When a new treatment center signs with us, the first day’s work is verifying every part of how the program is set up to bill. Claim submission comes later.
State licenses, NPI structures, Joint Commission addresses, MD credentials, EFT setup, EIN configuration. Every one of those affects whether a claim pays, whether a future contract becomes available, and whether the program can scale without rebuilding its foundation. The same diligence sits underneath how we approach behavioral health billing and RCM with operators who are about to grow.
Most centers cannot run a billing operations checklist consistently in-house at scale. Picking the right RCM partner, one that publishes operational benchmarks and runs the checklist against them, is the single biggest lever on this metric.
Most billing companies skip this layer entirely. The setup is treated as something the operator handled. The billing partner takes whatever is in place and starts submitting claims.
That is the lazy version. The lazy version produces revenue for a quarter, breaks at the first audit, and leaves the operator wondering why their billing operation cannot grow with their census.
The version that actually scales is a phased operations checklist. The setup phase happens before any claim goes out.
The weekly operating phase runs every week thereafter. The quarterly audit phase runs against the live portfolio four times a year. The scale phase is what changes in each of the prior three when the program grows.
The billing operations checklist is the operating control panel for the program. Most centers treat it as a back-office form. The growing centers treat it as the first thing they upgrade when census moves.
Kyle McHenry, Founder, Revenue Logic
Key Takeaways
- A billing operations checklist runs in four phases — setup, weekly operating rhythm, quarterly audit, and scale — and each phase is the prerequisite for the next. Skipping setup produces revenue for a quarter and breaks at the first audit.
- Phase 1 verifies state licenses, NPI structure, EIN alignment, Joint Commission addresses, MD credentials, EFT routing, payer enrollment, and clearinghouse/EDI configuration before the first claim ships. One week of work on a clean program; three to four on a program that has been running without an audit.
- Phase 2 is a weekly seven-domain review: VOB, utilization review, claim submission, claim follow-up, payment posting, credentialing, and medical records evaluations. The cadence relaxes as the team matures but the domains do not change.
- Phase 3 is a backward-looking quarterly audit: chart-to-auth alignment, payer mix and concentration, denial pattern review, routing audit, and contract pipeline review. The five-review structure is what surfaces payer rule changes before they become recoupment letters.
- Three symptoms tell you the current checklist has been outgrown: denial rate stagnation, AR aging drift (60 → 90 → 120 days), and surprise audit letters. Any one is a signal; two together means the checklist is being used as a form, not a working operational document.
This guide walks through what each phase actually contains, what changes as a treatment center grows, and how to spot when the current checklist is no longer holding the operation up.
Phase 1: The setup checklist
The setup checklist verifies every billing-relevant configuration before the first claim is submitted. This is the work most billing companies skip and most operators do not know to ask about.
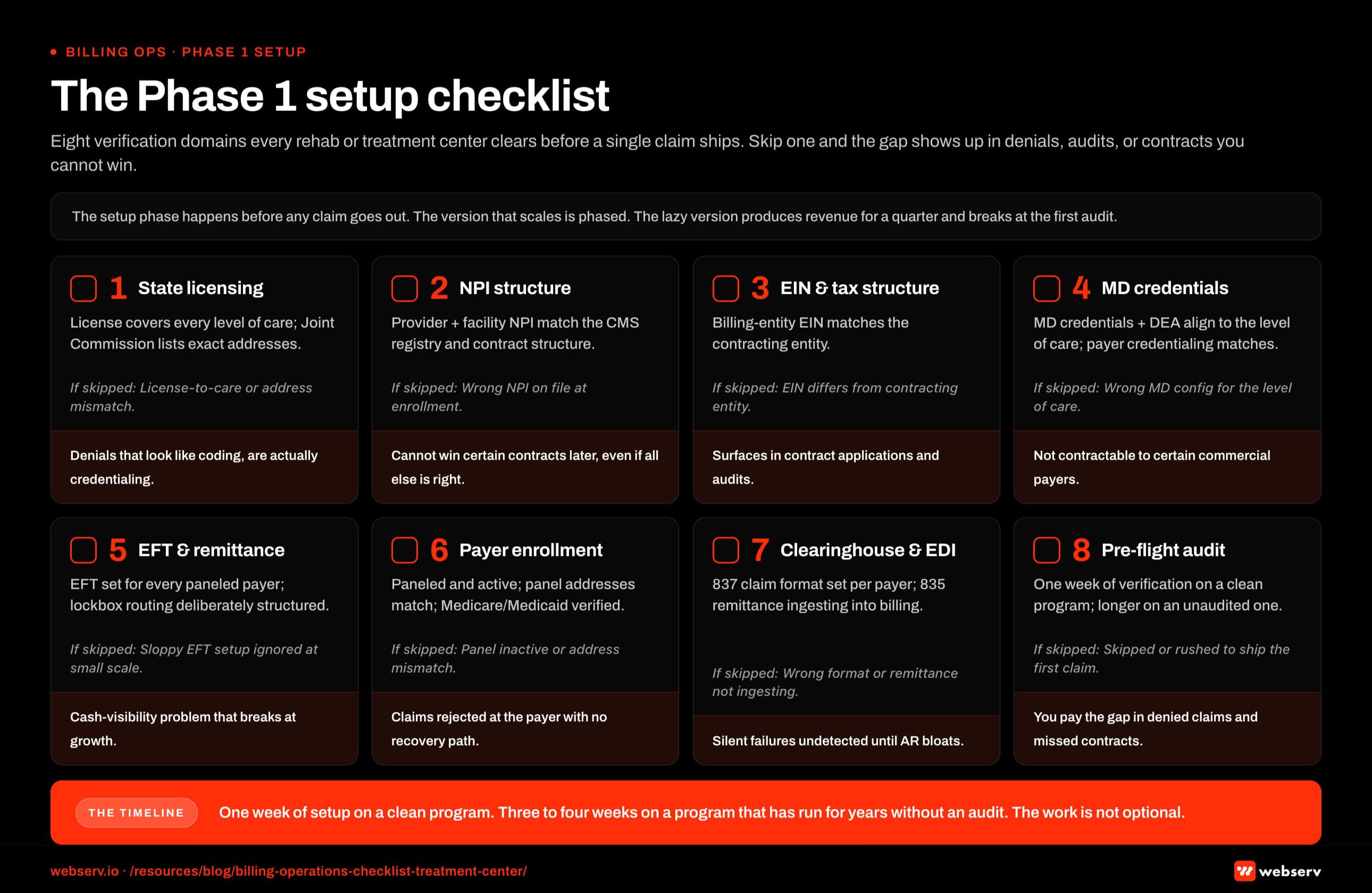 Infographic titled ‘The Phase 1 setup checklist’ showing the eight verification domains a rehab or treatment center must clear before its first billing claim is submitted, structured as a checklist grid laid out as four columns by two rows in landscape orientation. Each domain renders as a card with an empty check-box icon, a domain number in brand red, a domain name in bold, a one-line description of what gets verified, the failure mode that surfaces if the domain is skipped, and a consequence label running along the bottom of the card. Domain 1, state licensing and certification: verifies that the state license covers every level of care the program intends to bill and that the Joint Commission accreditation lists the exact physical addresses of every location; if skipped, the license does not match the level of care on the claim header or the address mismatches on the accreditation file; the consequence is denials that look like coding problems but are actually credentialing problems. Domain 2, NPI structure: verifies that the provider NPI and the facility NPI are configured correctly for the level of care being billed and the contract structure the program wants to pursue and that the record matches the CMS NPI Registry; if skipped, the wrong NPI configuration sits on file at panel enrollment; the consequence is the program cannot get certain contracts later even if every other condition is met. Domain 3, EIN and tax structure: verifies that the EIN tied to the billing entity matches the contracting entity; if skipped, the billing entity EIN differs from the contracting entity; the consequence surfaces during contract applications and audits, both expensive places to find a problem. Domain 4, MD credentials: verifies that the medical director credentials and DEA registrations align with the level of care delivered and that Joint Commission and payer credentialing matches are in place; if skipped, the wrong MD configuration sits for the level of care; the consequence is the program is not contractable to certain commercial payers tomorrow. Domain 5, EFT and remittance routing: verifies that electronic funds transfer is configured for every paneled payer and that lockbox routing for any paper checks is deliberately structured; if skipped, sloppy EFT setup at small scale gets ignored until cash visibility breaks; the consequence is a cash visibility problem at growth that nobody scoped during setup. Domain 6, payer enrollment status: verifies that the program is paneled with every commercial payer it intends to bill, that the panels are active, that the panel addresses match the credentialing addresses, and that Medicare and Medicaid enrollment are verified if applicable; if skipped, the panel is inactive, the address mismatches, or the panel is missing entirely; the consequence is claims rejected at the payer with no recovery path until the panel is fixed. Domain 7, clearinghouse and EDI setup: verifies that the 837 claim file format is configured for each payer and that the 835 remittance file is ingesting into the billing system; if skipped, the EDI file format is wrong or the remittance is not ingesting; the consequence is silent failure modes that go undetected until AR bloats. Domain 8, the pre-flight audit window itself: confirms one week of verification on a clean program and three to four weeks on a program that has been running without an audit; if skipped or rushed to ship the first claim faster, the program pays for the gap in denied claims and missed contracts. Top banner callout: the setup phase happens before any claim goes out, the version that scales is a phased operations checklist, and the lazy version produces revenue for a quarter and breaks at the first audit. Bottom strip callout: one week of setup work on a clean program, three to four weeks on a program that has been running for years without an audit, and the work is not optional.
Infographic titled ‘The Phase 1 setup checklist’ showing the eight verification domains a rehab or treatment center must clear before its first billing claim is submitted, structured as a checklist grid laid out as four columns by two rows in landscape orientation. Each domain renders as a card with an empty check-box icon, a domain number in brand red, a domain name in bold, a one-line description of what gets verified, the failure mode that surfaces if the domain is skipped, and a consequence label running along the bottom of the card. Domain 1, state licensing and certification: verifies that the state license covers every level of care the program intends to bill and that the Joint Commission accreditation lists the exact physical addresses of every location; if skipped, the license does not match the level of care on the claim header or the address mismatches on the accreditation file; the consequence is denials that look like coding problems but are actually credentialing problems. Domain 2, NPI structure: verifies that the provider NPI and the facility NPI are configured correctly for the level of care being billed and the contract structure the program wants to pursue and that the record matches the CMS NPI Registry; if skipped, the wrong NPI configuration sits on file at panel enrollment; the consequence is the program cannot get certain contracts later even if every other condition is met. Domain 3, EIN and tax structure: verifies that the EIN tied to the billing entity matches the contracting entity; if skipped, the billing entity EIN differs from the contracting entity; the consequence surfaces during contract applications and audits, both expensive places to find a problem. Domain 4, MD credentials: verifies that the medical director credentials and DEA registrations align with the level of care delivered and that Joint Commission and payer credentialing matches are in place; if skipped, the wrong MD configuration sits for the level of care; the consequence is the program is not contractable to certain commercial payers tomorrow. Domain 5, EFT and remittance routing: verifies that electronic funds transfer is configured for every paneled payer and that lockbox routing for any paper checks is deliberately structured; if skipped, sloppy EFT setup at small scale gets ignored until cash visibility breaks; the consequence is a cash visibility problem at growth that nobody scoped during setup. Domain 6, payer enrollment status: verifies that the program is paneled with every commercial payer it intends to bill, that the panels are active, that the panel addresses match the credentialing addresses, and that Medicare and Medicaid enrollment are verified if applicable; if skipped, the panel is inactive, the address mismatches, or the panel is missing entirely; the consequence is claims rejected at the payer with no recovery path until the panel is fixed. Domain 7, clearinghouse and EDI setup: verifies that the 837 claim file format is configured for each payer and that the 835 remittance file is ingesting into the billing system; if skipped, the EDI file format is wrong or the remittance is not ingesting; the consequence is silent failure modes that go undetected until AR bloats. Domain 8, the pre-flight audit window itself: confirms one week of verification on a clean program and three to four weeks on a program that has been running without an audit; if skipped or rushed to ship the first claim faster, the program pays for the gap in denied claims and missed contracts. Top banner callout: the setup phase happens before any claim goes out, the version that scales is a phased operations checklist, and the lazy version produces revenue for a quarter and breaks at the first audit. Bottom strip callout: one week of setup work on a clean program, three to four weeks on a program that has been running for years without an audit, and the work is not optional.State licensing and certification. The state license must cover every level of care the program intends to bill. The Joint Commission accreditation must list the exact physical addresses of every location.
A mismatch between any of these and the claim header will trigger denials that look like coding problems but are actually credentialing problems.
NPI structure. The provider NPI and the facility NPI need to be configured correctly for the level of care being billed and the contract structure the program wants to pursue in the future. Both should be verified against the CMS NPI Registry so the provider record matches the entity actually delivering care.
A program with the wrong NPI structure today cannot get certain contracts later, even if every other condition is met.
EIN and tax structure. The EIN tied to the billing entity needs to match the contracting entity. Misalignment here surfaces during contract applications and during audits, both of which are expensive places to find a problem.
MD credentials. The medical director’s credentials and DEA registrations need to align with the level of care being delivered. Joint Commission and many payers require a specific credentialing match. A program with the wrong MD configuration today is not contractable to certain commercial payers tomorrow.
EFT and remittance routing. Electronic funds transfer needs to be configured for every payer the program is paneled with. Lockbox routing for any paper checks should be deliberately structured. Both can be sloppy at smaller scale and become a serious cash visibility problem at growth.
Payer enrollment status. Verify that the program is paneled with every commercial payer it intends to bill, that the panels are active, and that the panel addresses match the credentialing addresses on file. Verify Medicare and Medicaid enrollment if applicable.
Clearinghouse and EDI setup. The 837 claim file format needs to be configured for each payer the program submits to. The 835 remittance file should be ingesting into the billing system. Both are silent failure modes when set up wrong.
These items take a week of work to verify on a clean program and three to four weeks on a program that has been running for years without an audit. The work is not optional. Programs that skip it pay for the gap in denied claims and missed contracts.
Phase 2: The weekly operating rhythm
Once setup is verified, the weekly cadence begins. The weekly call between the billing partner and the program covers seven domains.
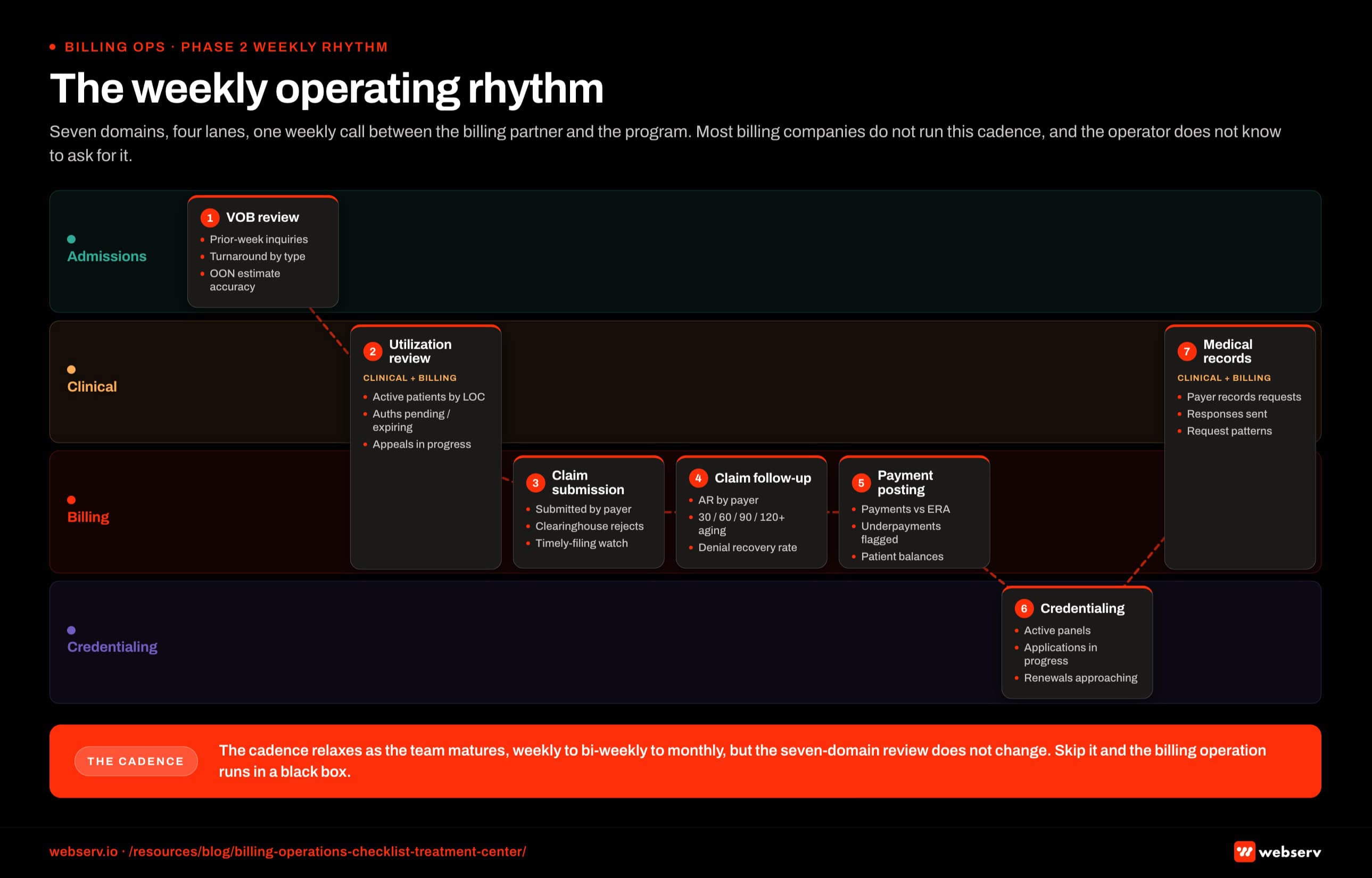 Infographic titled ‘The weekly operating rhythm’ showing the seven weekly operating domains a rehab or treatment center billing operation reviews every week, structured as a horizontal swim-lane diagram with four functional lanes stacked vertically and labeled Admissions, Clinical, Billing, and Credentialing from top to bottom. Seven domain cards sit across the lanes in cadence order from left to right, with arrows between cards showing the handoff direction. Domain 1, VOB review, sits in the Admissions lane and covers every patient inquiry from the prior week, turnaround times by inquiry type, out-of-network estimate accuracy compared to actual reimbursement, and payer behavior shifts the team flagged. Domain 2, utilization review status, spans the Clinical and Billing lanes and covers every active patient at every level of care, pending authorizations, authorizations approaching expiration, denial appeals in progress, UR specialist coverage, and payer-specific notes from the week. Domain 3, claim submission status, sits in the Billing lane and covers claims submitted in the last week by payer, claims rejected at the clearinghouse and re-routed, claims pending payer response, and claims approaching timely filing limits. Domain 4, claim follow-up, sits in the Billing lane and covers outstanding AR by payer, claims aged 30, 60, 90, and 120 or more days, recovery rate on denied claims, and patterns surfacing in denial reasons. Domain 5, payment posting, sits in the Billing lane and covers payments received in the last week, posting accuracy compared to ERA, underpayments flagged for appeal, and patient balance status. Domain 6, credentialing, sits in the Credentialing lane and covers active panels, credentialing applications in progress, credentialing renewals approaching, and provider terminations or additions. Domain 7, medical records evaluations, spans the Clinical and Billing lanes and covers records requests received from payers, records requests responded to, outstanding records requests with deadlines, and patterns in what specific payers are requesting. Admissions lane callout: VOB is the front door to every downstream billing metric and a weak VOB layer breaks every metric that follows. Clinical-Billing seam callout: utilization review and medical records sit at the clinical-billing seam, and these are the two domains where ownership confusion most often produces gaps. Card 4 callout: claim follow-up is where AR aging drift starts, and if 60-day claims are turning into 90-day claims the weekly follow-up is not moving the work fast enough. Bottom strip callout: the cadence relaxes as the team matures so weekly becomes bi-weekly and sometimes monthly, but the seven-domain review does not change, and the result of skipping it is a billing operation in a black box and an operator who finds out about problems three months after they started.
Infographic titled ‘The weekly operating rhythm’ showing the seven weekly operating domains a rehab or treatment center billing operation reviews every week, structured as a horizontal swim-lane diagram with four functional lanes stacked vertically and labeled Admissions, Clinical, Billing, and Credentialing from top to bottom. Seven domain cards sit across the lanes in cadence order from left to right, with arrows between cards showing the handoff direction. Domain 1, VOB review, sits in the Admissions lane and covers every patient inquiry from the prior week, turnaround times by inquiry type, out-of-network estimate accuracy compared to actual reimbursement, and payer behavior shifts the team flagged. Domain 2, utilization review status, spans the Clinical and Billing lanes and covers every active patient at every level of care, pending authorizations, authorizations approaching expiration, denial appeals in progress, UR specialist coverage, and payer-specific notes from the week. Domain 3, claim submission status, sits in the Billing lane and covers claims submitted in the last week by payer, claims rejected at the clearinghouse and re-routed, claims pending payer response, and claims approaching timely filing limits. Domain 4, claim follow-up, sits in the Billing lane and covers outstanding AR by payer, claims aged 30, 60, 90, and 120 or more days, recovery rate on denied claims, and patterns surfacing in denial reasons. Domain 5, payment posting, sits in the Billing lane and covers payments received in the last week, posting accuracy compared to ERA, underpayments flagged for appeal, and patient balance status. Domain 6, credentialing, sits in the Credentialing lane and covers active panels, credentialing applications in progress, credentialing renewals approaching, and provider terminations or additions. Domain 7, medical records evaluations, spans the Clinical and Billing lanes and covers records requests received from payers, records requests responded to, outstanding records requests with deadlines, and patterns in what specific payers are requesting. Admissions lane callout: VOB is the front door to every downstream billing metric and a weak VOB layer breaks every metric that follows. Clinical-Billing seam callout: utilization review and medical records sit at the clinical-billing seam, and these are the two domains where ownership confusion most often produces gaps. Card 4 callout: claim follow-up is where AR aging drift starts, and if 60-day claims are turning into 90-day claims the weekly follow-up is not moving the work fast enough. Bottom strip callout: the cadence relaxes as the team matures so weekly becomes bi-weekly and sometimes monthly, but the seven-domain review does not change, and the result of skipping it is a billing operation in a black box and an operator who finds out about problems three months after they started.VOB review. Every patient inquiry from the prior week. Turnaround times by inquiry type. Out-of-network estimate accuracy compared to actual reimbursement. Any payer behavior shifts the team flagged. The cadence is the same one I walked through in the VOB explainer — verification is the front door to every downstream billing metric.
Utilization review status. Every active patient at every level of care. Pending authorizations. Authorizations approaching expiration. Denial appeals in progress. UR specialist coverage and payer-specific notes from the week. The deeper mechanics live in the prior authorization playbook.
Claim submission status. Claims submitted in the last week by payer. Claims rejected at the clearinghouse and re-routed. Claims pending payer response. Claims approaching timely filing limits.
Claim follow-up. Outstanding AR by payer. Claims aged 30, 60, 90, 120+ days. Recovery rate on denied claims. Patterns surfacing in the denial reasons. The full pattern-detection layer is in reducing claim denials in behavioral health.
Payment posting. Payments received in the last week. Posting accuracy compared to ERA. Underpayments flagged for appeal. Patient balance status.
Credentialing. Active panels. Credentialing applications in progress. Credentialing renewals approaching. Provider terminations or additions.
Medical records evaluations. Records requests received from payers. Records requests responded to. Outstanding records requests with deadlines. Patterns in what specific payers are requesting.
These seven domains are the basic content of every weekly call we have with every client. The cadence reduces over time as the operator’s understanding deepens and the team’s interface with the workflow becomes routine.
It does not stop. It moves from weekly to bi-weekly, sometimes to monthly, but the seven-domain review remains.
Most billing companies do not run this cadence. The operator does not know to ask for it. The result is a program where billing is operating in a black box and the operator finds out about problems three months after they started.
Phase 3: The quarterly audit
Four times a year, the billing operation runs against the live portfolio in a different way. The weekly cadence is forward-looking. The quarterly audit is backward-looking.
Chart-to-auth alignment audit. Pull a sample of recent authorizations. Read the clinical notes that supported each one. Confirm a UR specialist could have built the auth from the documentation in the chart. Flag any gaps for clinical team follow-up.
Payer mix and concentration review. What share of revenue came from the top three payers in the last 90 days? What share from the top one? Have any payers exited or restructured? Is the concentration moving in the right direction? The longer arc lives in the payer mix strategy guide.
Denial pattern review. Aggregate denials by payer, denial reason code, and recovery rate. Identify clusters that suggest payer rule changes. Flag any code-set or criteria shifts that need a workflow response.
Routing audit. Confirm every active payer is being billed into the workflow that payer expects. Identify any payers being submitted to incorrectly that need to move to member submission, TPA routing, or balance billing.
Contract pipeline review. What contracts are coming up for renewal? What new contracts are being pursued? What credentialing work needs to happen in the next 90 days to support the contract pipeline?
These five reviews together give the operator a complete view of what is and is not working in the billing operation, and what is changing in the surrounding payer landscape that the program needs to adapt to.
Phase 4: How the checklist changes as the program grows
The setup, weekly, and quarterly phases above are common across most behavioral health programs. The specifics shift as the program scales.
At a single-location program with low admit volume, the weekly cadence can run on a single 60-minute call with the billing partner, the operator, and one clinical lead.
The quarterly audit can be light because the portfolio is small. The setup checklist needs to be airtight because there is no margin to absorb an error at low volume.
At a multi-location regional program, the weekly cadence often splits by location and by level of care. The operator delegates to a clinical director or admissions director who carries the weekly call on their behalf.
The quarterly audit becomes a more substantial document with cross-location patterns. New credentialing work for additional locations becomes a steady-state activity rather than a one-time event.
At a multi-state organization, the cadence has to scale into a structured reporting infrastructure. Each location has its own weekly review with a regional billing lead.
Cross-organization rollups go to the operator monthly. The quarterly audit becomes a board-level document that informs strategic decisions about market expansion and payer strategy. The framing that informs those decisions sits squarely in the Healthcare Financial Management Association‘s revenue cycle benchmarks — the same metrics commercial operators in other healthcare verticals are reporting against.
The threshold details, exact admit volumes, exact cadence frequencies, and exact reporting structures are program-specific and should be calibrated with a billing partner who knows the operation. The principle is constant: as census grows, the checklist does not get simpler. It gets more deliberate.
How a Tennessee treatment center tripled its paid media close rate and cut missed calls to 1%
Full CRM configuration, system integrations, and call tracking metrics unified a fragmented admissions process into a single high-converting workflow in two months.
Read the case study →Up from 17% — missed calls cut from 15% to 1%
Signs your current checklist is not holding up
Three patterns surface when the billing operations checklist has been outgrown by the program. Watch for these.
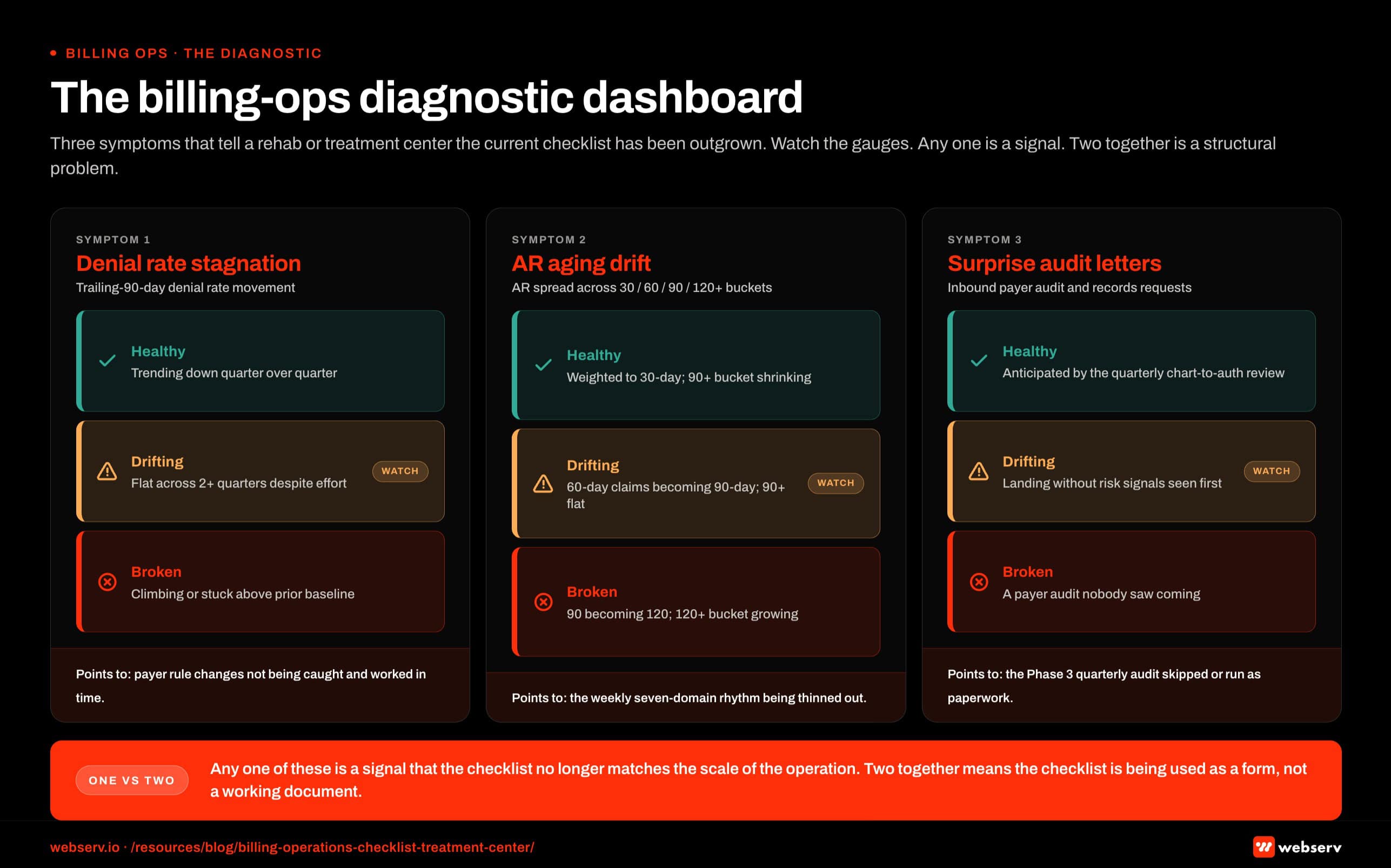 Infographic titled ‘The billing-ops diagnostic dashboard’ showing three diagnostic symptoms that tell a rehab or treatment center operator the current billing operations checklist has been outgrown by the program, structured as three vertical gauge cards arranged side by side in landscape orientation. Each card carries a symptom name in brand red at the top, the metric tracked beneath it, a horizontal traffic-light gauge with green healthy, amber drifting, and red broken zones, a three-line operational interpretation of the symptom, and a bottom strip naming the underlying checklist failure the symptom points at. Card 1, denial rate stagnation, tracks trailing-90-day denial rate movement; the healthy zone is denial rate trending down quarter over quarter, the drifting zone is denial rate flat across two or more quarters despite operational effort, the broken zone is denial rate climbing or stuck above the prior baseline; the meaning is that the weekly review is happening but the quarterly pattern detection is not, and the underlying checklist failure is payer rule changes not being caught and worked in time. Card 2, AR aging drift, tracks the distribution of accounts receivable across the 30, 60, 90, and 120 plus day buckets; the healthy zone is aging weighted to the 30-day bucket with the 90 plus bucket shrinking, the drifting zone is 60-day claims turning into 90-day claims and the 90 plus bucket holding flat, the broken zone is 90 turning into 120 and the 120 plus bucket growing; the meaning is that the weekly follow-up cadence is not moving the work fast enough or the team is working only the easy claims and letting the rest sit, and the underlying checklist failure is the Phase 2 weekly cadence being degraded or the seven-domain rhythm being thinned out. Card 3, surprise audit letters, tracks inbound payer audit requests and records requests; the healthy zone is audit requests anticipated by the quarterly chart-to-auth review and worked proactively, the drifting zone is audit requests landing without the team having seen risk signals first, the broken zone is a payer initiating an audit with nobody on the program seeing it coming; the meaning is that the chart-to-auth alignment audit is not happening at the cadence the program needs, and the underlying checklist failure is the Phase 3 quarterly audit being skipped or run as a documentation exercise. Card 1 callout: a flat denial rate is not stability, it is stalled pattern detection, and payer rule changes are accumulating in the data and not getting worked into the workflow. Card 2 callout: AR aging drift is the most visible early warning, operators can see this one on the AR report any week, and most miss it because they look at total AR rather than the bucket distribution. Card 3 callout: surprise audit letters are the latest warning, the most expensive to fix, and the most preventable, and the chart-to-auth audit is what catches the risk signals before they become recoupment letters. Bottom band callout: any one of these is a signal that the current checklist is not matching the scale of the operation, and two together is a signal that the checklist is being used as a form rather than as a working operational document.
Infographic titled ‘The billing-ops diagnostic dashboard’ showing three diagnostic symptoms that tell a rehab or treatment center operator the current billing operations checklist has been outgrown by the program, structured as three vertical gauge cards arranged side by side in landscape orientation. Each card carries a symptom name in brand red at the top, the metric tracked beneath it, a horizontal traffic-light gauge with green healthy, amber drifting, and red broken zones, a three-line operational interpretation of the symptom, and a bottom strip naming the underlying checklist failure the symptom points at. Card 1, denial rate stagnation, tracks trailing-90-day denial rate movement; the healthy zone is denial rate trending down quarter over quarter, the drifting zone is denial rate flat across two or more quarters despite operational effort, the broken zone is denial rate climbing or stuck above the prior baseline; the meaning is that the weekly review is happening but the quarterly pattern detection is not, and the underlying checklist failure is payer rule changes not being caught and worked in time. Card 2, AR aging drift, tracks the distribution of accounts receivable across the 30, 60, 90, and 120 plus day buckets; the healthy zone is aging weighted to the 30-day bucket with the 90 plus bucket shrinking, the drifting zone is 60-day claims turning into 90-day claims and the 90 plus bucket holding flat, the broken zone is 90 turning into 120 and the 120 plus bucket growing; the meaning is that the weekly follow-up cadence is not moving the work fast enough or the team is working only the easy claims and letting the rest sit, and the underlying checklist failure is the Phase 2 weekly cadence being degraded or the seven-domain rhythm being thinned out. Card 3, surprise audit letters, tracks inbound payer audit requests and records requests; the healthy zone is audit requests anticipated by the quarterly chart-to-auth review and worked proactively, the drifting zone is audit requests landing without the team having seen risk signals first, the broken zone is a payer initiating an audit with nobody on the program seeing it coming; the meaning is that the chart-to-auth alignment audit is not happening at the cadence the program needs, and the underlying checklist failure is the Phase 3 quarterly audit being skipped or run as a documentation exercise. Card 1 callout: a flat denial rate is not stability, it is stalled pattern detection, and payer rule changes are accumulating in the data and not getting worked into the workflow. Card 2 callout: AR aging drift is the most visible early warning, operators can see this one on the AR report any week, and most miss it because they look at total AR rather than the bucket distribution. Card 3 callout: surprise audit letters are the latest warning, the most expensive to fix, and the most preventable, and the chart-to-auth audit is what catches the risk signals before they become recoupment letters. Bottom band callout: any one of these is a signal that the current checklist is not matching the scale of the operation, and two together is a signal that the checklist is being used as a form rather than as a working operational document.Denial rate stagnation. Despite operational effort, the denial rate is not moving. This usually means the weekly review is happening but the quarterly pattern detection is not, so payer rule changes are not being caught and worked.
AR aging drift. Outstanding receivables are creeping up by aging bucket. 60-day claims are turning into 90-day claims and 90 into 120. The weekly follow-up cadence is not moving the work fast enough, or the team is working only the easy claims and letting the rest sit.
Surprise audit letters. A payer requests medical records or initiates an audit, and nobody on the program saw it coming. The chart-to-auth alignment audit is not happening at the cadence the program needs, and the audit risk has been quietly accumulating.
Any one of these is a signal that the current checklist is not matching the scale of the operation. Two together is a signal that the checklist is being used as a form rather than as a working operational document.
Frequently asked questions about treatment center billing operations checklists
How often should we audit our billing operations checklist?
The checklist should be audited quarterly at minimum, with monthly review of the weekly operating rhythm items. Payer behavior changes faster than most operators expect. Code-set updates from UnitedHealthcare, Aetna, BCBS, and Cigna come without advance notice, and a checklist that worked perfectly six months ago can have multiple stale line items today.
The quarterly audit covers four things: which line items consistently produce the highest yield (and should be expanded), which line items rarely produce findings (and should be deprioritized), which payer-specific patterns have shifted and require new line items, and which staff capabilities have changed enough to affect ownership assignments.
Programs that audit annually or less frequently typically have checklists that look good on paper and miss the issues that actually move revenue. The audit cadence is what separates a working operational tool from a documentation artifact that nobody references.
What is the right ratio of in-house to outsourced billing roles?
Most treatment centers under 30 beds outsource all billing roles. Most centers between 30 and 80 beds run a hybrid model with in-house VOB and UR plus outsourced claim submission, denial management, and collections. Most centers above 80 beds can support more in-house roles, but the highest-return layers (claim submission, denial appeals, payer relationship management) typically stay outsourced because the specialist expertise is hard to staff at facility scale.
The variable that matters more than headcount is which roles are aligned with the operational checklist. A billing operation where the in-house team owns intake-to-VOB and the outsourced team owns submission-to-collection works well when the handoff is clean. A billing operation with overlapping ownership or unclear handoffs produces gaps regardless of how the headcount splits.
Programs we work with that have switched ratios usually moved in the in-house direction over time as scale produced the case for it. The reverse (moving from in-house to outsourced) is rare and usually indicates the in-house operation was producing worse results than the operator thought.
How do we know if our billing partner is using a real operational checklist?
Three diagnostic questions surface most of the gap. First: can the partner walk you through their weekly operating rhythm in specifics, with named owners and decision points at each step? A specialist partner answers in operational detail. A vendor partner answers in generic capability language. Second: can the partner show you their checklist documentation, even in redacted form? Real checklists exist as documents that get referenced.
Third: what is the partner’s process when a checklist line item produces a finding? A specialist partner has a documented escalation pattern. A vendor partner usually has informal patterns that depend on the specific staff member who caught the issue. The first scales reliably. The second produces variance that compounds into revenue loss.
If you are already in an engagement, the request is direct: ask your billing partner to walk you through your facility’s specific checklist in the next call. The walkthrough reveals whether the system exists and is current, or whether it is an aspirational document. The latter is more common than operators expect.
What is the difference between a billing checklist and an RCM playbook?
The checklist is the line-by-line operational document the billing team uses week-to-week and quarter-to-quarter. The RCM playbook is the strategic document that explains why the operation is structured the way it is, which decisions get made by which roles, and how the operation should evolve as the program grows. The checklist is execution. The playbook is the strategic context the execution lives inside.
Most billing operations have a checklist of some kind. Fewer have a real playbook. The gap shows up in strategic decisions: when to push back on a payer, when to write off a class of claims, when to renegotiate a contract, when to add or drop in-network status. Without a playbook, those decisions get made on the operator’s intuition rather than on a documented framework.
The right pairing is a working checklist for day-to-day execution and a quarterly-reviewed playbook for strategic decisions. Most growing programs underinvest in the playbook because the checklist feels like enough. The playbook becomes necessary the moment the program scales past 50 beds or expands across multiple states with different payer mixes.
Can a treatment center under 30 beds run this checklist effectively?
Yes, with adaptations. Smaller programs need a leaner version of the checklist that consolidates ownership across fewer roles. A 20-bed program where the same staff member owns intake, VOB, and UR cannot run the same role-segmented checklist a 60-bed program uses. The work has to be sequenced rather than parallelized.
The biggest risk for smaller programs is checklist complexity that exceeds operational capacity. A checklist with 80 line items per week is unworkable for a billing operation with 1.5 FTE supporting it. The right adaptation reduces the checklist to 30 to 40 line items per week, prioritized by yield, with the lower-priority items running monthly or quarterly instead of weekly.
Programs under 30 beds also benefit from outsourced specialist support for the checklist items requiring depth (denial appeals, payer-specific code-set tracking, single-case agreement negotiation). The in-house team executes the daily and weekly checklist; the outsourced specialist handles the items that need expertise the in-house team cannot maintain at sub-FTE scale.
What this looks like in practice
The billing operations checklist is the operating control panel for the program. The version that scales is a phased system. It gets built once during onboarding, runs weekly thereafter, gets audited quarterly, and gets upgraded every time the program crosses a meaningful growth threshold.
The programs that treat the checklist this way grow with their census. The programs that treat the checklist as a back-office form hit a ceiling at the first scale where the work becomes complex enough to require structure.
Most operators do not see this until the ceiling becomes visible. The growth slows, the AR climbs, the denial rate sits flat. The cause is rarely a billing problem. The cause is usually a checklist problem.
If your current billing partner cannot show you the weekly cadence, the quarterly audit deliverables, and the setup verification documentation from your onboarding, the checklist is most likely not being run at the level the program needs.
That gap is closeable. The first quarter of a structured rebuild produces visible improvement in denial recovery, AR aging, and operator visibility. The full payoff lands in the second quarter, when the cadence has run long enough to surface the deeper payer patterns the previous setup was not catching. If you want to know what a structured rebuild would look like for your program, book an intro call and we can walk through the diligence framework before any retainer work begins.
The perspective in this article comes from 9 years working exclusively inside behavioral health.
We are a team built by people in recovery who understand that behind every admission is someone asking for help. If that resonates, get to know us.
Kyle McHenry is the founder of Revenue Logic, a behavioral health revenue cycle management firm. He has spent 15 years working with treatment center operators on verification, utilization review, and claims management. Webserv partners with Revenue Logic to surface RCM-side guidance for behavioral health admission operations.