An owner called us in February. A major national payor had opened an audit on the facility in late fall. Reimbursement had been falling for two months when the audit was discovered in the new year. As of the call, six months later, the audit was still open.
Ninety percent of the facility’s census was tied to that payor. The day-rates the operating model had been built on were no longer arriving on the standard payment cycle. Payroll was the same. Lease was the same. Clinical staffing was the same.
The owner’s question was direct: do we pause marketing until this is resolved?
The answer is more nuanced than the panic of the moment suggests. Pausing everything is not a conservative decision. It is a second bet against your own census, layered on top of the bet that is already going against you.
What follows is the marketing playbook for treatment center operators going through a payor audit or any other out-of-network reimbursement compression event.
It is grounded in what we have watched dozens of facilities do, what worked, and what made the post-audit recovery harder than it had to be.
The piece is about marketing decisions only. The audit itself is for your billing counsel and revenue cycle team.
Key Takeaways
- Out-of-network reimbursement can change overnight. Payors can adjust rates, open audits, and slow claims with no contract protecting the facility, which means treatment centers operating largely or fully OON are exposed to revenue shocks that have nothing to do with marketing performance.
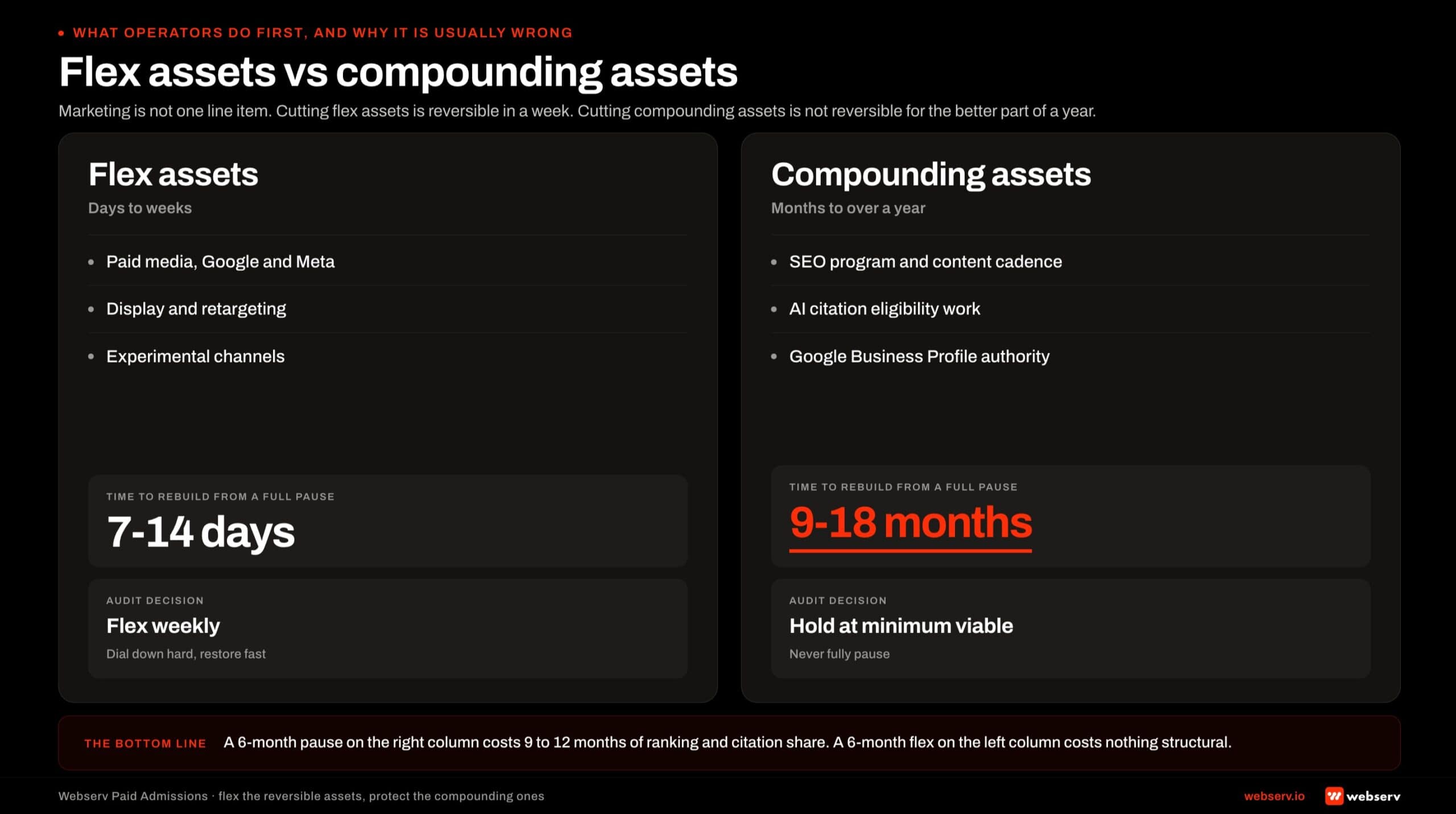
- Pausing all marketing during a payor audit is not the conservative call it looks like. Paid media can flex weekly. Organic search, AI citations, and Google Business Profile authority cannot. Going dark on the slow assets during a 6-month audit puts the facility at a standing start exactly when census recovery matters most.
- Shift targeting before shifting budget. If the audited payor was 80 to 90 percent of census, the underlying issue is payor concentration, not lead volume. Insurance-specific campaigns and carve-out keywords can rebalance the policy mix faster than cutting spend can save the facility from the squeeze.
- The Blue Card trap is the OON economics surprise most operators discover during an audit, not before. Out-of-state Blue Cross Blue Shield members get reprocessed through the in-state Blue plan, which routes the facility’s OON rate down to the in-state in-network rate. Modeling the policy mix with this in view prevents the worst surprise.
- The re-entry plan matters more than the pause. What week one looks like after the audit closes should be decided before the pause begins, because the cost of the pause is determined by how quickly the facility can re-enter at productive levels.
Why Out-of-Network Reimbursement Can Collapse Overnight
The economics of an out-of-network treatment center are built on a structural fragility most operators understand intellectually and underestimate operationally. Out-of-network reimbursement rates are not contractual.
Payors can adjust them at their discretion. They can open audits without a committed end date. They can slow-pay claims while the audit is open. The facility absorbs the variable cost in real time.
The National Association of Insurance Commissioners has documented the network adequacy standards that govern when in-network coverage applies, but those standards do not protect facilities operating outside the network. State-by-state variation in how OON claims are processed adds another layer of unpredictability.
For an OON treatment center, this is the basic business risk. One policy at a $1,000 day-rate is worth five at $200. The whole business model rests on a payor-set rate that can move against the facility on any given quarter.
Audits do not happen randomly. They tend to cluster around facilities with unusual billing patterns, high day-rates relative to in-state in-network norms, and concentrated payor mix.
The day-pay compression cycles through 2024 and the audit waves through 2025 and 2026 are not new behavior. They are the same payor incentive structure expressed on a different policy cycle.
For operators, the implication is not “diversify everything by Friday.” It is that the marketing system has to be built to absorb these shocks without going to zero, and the playbook for what to do during an audit should already exist before the audit opens.
What a Payor Audit Actually Does to a Treatment Center
A payor audit is rarely a clean process. Claims slow or stop paying. The facility submits documentation. The payor requests more documentation. Six to twelve months pass.
During that window, three things happen at once. First, cash flow tightens. The facility is still admitting patients and still incurring full operating cost, but reimbursement is delayed or partial.
Second, the policy mix often shifts because admissions teams start triaging for cleaner policies, which can drop census volume. Third, marketing performance gets re-evaluated against the new cash reality, which is where the panic decisions usually live.
The instinct is to cut what feels cuttable. Marketing is high on that list because it is a visible monthly line item and because the operator’s intuition says “we have plenty of leads already, we just can’t process them fast enough.”
Both feel true. Both can be misleading inside an audit.
The leads that look high-quality on the dashboard today were generated by marketing spend that was active 30 to 90 days ago. The leads that arrive 30 to 90 days after the audit opens will reflect whatever spend decisions get made this week.
By the time the audit is resolved, the lead-gen curve looks nothing like the dashboard the cut decision was made on.
The Blue Card Trap
One of the most expensive OON economics surprises in behavioral health is the Blue Card mechanism. Blue Cross Blue Shield is a federation, not a single payor. Plans are operated by state-level Blue companies.
When a member of one state’s Blue plan receives treatment in another state, the claim is processed by the in-state Blue plan, not the home-state plan.
For an OON treatment center in California, this means an out-of-state Blue policy that the facility expected to bill at a $1,500-per-day OON rate may end up reimbursed at the in-state in-network rate of roughly $310, depending on the state and the plan.
The Blue Card program routes the claim through the host-state Blue, which applies its own contracted rate.
The KFF analysis of out-of-network billing dynamics covers the policy and consumer-protection side. The Blue Card piece is a separate operational mechanism that has been routing claims this way for decades.
Most operators discover the Blue Card economics only after a payor audit forces them to reconstruct the policy mix in detail. The audit becomes the moment the facility learns it has been overestimating revenue per admit by 30 to 60 percent on out-of-state Blue policies.
Building this into the policy-mix model before the audit is the only way to avoid the surprise.
The fix is to know which states route Blue policies this way (at least ten do, with variation by plan), and to model the expected reimbursement against host-state in-network rates rather than home-state OON rates.
What Operators Do First (And Why It’s Usually Wrong)
MOST COSTLY REACTION
The two moves operators make in the first week of an audit that make the situation worse: pausing all paid media, and cutting the private-pay advertising that was funding the census. Both feel prudent. Both accelerate revenue collapse. Paid media pause kills the pipeline that would have replaced audit-flagged claims. Cutting private-pay severs the exact revenue stream the audit is not touching.
The most common first move during a payor audit is to pause all paid media. The second most common is to cancel the SEO and content marketing engagement. The third is to drop the Google Business Profile work and the AI search citation work entirely.
Each of these is understandable. Each is also wrong in a different way.
Paid media is the right asset to flex, but it is rarely the right asset to zero out. Paid media can scale from $80,000 to $20,000 in a week and back up in a week.
The platform learning resets on the dial-down are minor relative to the cash savings.
SEO and content marketing are the wrong assets to cancel. Organic rankings, AI citations, and topical authority compound over 90 to 180 days.
Cancellation in month two of an audit produces a search and AI visibility hole the facility is still climbing out of in month nine, which is exactly when census recovery has to start.
Google Business Profile authority and review velocity are the slowest assets to rebuild. A facility that pauses GBP work for six months loses local-search positioning that took 18 months to earn. Re-earning it takes another 18 months.
The pattern across most facilities is the same. The cuts that feel safest in week one of the audit produce the longest tail of revenue damage. The cuts that feel scarier in week one (flexing paid media down sharply but holding the slow assets steady) produce the cleanest recovery curve.
Pausing everything is not a conservative decision. It is a second bet against your own census, layered on top of the bet that is already going against you. The operators who come out of an audit with the cleanest recovery curve are the ones who flexed paid media and protected the slow assets, not the ones who went dark across the board.
Mitch Marowitz, Director of Paid Media at Webserv
The Marketing-Through-Audit Playbook
Four moves, in this order, with one principle behind all of them: optimize for the re-entry, not for the pause.
Move 1: Flex paid media weekly, do not cancel. Cut the paid media budget by the percentage of cash compression the audit has caused, and then revisit the cut weekly as audit status changes.
A 50 percent cut to paid media reduces the cash burn fast, preserves the campaign learning, and allows a fast scale-back-up when the audit resolves.
This is the asset built for this kind of compression. Google Ads strategy for behavioral health covers the campaign architecture that flexes cleanly.
The campaigns built on Smart Bidding and broad-match foundations recover from spend dial-downs in 7 to 14 days. The campaigns built on rigid manual structures do not.
Move 2: Never zero out the slow assets. Hold the SEO program, the content production cadence, the AI citation work, and the GBP optimization at minimum viable level rather than cutting them. The compounding-asset side of the marketing program should not be the place the cash compression hits.
The math is straightforward. A six-month pause on SEO and AI citation work costs the facility 9 to 12 months of ranking and citation share rebuild after the audit resolves.
The monthly savings during the pause are a small fraction of the revenue cost of the rebuild. Hold the slow assets steady.
Move 3: Shift targeting before shifting budget. If the audited payor was 80 to 90 percent of census, the marketing problem the facility actually has is payor concentration. The fix is insurance-specific campaign work that builds census on policies other than the audited payor.
The exclude-zip strategy for out-of-network family targeting is one example of the targeting shift that rebalances policy mix without raising total spend.
Carve-out keyword campaigns by policy type, landing pages that screen by insurance carrier, and lead-routing rules that prioritize non-audited payors all work in parallel to the spend dial-down. The lead-volume target shifts. The policy-mix target tightens.
Move 4: Design the re-entry plan before the pause. What week one looks like after the audit closes determines whether the pause was strategic or just a delay.
Map the campaign re-activation order, the spend ramp curve, the landing-page asset refresh, the GBP post calendar, and the content production restart sequence before the pause begins.
The re-entry plan is a one-page document with weekly milestones for the first 60 days after audit close. It assumes the facility wants to be at 80 percent of pre-audit lead volume by day 30 and 100 percent by day 60.
The plan exists so that the decision to flex during the audit does not require a separate decision at the end of it.
How to Sequence the Cuts (When You Have to Cut)
Sometimes the cash compression is severe enough that “flex everything down a notch” is not enough. When deeper cuts are required, the sequence matters.
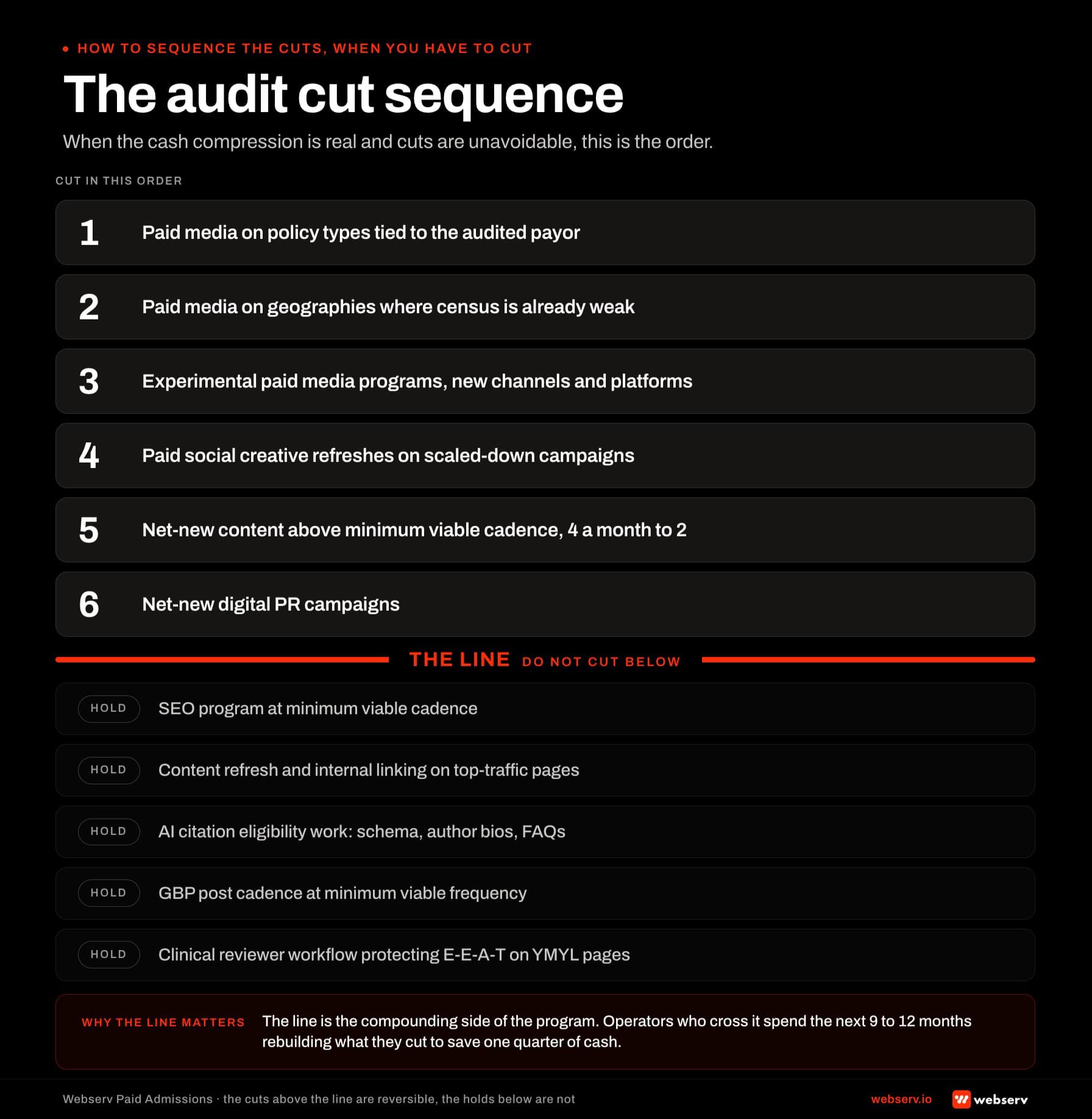
Cut first: paid media spend on the policy types tied to the audited payor. Cut second: paid media spend on geographies where census is already weak. Cut third: experimental paid media programs (new channels, new platforms, new campaign types still in learning).
Cut fourth: paid social ad creative refreshes for the campaigns being scaled down (the 14 paid social strategies for sub-$20K budgets doc is the reference for what to keep at the lower spend tier).
Cut fifth: net-new content production above the minimum-viable cadence (4 pieces per month becomes 2). Cut sixth: net-new digital PR campaigns.
Do not cut: the SEO program at minimum viable cadence. The content refresh and internal-linking optimization work on existing top-traffic pages. The AI citation eligibility work (schema, named author bios, FAQ build-outs).
The GBP post cadence at minimum viable frequency. The clinical reviewer workflow that protects E-E-A-T signal on YMYL pages.
The “do not cut” list is the compounding side of the marketing program. The facility that exits the audit with these assets intact recovers in 90 to 120 days. The facility that exits with them gone takes 270 to 365 days.
Frequently Asked Questions
Should we pause all marketing during a payor audit?
No. Pausing all marketing during a payor audit treats marketing as a single line item, but it is not one. Paid media is the asset built to flex weekly without compounding damage. SEO, content marketing, AI citation work, and Google Business Profile authority are compounding assets that take 9 to 18 months to rebuild from a full pause.
The conservative call is to flex paid media down sharply (often by 30 to 60 percent of pre-audit spend depending on cash compression) and hold the slow assets at minimum viable cadence. The cash savings on the slow-asset side are small relative to the rebuild cost when the audit resolves.
Operators who flex paid media and protect SEO recover census in 90 to 120 days after audit close. Operators who cancel everything take 270 to 365 days to get back to pre-audit volume, which is the difference between a manageable disruption and a structural one.
Why do insurance companies deny rehab claims or open audits on treatment centers?
Audits and denials cluster around facilities with billing patterns that diverge from in-state in-network norms. High day-rates, long lengths of stay, concentrated payor mix, and unusual claim volume all increase audit probability. None of these are inherently improper, but each is a signal that a payor’s utilization review team uses to prioritize audit targets.
The other driver is policy-cycle economics. Payors face their own cost pressure on out-of-network claims, and audits are one mechanism for slowing reimbursement during high-cost quarters. The cycles through 2024, 2025, and 2026 reflect the same payor incentive structure expressed on different quarters of pressure.
For operators, the implication is that audits are not random and are not personal. They are a predictable feature of the OON economics environment, which is why the marketing playbook for going through one should already exist before it opens.
How long do insurance companies pay for rehab once a member is admitted?
Authorized length of stay varies by level of care, clinical presentation, and payor utilization review patterns. Residential treatment authorizations typically run in 7 to 14 day increments with continued-stay reviews, partial hospitalization in 5 to 10 day increments, and intensive outpatient in 30 to 60 day blocks. Most payors review utilization repeatedly rather than authorizing a full episode of care up front.
The marketing implication is that admit count alone does not predict reimbursement. Length-of-stay compression and continued-stay denials can collapse revenue per admit even when admission volume holds steady. Tracking authorized days alongside admit count gives operators a more honest view of the marketing-to-revenue conversion.
Operators planning marketing spend against admit projections without modeling expected authorized days end up overestimating revenue per admit during normal periods and overestimating it by even more during audit windows.
How fast can paid media scale back up after a deep cut?
Seven to 14 days to recover lead volume after a 50 percent dial-down, 14 to 30 days after a full pause. The recovery curve depends on the campaign architecture: Smart Bidding campaigns with broad-match and audience-driven targeting recover faster than rigid manual structures because the platform learning resets are smaller.
The biggest variable is whether the conversion signal stayed clean during the dial-down. If the conversion event was misconfigured or the admissions scoring loop drifted during the pause, the campaign is recovering on a degraded signal and the recovery curve runs longer.
Operators with disciplined offline conversion tracking and clean admissions scoring see paid media volume rebuild inside two weeks of a budget restoration. Operators with broken or stale conversion signals take twice as long for the same restoration.
How long does it take to recover SEO and AI citation share if we cancel during an audit?
Eighteen to 24 months for full SEO recovery from a complete cancellation. Twelve to 18 months for AI citation share recovery. The recovery curve runs this long because organic ranking and AI citation eligibility are compounding signals, and a full pause reverses the compounding rather than just pausing it.
The deeper read on SEO timeline for rehab websites covers the underlying mechanics. The short version is that competitors do not stop publishing during the pause, the content library ages out without refresh, and the named-clinician authorship signal weakens as bylines and review cadence go stale.
Holding the SEO program at minimum viable cadence (typically 2 pieces per month instead of 4 to 6) costs a small fraction of full cadence but preserves the compounding. The math heavily favors holding rather than cancelling.
Plan the Audit Recovery Before the Audit Starts
Payor audits and out-of-network reimbursement compression are structural features of the OON treatment center economy, not surprises. The operators who come out the other side with census intact are the operators who decided what to flex and what to protect before the audit opened, not during it.
The four-move playbook (flex paid media, protect the slow assets, shift targeting before budget, design the re-entry before the pause) is built on a single principle: optimize for the recovery curve, not for the cash savings during the pause.
We work with treatment center operators on the marketing strategy that holds through reimbursement compression and audit cycles. The work includes paid media architecture that flexes cleanly, SEO and AI citation programs that compound through pauses, GBP authority that survives quiet quarters, and the re-entry sequencing that turns a 6-month audit into a 90-day recovery rather than a 12-month rebuild.
The pairing piece on how PMax behaves under spend dial-downs covers one of the specific campaign mechanics that matters most for behavioral health operators flexing paid spend during an audit.
Book an intro meeting to walk through your current marketing program, where the audit-resilience gaps are likely costing you recovery speed, and what the four-move playbook would look like if it were already in place.
For the broader picture of how paid media, SEO, and AI citation work fit inside a full treatment center marketing program, see our ultimate guide to behavioral health marketing.
Preston Powell is the CEO at Webserv, where he leads the team building paid media, SEO, AEO, and digital PR programs for behavioral health and addiction treatment centers across the U.S. He writes about the operating-side decisions treatment center owners and EDs make under reimbursement pressure and the marketing strategy that supports census stability through volatile payor cycles.