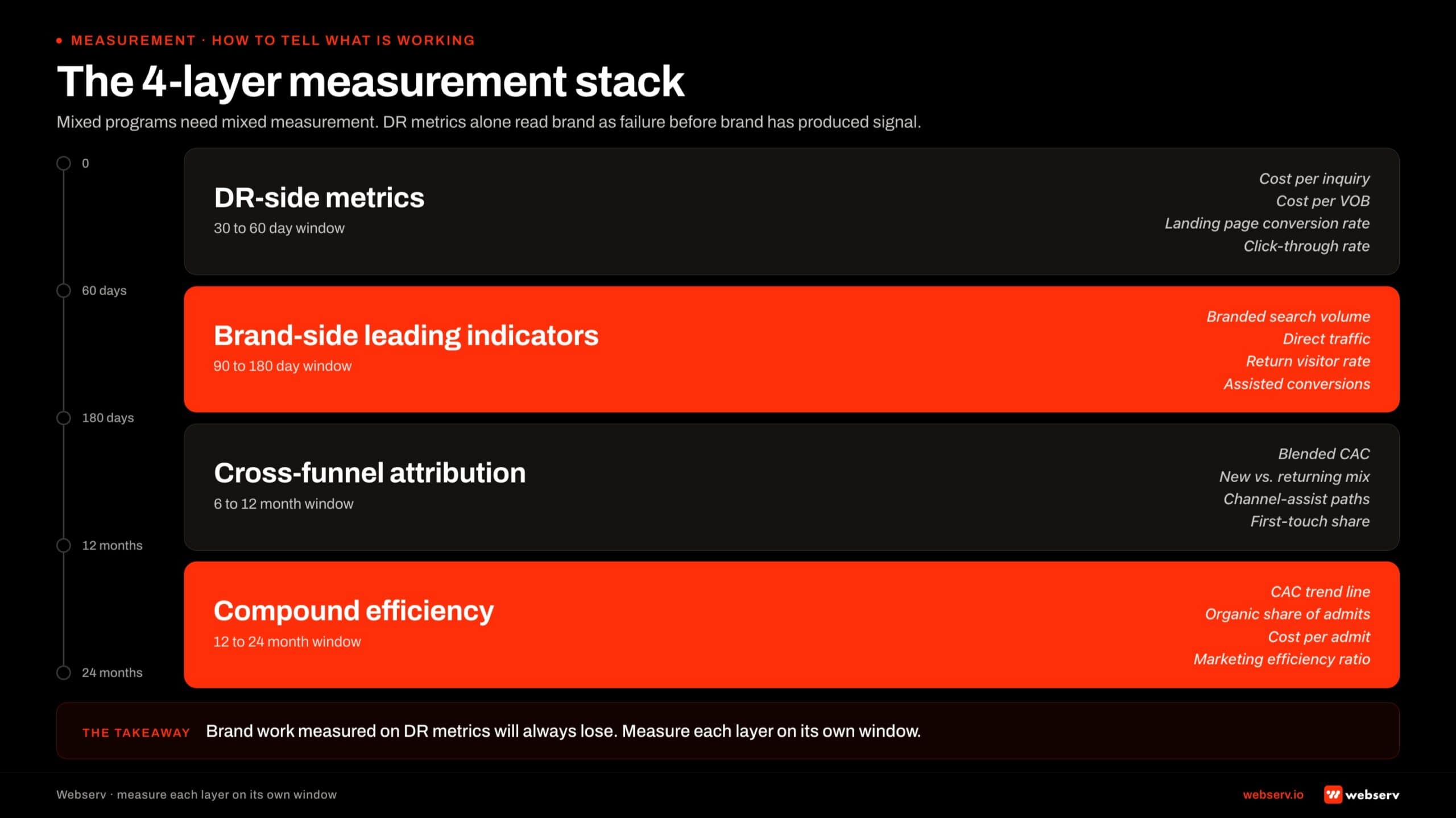
The measurement framework for a mixed brand-and-DR program is different from the framework for a pure DR program. Operators who keep measuring brand work on DR metrics conclude brand is failing before it has had time to produce signal.
Four measurement layers work together for a mixed program.
DR-side metrics inside a 30 to 60 day window. Cost per inquiry, cost per qualified lead, cost per admit attributed to paid clicks. These continue running on the standard cycle and remain the primary success measurement for the DR portion of the mix.
Brand-side leading indicators inside a 90 to 180 day window. Branded search volume in Google Trends, direct traffic to the facility’s domain, branded query click-through rate, and aided brand recall via survey panels for facilities at scale.
These metrics move first when brand creative is working, and they move before the DR-side lift shows up. Operators who track them early can validate the brand investment is producing signal months before the cost-per-admit shift shows up in the admissions data.
The cross-metric: DR efficiency over time. A working brand program shows up as DR cost per inquiry stabilizing or declining month over month at the same spend. The brand work is making the DR creative more efficient, which is the compounding interaction that justifies the brand budget.
Operators tracking DR efficiency alongside the brand-side leading indicators see the connection clearly inside 6 to 9 months of running the mixed program. Our 9 ways to lower cost per admit without cutting your ad budget covers the broader efficiency frame.
Cost per admit as the trailing indicator. The 12 to 18 month indicator. Cost per admit shifts last because it depends on every other variable in the program: lead quality, admissions team performance, payor mix, length of stay, and the audience evaluation cycle.
When cost per admit moves in the direction of the mix shift, the program is working at the compounding level.
The framework: DR-side metrics every 30 days, brand-side leading indicators every 90 days, DR efficiency trend every quarter, cost per admit annually. Each window matches the audience timeline of the creative type it measures.
The Right Mix by Facility Stage
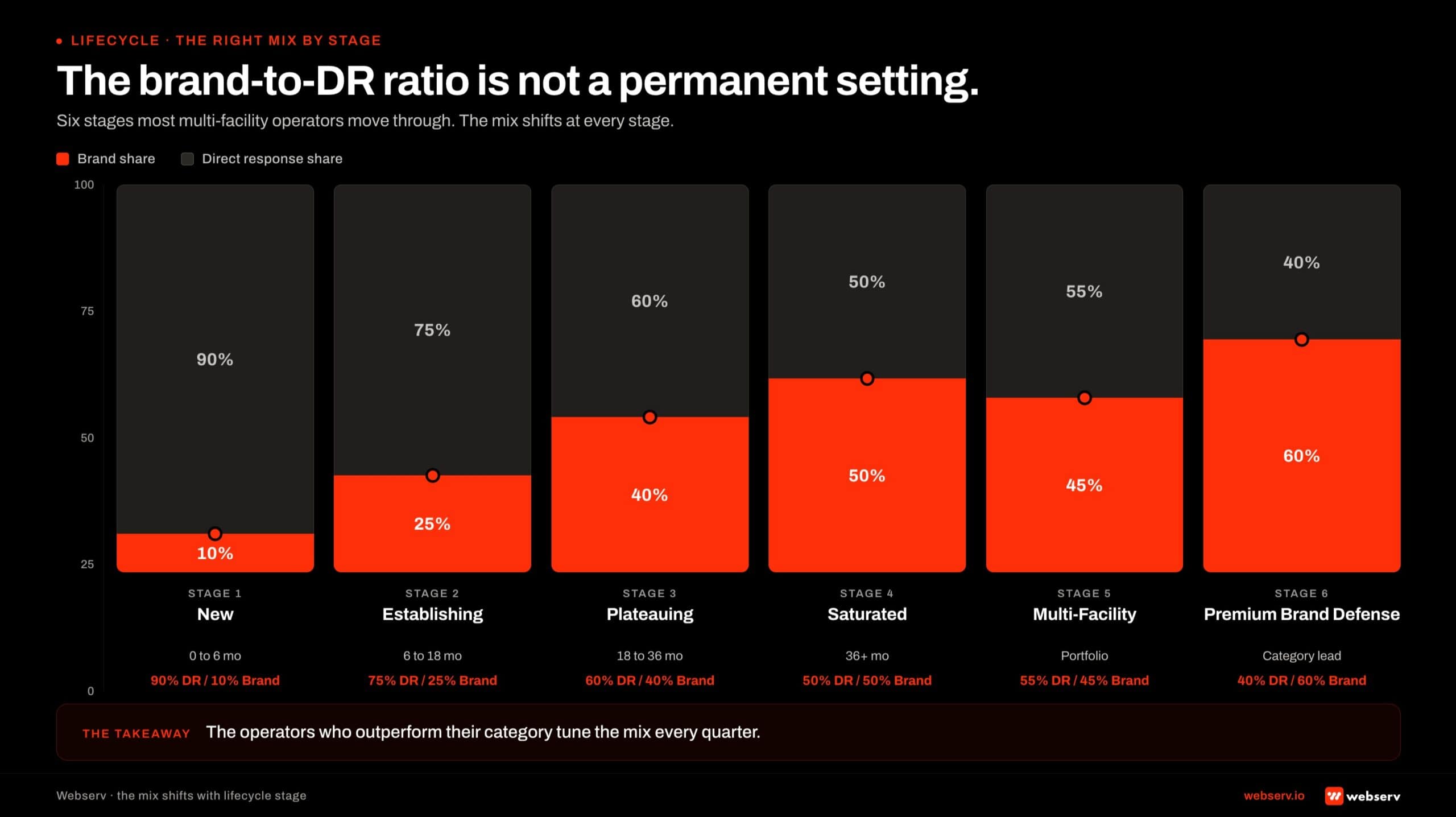
The brand-to-DR ratio is not a permanent setting. It should shift as the facility moves through lifecycle stages. Six stages cover most multi-facility operators we work with.
Stage 1: New facility, months 0 to 6. 90 percent DR / 10 percent brand. Lead volume is the load-bearing constraint. DR creative produces measurable inquiry volume in 30-day cycles.
The 10 percent brand allocation is institutional: founding story, named clinical leadership intro pieces, and the facility-environment content that begins building the brand library for later phases.
Stage 2: Establishing facility, months 6 to 18. 75 percent DR / 25 percent brand. DR is still doing the volume work, but brand creative is now compounding inside the 30 to 120 day evaluation window.
The first measurable brand-side lift on DR efficiency typically shows up at month 9 to 12 in this stage.
Stage 3: Mature healthy facility. 60 percent DR / 40 percent brand. The facility has measurable brand recall in its primary geographies. DR is still producing volume but the marginal dollar shifts toward brand work that compounds across the audience evaluation cycle.
Cost per admit on DR campaigns has stabilized or declined from the earlier stages.
Stage 4: Mature plateaued facility. 50 percent DR / 50 percent brand. Lead volume has flattened despite consistent or increasing budget. The DR audience is saturated.
The fix is heavier brand work to refresh the audience and reopen the DR funnel. This is the most common stage we audit and the stage where the mix shift produces the largest measurable lift.
Stage 5: Saturated metropolitan market. 40 percent DR / 60 percent brand. Facilities in saturated metros with 8 to 12 well-funded competitors all running similar DR creative pay an auction tax that brand creative is the cleanest way to escape.
The brand work is what differentiates the facility outside the auction moment.
Stage 6: Multi-state portfolio. 40 percent DR / 60 percent brand at the portfolio level, with per-facility variation based on individual facility stage. The portfolio-level brand work (national clinical leadership, network-wide outcome reporting, parent-organization storytelling) compounds across facilities and produces lift that single-facility brand work cannot.
The ratios are starting points, not benchmarks. Specific market conditions, payor mix, competitive density, and admissions team capacity all shift the right ratio for a given facility. The pattern that holds is the direction: as facilities mature and markets saturate, the brand allocation grows.
Operators who hold their brand-to-DR ratio constant for 18 months across stage changes leave performance on the table at every stage. The ratio is a quarterly portfolio decision, not a one-time configuration.
Frequently Asked Questions
Should we run brand creative if our cost per inquiry is already low?
Yes, with a measurement caveat. Low cost per inquiry on a pure DR program usually indicates one of two patterns: the program is early enough that audience saturation has not yet kicked in (months 1 to 9), or the facility operates in a less competitive geographic market. Both states are temporary.
The window before cost per inquiry starts climbing is the right time to start brand work, not the wrong time. Brand creative deployed during a healthy DR period produces compounding lift over the 6 to 12 month horizon and prevents the saturation ceiling from arriving as quickly.
Operators who wait until cost per inquiry has already doubled to consider brand are repairing damage instead of preventing it.
The recommendation is to allocate 15 to 25 percent of the paid budget to brand work even when DR metrics look healthy. The brand spend is insurance against the ceiling, and the math compounds either way.
How long does it take for brand creative to show results in our paid program?
Six to 9 months for first measurable lift on the DR side. Nine to 12 months for cost-per-admit shift to show up clearly. Twelve to 18 months for the full compounding to express across branded search volume, direct traffic, and the audience preference signals that lift every DR campaign the facility runs.
The timeline runs this long for the same reason behavioral health admit attribution runs slow: the audience moves through a 30 to 120 day evaluation window, and the brand creative deployed today is touching audiences that will not inquire for weeks or months. The measurement frame has to match the audience timeline.
Operators measuring brand creative on a 30-day window will conclude it is not working before it has had time to produce signal. The right approach is to set the brand budget as a 12-month commitment and measure cost per admit at quarter 2, quarter 3, and quarter 4 rather than on weekly creative-level metrics.
Can we use the same creative for Google Ads and Meta Ads?
Rarely. The audience intent profile is different enough that creative built for Google Search underperforms on Meta and vice versa. Google traffic arrives on commercial-intent queries and rewards DR creative with clear CTAs and credibility signals. Meta traffic arrives in scroll-mode and rewards brand-quality storytelling, named clinical leadership, and longer-form video.
The minimum viable separation for most operators is two distinct creative tracks: a DR-heavy track for Google Search and a brand-leaning track for Meta and YouTube. Each track gets adapted for the platform-specific aspect ratios, sound-off vs sound-on optimization, and the platform’s ad policy variants.
The exception is operators below $20K monthly spend where the production cost of two tracks does not fit the budget. For those operators, the brand-informed DR hybrid model (brand-quality production with clear CTAs) works across both platforms at moderate efficiency loss on each.
What’s the right brand-to-DR ratio for a new treatment center?
Ninety percent DR, 10 percent brand for the first 6 months. New facilities need measurable inquiry volume now, and brand creative does not produce measurable inquiry lift inside the first 90 days. DR-heavy is the right answer when the facility is building from zero.
Starting at month 6 to 9, shift the ratio toward 75 percent DR, 25 percent brand. The DR creative has produced enough volume to validate the audience and the offer. The brand work starts compounding for the second half of year one and into year two.
By month 18 to 24, the ratio should stabilize at 60/40 DR/brand for most mature healthy operators. Operators in saturated metros or running multi-state portfolios push further toward 50/50 or even 40/60 as the brand work absorbs the auction-tax pressure that pure DR cannot.
Does compliance push us toward brand or DR creative?
Toward brand-quality and brand-informed DR. LegitScript certification and Google healthcare ads policy both restrict aggressive DR tactics: outcome promises, statistical claims without substantiation, urgency framing that crosses into manipulation, and testimonial language that exceeds 42 CFR Part 2 patient confidentiality.
Pure DR creative that maximizes urgency and outcome-style language in other categories triggers compliance review or loss of ad eligibility in behavioral health. The constraint is not blocking DR creative; it is pushing the format toward brand-quality production and credibility-signal-driven persuasion that earns trust without violating the compliance frame.
The hybrid brand-informed DR model fits the compliance frame naturally because the brand-quality storytelling does the persuasion work that hard DR creative tries to do with outcome promises. Operators running this model encounter materially fewer compliance issues than operators running aggressive DR.
How do we know if our creative mix is wrong?
Six signals together. Cost per inquiry climbing month over month at the same budget. Lead quality declining (admissions team flags low-intent calls more frequently). Same creative templates running for 6+ months without performance lift. Branded search volume flat or declining in Google Trends. Direct traffic to the facility’s domain stagnant. Cost per admit higher than the 6-month rolling average.
One of these signals in isolation is normal noise. Three or more together over a 90-day window is the diagnostic that the creative mix needs to shift, almost always toward more brand work.
The fix is rarely a full pivot. The first move is reallocating 15 to 20 percent of the existing budget from DR toward brand work, holding the DR campaigns running, and giving the brand work 90 days to show first signal.
If cost per inquiry stabilizes or improves by month 3, the mix shift is working. If not, the diagnostic moves elsewhere (audience targeting, landing pages, admissions follow-up).
Stop Picking a Side, Start Tuning the Mix
The brand versus direct response question is the wrong way to frame the creative decision for a treatment center. The right question is what mix of brand and DR fits the channel, the facility stage, the audience segment, and the cost-per-inquiry trend the program is producing this quarter.
The mix is not a permanent choice. It shifts every quarter as the facility moves through lifecycle stages, as competitors enter or exit the market.
It also shifts as the audience cycles through evaluation windows, and as the compounding interaction between brand and DR shows up in DR efficiency metrics over 6 to 18 month horizons.
The operators we work with who outperform their category are the ones who treat the creative mix as an active portfolio allocation rather than a settled debate. Pure DR is wrong for mature facilities.
Pure brand is wrong for new facilities. The hybrid brand-informed DR model fits most operators most of the time, and the right ratio shifts with stage.
We help treatment center operators audit their current creative mix against the channel, stage, and audience framework, identify where the ratio is out of step with the facility’s real conditions, and rebuild the creative portfolio against the right mix for the program’s next 12 months.
Book an intro meeting to walk through your current creative mix, where the brand-vs-DR ratio is likely off for your stage, and what a portfolio rebuild would produce for cost per admit over the next two quarters.
For the upstream brief framework that shapes the creative production work, see our guide to building a creative brief for a rehab marketing campaign.
For the tooling side that supports the production, see the best ad creative tools for rehab marketing. For the agency side, see the top creative agencies for behavioral health.
And for the paid-targeting layer that pairs with the creative work, see the exclude-zip strategy for out-of-network family targeting.
Mitch Marowitz is the Director of Paid Admissions at Webserv. Webserv works with behavioral health and addiction treatment centers on paid media, SEO, and full-funnel admissions strategy.