
A treatment center sent us their “creative brief” last quarter. The document was 800 words. Three hundred were boilerplate company background. Two hundred were a list of competitors. A hundred were taglines the CEO liked.
The remainder named the deliverables they wanted: nine Meta videos, twelve static ads, a landing page hero image, and “whatever else makes sense.”
The actual brief work was missing. No audience definition beyond “people looking for treatment.” No message hierarchy. No compliance constraints in language the creative team could use. No metrics for what good looked like.
The agency producing the creative spent three weeks thrashing on round one. Round two added another two weeks.
The campaign launched late, missed the seasonal admit window, and produced 40 percent fewer admits than the prior year on a higher media spend. The post-mortem identified the brief as the failure point.
Inside Webserv’s creative practice for treatment centers, we treat the creative brief as the single most load-bearing document in any behavioral health marketing campaign.
In 2026, 70 to 80 percent of paid social performance now traces back to the creative itself per Meta Performance Marketing Summit data. The brief is no longer the formality it was a decade ago.
It is the contract between marketing and creative that predicts whether the campaign will produce admits or burn budget.
Our Creative Strategy Ultimate Guide covers the broader strategic philosophy this article operationalizes at the brief level.
This article walks through the 10 sections a working rehab creative brief needs, the seven behavioral-health-specific elements most briefs miss, and the four-step pre-send testing framework that catches problems before the creative team starts work.
Key Takeaways
- The creative brief is the single most load-bearing document in behavioral health marketing. Meta’s 2026 performance data attributes 70 to 80 percent of paid social performance to the creative itself, with targeting and budget responsible for only 20 to 30 percent.
- Most rehab creative briefs fail in predictable ways: they read as logo-and-tagline docs, treat “the patient” as one audience instead of three (patient, family member, referral source), bury compliance constraints in legal language no creative team can use, and skip the success metrics that tell creative what “good” looks like.
- A working brief has 10 sections covering business objective, compound prompt, three-audience definition, behavioral-health-specific compliance constraints, message and proof points, tone, deliverables, required/forbidden elements, distribution context, and success metrics.
- Seven behavioral-health-specific elements separate working briefs from generic templates: family-member-as-primary-audience framing, clinical reviewer workflow, platform-policy language in creative-readable form, forbidden visual elements, forbidden language, crisis-state user context, and the handoff to admissions.
- The brief should be tested before it goes to creative. The four-step pre-send framework (objective check, audience check, compliance check, metric check) takes 30 minutes and prevents weeks of agency thrashing on round one.
Why Most Rehab Creative Briefs Fail
MOST COMMON FAILURE MODE
The logo-and-tagline doc disguised as a brief. Company history, competitor lists, tagline preferences — none of it helps a creative team produce paid social ads. The second failure mode compounds it: writing to one audience instead of three. Behavioral health campaigns serve the patient, the family member researching for someone else, and the referral source (therapist, EAP rep, discharge planner). Each has a different fear pattern, decision timeline, and proof requirement. Merging them into one persona is why 80% of the copy gets rejected in review.
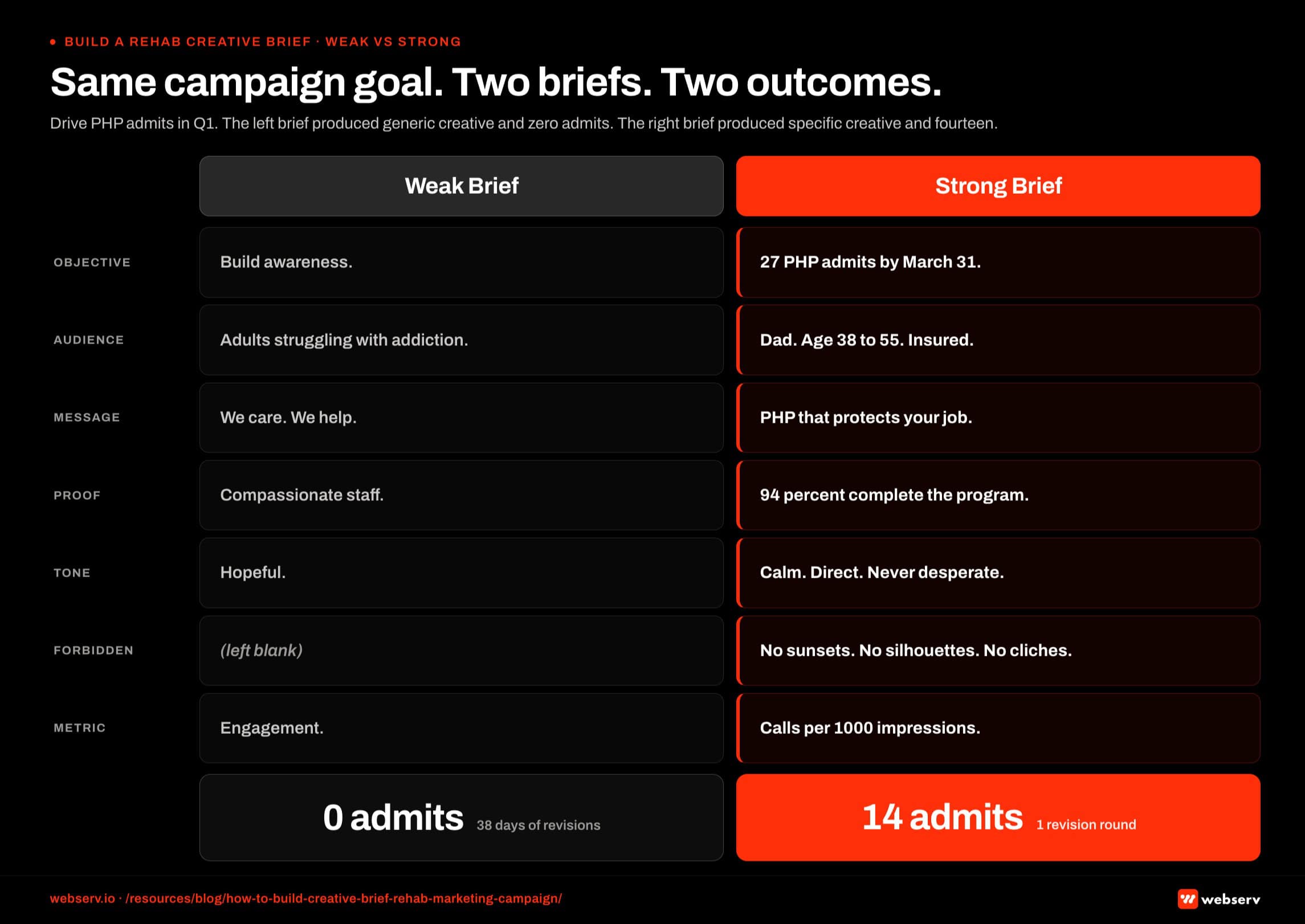 Side-by-side comparison infographic titled ‘Same campaign goal, two briefs, two outcomes.’ Two columns showing the same treatment center campaign briefed two different ways. Left column shows the weak brief: vague audience definition, missing compliance constraints, no message hierarchy, ambiguous tone. Outcome: 0 admits delivered, 38 days of revisions, 5 rounds of agency-versus-operator back and forth. Right column shows the strong brief: specific audience persona, clear compliance constraints documented, explicit message hierarchy, defined tone with examples. Outcome: 14 verified admits delivered, 1 revision round before launch, on-time delivery.
Side-by-side comparison infographic titled ‘Same campaign goal, two briefs, two outcomes.’ Two columns showing the same treatment center campaign briefed two different ways. Left column shows the weak brief: vague audience definition, missing compliance constraints, no message hierarchy, ambiguous tone. Outcome: 0 admits delivered, 38 days of revisions, 5 rounds of agency-versus-operator back and forth. Right column shows the strong brief: specific audience persona, clear compliance constraints documented, explicit message hierarchy, defined tone with examples. Outcome: 14 verified admits delivered, 1 revision round before launch, on-time delivery.Five failure modes show up repeatedly across the briefs we audit for treatment centers.
Failure mode 1: The logo-and-tagline doc disguised as a brief. Most behavioral health briefs are stuffed with company history, competitor lists, and tagline preferences. None of that helps the creative team produce paid social ads. The brief should be operator-current intent and audience truth, not corporate-marketing artifacts.
Failure mode 2: One audience instead of three. Behavioral health campaigns serve at minimum three audiences: the patient considering treatment, the family member researching options for someone else, and the referral source (clinician, therapist, EAP rep) directing patients.
Each has a different psychographic profile, decision frame, and creative response pattern. Briefs that lump them together produce creative that works for none of them.
Failure mode 3: Compliance buried in legal language. HIPAA, 42 CFR Part 2, LegitScript, and Meta’s healthcare advertising policies all impose creative constraints.
Briefs that list these as “follow all applicable regulations” force the creative team to re-derive the constraints from scratch every campaign, which produces inconsistent compliance and creative-review thrash.
Failure mode 4: No message hierarchy. Briefs that list ten things the campaign should say produce creative that says all ten badly. The working brief identifies one core message and three to five supporting proof points, and treats everything else as out of scope for this campaign.
Failure mode 5: No success metrics. “Drive admits” is not a metric.
The brief that defines success as “30 admits per month at under $3,200 cost per admit, with at least 40 percent commercial payer mix” gives the creative team a target. The brief that says “drive admits” lets the creative team produce anything and call it a win.
The 10-Section Brief Structure
The working brief has 10 sections. Each section gets a specific length, format, and content type. Skipping sections is more dangerous than padding them.
 Annotated anatomy infographic titled ‘The full anatomy of a working creative brief.’ Ten sections of the brief shown in their canonical order, each with the section name, the required output type, and the relative length budget. Sections include: campaign objective, audience definition, compliance constraints (HIPAA, LegitScript, self-harm classification), tone and voice, message hierarchy, format requirements per channel, asset deliverables list, approval workflow, success metrics, and reference materials. Annotations show which sections require operator input, which require strategy team input, and which require legal review before the brief ships.
Annotated anatomy infographic titled ‘The full anatomy of a working creative brief.’ Ten sections of the brief shown in their canonical order, each with the section name, the required output type, and the relative length budget. Sections include: campaign objective, audience definition, compliance constraints (HIPAA, LegitScript, self-harm classification), tone and voice, message hierarchy, format requirements per channel, asset deliverables list, approval workflow, success metrics, and reference materials. Annotations show which sections require operator input, which require strategy team input, and which require legal review before the brief ships.Section 1: Business Objective + Admit Target
The opening section defines the actual outcome the campaign exists to produce. Not “build awareness.” Not “drive engagement.” A specific admit volume, time horizon, and payer mix goal.
Strong example: “Produce 24 admits in Q2 2026 at or below $2,800 cost per admit, with at least 45 percent commercial-payer mix. Total media budget: $96,000.”
Weak example: “Increase brand awareness and drive qualified inquiries.”
The business objective is what every other section in the brief reverse-engineers from. Sections 2 through 10 don’t make sense without this anchor.
Section 2: The Compound Prompt the Campaign Answers
What’s the question the family member or patient is asking when they see this creative? Not the question the operator wishes they were asking. The actual question, in their words, at their moment of seeing the ad.
Strong example: “A mother whose 24-year-old son has been using fentanyl for 18 months is searching late at night for somewhere safe that will take him before he uses again.”
Weak example: “Adults seeking addiction treatment.”
The compound prompt frame comes from the AI search shift but applies equally to paid creative. Creative that answers a specific query outperforms creative that broadcasts to a category.
Section 3: Three-Audience Definition
Every behavioral health campaign serves at minimum three audiences. The brief defines each separately.
Audience A: The patient considering treatment. Demographic and psychographic profile. Decision frame. Common objections. Trigger events that move them from research to action.
Audience B: The family member researching for someone else. Often the primary audience for paid social. Different demographic skew (typically female, 45-65, mother of patient). Different decision frame (urgency, fear, hope). Different proof points that matter (safety, clinical credentials, family involvement in treatment).
Audience C: The referral source. Clinicians, therapists, EAP reps, judges in drug court. Smaller audience but high-value referrers. Different proof points (clinical outcomes, clinician communication, ASAM alignment).
The brief specifies which audience or audiences this specific campaign targets. “All three” is rarely the right answer for a single campaign.
Section 4: Behavioral-Health-Specific Compliance Constraints
Compliance lives in this section in creative-team-readable form. Not legal language. Not “follow all applicable regulations.” Specific, named, actionable.
The constraints that matter for most behavioral health paid social briefs:
42 CFR Part 2 prohibits any creative that identifies a person as having a substance use disorder. No “I was an addict” testimonials with identifiable faces. No before/after shots. No composite patient stories presented as real.
HIPAA prohibits any PHI use in creative. Even fictionalized clinical scenarios need to avoid implying real patients.
LegitScript landing-page standards require specific facility information and prohibit outcome promises. Creative that drives to LegitScript-certified landing pages must align with those standards.
Meta’s healthcare advertising policies prohibit personal-attribute targeting and limit some creative formats. The brief lists the specific Meta policies in play for this campaign.
Section 5: Core Message + Supporting Proof Points
One core message. Three to five supporting proof points. No more.
Strong example:
Core message: “Safe, clinician-led detox starting today: no waitlist for commercial insurance.”
Proof point 1: 24/7 medical detox supervision
Proof point 2: JCAHO accredited
Proof point 3: In-network with Aetna, Cigna, BCBS, United
Proof point 4: Median time from call to admit: 6 hours
Weak example: Ten bullet points covering history, modalities, levels of care, accreditations, location, payer mix, alumni stats, family programs, aftercare, and CEO quote.
The brief identifies the load-bearing message and ranks the proof points by importance. Creative production then has clear hierarchy decisions, not a buffet.
Section 6: Tone + Emotional Position
Tone defines how the creative feels, not what it says. For behavioral health, tone is constrained in specific ways.
Required: Compassion-first. Family-friendly. Clinically credible. Direct without being aggressive.
Forbidden: Fear-based. Shame-based. Outcome-promising. Patronizing.
The brief should give the creative team three to five reference points: existing creative they should match in tone, existing creative they should explicitly avoid, and the emotional register the family member viewing this should land in (relieved, hopeful, informed, not pressured).
Section 7: Required Formats + Deliverables
Platform-specific specifications. Asset counts. Aspect ratios. Durations. File formats.
Strong example by platform:
Meta: 8 video creatives (4 × 9:16 vertical 15s, 4 × 9:16 vertical 30s), 12 static creatives (6 × 1:1 square, 6 × 4:5 portrait)
Google Ads: 6 responsive search ads, 4 image extensions
Landing page: 1 hero image (1920×1080), 3 supporting graphics (800×600)
Production deadline: April 15, 2026 for May 1 launch
Weak example: “Standard paid social formats, plus whatever else makes sense.”
The format spec connects directly to the Meta ad formats that work for behavioral health in 2026 and the platform-specific creative requirements current at the time the campaign launches.
Section 8: Required vs. Forbidden Visual + Language Elements
This section catches what the rest of the brief might miss.
Required visual elements: trust badges (JCAHO, CARF, LegitScript), facility imagery (if appropriate), credentialed clinician images (with release), logo placement.
Forbidden visual elements: images implying patient identification, stock photo people who look like patients, before/after shots, drug paraphernalia imagery, anything that could read as glamorizing use.
Required language: facility name, credentials, payer mix language (“in-network with”), specific call to action.
Forbidden language: “addict” (use “person in recovery” or “person with substance use disorder”), outcome promises (“we cure”), guarantee language, exclusionary language that could violate fair housing or disability protections.
Section 9: Distribution + Media Plan Context
The creative team needs to know where the creative will run, against which audiences, at what frequency.
Strong example: “Primary distribution: Meta paid social, targeting custom audience of family members of past patients (anonymized) plus lookalike. Secondary distribution: Google Ads remarketing to landing page visitors. Frequency cap: 5 impressions per user per week.”
Weak example: “Paid social and Google Ads.”
The distribution context shapes creative decisions. Creative produced for a cold-traffic interruption looks different from creative produced for warm-audience retargeting. The brief specifies which.
Section 10: Success Metrics + Measurement Framework
The closing section defines what “this campaign worked” means in numbers.
Strong example by tier:
Primary: 24 admits at or below $2,800 cost per admit over the campaign period
Secondary: 45 percent commercial payer mix on admits attributed to the campaign
Tertiary: Creative-level CTR above 2.5 percent, video completion rate above 35 percent for video assets
Diagnostic: Form-fill to admit conversion rate, time-to-VOB, cost per qualified lead
The success metrics give the creative team a target. They also give the post-campaign analysis a framework that distinguishes creative performance from media buying performance from operational performance.
The 7 Behavioral-Health-Specific Elements Most Briefs Miss
Beyond the 10-section structure, seven specific elements separate working behavioral health briefs from generic templates.
Family member as primary audience for many campaigns, not the patient. Most behavioral health paid social does not actually target the patient. It targets the family member researching options for someone else.
The brief should specify this and design every other section (message, tone, proof points, format) around the family-member audience as primary, even when patient audiences are secondary.
The clinical reviewer credit and approval workflow baked into the brief. Healthcare YMYL content requires named clinical reviewer credit. The brief should specify which clinician at the facility will review the creative, what the review SLA is, and what the approval workflow looks like before creative goes live.
Platform-specific compliance language in creative-team-readable form. Most creative teams have not memorized Meta’s healthcare advertising policy. The brief should translate the policy into creative-actionable constraints: what visual elements trigger ad review, what language gets flagged, what audience targeting is restricted.
Forbidden visual elements named explicitly. Images implying patient identification. Stock photo people who look like patients. Before/after shots. Anything that could read as glamorizing substance use. Generic creative briefs do not catch these because they are behavioral-health-specific.
Forbidden language named explicitly. “Addict” as a noun. Outcome promises. Guarantee language. Patronizing tone. Family-blame language. Each of these has produced rejected ads or reputational issues at facilities we have worked with.
Crisis-state user context. The family member viewing this creative may be in tears at 11 PM looking for help. The creative must work in that emotional state. Generic templates do not specify this and produce creative tone-deaf to the actual viewing context.
The handoff to admissions. Creative produces a click. The next step (form, VOB, intake call) has to match the creative’s promise.
The brief should specify what happens after the click and confirm the creative does not over-promise relative to what the operator can deliver in the first 60 minutes after the inquiry.
The creative brief is the contract between marketing and creative. Briefs that try to be diplomatic produce creative that tries to be diplomatic, and diplomatic creative does not move admits. Briefs that name the audience, the message, the constraints, and the metrics directly produce creative that lands in the family member’s lap at 11 PM and makes the call easier to make. The brief is the most load-bearing document in the entire campaign.
Preston Powell, CEO of Webserv
How to Test the Brief Before Sending to Creative
A four-step pre-send framework catches most brief-level problems before the creative team starts work. The framework takes 30 minutes and prevents weeks of round-one thrashing.
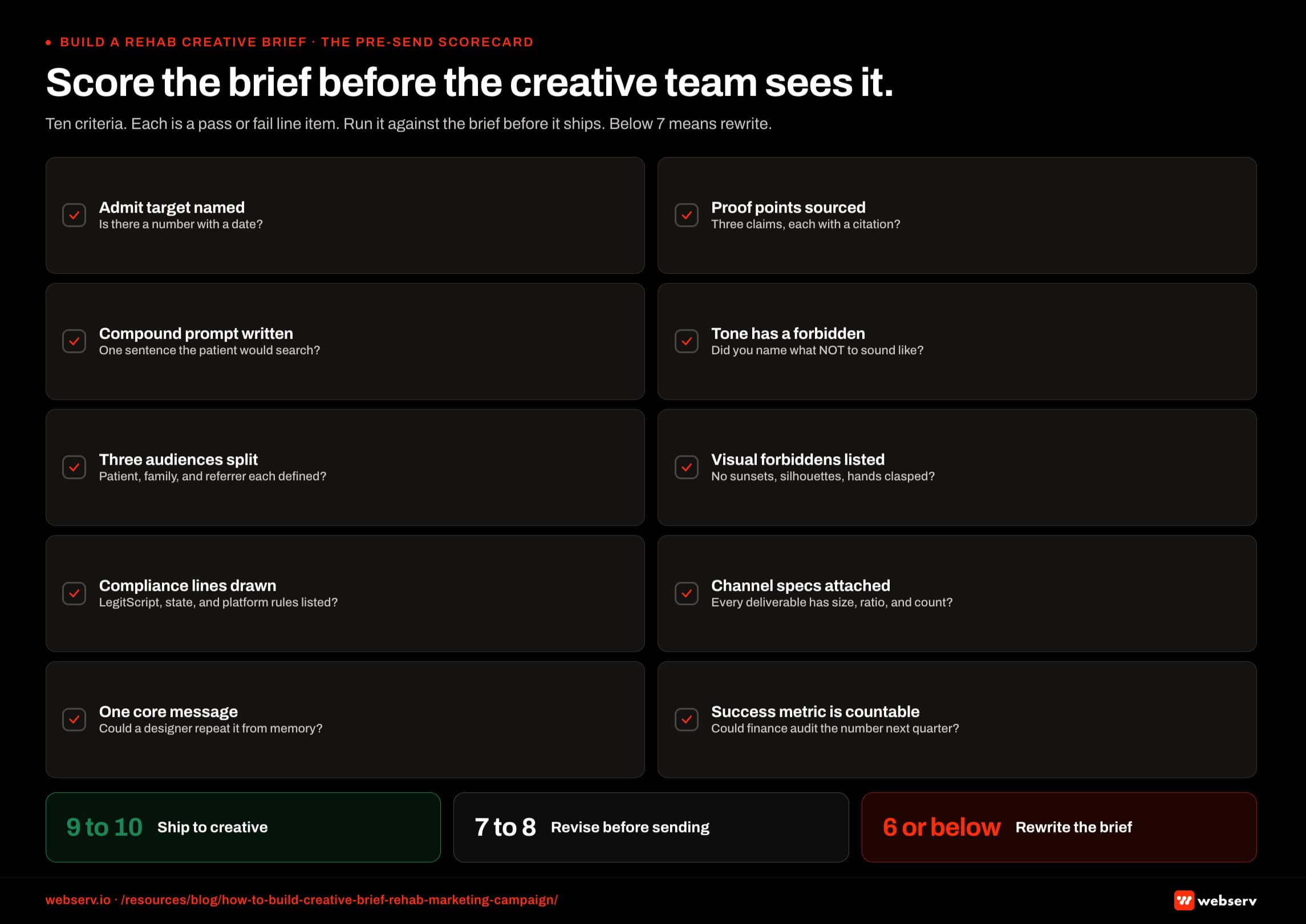 Ten-criterion pre-send scorecard infographic titled ‘Score the brief before the creative team sees it.’ Ten yes-no criteria the operator runs against the brief before shipping it to the creative team. Criteria include: audience defined with persona detail, compliance constraints documented, tone of voice specified with examples, message hierarchy ranked, success metrics named, deliverables itemized by channel, approval workflow mapped, reference materials linked, deadline calendar attached, and ownership assigned per section. Footer scoring band: 8 of 10 is the ship threshold, 6 to 7 of 10 requires revision, below 6 of 10 requires rewrite. Maps to the four-step pre-send framework in the article.
Ten-criterion pre-send scorecard infographic titled ‘Score the brief before the creative team sees it.’ Ten yes-no criteria the operator runs against the brief before shipping it to the creative team. Criteria include: audience defined with persona detail, compliance constraints documented, tone of voice specified with examples, message hierarchy ranked, success metrics named, deliverables itemized by channel, approval workflow mapped, reference materials linked, deadline calendar attached, and ownership assigned per section. Footer scoring band: 8 of 10 is the ship threshold, 6 to 7 of 10 requires revision, below 6 of 10 requires rewrite. Maps to the four-step pre-send framework in the article.Step 1: The objective check. Read Section 1 (business objective) and Section 10 (success metrics) back to back. If the numbers in Section 10 do not directly produce the outcome in Section 1, the brief is internally inconsistent. Fix before sending.
Step 2: The audience check. Read Section 3 (three-audience definition) and Section 5 (core message + proof points) together. Can each of the three audiences see themselves in the message?
If only one can, the campaign is single-audience and the brief should say so. If none can, the message is too generic. Fix before sending.
Step 3: The compliance check. Send Section 4 (compliance constraints) and Section 8 (required/forbidden elements) to the facility’s clinical reviewer and compliance lead. If either flags an issue, fix before sending to creative.
The cost of fixing a compliance issue at the brief stage is one hour. The cost of fixing it after creative production is two weeks.
Step 4: The metric check. Read Section 10 (success metrics) and ask: can the analytics stack actually measure these? If admit attribution is not working through to the ad platform, the campaign cannot be evaluated. Fix the measurement stack before the campaign runs, not after.
Briefs that pass all four checks ship to creative with high confidence of producing usable round-one work. Briefs that fail any check should not go to creative until the failure is resolved.
Frequently Asked Questions
How long should a rehab creative brief be?
Most working briefs run 1,500 to 3,000 words depending on campaign complexity. Single-platform campaigns (Meta paid social only) tend to land around 1,500 words. Multi-platform campaigns with multiple audiences run 2,500 to 3,000.
Briefs under 1,000 words almost always skip critical sections. Briefs over 4,000 words almost always pad with boilerplate that does not help the creative team produce work. The 1,500 to 3,000 word range is the operator-tested zone.
The length matters less than the section completeness. A 2,000-word brief that hits all 10 sections produces better creative than a 5,000-word brief that pads one section and skips another.
Should I include sample creative or moodboards in the brief?
Yes, but selectively. Three to five reference creatives the campaign should match in tone work well. Three to five reference creatives the campaign should explicitly avoid work even better. Twenty reference creatives confuse the creative team and signal that the operator does not actually know what they want.
The reference creatives should come with annotation: “match this tone, not this style,” or “avoid the fear-based hook in this ad,” or “the family-member voice in this script is what we want.” Bare reference dumps without annotation produce creative that mimics the references without understanding why.
For behavioral health specifically, include at least one reference of a creative that was rejected by Meta or Google ad review at another facility, with annotation on why it was rejected. This single inclusion catches more compliance issues than any other element of the brief.
Who should write the creative brief for a treatment center?
The marketing director typically writes the brief with input from three other functions: the admissions director (for the operational context of what happens after the click), a clinical reviewer (for the compliance and accuracy review), and the facility’s leadership (for the business objective and metric targets).
The agency or creative team consuming the brief should not write the brief. Agencies that write their own briefs end up briefing themselves toward what they want to produce, not what the facility needs.
If the marketing director is new to behavioral health and has not written a behavioral-health-specific brief before, the right move is to have a behavioral-health-specialist consultant review the brief before it goes to creative. The cost of that review (typically $500 to $2,000) is materially less than the cost of three weeks of agency thrashing on round one.
How often should we update the brief during a campaign?
The brief is a starting document for a campaign, not a living document. Once creative is in production, the brief should not change. Changes to the brief mid-production produce thrash and miss launch deadlines.
What should update is the next campaign’s brief, informed by what the prior campaign produced. After every campaign, the post-mortem feeds the next brief’s audience definition, message hierarchy, and success metrics. Briefs that learn from prior campaigns over 4 to 6 cycles produce much stronger creative than briefs written from scratch each time.
For multi-month evergreen campaigns, plan to re-brief every quarter. The audience, message, and creative formats shift faster in behavioral health than in most categories, and quarterly re-briefing catches the drift before it compounds.
What’s the right brief format: document, slide deck, or template tool?
For most behavioral health operators, a written document (Google Docs or Word) at 1,500 to 3,000 words is the right format. Slide decks force brevity that often skips load-bearing detail. Template tools (Asana, Monday, dedicated brief tools) work for high-volume creative shops but add overhead for the typical behavioral health operator running 4 to 8 campaigns per year.
The format matters less than the section completeness. A well-written Word doc beats a half-completed Asana template every time.
For campaigns involving multiple internal stakeholders (marketing, admissions, clinical, compliance, legal), a shared document with comment threads produces better internal alignment than a static document. The comments catch ambiguity before it reaches creative.
What’s the most important section in the brief?
Section 5 (core message + supporting proof points) is the single most important section because it constrains every creative decision downstream. A clear, single core message with ranked proof points produces tight creative. A vague message or unranked proof points produces creative that tries to say everything and lands nothing.
Even so, briefs that nail Section 5 but skip Sections 3 (audience) and 10 (metrics) still produce work that misses. The 10-section structure works as a system. The marginal value of any single section depends on the other nine being in place.
If you have to start somewhere, start with Section 1 (objective), Section 3 (audience), and Section 5 (message). Those three sections produce 70 percent of the impact. The other seven sections refine and constrain.
Build Briefs That Produce Admits, Not Agency Thrash
The creative brief is the most load-bearing document in behavioral health marketing. With 70 to 80 percent of paid social performance now traceable to the creative itself, the brief is the contract between marketing and creative that predicts whether the campaign produces admits or burns budget.
The 10-section structure, seven behavioral-health-specific elements, and four-step pre-send testing framework in this article produce briefs that ship to creative with high confidence of round-one usable work.
The cost of building a working brief is 4 to 8 hours of internal work. The cost of sending an incomplete brief is typically 3 to 6 weeks of agency thrashing plus a missed seasonal admit window.
We help treatment centers build briefs for paid social, paid search, content, and integrated campaigns. For operators running 4 to 8 campaigns per year, the brief framework produces compounding returns as each campaign’s brief informs the next.
Book an intro meeting to walk through your current campaign brief process, where the brief failures are likely costing you admits, and how a structured 10-section framework would change the creative output your facility receives.
For the broader picture of how creative fits inside a full treatment center marketing program, see our ultimate guide to behavioral health marketing and our creative strategy ultimate guide.
Mitch Marowitz is Director of Paid Media at Webserv, where he leads paid search, paid social, and CRO programs for behavioral health and addiction treatment centers across the U.S. He writes about treatment-center paid media performance, creative testing, and the operational realities of running high-acuity healthcare campaigns.






