The conversation I have most often with operators opening a new treatment center starts the same way. The facility is licensed, the team is hired, the clinical program is built, and they want to start marketing immediately. The instinct is right. The timing is wrong.
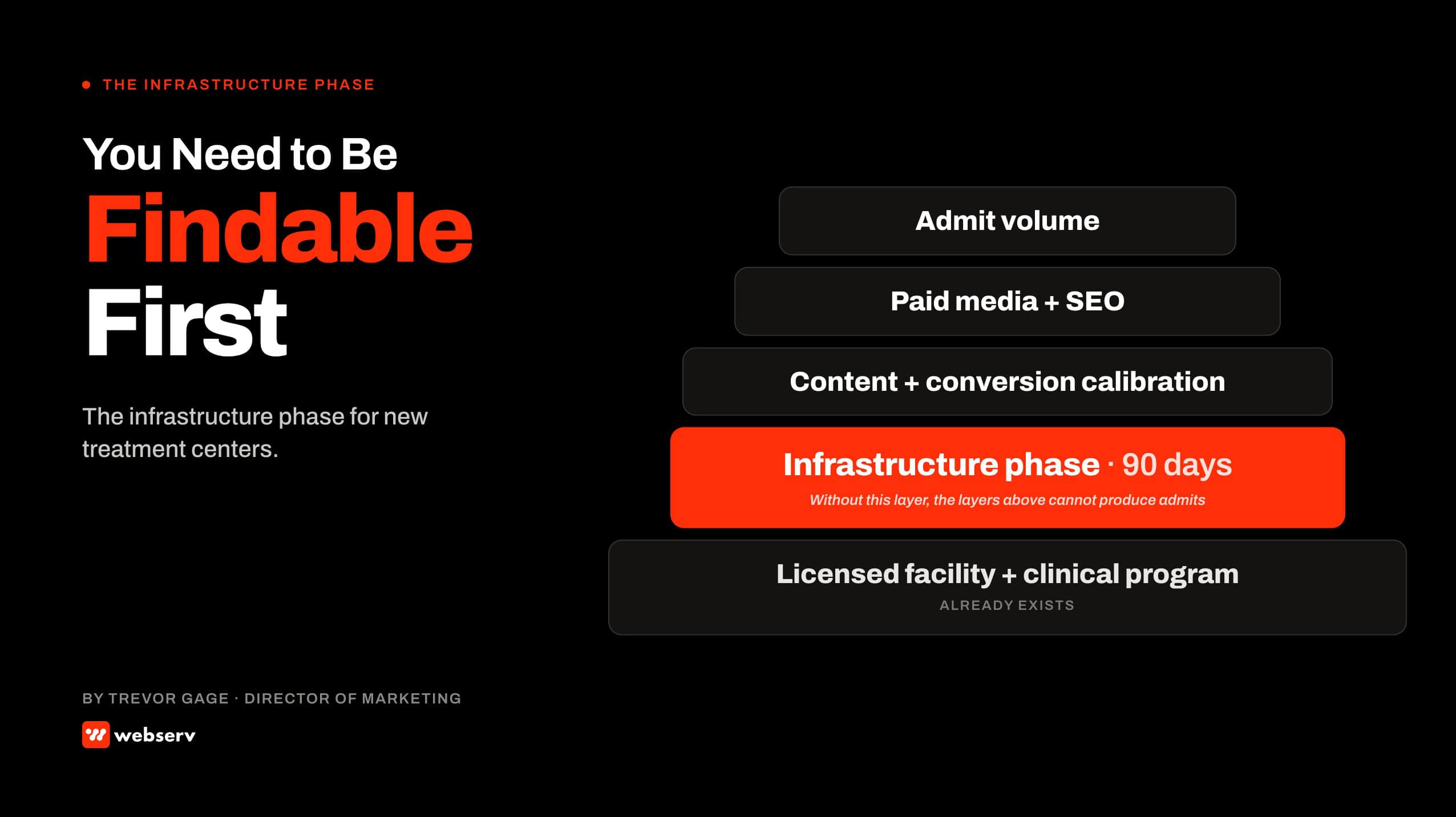
Marketing has nothing to attach to until the infrastructure underneath it exists. A paid search campaign cannot send people to a site that has not been built.
A content strategy cannot rank pages that do not exist. A conversion report cannot trace admits through a CRM that has not been configured. The foundation phase has to come first, and it has to be sequenced correctly, or the marketing dollars that follow it will not produce admits. Our capability stack is built around this sequence because it is the only one that produces a marketing program that compounds.
This article walks the 90-day build plan we run for operators launching a new treatment center or a new program line. It is written for the operator hearing “you need a website first” without a clear answer about what that actually means, what it costs, and what comes next.
We built this sequence across behavioral health marketing engagements for treatment centers from greenfield to first-year operation.
What “Findable” Actually Means
Key Takeaways
- The foundation phase is roughly 90 days. The deliverables are an indexable website, schema-correct structured data, a configured CRM with admit attribution, call tracking wired through to the CRM, a Google Business Profile, and a submitted LegitScript application. None of these are optional if paid media is in the future.
- The most common mistake new operators make is starting paid media before the foundation is in place. The campaigns produce traffic the site cannot convert, leads the CRM cannot trace, and reports that cannot tie marketing spend to admits.
- The right number of pages at launch is 10 to 15, not 100. Topical depth in the categories the operator actually serves beats volume across topics the operator does not. Content production at scale begins after the foundation is stable, not before.
- LegitScript certification has a 30 to 60 day application window. The application should start in week 1 of the foundation phase, not the day you plan to run paid media. Without active certification, Google and Meta will not let your campaigns serve on addiction treatment terms.
- The 90-day foundation costs real money before any admits come in. Operators who skip steps to save money in the foundation phase usually spend two or three times the savings on cleanup in the next 12 months. The shortcuts cost more than the work.
60-90 days
typical foundation phase from kickoff to launch-ready
30-60 days
LegitScript certification application window, runs in parallel
10-15
foundational pages at launch, not 100
DEFINITION
Infrastructure Phase
The 60 to 90 day period during which a new treatment center builds the website, schema, CRM, call tracking, ad accounts, and certifications required before any paid or organic marketing program can produce admit-attributable signal. The phase exists because marketing has nothing to attach to until the operational infrastructure underneath it is live.
“Findable” is more specific than “having a website.” A treatment center is findable when six things are in place at the same time.
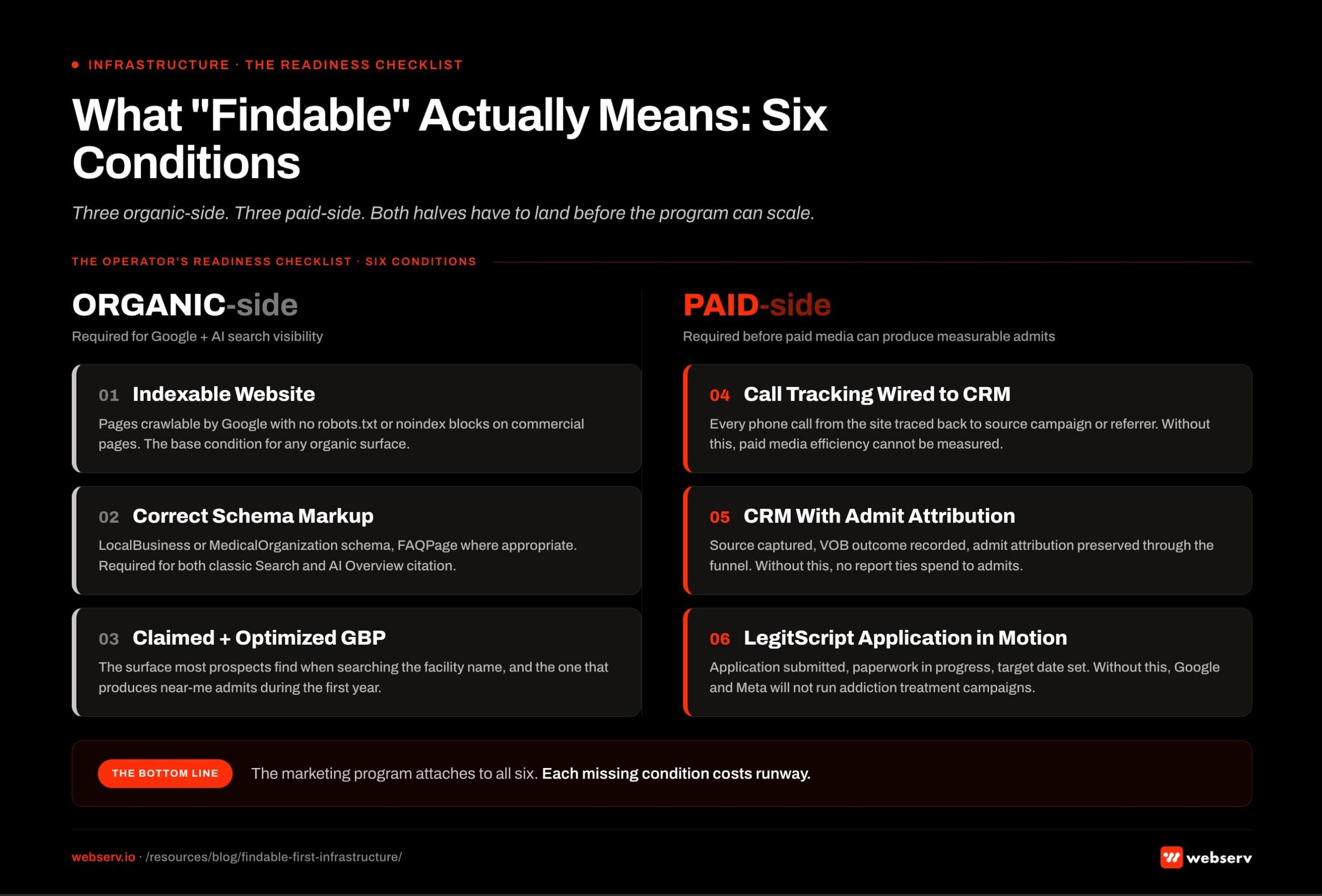 The six conditions that make a treatment center findable. Three organic-side conditions required for Google and AI search visibility: an indexable website with pages crawlable by Google and no robots.txt or noindex blocks on commercial pages; correct schema markup including LocalBusiness or MedicalOrganization schema and FAQPage where appropriate; a claimed and optimized Google Business Profile, which is the surface most prospects find when searching the facility name. Three paid-side conditions required before paid media can produce measurable admits: call tracking wired to the CRM so every phone call traces to source campaign; a configured CRM with source captured, VOB outcome recorded, and admit attribution preserved through the funnel; LegitScript application in motion with paperwork in progress, because Google and Meta will not run addiction treatment campaigns without it.
The six conditions that make a treatment center findable. Three organic-side conditions required for Google and AI search visibility: an indexable website with pages crawlable by Google and no robots.txt or noindex blocks on commercial pages; correct schema markup including LocalBusiness or MedicalOrganization schema and FAQPage where appropriate; a claimed and optimized Google Business Profile, which is the surface most prospects find when searching the facility name. Three paid-side conditions required before paid media can produce measurable admits: call tracking wired to the CRM so every phone call traces to source campaign; a configured CRM with source captured, VOB outcome recorded, and admit attribution preserved through the funnel; LegitScript application in motion with paperwork in progress, because Google and Meta will not run addiction treatment campaigns without it.The six conditions:
- An indexable website. Pages crawlable by Google, with no robots.txt or noindex blocks on the commercial pages. Google Search Central has documented the indexing requirements in detail in its “How Search Works” guide.
- Correct schema markup. LocalBusiness or MedicalOrganization schema, FAQPage where appropriate, and proper structured data identifying the facility as a healthcare provider. The schema vocabulary for medical organizations is documented at Schema.org, and Google has its own implementation guidance for local healthcare entities.
- A claimed and optimized Google Business Profile. GBP is the surface most prospects find when they search the facility name. It is also the surface that produces “near me” admits during the first year.
- Call tracking wired to the CRM. Every phone call from the site is tracked back to its source campaign or referrer. Without this, paid media efficiency cannot be measured.
- A configured CRM with admit attribution. The CRM has source captured, VOB outcome recorded, and admit attribution preserved through the funnel. Without this, no marketing report can tie spend to admits.
- LegitScript application in motion. Application submitted, paperwork in progress, target date for active certification set. Without this, Google and Meta will not run addiction treatment campaigns.
Three of the six (website, schema, GBP) are organic-side. Three (call tracking, CRM, LegitScript) are required before paid media can produce measurable admits. Both halves have to land before the program can scale.
The Sticker Shock Conversation
THE FOUNDATION PHASE COSTS REAL MONEY BEFORE ANY ADMITS COME IN
A serious foundation phase for a new treatment center typically runs $30,000 to $80,000 across the website build, schema implementation, CRM configuration, call tracking setup, GBP optimization, and the certifications and integrations required for marketing to work. Operators who try to compress this into $5,000 to $10,000 spend two to three times the savings on cleanup in the next 12 months. The shortcuts cost more than the work.
The foundation cost is not arbitrary. Each line item connects to a specific marketing function downstream. The site has to be production-quality because every paid click and every organic visitor lands on it.
The schema has to be correct because both Google Search and AI assistants now parse structured data to surface the facility. The CRM has to be configured because every admit attribution traces back through it.
Operators who try to cut corners in the foundation usually do so in one of three ways. They use a templated site that will not convert paid traffic.
They skip the CRM configuration and try to track admits in a spreadsheet. They defer LegitScript on the assumption that “we can apply later when we are ready for paid.”
All three create a downstream problem that costs more to fix than it would have cost to do correctly the first time.
The hardest conversation with a new-facility operator is the one where I explain that the first 90 days of investment produces no admits directly. The admits come from months 4 through 12, on the back of the infrastructure built in months 1 through 3. Operators who understand that pattern fund the foundation. Operators who do not usually run into a wall in month 6.
Trevor Gage, Director of Marketing, Webserv
The 90-Day Build Sequence
- Days 1-14: Foundation Setup. Domain registered or transferred, hosting selected, brand identity finalized at minimum-viable level, GBP application submitted, LegitScript application submitted, ad accounts created under client ownership, CRM provider selected.
- Days 15-30: Architecture and Strategy. Site architecture and page templates finalized. Schema strategy mapped (LocalBusiness or MedicalOrganization, FAQPage, BreadcrumbList). Content outlines for the 10-15 foundational pages drafted. CRM configuration plan locked. Call tracking provider selected.
- Days 31-60: Build. Site built and populated with the foundational pages. Schema implemented and validated. Call tracking integrated and tested. CRM configured with source capture, VOB tracking, and admit attribution. GBP populated with photos, hours, services, and accurate NAP.
- Days 61-75: Launch and Validate. Site goes live. Submitted to Google Search Console. Conversion tracking validated end-to-end. Call tracking validated by making test calls through to admit attribution. Initial backlinks acquired through directories and legitimate citations (not link building at scale).
- Days 76-90: Optimize and Hand Off. Indexing confirmed across all foundational pages. GBP optimized through the first 30 days of real data. Initial content additions scoped for months 4-12. Paid media calibration begins if LegitScript is now active; otherwise queued until certification lands.
The sequence is sequential, not parallel. Step 1 has to land before step 2 because the LegitScript application takes 30 to 60 days and has to start at the front of the timeline to be active by the end.
The CRM and ad account ownership has to be settled at the same time because retroactive transfers create attribution gaps.
Step 2 builds the strategic foundation that step 3 executes against. Skipping step 2 (architecture and schema strategy) produces a built site that has to be partially rebuilt three months later. The architecture decisions are cheaper to make on paper than to refactor in production.
Steps 3 through 5 are the visible work. The website, the CRM, the GBP, the validation. Most operators only see this part of the foundation. The first two steps are usually invisible to anyone outside the engineering and strategy team but determine whether the visible work compounds.
What Goes on the Foundational Pages
PAGES, NOT CONTENT VOLUME
The right number of pages at launch is 10 to 15. The instinct to publish 100 articles at launch is wrong. Topical depth in the categories the operator actually serves (specific levels of care, specific modalities, specific clinical conditions) beats volume across topics the operator does not. Content production at scale begins after the foundation is stable, not before.
The foundational page set for a new treatment center typically includes:
- Home page. Positions the facility, names the levels of care offered, surfaces clinical leadership, and routes visitors to verification or contact.
- About / clinical leadership. Names the clinical director, medical director, and key clinical staff with verifiable credentials. YMYL E-E-A-T expectations require named, credentialed authorship of clinical claims.
- Levels of care pages. Separate pages for each level the facility offers (detox, residential, PHP, IOP, OP, sober living). One page each, not a single combined page.
- Insurance and verification page. Lists accepted payers, explains in-network and out-of-network handling, and routes prospects to verification of benefits.
- Locations and contact page. Physical address, hours, phone, and a routing path to the intake conversation (Webserv standard is to use /intro-meeting/ or similar booked-call patterns, not a generic contact form).
- Three to five foundational clinical topic pages. The conditions the facility treats most often, written with named clinical authorship and proper schema. These are the pages organic search will eventually surface.
- Resources hub. A landing page for the blog and resource library, even if only seeded with two or three articles at launch. The architecture matters more than the volume.
- Privacy and compliance pages. Privacy policy, HIPAA notice of privacy practices, and 42 CFR Part 2 disclosure where applicable. Required by law and required by Meta and Google to run paid media.
These 10 to 15 pages are what the marketing program attaches to. They are also what AI assistants will read when the facility is referenced in search results. The accuracy, completeness, and structured-data quality of these pages determines how the facility gets surfaced for the next 12 to 24 months.
How to Sequence Paid Media into the Build
WORKING PAID MEDIA SEQUENCING IN A NEW BUILD
- Submit LegitScript application in week 1 of foundation phase
- Wait until conversion tracking is validated end-to-end before any spend
- Calibrate paid search against site convert-ability after foundation launches
- Use the first 30 days of post-launch paid spend as calibration, not scale
- Coordinate paid creative with the site’s conversion pages, not in isolation
BROKEN PAID MEDIA SEQUENCING IN A NEW BUILD
- Defer LegitScript application until ‘ready for paid’ in month 4
- Launch paid search with conversion tracking still being wired
- Run paid against a site that has not yet been tested for conversion
- Scale paid to full budget in the first 30 days of post-launch
- Build paid creative separately from the landing page experience
The temptation to start paid media before the foundation is complete is the most expensive mistake in the foundation phase. The math is clear about why.
The right sequencing protects the foundation. Paid traffic landing on a partially-built site burns budget on prospects who do not convert.
Conversion tracking validated after the spend has started cannot reconstruct the missed attribution from the first weeks. LegitScript applied in month 4 means the operator has paid for three months of staff and overhead without any paid media coverage during that window.
The operators who do this well treat paid media as the activation phase, not the foundation phase. The site, the schema, the CRM, the call tracking, the GBP, and the certification all land first. Paid media starts after, against a calibrated foundation that can convert the traffic it receives.
What Comes After the Foundation
The 90-day foundation is not the marketing program. It is what the marketing program is built on. The work that produces compounding growth lands in months 4 through 12.
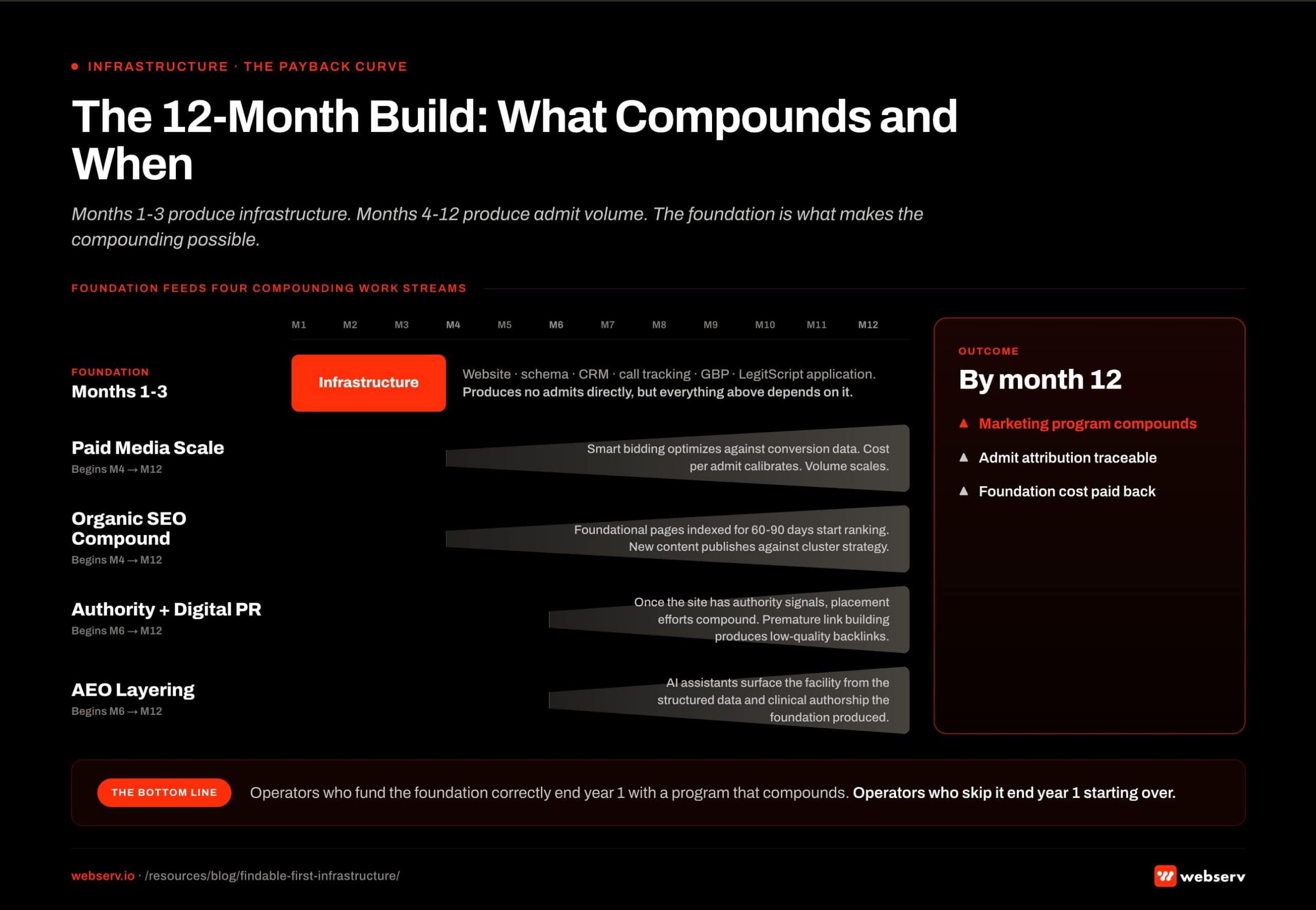 The 12-month build timeline for new treatment centers. The infrastructure phase runs months 1 through 3 and produces the website, schema, CRM, call tracking, GBP, and LegitScript application. Four compounding work streams begin afterward. Paid media scale begins in month 4 and scales through month 12 as smart bidding optimizes against conversion data and cost per admit calibrates. Organic SEO compound begins in month 4 and compounds through month 12 as foundational pages indexed for 60 to 90 days start ranking. Authority and digital PR begins in month 6 and compounds through month 12 after the site has enough authority signals for placement efforts to land. AEO layering begins in month 6 as AI assistants surface the facility based on the structured data and clinical authorship the foundation produced.
The 12-month build timeline for new treatment centers. The infrastructure phase runs months 1 through 3 and produces the website, schema, CRM, call tracking, GBP, and LegitScript application. Four compounding work streams begin afterward. Paid media scale begins in month 4 and scales through month 12 as smart bidding optimizes against conversion data and cost per admit calibrates. Organic SEO compound begins in month 4 and compounds through month 12 as foundational pages indexed for 60 to 90 days start ranking. Authority and digital PR begins in month 6 and compounds through month 12 after the site has enough authority signals for placement efforts to land. AEO layering begins in month 6 as AI assistants surface the facility based on the structured data and clinical authorship the foundation produced.Organic SEO begins compounding once the foundational pages have been indexed for 60 to 90 days and additional content starts publishing against the operator’s actual cluster strategy. The organic SEO program for treatment centers uses the 10 to 15 foundational pages as the spine that 50 to 100 supporting articles attach to over the first year.
Paid media scales once the foundation has been calibrated and the conversion tracking has produced enough data for smart bidding to optimize against. Months 4 through 6 are typically the paid scale window, after the foundation has been live for 90 days and the first conversion data has accumulated.
Authority content and digital PR begins in months 6 through 12, after the site has enough authority signals to make placement efforts compound. Trying to build backlinks at scale into a 90-day-old site usually produces low-quality links that have to be disavowed later.
AI search optimization (AEO) layers in once the site has been crawled and indexed long enough for AI assistants to surface the facility in their training and retrieval. The foundation phase produces the structured data and clinical authorship that AI assistants need to cite the facility accurately.
The compounding pattern is what makes the foundation phase worth funding. Months 1 through 3 produce infrastructure. Months 4 through 12 produce admit volume.
The operators who fund the foundation correctly end year 1 with a marketing program that compounds. The operators who skip the foundation end year 1 starting over. Book an intro meeting if you want to walk your foundation plan with us live.
Frequently Asked Questions
How long should a new treatment center expect to wait before marketing produces admits?
The honest timeline is three to four months from kickoff to the first admit attributable to marketing. The foundation phase runs 90 days. Paid media calibration adds another 30 to 60 days after foundation launch. Organic admits typically land in months 6 through 9.
Operators who run paid media starting at month 4 with LegitScript active and the foundation in place can see admit volume in months 4 through 6. The earlier paid timing requires the foundation to be ready earlier.
Operators who try to compress this timeline by skipping foundation steps usually delay rather than accelerate the first admit. The compressed version of the timeline costs more and produces less.
What does a serious foundation phase actually cost?
A serious foundation phase for a new treatment center typically runs $30,000 to $80,000 across all line items: website design and build, schema implementation, CRM configuration, call tracking setup, GBP optimization, content for the foundational pages, and the integrations required for paid media.
Operators who try to do this for $5,000 to $10,000 typically end up with a templated site that does not convert paid traffic, a CRM that does not track source attribution, and a foundation that has to be partially rebuilt within 12 months.
The investment is real and is paid back across months 4 through 24 as the foundation produces compounding organic, paid, and AEO admit volume. The math works if the operator can fund the foundation without compromising the clinical program.
Can we run a small amount of paid media during the foundation phase?
Generally no. Paid media during the foundation phase usually produces wasted spend because the conversion tracking is not yet validated, the LegitScript certification is not yet active, and the site that the traffic lands on is not yet finished.
There is one exception: branded paid search (the operator’s own facility name and trademark terms) can run earlier because the conversion paths are simpler and the search intent is captive. Even this is usually deferred until at least the call tracking and CRM are live so that the resulting calls can be attributed.
Non-branded paid search, paid social, display, and YouTube should all wait until the foundation phase is complete and LegitScript is active.
Do we need a CRM if our admissions team is small?
Yes, even if the admissions team is one person. The CRM is not primarily for the admissions team’s workflow. It is the source-of-truth for admit attribution. Without it, no marketing report can connect a paid search click to an admitted patient.
The CRM does not have to be expensive or complicated. Webserv has worked with treatment centers using everything from KIPU and Sunwave to Dazos to lightweight HIPAA-compliant CRMs. The requirement is that source capture, VOB outcome, and admit attribution all live in the same system.
A treatment center launching without a CRM is making a decision that costs 12 months of marketing efficiency to undo. The right CRM at the start is usually cheaper over the first 24 months than skipping it and patching the attribution gap later.
Trevor Gage is the Director of Marketing at Webserv, a digital marketing agency for treatment centers.