If you are running 30 beds at 40 percent occupancy this week, your timeline is not the same as the timeline most marketing articles are written for. You need admits in the next two to four weeks.
SEO does not move that fast. Content does not move that fast. A new website does not move that fast.
Paid media and admissions operations are the two levers that move on this timeline. Everything else is the wrong tool for the problem in front of you. The work below is the operating model we run inside our paid media program for treatment centers when an operator hits the door in active distress.
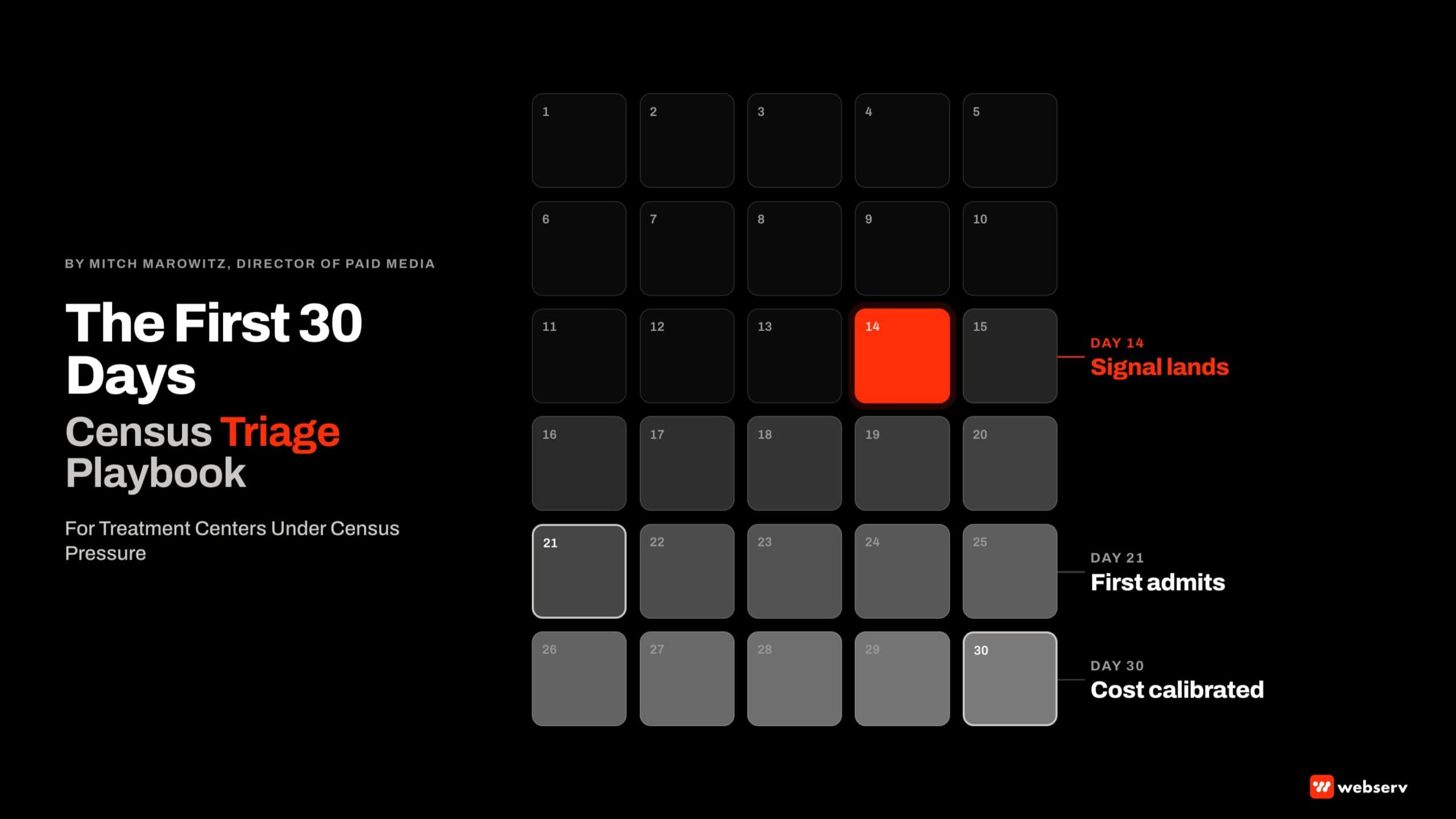
The honest framing matters. We do not promise admits in 30 days. We commit to producing measurable signal inside 14 days, compounding through day 30, and holding discipline on what should not be touched in the first month because it burns runway you do not have.
Key Takeaways
- The only marketing levers that produce admit-side signal in under 30 days are paid search, paid social where the operator is certified, and admissions team performance. Organic SEO, content, and site rebuilds are the wrong tools for census pressure.
- The triage sequence is sequential: admissions audit in days 1 to 3, paid search restart in days 4 to 7, admissions retraining in days 8 to 14, creative and landing page tightening in days 15 to 21, optimization against real data in days 22 to 30.
- The cost per admit will be elevated in week 1 (typically $14,000 to $20,000) and should drop to $10,000 to $13,000 by week 4 as the campaigns calibrate against actual conversion data. Operators who panic at the week-1 number and pull spend never reach the optimization window.
- The single highest-impact non-media fix is the admissions team’s missed-call rate. Most distressed operators are losing 25 to 40 percent of inbound calls before the team picks up. Closing that gap usually produces more admit lift than the first $20,000 of new paid spend.
- Do not launch a new PMAX campaign, build a new website, or switch CRMs in the first 30 days. All three are 60-to-90-day projects that will burn cash and operational bandwidth you need elsewhere.
<50%
occupancy at the triage threshold for most distressed operators
$14-20K
realistic week-1 cost per admit on a restarted paid program
14 days
honest window for measurable funnel signal, not admits
The Reality of Where You Are
Most operators who hit triage timing share four conditions. Bed count is 30 or fewer. Occupancy is below 50 percent. Operating margin has gone negative or close to it in the last quarter. Marketing budget was cut at the start of the slide rather than maintained through it.
The fastest mistake in this situation is treating the marketing problem and the operations problem as one problem. They are not.
DEFINITION
Marketing Triage
The discipline of allocating limited time and budget to the marketing actions that produce admit-side signal within the operator’s runway window. In behavioral health, the triage window is typically 30 days. Inside that window, paid media and admissions ops are the levers that move. Everything else is the wrong tool for the timing.
The marketing problem is that the campaigns are dark, miscalibrated, or starved of budget. The operations problem is that the admissions team is missing calls, slow on VOB, or losing prospects at the closing conversation.
Both have to be addressed in parallel. Fixing marketing without fixing admissions produces more leads that the team cannot convert. Fixing admissions without fixing marketing produces a great closing team with nothing inbound.
The math is unforgiving. Each week of empty beds at $400 to $700 of true daily cost per bed is real money leaving the facility. The pressure is real. The wrong response to real pressure is to fire random tactics and hope. The right response is the triage sequence below.
What Actually Moves in 30 Days
What can move inside 30 days:
- Paid search activation or restart. With LegitScript certification already in place, paid search can produce qualified phone calls and form fills within days. Calibration to a real cost per admit takes 14 to 30 days.
- Paid social where certification permits. Meta and TikTok can produce signal in similar windows, but only with active LegitScript and platform-level certification. If certification is not in place, paid social is a 60-day project, not a 30-day lever.
- Admissions team performance. Missed-call rate, callback time, and VOB turnaround can all be improved in days, not weeks. The lift is often larger than the lift from the same dollars in new media spend.
- Existing landing page optimization. Tightening the highest-traffic landing pages, fixing call-tracking, and ensuring conversion events are firing produces immediate efficiency gains without new spend.
What cannot move inside 30 days:
- Organic SEO. Three to six months minimum before keyword movement translates into admit volume. The wrong tool for census pressure.
- New website build. A treatment center website rebuild is a 60-to-90-day project at minimum. Starting one in week 1 of triage is operational suicide.
- New content production. Content compounds slowly. Useful for the next quarter, not this one.
- CRM migration. Switching CRMs during a census crisis breaks operational continuity exactly when continuity matters most.
- PMAX scaling from a cold start. PMAX needs conversion data to optimize. A cold PMAX campaign will burn budget for the first 14 to 21 days while the learning phase resolves.
The 30-Day Triage Sequence
- Days 1-3: Admissions Audit. Pull the last 90 days of inbound calls, form fills, and CRM activity. Calculate missed-call rate, average callback time, VOB turnaround, and source-to-admit conversion by channel. The audit identifies the operational leaks before any new dollar moves.
- Days 4-7: Paid Search Restart. Activate or restart paid search with manual exact-match and phrase-match campaigns, geo-narrowed to the operator’s strongest INN footprint. Hold off on PMAX. Confirm LegitScript is active and conversion tracking is wired before any budget moves.
- Days 8-14: Admissions Team Retraining. Address the leaks identified in the audit. Missed-call rate, callback time, intake script alignment, VOB turnaround. The admissions changes land in days, not weeks, and produce admit lift before the paid search calibrates.
- Days 15-21: Creative and Landing Page Tightening. With the first two weeks of conversion data in, tighten the creative and landing pages. Fix what is not converting. Hold scope to what can ship inside the week. Big rebuilds wait until past day 30.
- Days 22-30: Optimize Against Real Data. By week 4, the paid campaigns have enough conversion data to calibrate seriously. Cost per admit should drop materially from the week-1 number. The optimization window is where the program transitions from triage to stable operation.
The sequence is sequential, not parallel. Step 1 has to land before step 2 because the audit determines where the leaks are and what budget targeting will actually convert. Step 2 produces the data that steps 3, 4, and 5 calibrate against.
The most common mistake is starting at step 2 without doing step 1. The operator activates paid search, the leads come in, the admissions team is still leaking 30 percent of calls, and the cost per admit reads as a marketing failure when it is actually an operations problem.
The first 14 days are about producing signal, not admits. If we can see VOB volume moving and viable VOB rate landing where it should, the admits land in weeks 3 and 4. Operators who panic at the week-1 number and pull spend never get to the optimization window.
Mitch Marowitz, Director of Paid Media, Webserv
The Big Lever: Paid Search Done Honestly
DO NOT LAUNCH PMAX IN WEEK 1
PMAX needs at least 14 to 21 days of conversion data to optimize against. From a cold start under triage pressure, it will burn budget on irrelevant searches before the algorithm converges. Use manual exact-match and phrase-match campaigns instead, geo-narrowed to your strongest in-network markets. PMAX becomes appropriate after day 30, once the conversion data has calibrated.
Paid search in triage looks different from paid search in a healthy program. The constraints are tighter and the calibration matters more.
Geographic targeting should be narrowed to the operator’s strongest in-network commercial footprint, not their full national catchment. The campaigns are producing volume against a fixed budget, and narrow targeting beats broad targeting at this scale.
Keyword targeting should lean on phrase and exact match, not broad. Broad match without negative-keyword maintenance burns budget on tangential queries. The negative-keyword list should be aggressive in the first 14 days and adjusted weekly thereafter.
Conversion actions should tie to the right intake event, typically a verified phone call or a completed form fill, not page visits or low-value micro-conversions. Google has published detailed guidance on how conversion tracking quality determines bidding performance and learning-phase efficiency.
Creative should match the urgency. Family-first proof points, in-network verification language, and clear intake CTAs. This is not the moment for brand-awareness creative. Distressed operators need direct-response volume, and the creative should reflect that.
The Other Fast Lever: Admissions Team Performance
DEFINITION
Missed-Call Rate
The percentage of inbound prospect calls that are not answered by the admissions team within the standard answer threshold (typically 30 seconds). In behavioral health, the typical missed-call rate at distressed operators is 25 to 40 percent. Closing this gap usually produces more admit lift than the first $20,000 of new paid spend.
The admissions team is the load-bearing variable in a triage situation. Marketing produces leads. The team converts them. If the team is missing a third of calls and taking 45 minutes to verify benefits, no amount of new media spend will solve the census problem.
The fastest fixes:
- Reduce missed-call rate. Add coverage for the call windows where most leads are dropping. Implement callback queues so missed calls trigger automated recovery within 60 seconds. Track every call against the source campaign.
- Tighten VOB turnaround. The prospects who wait 24 hours for benefits verification often go elsewhere. Move VOB to same-shift turnaround. Real-time verification tools have made this faster than it was three years ago.
- Standardize the intake script. A consistent intake script aligned to commercial verification language, in-network status, and family-engagement framing converts at higher rates than the team improvising each call.
- Track close rate by source. Separate close rate for paid search prospects, organic prospects, referrals, and walk-ins. The team’s performance varies by channel. Triage requires knowing where the gaps are.
These changes do not require new technology, new budget, or new headcount. They require attention and accountability. They land within days.
What Honest Looks Like Compared to Fast-Promise Pitches
WHAT AN HONEST 30-DAY TRIAGE COMMITMENT SOUNDS LIKE
- We will show measurable funnel signal inside 14 days, with admits landing in weeks 3 and 4
- Week 1 cost per admit will be elevated. By week 4 we expect it to drop into your model range
- Paid search is our main lever. Organic and content compound for next quarter, not this one
- The admissions team performance is half the work. We need to fix that in parallel with media
- We will not launch PMAX in week 1 because it needs conversion data to calibrate
WHAT A FAST-PROMISE 30-DAY PITCH SOUNDS LIKE
- We will get you 10 admits in 30 days
- Our cost per admit will hit your target in week 1
- We will run a full multichannel program in 30 days
- The admissions team is your problem. We just handle marketing
- We are launching PMAX day 1 to maximize coverage
The fast-promise pitches break for predictable reasons. Cost per admit cannot be calibrated in week 1 because the conversion data is not there yet.
Multichannel programs require operational depth that 30 days does not allow. PMAX from a cold start burns budget. And no marketing partner can promise admit volume without knowing the admissions team’s close rate.
The honest framing produces better outcomes because it sets expectations the program can actually meet.
Operators who hear “10 admits in 30 days” and get 4 admits in 30 days feel cheated. Operators who hear “signal in 14 days, admits in weeks 3 and 4” and get exactly that feel served.
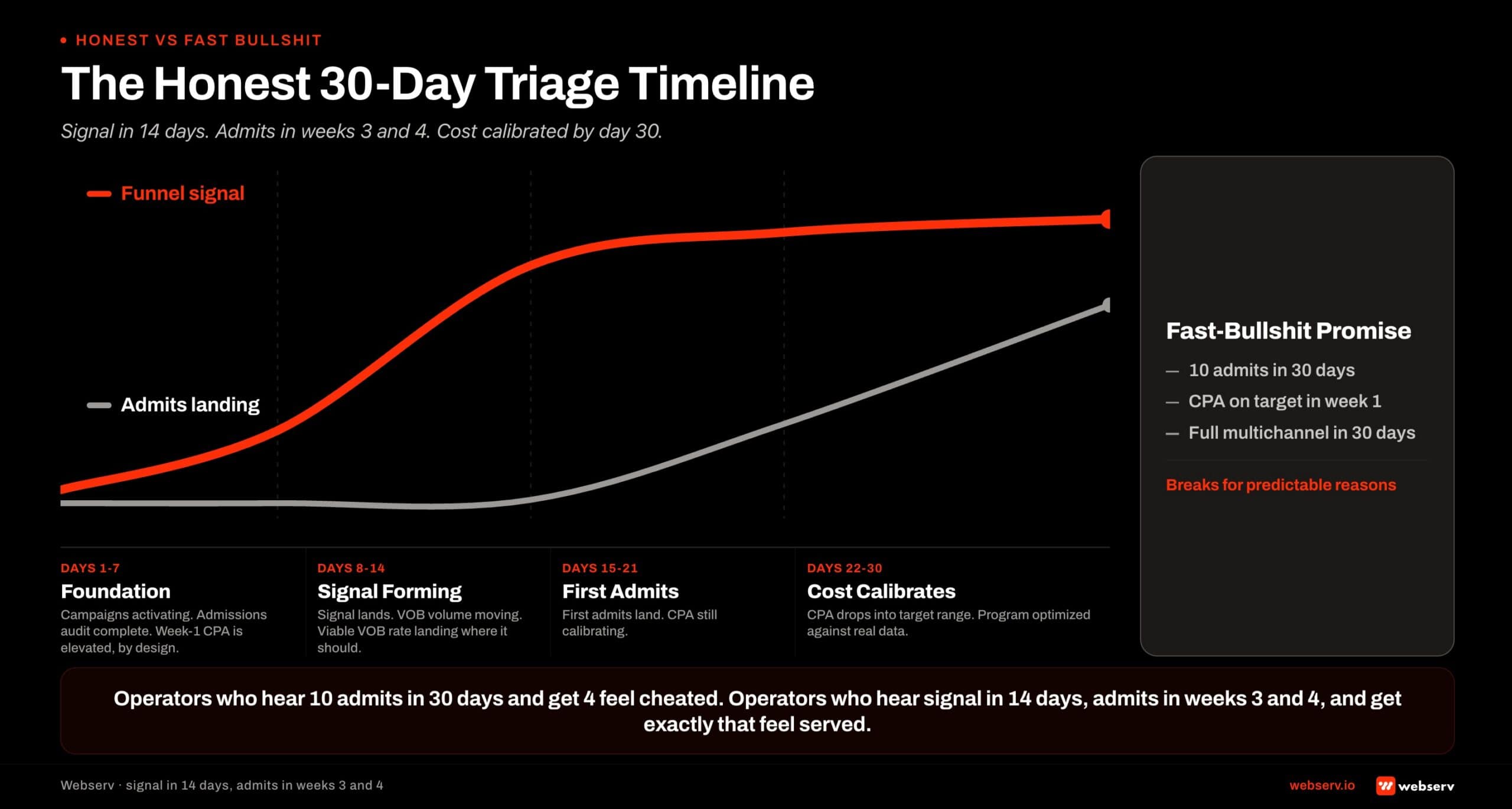 The honest 30-day triage timeline for treatment center census recovery. Days 1 to 7 foundation phase: paid search campaigns activate, admissions audit completes, week-one cost per admit is elevated by design. Days 8 to 14 signal forming: funnel signal lands, viable VOB volume moves, viable VOB rate calibrates. Days 15 to 21 first admits: admits begin landing while cost per admit is still calibrating. Days 22 to 30 cost calibrates: cost per admit drops into target range as the program optimizes against real data.
The honest 30-day triage timeline for treatment center census recovery. Days 1 to 7 foundation phase: paid search campaigns activate, admissions audit completes, week-one cost per admit is elevated by design. Days 8 to 14 signal forming: funnel signal lands, viable VOB volume moves, viable VOB rate calibrates. Days 15 to 21 first admits: admits begin landing while cost per admit is still calibrating. Days 22 to 30 cost calibrates: cost per admit drops into target range as the program optimizes against real data.What Not to Do in the First 30 Days
PROTECT THE RUNWAY YOU HAVE
The biggest mistake distressed operators make in week 1 is committing to long-cycle projects: site rebuilds, content investments, CRM migrations, new agency searches that take 60 days. All of these compete for attention and cash that the triage needs. The 30-day window is for the levers that move. The 90-day window picks up the longer projects once census stabilizes.
Specific things to defer:
- New website build. A 60-to-90-day project that adds nothing to the 30-day triage. Defer.
- Content production at scale. Compounds slowly. Useful for next quarter. Defer.
- CRM migration. Breaks operational continuity at the worst possible moment. Defer to past day 90.
- PMAX from cold start. Burns budget on the learning phase. Wait until conversion data has accumulated.
- New ad accounts. If the operator is moving agencies, the new agency should operate inside the existing client-owned accounts where possible to preserve conversion history. New accounts add 14 days of learning-phase friction.
The discipline of NOT doing things in the first 30 days is as important as the discipline of executing the triage sequence. Distressed operators have a tendency to over-commit because every action feels like progress. Over-commitment is what produced the distress in the first place.
The work for past day 30 is real and important. Site improvements, content production, organic SEO, CRM optimization, and creative deepening all matter. They do not matter inside the 30-day triage window. Book an intro meeting if you want to walk your triage timeline with us live.
Frequently Asked Questions
Can paid search really produce admits in 30 days?
Paid search produces qualified calls and form fills within days of activation, assuming LegitScript certification is in place and conversion tracking is properly wired. The first admits typically land in weeks 3 and 4 as the prospects move through assessment, VOB, and intake.
The honest framing is that paid search produces measurable funnel signal inside 14 days. The cost per admit during weeks 1 and 2 is elevated because the campaigns have not yet calibrated against real conversion data. By weeks 3 and 4, the cost should drop to within the operator’s target range.
Operators who pull spend in week 2 because the cost per admit looks high never reach the calibration window. The discipline of holding through weeks 1 and 2 is the variable that separates programs that work from programs that do not.
What if our LegitScript certification has lapsed or never existed?
LegitScript certification is required for paid search and paid social on addiction treatment terms. If certification has lapsed or never been in place, paid media on regulated terms is not an immediate lever. The certification process typically takes 30 to 60 days from application to active.
For operators in active triage without certification, the immediate paths are admissions team optimization, existing landing page tightening, and re-engaging existing referral relationships. None of these require LegitScript. They produce real lift inside 30 days.
The certification application should start in week 1 of triage so paid media becomes available for the 60-day window even though it is not available for the 30-day window.
How do I know if our admissions team is the bottleneck or our marketing is the bottleneck?
Pull the last 90 days of inbound calls and form fills, segmented by source. Calculate missed-call rate, lead-to-VOB conversion, and VOB-to-admit conversion for each channel.
If missed-call rate is above 20 percent or lead-to-VOB conversion is below 60 percent, the admissions team is the primary bottleneck. New media spend will not solve the census problem until those numbers move.
If both numbers are healthy and the volume is simply too low, marketing is the primary bottleneck. The triage sequence will land. In most distressed operators we audit, the answer is both, with the admissions side producing faster initial wins than the media side.
Can we afford to spend on marketing if our margins are already negative?
The question is not whether you can afford to spend. It is what spend produces a positive contribution margin given your current cost per admit and your average revenue per admit. If a $10,000 paid search investment is expected to produce 5 admits at $12,000 average revenue, the spend pays back.
The math has to be modeled before any budget moves. Webserv runs this calculation as part of the triage intake. The output is a contribution-margin-positive spend plan, not a flat budget recommendation.
Operators who cut all marketing spend during distress usually lose census faster than the savings cover. Operators who triple marketing spend without modeling contribution margin usually run out of cash before the program calibrates. The middle path is a disciplined spend tied to expected unit economics.
Preston Powell is the CEO at Webserv, a digital marketing agency for treatment centers.