A treatment center founder forwarded me a pitch from a healthcare content farm last month. The pitch was for 60 articles a month at $42 per piece.
The agency promised “SEO-optimized, healthcare-compliant content” produced by their “team of healthcare writers.” The pricing came out to $2,520 a month for the equivalent of two full-time writers’ worth of output. The founder asked me whether the math made sense for his treatment center’s authority content program.
I pulled the agency’s portfolio. They were running content for 14 other treatment centers, plus 30 dental practices, 20 medspa chains, and a handful of urgent care groups. The bylines on the BH content read “Healthcare Writing Team” on every piece. None of the articles had credentialed clinical attribution.
The content was technically accurate (it described levels of care reasonably, covered insurance verification adequately, and met minimum YMYL bars on factual claims) but operationally generic.
None of the pieces referenced the specific facility, the specific clinical approach, the specific payer mix, or the specific patient population that any of the operators actually served. Across the 14 BH clients, the content was 80 percent interchangeable.
I ran a citation audit on three of the farm’s BH clients. None of the three had earned AI Mode citations in the prior 90 days across a basket of 30 representative prompts.
All three were producing 50+ pieces a month and ranking on long-tail queries that did not produce admissions. The dental clients and medspa clients showed similar patterns. The content farm had a working business model. It was working at the expense of the operators paying for it.
This piece makes the case against that model for behavioral health. Generic healthcare content farms produce content that is technically functional but strategically worthless in the 2026 retrieval environment. The economics that justify them rely on counting word volume rather than admission impact.
The alternative is sharply different in shape and unit economics. Our authority content practice is built around the alternative because the farm model stopped working for BH operators in 2024 and has gotten worse since.
Key Takeaways
- Generic healthcare content farms produce content that meets minimum YMYL standards but lacks the credentialed clinical attribution, operational specificity, and entity signal that 2026 AI retrieval models reward.
- The economics that justify content farms (volume at low per-piece cost) inverted in 2025 when AI search engines started weighting author entity and claim specificity more heavily than raw word count.
- Three specific risks make farms worse for behavioral health than for other healthcare verticals: compliance gaps around addiction services policy, HIPAA exposure in client-shared content infrastructure, and brand damage when content is reused across competing facilities.
- The retrieval layer is increasingly capable of detecting generic content patterns. Sites running heavy farm output produce ranking without citations, which translates to traffic without admissions for buyers using AI search.
- The alternative is fewer pieces with real clinician contribution. Most BH operators can produce 4 to 8 high-authority pieces per month for less total budget than the farm model and generate much more admission lift over 12 months.
What a generic healthcare content farm actually looks like
The distinguishing characteristics of a content farm are not always obvious from the agency pitch. Six markers separate the farm model from working alternatives.
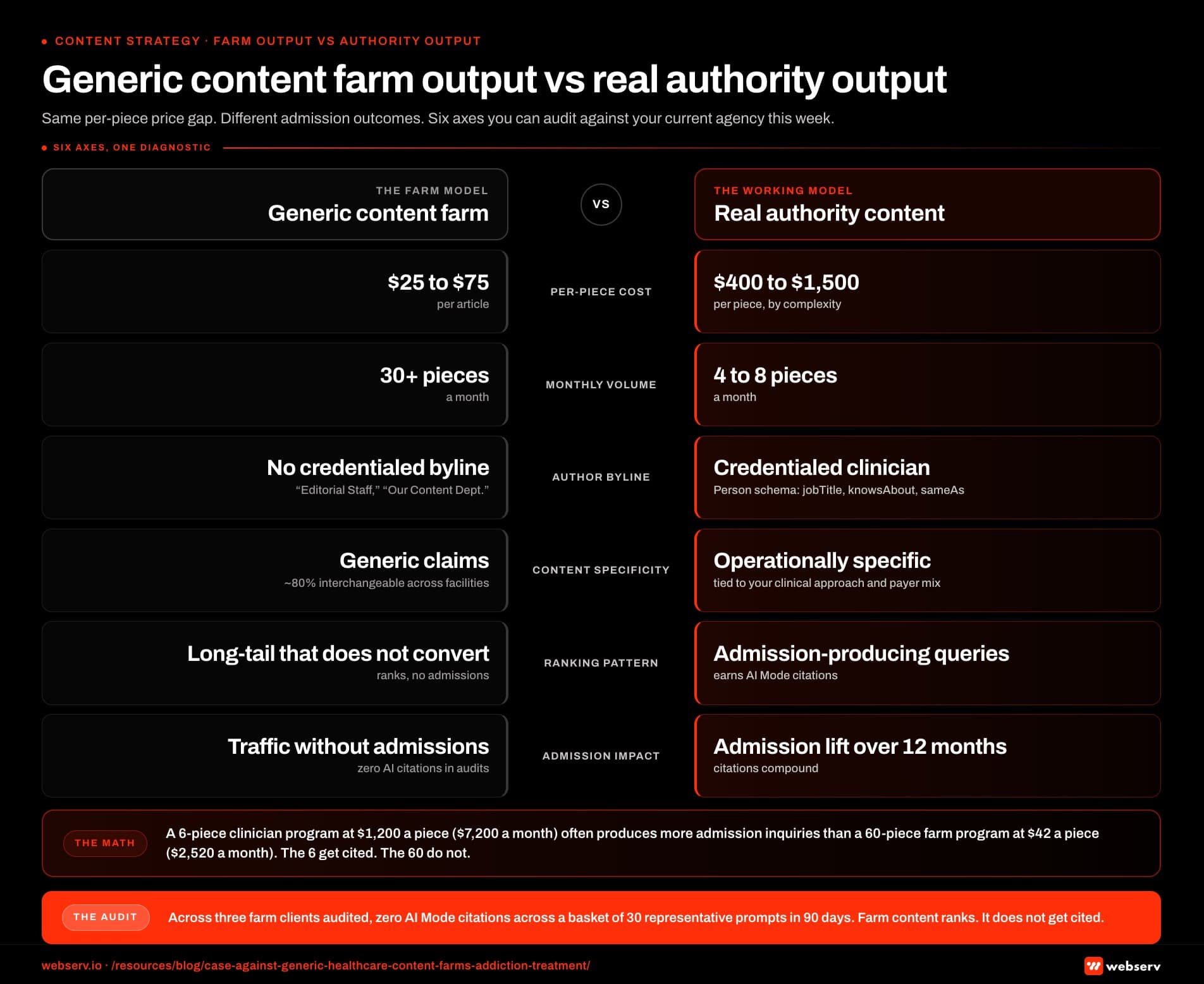 Infographic titled ‘Generic content farm output vs real authority output’ showing a two-column side-by-side comparison of the generic healthcare content farm production model on the left and the real authority content production model on the right, structured as six comparison axes. Per-piece cost: farm runs $25 to $75 per article, authority runs $400 to $1,500 per piece depending on complexity. Monthly volume: farm produces 30 plus pieces a month, authority produces 4 to 8 pieces a month. Author byline: farm uses Healthcare Writing Team, Editorial Staff, or Our Content Department with no credentialed attribution, authority uses credentialed clinical attribution with Person schema including jobTitle, knowsAbout, and sameAs properties. Content specificity: farm produces generic claims that are roughly 80 percent interchangeable across competing facilities, authority produces operationally specific claims tied to the facility’s clinical approach, payer mix, and patient population. Ranking pattern: farm ranks on long-tail queries that do not produce admissions, authority earns AI Mode citations on queries that do produce admissions. Admission impact: farm produces traffic without admissions and zero AI citations across audited prompt baskets, authority produces admission lift over 12 months with citations that compound. Left-column callout: 80 percent of farm content is interchangeable across competing facilities, and two operators in the same metro running the same farm often have substantial content overlap they do not know about. Right-column callout: a 6-piece clinician-driven program at $1,200 per piece for $7,200 monthly often produces more admission inquiries than a 60-piece farm program at $42 per piece for $2,520 monthly, because the 6 pieces get cited and the 60 do not. Bottom strip: across three farm clients audited, zero AI Mode citations were earned across a basket of 30 representative prompts in 90 days, because farm content ranks but does not get cited.
Infographic titled ‘Generic content farm output vs real authority output’ showing a two-column side-by-side comparison of the generic healthcare content farm production model on the left and the real authority content production model on the right, structured as six comparison axes. Per-piece cost: farm runs $25 to $75 per article, authority runs $400 to $1,500 per piece depending on complexity. Monthly volume: farm produces 30 plus pieces a month, authority produces 4 to 8 pieces a month. Author byline: farm uses Healthcare Writing Team, Editorial Staff, or Our Content Department with no credentialed attribution, authority uses credentialed clinical attribution with Person schema including jobTitle, knowsAbout, and sameAs properties. Content specificity: farm produces generic claims that are roughly 80 percent interchangeable across competing facilities, authority produces operationally specific claims tied to the facility’s clinical approach, payer mix, and patient population. Ranking pattern: farm ranks on long-tail queries that do not produce admissions, authority earns AI Mode citations on queries that do produce admissions. Admission impact: farm produces traffic without admissions and zero AI citations across audited prompt baskets, authority produces admission lift over 12 months with citations that compound. Left-column callout: 80 percent of farm content is interchangeable across competing facilities, and two operators in the same metro running the same farm often have substantial content overlap they do not know about. Right-column callout: a 6-piece clinician-driven program at $1,200 per piece for $7,200 monthly often produces more admission inquiries than a 60-piece farm program at $42 per piece for $2,520 monthly, because the 6 pieces get cited and the 60 do not. Bottom strip: across three farm clients audited, zero AI Mode citations were earned across a basket of 30 representative prompts in 90 days, because farm content ranks but does not get cited.Per-piece pricing in the $25 to $75 range. Real clinical content (drafted by experienced healthcare writers, reviewed by credentialed clinicians, schema-deployed) costs $400 to $1,500 per piece depending on complexity. Per-piece pricing below $100 reflects production economics that cannot support real clinical review.
Volume promises of 30+ pieces a month. The volume is the giveaway. A working clinical content program at a single facility produces 4 to 8 pieces a month with clinician input. 30+ pieces requires the kind of factory-line production that cannot incorporate real clinical contribution at the per-piece cost level.
Shared writer pools across many clients. A farm with 60 BH clients employs 4 to 8 writers who rotate across all of them. The writers cannot develop facility-specific expertise. The output reads generic because the writers are generic across the client base.
Each writer produces 10 to 30 pieces a month, which leaves no time for facility research, clinical interviews, or content customization.
No credentialed author bylines. The bylines read “Healthcare Writing Team,” “Editorial Staff,” “Our Content Department,” or rotate through first-name attributions that do not resolve to verifiable credentials. The author entity infrastructure that 2026 E-E-A-T author bios require is absent because the farm model cannot support it economically.
Reused content across competing facilities. The pattern most operators do not realize is that the same articles often appear across multiple facilities the farm serves, with the facility name swapped and a few sentences customized. Some farms call this “templated content.”
In practice it is duplicate or near-duplicate content distributed across competing operators. Two BH operators in the same metro running the same farm often have substantial content overlap they do not know about.
Pitch language focused on volume, ranking, and “SEO compliance.” The pitch describes the deliverable as articles produced, keywords targeted, and rankings projected. It does not describe admission attribution, clinical authority development, or AI citation rate. The framing reveals the optimization target.
Operators evaluating a content agency should probe for these six markers explicitly. Agencies that pass all six checks are not farms. Agencies that fail more than two are almost certainly running the farm model regardless of how they describe themselves.
Why the economics that pitch farms are misleading
The case for content farms always lands on the per-piece economics. $42 per article times 60 articles is $2,520 a month, which sounds inexpensive next to a $15,000-a-month clinical content program. The math relies on two assumptions that no longer hold in 2026.
Assumption 1: more pieces produces more traffic. This was directionally true in 2018 to 2020 when Google’s quality systems were less mature and “topical authority” could be built through volume.
It is not true in 2026. Google Search Central’s helpful content guidance explicitly weights content quality and author expertise above content volume.
Sites producing 60 pieces a month of farm content typically rank on fewer commercial queries than sites producing 6 pieces a month of clinician-quoted content. The volume math does not survive the quality filter.
Assumption 2: more traffic produces more admissions. This was directionally true when admission inquiries came mostly from organic blue-link clicks. In 2026, an increasing share of treatment-seeking research routes through AI search engines that cite specific sources, not browsing patterns that aggregate across many sites.
Farm content rarely gets cited because the credential signal is absent and the claim specificity is generic. Traffic that does not get cited in AI answers does not translate to the brand exposure that drives admissions.
The right metric is admission impact per dollar of content spend, not pieces per dollar. On that metric, the farm model usually produces worse unit economics than the clinician-driven model despite the per-piece price difference.
A 6-piece clinician-driven program at $1,200 per piece ($7,200 monthly) often produces more admission inquiries per month than a 60-piece farm program at $42 per piece ($2,520 monthly), because the 6 pieces get cited and the 60 do not.
The honest accounting is that operators paying for content farm output are usually paying for words that do not contribute to admissions. The healthcare content creation framework we recommend treats every piece as an admission-economics decision rather than a word-output decision.
The lower per-piece price is real. The total program cost-to-admission ratio is much worse than the alternative.
“The honest accounting is that operators paying for content farm output are usually paying for words that do not contribute to admissions.”
Preston Powell, Chief Executive Officer, Webserv
Behavioral-health-specific risks farms miss
Three risks make content farms worse for addiction treatment than for general healthcare. Each one compounds the underperformance covered above.
 Infographic titled ‘The 3 BH-specific risks content farms miss’ showing the three risks that make generic healthcare content farms worse for addiction treatment than for general healthcare, arranged as a three-card horizontal diagnostic. Card 1 compliance gap around addiction services policy: farm writers producing 15 behavioral health pieces a month across many operators rarely understand which language triggers a Google Ads disable, which claims violate Meta’s healthcare creative policy, or which LegitScript compliance obligations the operator carries; the exposure pattern is that generic farm content frequently includes language that creates compliance exposure the operator does not catch until an account disable or policy strike forces remediation; how it surfaces is a Google Ads disable, a Meta creative reject, or a LegitScript flag. Card 2 HIPAA exposure in client-shared content infrastructure: farms typically use shared CMS access, shared analytics, and shared editorial pipelines across many clients, and the infrastructure is not configured for HIPAA Business Associate Agreement coverage at the level behavioral health operators need; the exposure pattern is that when the farm’s editorial team can see CRM data, intake patterns, or any other operator-specific information that touches PHI, the exposure is real even if the farm believes it is only handling marketing content; how it surfaces is HHS-OCR enforcement under the 2026 online-tracking guidance. Card 3 brand damage when content is reused across competing facilities: a farm serving 14 behavioral health operators is producing content that overlaps heavily across all 14, and two operators in the same metro running farm content from the same agency often end up with near-identical pages competing for the same queries; the exposure pattern is that the duplicate-content pattern degrades both operators’ rankings and a clinical claim accurate for one facility can be inaccurate for another served by the same farm; how it surfaces is when a third party such as a competitor, journalist, or regulator surfaces the pattern publicly. Bottom strip callout: these three risks are specific to behavioral health and especially to facilities serving substance use disorders, and general healthcare farms are not optimized to manage them while behavioral health operators using those farms inherit the exposure.
Infographic titled ‘The 3 BH-specific risks content farms miss’ showing the three risks that make generic healthcare content farms worse for addiction treatment than for general healthcare, arranged as a three-card horizontal diagnostic. Card 1 compliance gap around addiction services policy: farm writers producing 15 behavioral health pieces a month across many operators rarely understand which language triggers a Google Ads disable, which claims violate Meta’s healthcare creative policy, or which LegitScript compliance obligations the operator carries; the exposure pattern is that generic farm content frequently includes language that creates compliance exposure the operator does not catch until an account disable or policy strike forces remediation; how it surfaces is a Google Ads disable, a Meta creative reject, or a LegitScript flag. Card 2 HIPAA exposure in client-shared content infrastructure: farms typically use shared CMS access, shared analytics, and shared editorial pipelines across many clients, and the infrastructure is not configured for HIPAA Business Associate Agreement coverage at the level behavioral health operators need; the exposure pattern is that when the farm’s editorial team can see CRM data, intake patterns, or any other operator-specific information that touches PHI, the exposure is real even if the farm believes it is only handling marketing content; how it surfaces is HHS-OCR enforcement under the 2026 online-tracking guidance. Card 3 brand damage when content is reused across competing facilities: a farm serving 14 behavioral health operators is producing content that overlaps heavily across all 14, and two operators in the same metro running farm content from the same agency often end up with near-identical pages competing for the same queries; the exposure pattern is that the duplicate-content pattern degrades both operators’ rankings and a clinical claim accurate for one facility can be inaccurate for another served by the same farm; how it surfaces is when a third party such as a competitor, journalist, or regulator surfaces the pattern publicly. Bottom strip callout: these three risks are specific to behavioral health and especially to facilities serving substance use disorders, and general healthcare farms are not optimized to manage them while behavioral health operators using those farms inherit the exposure.Compliance gap around addiction services policy. Google’s addiction services policy and Meta’s healthcare sensitive category restrictions require specific knowledge to comply with.
A farm writer producing 15 BH pieces a month across multiple operators rarely understands which language triggers a Google Ads disable, which claims violate Meta’s healthcare creative policy, or which LegitScript compliance obligations the operator carries.
The healthcare blog and article writing standards we follow require category-specific compliance knowledge that farms generally lack. Generic farm content frequently includes language that creates compliance exposure the operator does not catch until an account disable or policy strike forces remediation.
HIPAA exposure in shared content infrastructure. Farms typically use shared CMS access, shared analytics, and shared editorial pipelines across many clients. The infrastructure is not configured for HIPAA Business Associate Agreement coverage at the level BH operators need.
When the farm’s editorial team can see CRM data, intake patterns, or any other operator-specific information that touches PHI, the exposure is real even if the farm believes it is “only handling marketing content.”
Per the HHS-OCR guidance on HIPAA-regulated online tracking, the 2026 enforcement environment makes this risk notably higher than it was in prior years, on top of the broader compliance mistakes that surface across paid and organic channels.
Content reuse across competing facilities. A farm serving 14 BH operators is producing content that overlaps heavily across all 14. Two operators in the same metro running farm content from the same agency often end up with near-identical pages competing for the same queries.
The duplicate-content pattern degrades both operators’ rankings. Worse, the healthcare advertising compliance constraints that govern claim accuracy can produce strange situations where a clinical claim accurate for one facility is inaccurate for another served by the same farm.
The operators usually do not realize this until a third party (a competitor, a journalist, a regulator) surfaces the pattern. These three risks are specific to BH and especially to facilities serving substance use disorders.
General healthcare farms underweight them because their dental and medspa clients do not face the same compliance posture. BH operators using the same farms inherit risk the farms are not built to manage.
How the 2026 retrieval layer discounts farm content
The pattern across the citation audits we run on farm-content sites is consistent. Generic healthcare content produced at farm scale is increasingly invisible in AI search even when it ranks organically.
Three retrieval-layer mechanisms produce the discount.
Author entity recognition. Farm content lacks the credentialed author entity signal the retrieval models look for in YMYL. Person schema with jobTitle, knowsAbout, and sameAs properties cannot be deployed authentically when the byline is “Editorial Team.”
Sites running farm content fail the entity infrastructure bar that 2026 AI citation eligibility requires.
Claim specificity scoring. The retrieval models have learned to distinguish generic clinical claims from operationally specific claims. Farm content clusters around generic claims because the writers do not have facility-specific clinical knowledge. “Patients with co-occurring disorders benefit from integrated treatment approaches” gets discounted.
“Our 14-year dual-diagnosis residential program saw a 38 percent to 19 percent reduction in 90-day readmission when families participated in the first three multi-family sessions” gets cited. The specificity gap is exactly what farm economics cannot close.
Topical authority dilution. Sites running 50+ pieces a month of generic content develop weaker topical authority than sites running 6 to 8 pieces a month of focused content. The retrieval models evaluate authority on the cluster, not on the volume.
A cluster with 200 pieces of farm content reads as thinner authority than a cluster with 30 pieces of clinician-driven content because the per-piece signal strength is lower.
The combined effect across all three mechanisms is the pattern in the opening audit: farm-content sites rank on long-tail queries that do not produce admissions, while clinician-driven sites at smaller volume earn AI citations on the queries that do.
The keyword strategy work that maps queries to admission-economics impact is what surfaces this gap. The 2026 retrieval environment punishes the farm model in ways the 2020 environment did not, and the gap is widening as the AI search models improve.
How SoCal Sunrise generated 85 admissions and 2,297% ROI from SEO in 6 months
A ground-up SEO rebuild using the Pathfinder Parents Methodology turned an invisible online presence into a top-ranking admissions engine.
Read the case study →85 admits and 3,152 leads attributed to organic
What to do if you are already running a content farm
The first instinct most operators have when this argument lands is to fire the agency. That is not always the right first step. The transition needs sequencing.
Step 1: audit what you actually have. Pull the 100 to 200 farm-produced pieces, group them by topic cluster, identify which (if any) are producing admission inquiries.
Most farm libraries have 5 to 20 pieces that incidentally produce admissions and 100+ pieces that produce nothing. The audit surfaces the small set worth keeping.
Step 2: identify the content gaps. The content gap analysis work surfaces what the cluster actually needs that the farm has not produced. The gap inventory becomes the input to the new content program.
Most operators discover that the gaps are 80 percent of the addressable space, which the farm volume hid by producing tangential content that filled the dashboard without filling the gaps.
Step 3: build the new infrastructure in parallel. Before terminating the farm, set up the clinician-driven program (credentialed authors, author bio infrastructure, Person schema deployment, editorial workflow). This takes 4 to 8 weeks. Running it in parallel with the farm prevents a content-output gap during the transition.
Step 4: stop new farm output, start new program output. Once the new infrastructure is in place, end the farm contract and start the clinician-driven cadence at 4 to 8 pieces a month.
The farm library stays live (with the exception of any pieces that are duplicate, non-compliant, or actively harmful), and the new pieces compound on top.
Step 5: retire the underperforming farm content over 12 to 18 months. Pieces from the audit that do not produce admissions and do not contribute to topical authority get 301-redirected to the closest relevant new piece or to the cluster pillar.
This is the same logic that governs doorway pages cleanup for site architecture: underperforming content should not stay indexed, and the redirect preserves whatever incidental equity exists.
The transition usually runs 6 to 12 months end to end. Operators who try to rip out the farm in week one without the replacement infrastructure produce a content output gap that hurts in the short term.
Operators who run the parallel build avoid that gap and end up with a stronger program by month 12.
What the alternative actually looks like
The alternative to the farm is not “we hire one expensive writer” or “we wait for clinicians to write the content themselves.”
The alternative is the human-in-the-loop model where credentialed clinicians contribute through interviews and quote sourcing, non-clinical writers draft based on that input, and the editorial pipeline supports both the clinical contribution and the publication cadence.
The economics for a typical BH operator running this model:
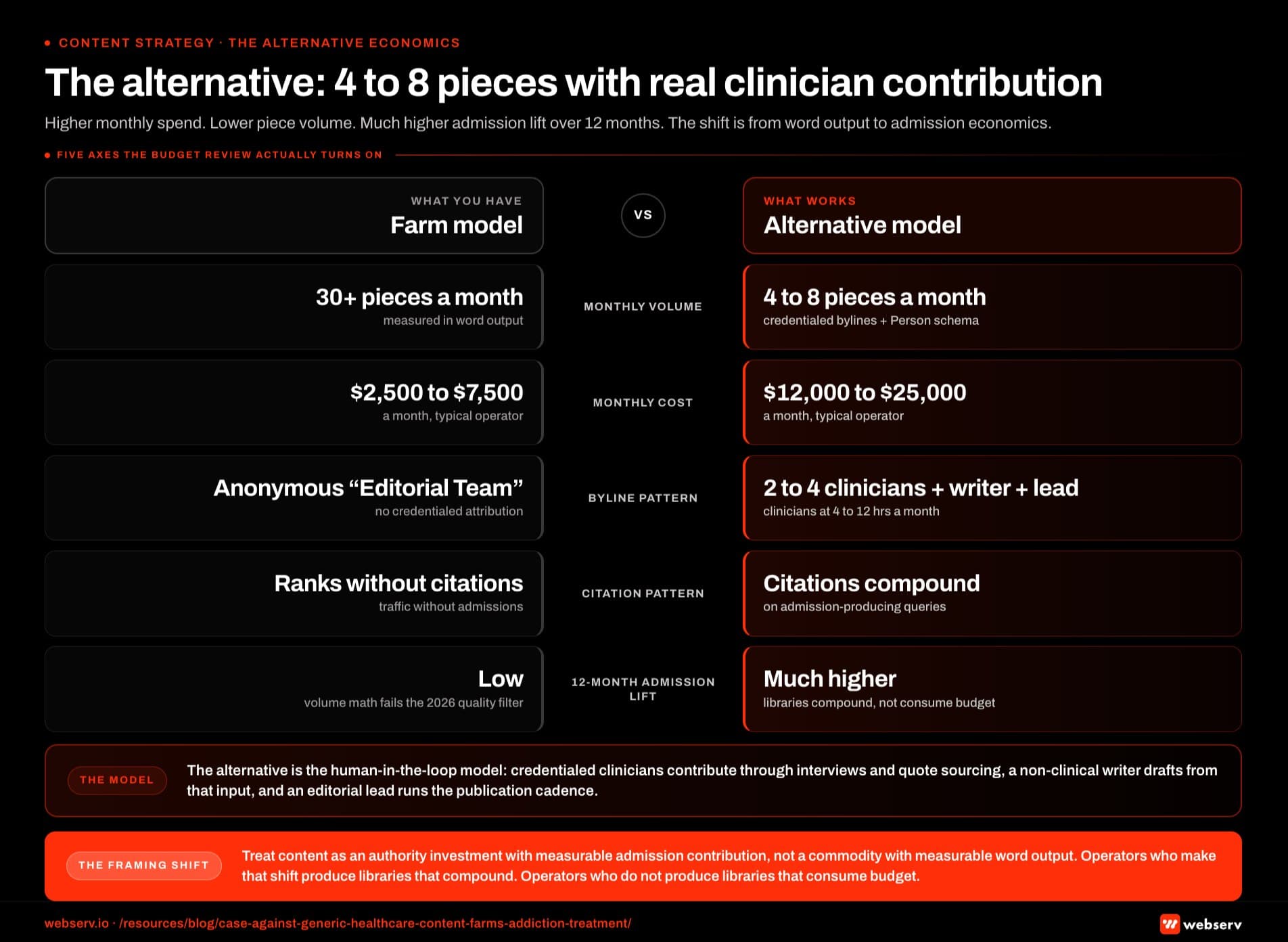 Infographic titled ‘The alternative: 4 to 8 pieces with real clinician contribution’ showing a side-by-side economics comparison of the farm content production model on the left and the human-in-the-loop alternative model on the right, structured as five economic axes. Monthly volume: farm produces 30 plus pieces a month, alternative produces 4 to 8 pieces a month with credentialed bylines and Person schema. Monthly cost: farm runs $2,500 to $7,500 a month at a typical operator, alternative runs $12,000 to $25,000 a month at a typical operator. Byline pattern: farm uses anonymous Editorial Team or rotating first names with no credentialed attribution, alternative uses 2 to 4 credentialed clinical contributors at 4 to 12 hours per month with 1 non-clinical writer drafting and 1 editorial lead managing the workflow. Citation pattern: farm ranks without citations and produces traffic without admissions, alternative earns citations that compound on the queries that produce admissions. 12-month admission lift: farm produces low admission lift because the volume math does not survive the 2026 quality filter, alternative produces much higher admission lift over 12 months because libraries compound rather than consume budget. Left-panel callout: the farm model produces words that do not contribute to admissions, the lower per-piece price is real, but the total program cost-to-admission ratio is much worse than the alternative. Right-panel callout: the alternative is the human-in-the-loop model where credentialed clinicians contribute through interviews and quote sourcing, non-clinical writers draft based on that input, and the editorial pipeline supports both the clinical contribution and the publication cadence. Bottom strip callout: treat content as an authority investment with measurable admission contribution rather than as a marketing commodity with measurable word output; operators who make that framing shift produce libraries that compound and operators who do not produce libraries that consume budget.
Infographic titled ‘The alternative: 4 to 8 pieces with real clinician contribution’ showing a side-by-side economics comparison of the farm content production model on the left and the human-in-the-loop alternative model on the right, structured as five economic axes. Monthly volume: farm produces 30 plus pieces a month, alternative produces 4 to 8 pieces a month with credentialed bylines and Person schema. Monthly cost: farm runs $2,500 to $7,500 a month at a typical operator, alternative runs $12,000 to $25,000 a month at a typical operator. Byline pattern: farm uses anonymous Editorial Team or rotating first names with no credentialed attribution, alternative uses 2 to 4 credentialed clinical contributors at 4 to 12 hours per month with 1 non-clinical writer drafting and 1 editorial lead managing the workflow. Citation pattern: farm ranks without citations and produces traffic without admissions, alternative earns citations that compound on the queries that produce admissions. 12-month admission lift: farm produces low admission lift because the volume math does not survive the 2026 quality filter, alternative produces much higher admission lift over 12 months because libraries compound rather than consume budget. Left-panel callout: the farm model produces words that do not contribute to admissions, the lower per-piece price is real, but the total program cost-to-admission ratio is much worse than the alternative. Right-panel callout: the alternative is the human-in-the-loop model where credentialed clinicians contribute through interviews and quote sourcing, non-clinical writers draft based on that input, and the editorial pipeline supports both the clinical contribution and the publication cadence. Bottom strip callout: treat content as an authority investment with measurable admission contribution rather than as a marketing commodity with measurable word output; operators who make that framing shift produce libraries that compound and operators who do not produce libraries that consume budget.- 2 to 4 credentialed clinical contributors at 4 to 12 hours per month each
- 1 non-clinical content writer (full-time, part-time, or freelance) producing first drafts from clinician input
- 1 editorial lead managing planning, workflow, and SEO/technical deployment
- 4 to 8 published pieces per month with credentialed bylines and Person schema
The total monthly cost lands at $12,000 to $25,000 for most operators. The farm model at the same operator usually runs $2,500 to $7,500 a month.
The difference is real. The difference is also justified by the admission economics, which favor the more expensive model on every measure operators actually care about.
The shift in framing that makes this work is treating content as an authority investment with measurable admission contribution rather than as a marketing commodity with measurable word output.
Operators who make that framing shift produce content libraries that compound. Operators who do not produce libraries that consume budget without producing admissions.
This is the same logic that powers the clinician-quote moat argument we publish elsewhere. Both pieces argue against the volume-as-strategy model.
This piece focuses on why the existing volume-strategy infrastructure (the content farm) is the wrong infrastructure to keep, even if the operator agrees with the strategic direction.
The broader behavioral health marketing program only compounds when the content engine is built on credentialed authority, not on volume.
Frequently Asked Questions
How do we know if our current agency is running the farm model?
Run the six markers test from earlier in this piece. Per-piece pricing under $100, volume promises above 30 pieces a month, shared writer pools, “Editorial Team” bylines, evidence of reused content across clients, and pitch language focused on volume rather than admission attribution.
Agencies that fail more than two markers are running the farm model regardless of how they describe themselves.
The second test is to ask the agency to walk you through a specific clinical claim in one of their recent pieces and identify which credentialed contributor sourced it.
Real clinical content programs can answer this in detail. Farm programs cannot, because the claims come from research aggregation rather than from a specific clinical voice.
The third test is to compare three recent pieces from your account against three recent pieces the same agency produced for a different BH client. If the structural similarity is high (same outline, same sub-headers, same talking points with the facility name swapped), the farm pattern is confirmed.
What about Google’s spam policies on scaled content abuse?
Google introduced scaled content abuse as a specific spam policy violation in 2024, and the enforcement intensified through 2025 and 2026.
The policy targets content produced at scale primarily for ranking manipulation rather than user value, which describes much of the farm model directly. Sites running heavy farm output can face manual actions or algorithmic demotion under this policy.
Most farm operators argue that their content has human review and meets minimum quality bars, which keeps the work technically inside the policy boundary. The enforcement reality is that the boundary is moving.
Sites that operated comfortably inside the policy in 2024 face more scrutiny in 2026, and the discount applied to scaled content is widening even when the manual action threshold is not crossed.
For BH operators, the risk is that the content farm’s broader client base creates a guilt-by-association pattern in the retrieval layer.
Sites associated with farms whose other clients have been flagged tend to inherit some of the discount. This is hard to verify but consistent with the audit data we see.
Can we use AI tools to produce content faster without running a farm?
Yes, with discipline. AI tools used as drafting and research assistance within a clinician-driven workflow are different from AI tools used to produce content at scale. The line is whether the credentialed clinical contribution is real and substantial.
A writer using ChatGPT to help structure an outline based on clinician interview notes, then drafting the piece with the AI assistance, and submitting it to the credentialed clinician for review and quote integration, is using AI productively.
The content’s final form includes real clinical contribution that the AI cannot manufacture.
A writer asking ChatGPT to produce a full draft on a topic without any clinician input, then publishing it under an anonymous byline, is running the farm model with AI instead of a writer pool. The economics shift slightly but the strategic problem is the same.
The right test is whether a credentialed clinician could defend the specific clinical claims in the piece as their own.
If yes, the AI assistance is supplementary. If no, the AI is producing the content and the farm model risks apply.
Is there ever a case for the farm model?
For non-YMYL marketing content (general operations, industry news, broad business context that does not make clinical claims), the farm model can be defensible.
The compliance risk is lower because no specific clinical claims are made, and the entity signal matters less because the content is not the kind that earns AI citation.
For YMYL content (anything that touches treatment, clinical decisions, admissions, payer mix, family decision-making), the farm model is the wrong fit. The retrieval layer treats YMYL content differently from non-YMYL content, and the credentialed signal is much more important in the YMYL space.
Most BH content is YMYL by definition. The exceptions (operational logistics, the surrounding regional context for a facility, light brand or culture content) are a small fraction of the content the operator should be producing. The farm model is wrong for the bulk of the work.
What about agencies that say they have clinical reviewers on staff?
The right question to ask is whether the clinical reviewer is named, credentialed, and bylined on the content.
A reviewer who is internal to the agency and never appears as a bylined author cannot produce the E-E-A-T signal the retrieval models look for. The reviewer’s credentials need to attach to the published content through Person schema and visible attribution.
Agencies that have a clinical reviewer but do not byline that reviewer on the content are usually using the reviewer as a fact-check pass without integrating their authority into the published work. The model still produces content that fails the 2026 author entity bar.
The working model has the clinical reviewer as the bylined author or as the named co-author with a non-clinical writer.
The reviewer’s credentials, byline, photograph, and Person schema appear on the published piece. The agency’s role is to produce the workflow that enables this, not to use the reviewer as an internal-only fact-checker.
How fast can we transition off a farm to the alternative?
The clinical infrastructure (credentialed contributors, author bios, Person schema deployment) takes 4 to 8 weeks to set up.
The new content program reaches steady-state cadence at 8 to 16 weeks from the initial commitment. The full transition off the farm, including content audit, gap analysis, and underperforming-content retirement, takes 6 to 12 months.
The fastest transitions happen when operators are willing to run the parallel build with the new program. The slowest transitions are when operators try to keep the farm running indefinitely while the new program ramps, which produces ambiguity about which content is contributing and which is not.
The cleanest pattern is: 4-week build phase, 8-week parallel run, then end the farm contract and run the new program alone with a 6-month retirement plan for the old library. This sequencing avoids content gaps and gives the new program room to compound without competing with the farm output.
The perspective in this article comes from 9 years working exclusively inside behavioral health.
We are a team built by people in recovery who understand that behind every admission is someone asking for help. If that resonates, get to know us.
Trevor Gage is the Director of Earned & Owned Media at Webserv, where he leads SEO, content strategy, and organic acquisition for behavioral health treatment centers.
He has overseen audits of more than 200 behavioral health sites and writes about the technical and editorial SEO standards Webserv applies to client work.