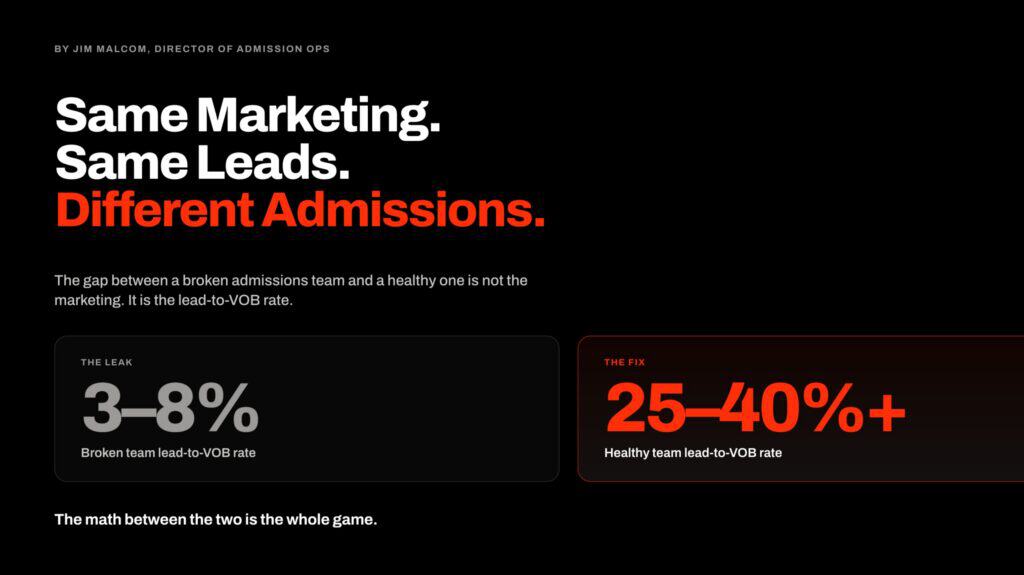
A treatment center we audited last quarter had 247 blog posts published over 30 months. The architecture was the WordPress default: a chronological /blog/ feed, posts assigned to one or two broad categories, no clear hub pages, no named author pattern.
Organic search was producing 14,200 sessions a month. Admit-attributed conversion from blog traffic over the prior six months: 1 admit.
The reorganization took 90 days. We collapsed the post library into a hub-and-spoke architecture organized around condition pillars, modality clusters, level-of-care pages, geographic anchors, and a family-facing resource hub.
Every YMYL post got a named clinical author and reviewer credit. Internal linking density tripled. Forty-three orphaned thin posts were 301-redirected to relevant hubs and unpublished. Schema was deepened across the cluster.
Over the following 120 days, organic search sessions to the blog held roughly flat. AI Overview citation share for the facility’s condition queries rose 4x. Admit-attributed conversion from organic traffic rose 31 percent.
The post count went from 247 to 168. The volume of work decreased; the architecture made the remaining work compound.
247 → 168
Post count after a 90-day reorganization (-32%)
4x
AI Overview citation share for condition-cluster queries
+31%
Admit-attributed conversion from organic traffic
This piece is the operator-facing playbook for blog and resource architecture that actually drives treatment center admissions in 2026.
The framework synthesizes the current state of the art with what Google itself published in its official June 2026 generative AI optimization guide and reflects the practical reality of how the BH category specifically converts.
The full SEO program context lives in our content SEO capability work. This article is the architecture layer that decides which posts you build, how they link, and what makes the library compound rather than dilute.
The 2026 Reframe: AEO Is Still SEO
Key Takeaways
- The 2026 architecture conversation is not “SEO vs AEO.” Per Google’s June 2026 official guidance, optimizing for generative AI search is still SEO, and the same architectural principles that produce strong organic ranking produce strong AI citation share. The frame is unified, not split.
- The hub-and-spoke architecture remains the load-bearing pattern, but its 2026 form is shaped by how RAG (retrieval-augmented generation) and query fan-out actually work. Google’s AI features pull from the index using the same ranking systems. The architecture has to serve both human readers and the model’s fan-out queries.
- Google’s official guidance now centers on “non-commodity content” (unique, experience-led perspective) over “commodity content” (the “7 Tips” listicle pattern). Treatment center blog libraries built on commodity content are at structural disadvantage in both organic ranking and AI citation. The architecture has to reward depth, not volume.
- Five hub categories cover almost every admit-driving content category in BH: condition pillars, modality clusters, level-of-care pages, geographic anchors, and the family-facing resource hub. The architecture is the matrix that interconnects them, not the individual posts in isolation.
- The 90-day reorganization sequence produces traffic-holding-flat with materially better conversion. Most BH facilities should expect post count to decrease 20 to 40 percent and admit-attributed conversion to rise 20 to 40 percent in the first 120 days after reorganization. The compounding effect runs longer.
Before the architecture conversation makes sense, the operator needs to internalize the framework Google itself articulated in mid-2026.
The AEO and GEO industry that emerged in 2023 and 2024 around AI Overviews and ChatGPT citations was operating on the assumption that AI search was a fundamentally different optimization surface from traditional SEO.
GOOGLE’S JUNE 2026 POSITION
Per Google’s official Generative AI Search Optimization guide (updated June 15, 2026): "optimizing for generative AI search is optimizing for the search experience, and thus still SEO." AI Overviews and AI Mode rely on Google’s core ranking and quality systems. The infrastructure is unified, not split.
DEFINITION
Query Fan-Out
The mechanism Google’s AI search systems use to decompose one user query into 6 to 15 concurrent sub-queries (interventions, MAT, family resources for a question about “fentanyl treatment for my son”), each routed through Google’s ranking. The cited sources are the union of what gets retrieved across the fan-out set.
Google’s official position, published June 15, 2026, is the opposite. AI Overviews and AI Mode rely on Google’s core ranking and quality systems. Retrieval-augmented generation (RAG) pulls candidate sources from the same Search index that ranks classic blue-link results.
Query fan-out generates additional related searches that the model then runs through the same ranking systems. The infrastructure is unified.
For treatment center operators, the implication is simple. The architecture that ranks well in classic organic search is also the architecture that earns AI Overview citation share. The architecture that scatters thin posts across a generic /blog/ feed underperforms in both surfaces simultaneously.
The 90-day reorganization work is not “AEO” work distinct from “SEO” work. It is the unified work that serves both.
What does change in the 2026 frame is the emphasis. Three pieces of Google’s guidance matter most for treatment center architecture.
Non-commodity content over commodity content. Google explicitly contrasts “7 Tips for First-Time Homebuyers” (commodity, recyclable) against “Why We Waived the Inspection and Saved Money: A Look Inside the Sewer Line” (non-commodity, experience-led). The non-commodity frame favors expert depth over surface-level coverage.
For BH, this means named clinician perspective over generic “what is addiction” explainer content. The deeper read on the YMYL implications lives in how to build clinical content Google trusts and patients actually find. Google’s own helpful-content guidance (updated December 2025) is the official reference for the broader people-first framework.
Architecture for query fan-out. When the user types “how do I help my son who’s using fentanyl,” Google’s model generates concurrent fan-out queries like “fentanyl addiction treatment,” “interventionist for opioid use,” “rehab for fentanyl users,” and routes each through ranking.
The architecture has to cover the fan-out surface, not just the originating query. We covered the tactical fan-out layer in our fan-out query analysis for AI search optimization piece.
Avoid mass-produced fan-out content. Google’s same guidance is explicit that creating separate posts for every possible fan-out query, primarily to manipulate ranking, violates the scaled content abuse spam policy.
The right architecture covers fan-out through depth in hub pages and natural cross-linking, not through 200 thin posts targeting micro-variations.
The Hub-and-Spoke Architecture Updated for 2026
The hub-and-spoke model has been the dominant content architecture pattern for healthcare SEO since 2018. The 2026 form retains the core structure but adjusts the implementation for current ranking realities.
Hub pages are the deep, authoritative pages that anchor a topic. For treatment centers, hubs cover conditions (alcohol use disorder, opioid use disorder, anxiety, depression, co-occurring disorders, eating disorders, trauma) and modalities (CBT, DBT, EMDR, MAT, ketamine-assisted therapy, TMS).
Hubs also cover levels of care (detox, residential, PHP, IOP, outpatient, sober living, aftercare), geographies tied to real facility presence, and the family-facing resource cluster.
A hub page runs 2,500 to 6,000 words, is anchored by a named clinical author and reviewer, cites peer-reviewed sources inline, and serves both the human reader and the RAG retrieval pattern.
The hub is the page that earns most of the cluster’s links, ranks for the high-volume head terms, and appears in AI Overviews when the originating query maps to the hub topic.
Spoke articles are the cluster pages that orbit the hub. Each spoke addresses a more specific question, sub-topic, or audience segment within the hub topic.
A spoke runs 1,200 to 2,800 words, links back to the hub and to other relevant spokes, and serves the long-tail and fan-out queries the hub does not cover directly.
The relationship between hub and spoke is the load-bearing piece. The hub gets linked from every spoke in the cluster. The spokes get linked from the hub via a structured “related topics” or “explore further” section.
The internal linking density across the cluster is what produces the topical authority signal Google’s ranking system rewards.
What changes in 2026 is the criteria for what makes a spoke worth building.
The pre-2024 rule was “build a spoke for every long-tail keyword.” The 2026 rule, per Google’s own guidance, is “build spokes where you have something non-commodity to say.”
Spokes that exist only to capture a keyword variation get categorized as scaled content abuse and produce ranking drag, not lift. Spokes that exist because a named clinician has direct, experience-led perspective on a specific question produce the lift.
Topical authority for treatment centers covers the broader framework. The hub-and-spoke architecture is the structural pattern that implements the topical-authority strategy.
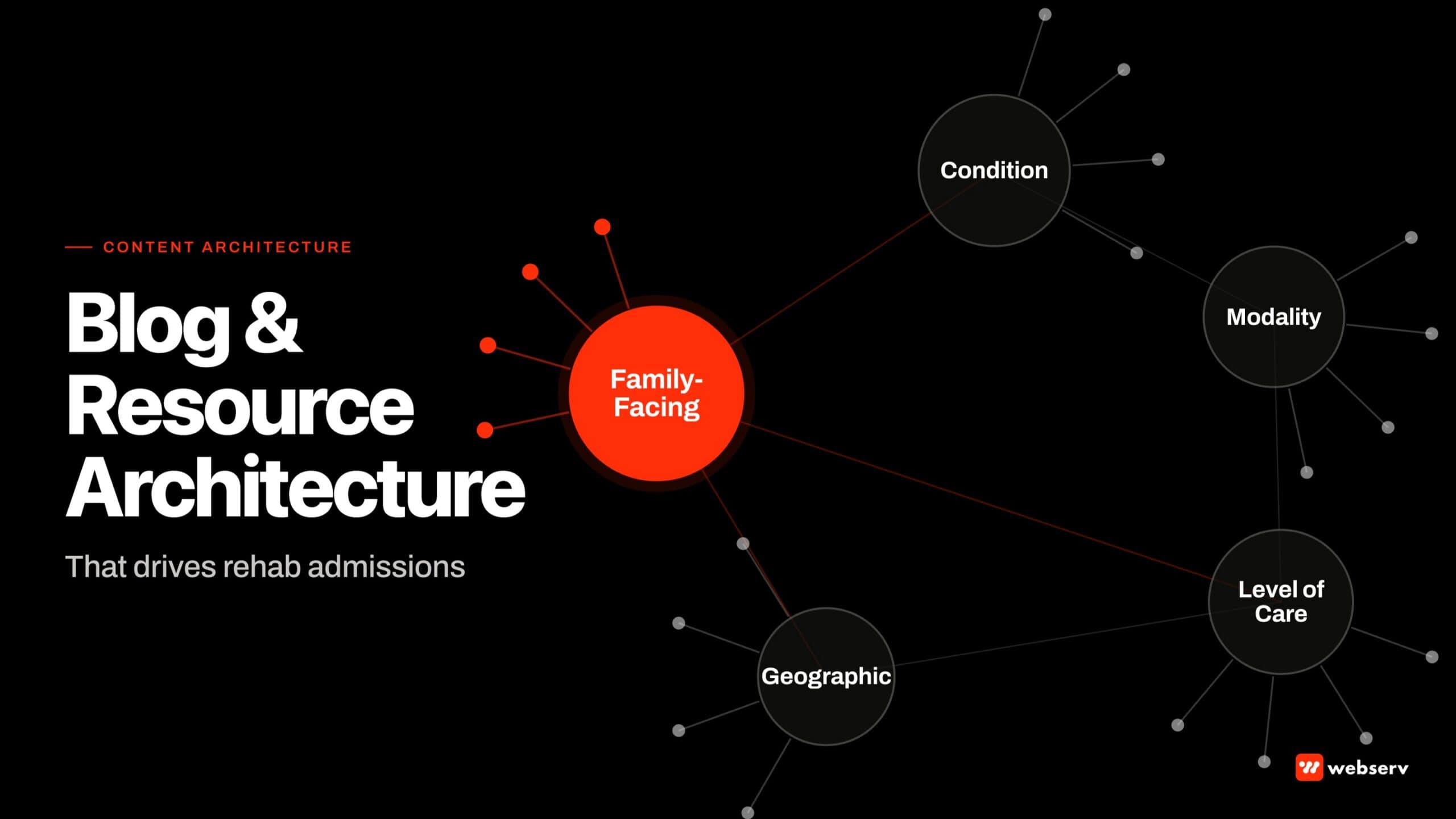
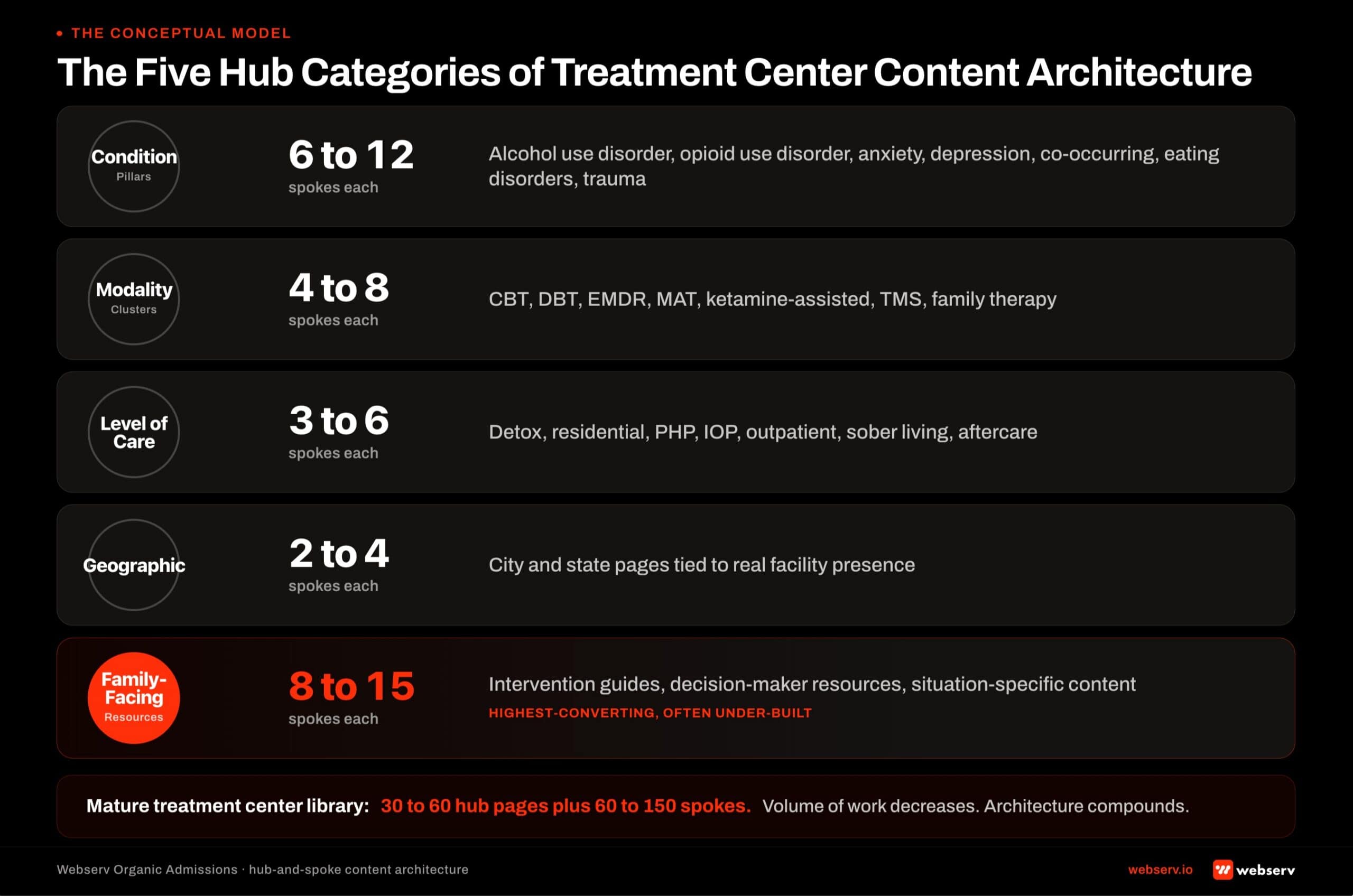
Five Hub Categories That Drive Admit Conversion
Treatment center blog and resource architecture clusters around five hub categories. Almost every admit-converting content category fits into one of these five.
1. Condition pillar hubs. Alcohol use disorder, opioid use disorder, anxiety disorders, depression, co-occurring disorders, eating disorders, trauma. Each condition is a hub.
The hub covers clinical definition, prevalence, symptoms, common patient and family questions, treatment approaches, what to expect at the facility, and the bridge to the inquiry call.
Each condition pillar gets 6 to 12 spoke articles that address sub-topics: “alcohol withdrawal timeline,” “opioid use disorder and pregnancy,” “high-functioning depression at work.”
2. Modality cluster hubs. Treatment approaches the facility offers. CBT, DBT, EMDR, medication-assisted treatment, ketamine-assisted therapy, TMS, trauma-informed care, family therapy, group therapy.
The hub covers how the modality works, what conditions it is most effective for, what the evidence base looks like, and how the facility delivers it. Each modality hub gets 4 to 8 spokes that go deeper on specific applications.
3. Level-of-care hubs. Detox, residential, partial hospitalization (PHP), intensive outpatient (IOP), outpatient, sober living, aftercare. The hub covers what the level of care involves, the typical day, the clinical hours, who fits and who does not, insurance patterns, and transition criteria to the next level.
Each LOC hub gets 3 to 6 spokes for sub-topics like “what to bring to detox,” “how to talk to your employer about IOP,” “PHP weekend schedule expectations.”
4. Geographic and intent-modifier hubs. Tied to real facility presence. Hubs for the cities and states where the facility operates, the in-state insurance pattern, and the local treatment landscape.
Each geographic hub gets 2 to 4 spokes for specific intent modifiers like “alcohol rehab covered by [in-state Blue Cross plan]” or “12-step alternatives in [city].”
The deeper read on the geographic-architecture trap lives in the cost of doorway pages on behavioral health sites. Geographic hubs only work when grounded in real local presence.
5. Family-facing resource hub. Often the most under-built and highest-converting hub category.
The hub covers the questions family members actually ask: “how do I get my child into rehab,” “what to do when a loved one refuses treatment,” “interventions and how they work.” The family-facing hub gets 8 to 15 spokes for the specific situations family members find themselves in.
The five hubs together typically cover 30 to 60 hub pages and 60 to 150 spoke articles for a mature treatment center library.
The 247-post library in our intro war story had post volume but not category coverage. The reorganized 168-post library covered all five hubs deeply and produced more admit-attributed conversion across less content.
The Spoke Articles That Compound Per Hub
What separates a spoke that compounds from a spoke that dilutes is whether the article has something non-commodity to say. The Google-published distinction between “7 Tips” content and experience-led content applies directly to BH spoke selection.
Three spoke patterns reliably compound.
The clinician perspective spoke. A spoke written by or in close collaboration with a named clinician at the facility, addressing a specific clinical question with first-hand experience. “How our clinical team approaches dual-diagnosis assessment during residential admission” outperforms “What is dual diagnosis treatment” because the former is non-commodity and the latter is commodity.
The family member perspective spoke. A spoke written for the family member with specific, situation-based framing. “What to say to your adult child after their third overdose” outperforms “How to talk to a loved one about addiction” by orders of magnitude on conversion. The specificity is the non-commodity signal.
The operational reality spoke. A spoke that exposes the actual operational reality of treatment, written with the candor that a marketing-voice piece typically avoids. “What insurance actually pays for residential treatment in 2026” outperforms “Does insurance cover rehab” because the former takes a real position and provides defensible information.
What does not compound: the keyword-targeting spoke. Articles built primarily to capture a specific search query, without something non-commodity to say, get categorized by Google’s systems as scaled content abuse and produce ranking drag. The case against generic healthcare content farms in addiction treatment covers the broader pattern.
Volume was the strategy from 2018 to 2023. Depth is the strategy from 2024 forward. The treatment centers winning the next decade of organic admissions are the ones reorganizing the library to compound rather than dilute, and that reorganization is structural, not a content calendar tweak.
Preston Powell, CEO of Webserv
The right read on spoke selection is to start with the question and ask “does our facility have non-commodity perspective on this?” If the answer is yes, build the spoke.
If the answer is no, do not build the spoke just because the keyword has volume. The architecture is better off with 60 high-perspective spokes than 200 keyword-targeting spokes.
Internal Linking Architecture: The Relational Layer
The architecture is not the hubs and spokes themselves; the architecture is the relationships between them. Internal linking is the relational layer that produces topical authority and, in 2026, increasingly mediates how AI systems understand the cluster.
Three linking patterns reliably compound.
Hub-to-spoke and spoke-to-hub. Every spoke links to its parent hub in the first 300 words of the article. The hub links to every spoke in a structured “explore further” or “in this series” section, ideally with descriptive anchor text rather than generic “click here” patterns.
The hub-spoke linking density is the load-bearing topical authority signal.
Cross-cluster linking. Spokes link to relevant spokes in adjacent hubs where the cross-reference produces reader value. An “EMDR for trauma” spoke in the EMDR modality cluster links to the “PTSD” condition hub and to the “trauma-informed care” modality hub.
The cross-linking is what makes the cluster behave as an interconnected knowledge graph rather than a set of isolated articles.
Resource and capability page linking. Spokes link back to the relevant capability page (for example, our work on entity SEO for treatment centers in AI search) and to the broader resource hub. The capability links serve the conversion function. The resource hub links serve the navigational function.
The 1-link-per-300-words density rule remains the practical benchmark for internal linking in 2026, with adjustments by content type. Hubs typically run higher density (more spokes to link to).
Spokes run at the standard density. Service pages and capability pages run lower density (sales pages should not be link farms).
What does not work: orphan articles with no inbound or outbound internal links, deep-nested articles that take 4 clicks to reach from the homepage, and “related posts” widgets that auto-populate based on category rather than editorial curation.
Each of these breaks the relational layer that Google’s ranking systems rely on to evaluate topical authority.
Non-Commodity Content Per Google’s 2026 Framework
The single most important shift in Google’s 2026 official guidance is the explicit framing of “non-commodity content” as the differentiator that produces ranking and AI citation lift. The implication for treatment center blog architecture is meaningful.
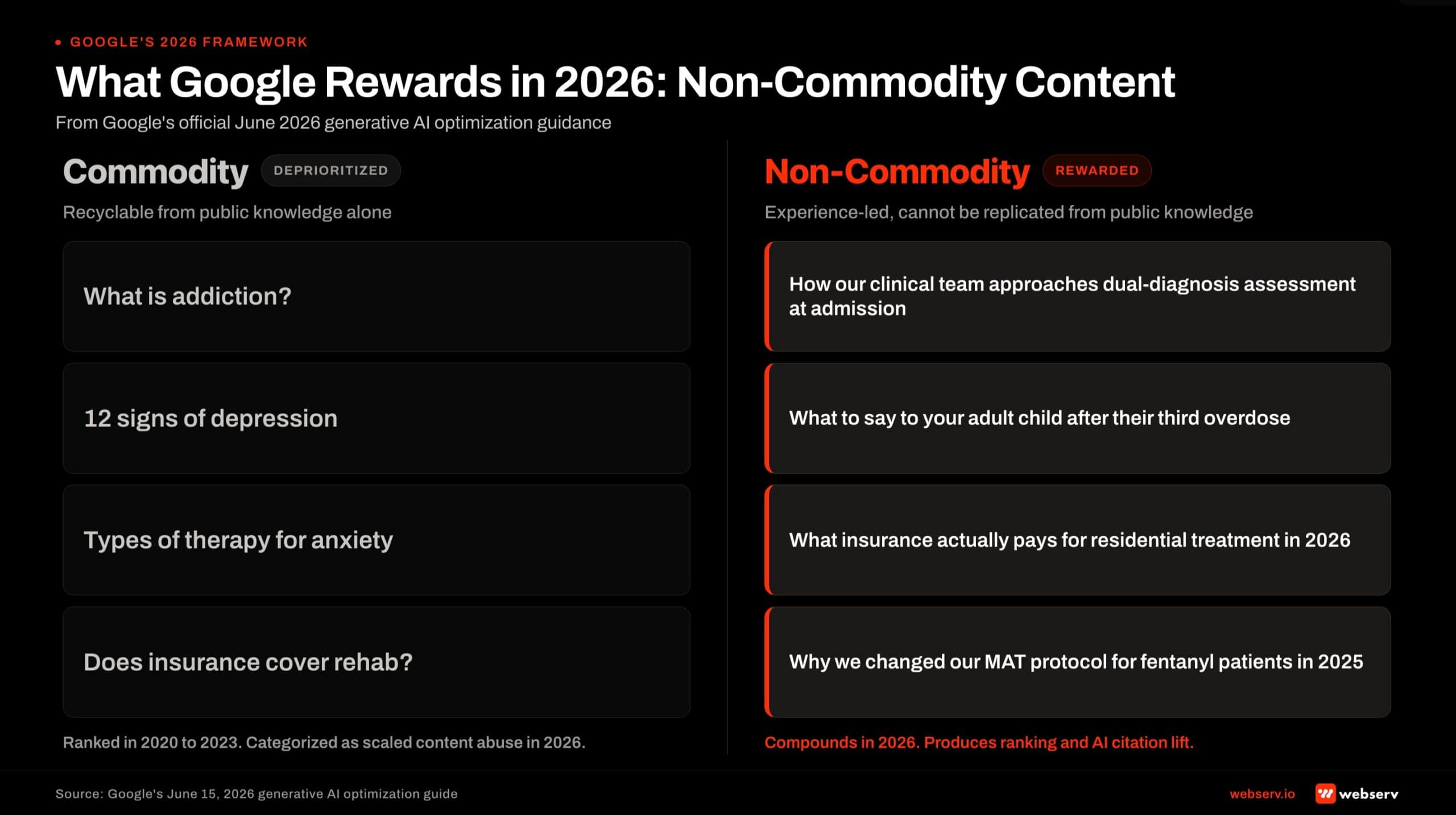
Commodity content for BH includes: generic “what is addiction” explainers, “12 signs of depression” listicles, “types of therapy for anxiety” overview pages, and other articles that any AI model could produce from common knowledge.
These articles ranked in the 2020-2023 era because volume mattered more than depth. In 2026, Google’s systems specifically deprioritize commodity content that adds no unique perspective.
Non-commodity content for BH includes: first-person clinician reflections on treating specific patient profiles, anonymized case study walk-throughs (with appropriate 42 CFR Part 2 consent), facility-specific outcome data discussions, named clinical staff debate on treatment philosophy, and the operational-reality articles we discussed earlier.
These articles rank because they cannot be replicated from common knowledge alone.
The architectural implication is that the spoke selection process should default to non-commodity over commodity. Operators evaluating whether to build a spoke should ask: “What does our facility know about this that an AI could not write from public information alone?” If the answer is “nothing distinctive,” skip the spoke. If the answer is “we have direct experience that produces a distinctive perspective,” build the spoke.
The named clinical authorship pattern reinforces non-commodity content. A spoke with “Dr. Sarah Chen, Clinical Director” as author and her professional bio, headshot, and credential page linked is structurally non-commodity in a way a “by Editorial Team” article cannot be. The author bios that build E-E-A-T for behavioral health blogs framework covers the bio anatomy that makes this work.
Author Architecture: The E-E-A-T Foundation
Named clinical authorship is the load-bearing E-E-A-T signal for treatment center YMYL content. Google’s helpful-content guidance treats clinician-credentialed articles as fundamentally different from articles written by uncredentialed staff or AI tools.
Three components of the author architecture matter most for the hub-and-spoke build.
Named author + named clinical reviewer on every YMYL piece. The author is the primary writer (often a senior clinician or the content team supported by a clinician). The reviewer is a different named credentialed clinician who validates the clinical claims. Both names appear on the byline. Both have linked author archive pages.
Structured author bio pages. Each author has a dedicated /author/[name]/ page with full credentials, licensure, NPI sameAs link, professional photo, brief bio, and a paginated list of every article they have authored or reviewed. The author page is the entity anchor Google’s knowledge graph uses to attribute content to the person.
Author connection to professional identity. The author bio page should link out to the clinician’s LinkedIn, professional association profile, published research, and any other authoritative references that establish the clinician as a real, credentialed entity. Clinicians as AEO moat: why author quotes beat generative AI covers why this matters specifically for AI citation eligibility.
Operators with strong author architecture frequently see AI citation share lift 3-5x relative to operators publishing the same content under “Editorial Team” bylines. The architecture work is upstream of the writing work.
Schema and Technical Infrastructure (With Important Nuance From Google)
Google’s June 2026 guidance is specific that structured data is not required for AI search to surface a page. The systems can crawl and interpret well-structured HTML without schema. That said, schema remains valuable for treatment center content for the same reasons it has always been valuable: it eliminates ambiguity, helps Google’s entity graph map the facility, and supports rich result eligibility. For a facility that has not published its first post, schema belongs in the findable-first infrastructure work that comes before the content calendar.
For treatment center cluster builds, four schema types earn their keep.
Organization and MedicalOrganization schema deployed sitewide with a stable @id. This anchors the facility’s entity in Google’s knowledge graph and prevents disambiguation problems when multiple facilities share a name.
Article schema with Person author and Organization publisher on every clinical content piece. The Person author should link to the structured author bio page; the Organization publisher should reference the facility’s stable @id.
FAQPage schema on articles with visible FAQ sections, paired with the visible Q&A markup. The Webserv pattern uses the Rank Math FAQ Block, which renders both the visible content and the JSON-LD in one unit.
BreadcrumbList schema across the cluster, supporting navigational legibility for both Google and AI systems.
What Google’s 2026 guidance explicitly deprioritizes: “AI-specific” schema markup that does not map to standard schema.org types, “chunking” markup designed to help LLMs parse content, and any speculative schema that exists primarily to manipulate AI surface behavior. Operators investing heavily in AI-only schema in 2024 and 2025 sometimes overbuilt this layer. The right 2026 read is to keep the standard schema stack mature and stop there.
The Resource Hub: Guides, Calculators, Glossaries, Outcomes Pages
Beyond the hub-and-spoke blog architecture, mature treatment center sites build a structured resource hub that hosts the non-blog content forms: guides, calculators, glossaries, outcomes pages, family-facing checklists, and downloadable resources.
The resource hub serves three jobs the blog cannot.
The lead magnet job. Downloadable family-facing guides (“What to expect in the first week of residential treatment,” “Insurance verification checklist for families”) earn email captures that turn anonymous research traffic into nurture-cycle inquiries.
The authority anchor job. Outcomes pages with anonymized facility data, glossaries of clinical terms with named clinician contributions, and structured guides serve as the canonical references that earned media, healthcare journalists, and AI systems cite when describing the facility. The content gap analysis diagnostic surfaces which resource gaps to close first.
The conversion bridge job. Resource pages convert at materially higher rates than blog posts because they reach the visitor at a more decision-ready point in the consideration window. The family member who downloads the insurance verification checklist is closer to the inquiry call than the family member reading a generic blog explainer.
The resource hub URL structure should mirror the blog architecture: /resources/[category]/[name]/, with cross-linking between the blog spokes and the resources that serve adjacent jobs.
Most treatment center sites build the resource hub last in the 90-day reorganization sequence, after the hub-and-spoke blog architecture and author infrastructure are mature. The resource hub layered on top of weak architecture underperforms. Layered on top of mature architecture, it compounds.
The Calendar and Editorial Cadence
Steady-state editorial cadence for a mature treatment center library runs 4 to 6 articles per month. The cadence is anchored in the named clinical author capacity rather than in keyword volume.
Each article requires meaningful clinician time: 2 to 4 hours for the clinician contributor, plus the editorial team’s writing, fact-checking, schema deployment, internal linking, and publication work. The cadence is rate-limited by clinician availability, not by content team capacity.
Operators trying to run 8 to 12 articles per month with the same clinician roster either skip the clinician input (producing the “Editorial Team” commodity library the protocol is built to prevent) or burn out the clinicians who are supposed to be the load-bearing E-E-A-T signal.
The 4-to-6 cadence works because it sustains the non-commodity standard across every piece. Some months produce 4 deep clinician pieces; some months produce 6 mid-depth pieces. The variance is normal.
What does not work is the calendar-driven cadence that publishes a post every Tuesday regardless of whether the team has something non-commodity to say. That pattern produces the drift that the architecture work is designed to fix.
The right read on cadence is: publish when the team has earned the post, not when the calendar says to publish. The editorial team owns the cadence. The clinician availability sets the ceiling.
Common Architecture Failure Modes
The pattern across treatment center blog audits we run is consistent. Four failure modes account for most of the architecture drag we see.
The chronological /blog/ feed with no hub pages. The WordPress default architecture: posts published into a flat reverse-chronological feed, organized only by date and a few broad categories. The architecture has no spine. Posts compete with each other for ranking signals instead of compounding.
The “Editorial Team” byline on YMYL content. Generic byline on clinical content. No named clinician, no reviewer credit, no structured author bio page. The architecture is at the foundation gap that no other layer can compensate for.
The volume-without-depth library. 200+ thin posts targeting keyword variations, each under 1,000 words, with no clear hub or non-commodity perspective. Google’s 2025-2026 systems categorize this pattern as scaled content abuse and apply ranking drag to the entire domain, not just the offending posts.
The orphan-post problem. Posts that have no inbound internal links from other published content, no outbound links to hubs or related spokes, and no breadcrumb path from the homepage. These posts exist as architectural dead ends. They consume crawl budget and contribute nothing to topical authority.
WHAT NON-COMMODITY SPOKES LOOK LIKE
- Clinician-authored spoke with first-hand clinical perspective
- Family-member-perspective spoke with situation-specific framing
- Operational-reality spoke that takes a defensible position
- Spoke that ties to a named clinician’s authored body of work
- Spoke that exists because the team has something distinctive to say
WHAT COMMODITY SPOKES LOOK LIKE
- “What is dual diagnosis” explainer any AI could write
- “How to talk to a loved one about addiction” generic primer
- “Does insurance cover rehab” copy-paste piece
- “Editorial Team” bylined article with no named author
- Spoke built primarily to capture a keyword variation
Most facilities have 2 to 3 of these failure modes in their current architecture. The 90-day reorganization sequence is built to surface and close them in priority order.
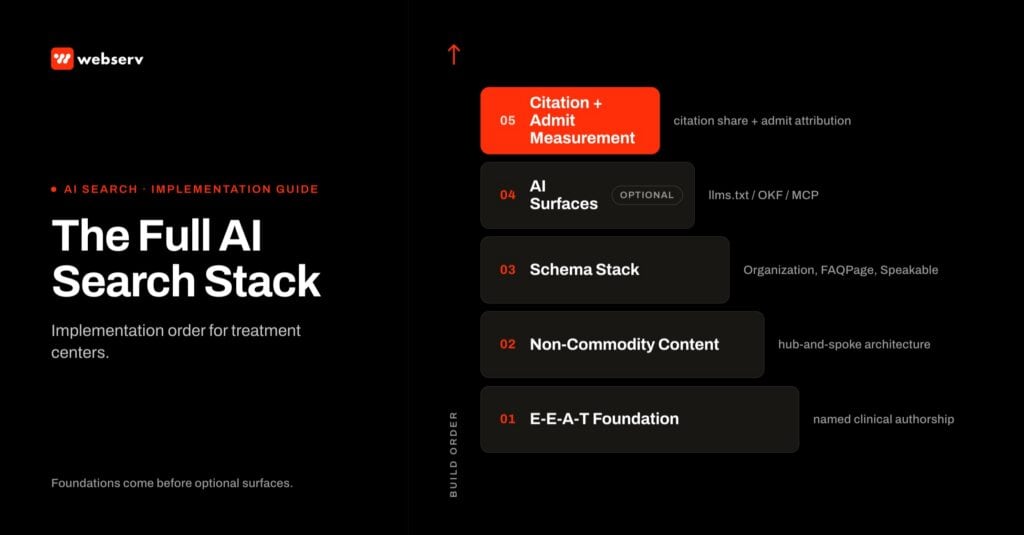
The 90-Day Reorganization Sequence
The reorganization that produces durable lift has three phases operating on a 90-day cadence. The phases are sequential. Phase 2 spokes do not work without Phase 1 hubs. Phase 3 measurement does not work without Phase 1 and Phase 2 in place.
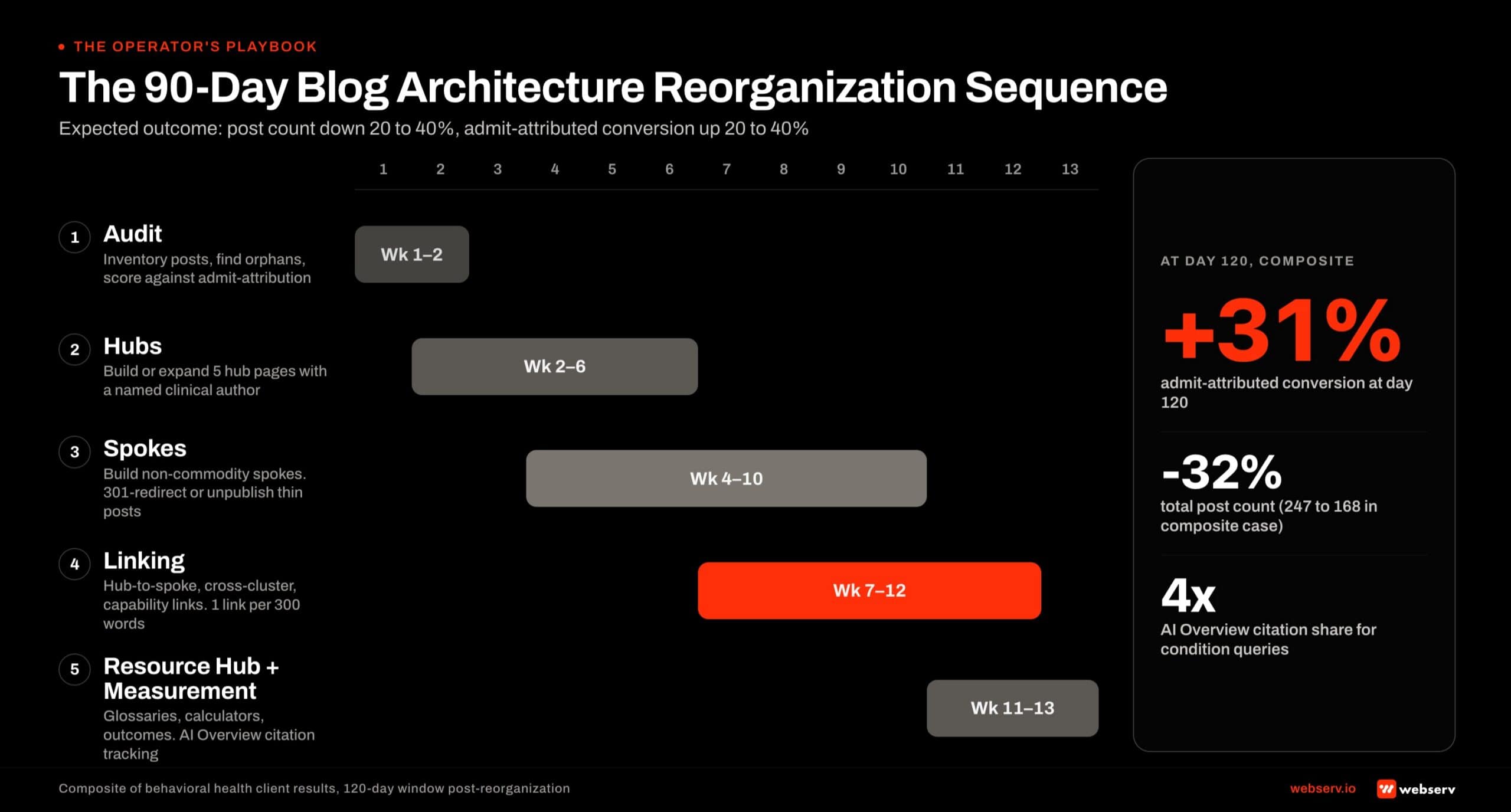
Days 1-30 · Audit + Hubs
Map the current library against the 5 hub categories. Identify thin/orphaned posts for 301 redirect. Build or rebuild the hub pages first; spokes wait for the hubs to anchor.
Days 31-60 · Spokes + Linking
Refresh or build the spokes that have non-commodity perspective. Wire the internal linking density: hub-to-spoke, spoke-to-hub, cross-cluster. Drop scaled-keyword spokes that lack distinctive perspective.
Days 61-90 · Resource Hub + Measurement
Stand up the family-facing resource hub. Deploy schema across the cluster. Establish the citation share + admit attribution measurement infrastructure that confirms the work compounded.
The audit in Days 1-30 is where most reorganizations either succeed or fail. The audit needs to surface the genuine gaps (under-built hub categories, orphaned posts, missing clinical authorship, broken internal linking) rather than just produce a list of articles ranked by traffic.
The hub build in the same window establishes the cluster anchors. Hubs go first because spokes need hubs to link to. Trying to build spokes against placeholder or thin hubs produces architecture that does not compound.
The Days 31-60 spoke phase is where the editorial discipline matters most. The team is producing or refreshing 8 to 20 spokes against the new hub architecture, while simultaneously 301-redirecting thin orphan posts and wiring the linking density. The temptation is to keep weak spokes alive “just in case.” The discipline is to redirect them and trust the architecture.
The Days 61-90 measurement phase is the one operators most often skip. Standing up the citation share baseline + admit attribution measurement is what confirms whether the reorganization produced lift, and at what point in the funnel.
Without the measurement layer, the architecture work cannot be defended at the C-suite level when the cost question comes up. The deeper read on attribution timing lives in how long SEO takes to work for a rehab website.
Frequently Asked Questions
Should we delete old blog posts that are not performing?
Yes, but with structured 301 redirects, not bulk deletion. Thin or orphaned posts that have no inbound traffic, no internal links pointing to them, and no non-commodity perspective should be 301-redirected to the most relevant hub page in the new architecture, then unpublished. Deleting them without a redirect throws away whatever residual link equity they hold.
The audit pattern: pull every post with under 50 monthly organic sessions, no inbound internal links from other published posts, and no distinctive clinical perspective. That set is typically 20-40 percent of a treatment center library that was built on volume rather than depth. Each gets a 301 to the closest hub. The hub absorbs the equity. The library gets shorter and stronger at the same time.
What does not work: deleting posts without redirects (creates 404s), redirecting everything to the homepage (Google treats that as soft-404), or keeping thin posts because “they might rank someday.” The right action is the disciplined audit + 301 sweep, run once per quarter as the library matures.
How do we know which hub categories to build first?
Build condition pillars first if the facility’s primary positioning is clinical (alcohol use disorder, opioid use disorder, anxiety, depression, trauma). Build level-of-care pages first if the facility competes primarily on care intensity (detox, residential, PHP, IOP). Build the family-facing resource hub first if the facility serves family-member-initiated admits (most BH operators do, but few build for it).
The diagnostic: pull the last 90 days of inquiry sources. If the majority of admissions came from family members researching for a loved one, the family-facing hub is the highest-impact build. If most came from patients searching their own condition, the condition pillars are the highest use. Modality clusters and geographic hubs tend to be Phase 2 builds rather than Phase 1.
The 90-day sequence we run starts with whichever of the five hub categories is most under-built relative to the facility’s actual admit-driving inquiry mix. The audit reveals the gap. The build closes it.
How does this approach work with AI search and ChatGPT citations?
The same hub-and-spoke architecture that ranks well in classic organic search is the architecture that earns AI Overview and ChatGPT citation share. Google’s June 2026 official guidance is explicit: AI search systems pull candidate sources from the same Search index that ranks blue-link results, using the same core ranking systems. The unified architecture serves both.
What changes specifically for AI search is the value of depth and named authorship. AI systems weight named clinical authorship, peer-reviewed citations, and irreducible first-hand perspective heavily when selecting which sources to cite. The non-commodity content rule is even more load-bearing for AI citation than it is for classic organic ranking.
What does NOT separately help AI search: llms.txt files (Google explicitly says these are not used for ranking), AI-specific schema markup (Google deprioritizes speculative AI-only schema), or content rewritten specifically “for AI” rather than for human readers. The architecture that serves the human reader is the architecture that earns the citation.
How long does this architecture take to produce measurable results?
First ranking lift typically lands at 6 to 9 months as the rebuilt hubs accumulate authority signals. Cluster-wide ranking lift compounds at 9 to 12 months. Admit-attributed conversion lift lands at 12 to 18 months as the funnel catches up to the architecture work and the citation share matures across AI surfaces.
The 90-day reorganization itself produces some immediate signal: traffic typically holds flat (the redirects preserve equity), but the conversion rate from organic traffic improves measurably as the architecture starts driving admit-relevant traffic to the hubs that convert rather than thin posts that don’t. We typically see 20-40 percent admit-attributed conversion lift in the first 120 days post-reorganization.
Operators expecting faster results are typically being misled. The architecture work is durable but the timeline is not compressible. The compounding effect is what makes the investment worth it.
Should we hire a content marketing agency to do this work?
Sometimes, but check the agency’s E-E-A-T pattern first. The architecture work requires named clinical author integration, peer-reviewed citation discipline, and the editorial judgment to skip scaled-keyword spokes that would drag the cluster down. Most generalist content marketing agencies cannot do this without operator-side clinical input.
The agency model works best when the agency owns the architecture, internal linking, schema, and editorial workflow while the operator provides the clinical author roster, reviewer credit, and operational-reality perspective. The hybrid model is the most common pattern that produces results in 2026.
What to avoid: an agency that promises 8+ articles a month without naming the clinical authors who will appear on the bylines. That pattern produces the 184-post commodity library that the protocol is built to fix, not avoid. The right agency engagement is structured around fewer, deeper, named-author pieces and the architecture that connects them.
What about llms.txt files and AI-specific markup?
Google’s June 2026 official position is that llms.txt is not used by Google Search for ranking. The exact quote from the published guidance: "Doing so won’t harm (nor help) your visibility or rankings in Google Search." Operators investing in llms.txt should size the investment to non-Google AI surfaces (ChatGPT, Claude, Perplexity, emerging agents) rather than expect Google ranking lift.
The same logic applies to AI-specific schema markup, the "chunking" content patterns that emerged in early 2025, and content rewritten specifically "for AI". Google’s systems either ignore these patterns or actively deprioritize them under the scaled content abuse policy. The architecture that serves the human reader is the architecture that earns both rankings and AI citations.
The right read on AI infrastructure investments (Open Knowledge Format, MCP servers, AI Information pages) is asymmetric: the cost is bounded, the upside compounds if AI search behaviors evolve as projected, and the downside is small if they don’t. Worth shipping for the non-Google AI surface, but not load-bearing for Google ranking.
Build the Architecture That Compounds, Not the Calendar That Drifts
The treatment center libraries producing durable admit-attributed conversion in 2026 are the ones organized around the five-hub architecture with non-commodity content, named clinical authorship, and the relational layer of internal linking that ties the cluster together.
The treatment center libraries losing ground to AI search are the ones still operating on the 2020-2023 playbook: chronological /blog/ feed, “Editorial Team” bylines, volume-without-depth spokes, and the assumption that AEO is a separate optimization surface from SEO. Per Google’s own June 2026 guidance, it is not. The architecture is unified.
The 90-day reorganization is the work that gets a treatment center library from one pattern to the other. The full BH marketing context sits inside the ultimate guide to behavioral health marketing, and this architecture layer is what makes every other layer in the program compound.
If your facility is evaluating where the current architecture stands or wants to plan the reorganization, book an intro meeting with the Webserv team. We will run the audit against the five-hub framework and lay out the sequence that fits your library and clinical capacity.
Trevor Gage is the Director of Marketing at Webserv. Webserv works with behavioral health and addiction treatment centers on SEO, paid media, and full-funnel admissions strategy.