A treatment center we audited last quarter had published 184 blog posts over 30 months. The posts averaged 850 words. The bylines all read “Editorial Team.”
The topics covered condition pages, modality explainers, level-of-care primers, and family-member resources. Total organic search traffic to the blog: 1,420 sessions per month. Total admit-attributed conversions from blog traffic over six months: zero.
A second treatment center we work with had published 23 blog posts over the same 30 months. The posts averaged 2,800 words.
Every byline named a credentialed clinician. Every post included reviewer credit, peer-reviewed citations, and structured author bios. Total organic search traffic to the blog: 9,100 sessions per month. Total admit-attributed conversions from blog traffic over six months: 47 admits.
The gap is not the volume. The gap is the system that produces clinical content Google trusts and that patients (and the family members who often search on their behalf) actually find.
Inside Webserv’s content SEO program for treatment centers, we run a clinical content production system that combines named clinical authorship, peer-reviewed citation discipline, condition-modality-level-of-care content architecture, and AI citation eligibility work into a single editorial cadence.
The system produces content that ranks, content that earns AI search citations across ChatGPT, Perplexity, Claude, and Google AI Overviews, and content that actually converts the family member at 11 PM into the inquiry call at 11:14.
This article walks through the full system in six pillars.
We cover why clinical content sits inside a stricter Google evaluation frame than almost any other category, what patients and family members actually search for in 2026, and the E-E-A-T system Google rewards.
We also cover the content architecture that compounds across a condition cluster, how AI citation eligibility works for clinical content, and the editorial production system that scales the work to 30 to 50 high-quality pieces per year without compromising clinical accuracy.
Key Takeaways
- Clinical content sits inside Google’s strictest evaluation frame. Healthcare YMYL pages get E-E-A-T evaluation at a higher threshold than almost any other category, and the September 2025 Quality Rater Guidelines update made authorship the single highest-impact compliance signal.
- Patient and family-member search behavior is shaped by stigma. People struggling with addiction often do not search “addiction treatment” or “rehab”; they search “how to stop drinking” or “feeling hopeless all the time.” Clinical content has to meet readers where their actual search vocabulary lives.
- Named clinical authorship is required. Every YMYL page on a treatment center site should have a named, credentialed author attached, with reviewer credit on every clinical claim. “Editorial Team” bylines actively undermine ranking and conversion.
- The content architecture that compounds is condition by modality by level of care by geography. Treatment centers that build pillar pages for each major condition, cluster pages for each modality, and leaf pages for each level-of-care variant produce topical authority that earns AI citation share across thousands of related queries.
- The 2026 production system requires editorial workflow, clinical reviewer integration, AI citation strategy, and measurement against admit-attributed conversions (not just sessions). Operators producing 30 to 50 high-quality pieces annually outperform operators producing 200+ low-quality pieces by every measure that matters.
Pillar 1: Why Clinical Content Is Different From Regular Health Content
The YMYL frame is the load-bearing context for everything in this article. Pages that affect a reader’s health, financial stability, or safety fall into Google’s “Your Money or Your Life” category, and addiction treatment plus mental health sit inside YMYL at the strictest threshold tier.
Three implications follow from the YMYL classification.
First, the E-E-A-T threshold is higher. Experience, Expertise, Authoritativeness, and Trustworthiness signals are evaluated more strictly for YMYL content.
A YMYL page with weak E-E-A-T signals is not just a ranking miss; it is treated as a potential safety issue.
The September 2025 Quality Rater Guidelines update extended this framework to AI Overviews, meaning the same E-E-A-T evaluation now governs AI citation eligibility alongside traditional ranking.
Second, the consequences of getting it wrong are larger. Google’s December 2025 Core Update produced sizable ranking changes on 67 percent of health-related websites per industry reporting, with E-E-A-T signals as the load-bearing differentiator.
Treatment centers running content marketing on a 2022 framework lost ranking position and AI citation share in measurable ways during that update.
Third, the audience is different from non-YMYL audiences. Patients in active addiction or mental health crisis, family members searching at 11 PM about a loved one’s overdose, referral sources looking for the right facility for a specific clinical presentation.
All of these audiences are time-pressured, emotionally activated, and applying their own version of E-E-A-T evaluation in the first 5 to 10 seconds on any page.
The content that works in this frame is structurally different from content that works in lower-stakes categories. The voice has to be more direct. The citations have to be peer-reviewed. The author has to be named and credentialed.
The compliance frame (42 CFR Part 2, HIPAA, LegitScript landing-page standards, Meta and Google healthcare advertising policies) has to be respected at the content level, not bolted on at review.
Treatment centers that treat clinical content as a marketing exercise and skip the YMYL frame produce content that fails on both ranking and conversion. Treatment centers that treat clinical content as a clinical credibility statement that happens to also serve a marketing function produce content that compounds across years.
We’ve covered the failure mode in depth in the case against generic healthcare content farms in addiction treatment, which is the long version of why “Editorial Team” content libraries lose ranking share even when the volume looks healthy on a content calendar.
Pillar 2: What Patients (and Family Members) Actually Search For
The search intent reality for behavioral health is different from what most marketing teams design content around. Three audience segments search differently, and stigma shapes vocabulary in ways that surprise operators new to the category.
Segment 1: The patient considering treatment. Patients in active substance use or mental health distress often do not search clinical terminology.
A person struggling with alcohol use disorder rarely searches “alcohol use disorder treatment options.” They search “how to stop drinking,” “why can’t I stop drinking,” or “feeling hopeless all the time.”
This stigma-shifted search vocabulary is the largest blind spot in most treatment center content libraries. Operators publishing service pages on “Alcohol Use Disorder Treatment” and “Substance Use Disorder Care” miss the search volume living in the patient-vocabulary equivalents.
Content that uses both registers (clinical terminology for credibility plus patient vocabulary for discoverability) wins both the ranking competition and the patient-trust competition.
Segment 2: The family member researching for someone else. Family members are increasingly the primary inquiry-driver in behavioral health paid social and organic content.
A mother searching for her 22-year-old son in active opioid use does not type “addiction treatment center.” She types “what to do when your child won’t stop using,” “best treatment for fentanyl addiction,” or “how to get someone into rehab.”
Family-member search vocabulary skews toward action-oriented and time-pressured language. “How to,” “what to expect,” “what to do when,” and “best for” framings dominate.
Content that addresses the family member directly (acknowledging the role, the crisis state, and the time pressure) outperforms content written as if the patient is the sole reader.
Segment 3: The referral source. Clinicians, therapists, EAP representatives, drug court coordinators, and other professional referrers search differently from patients and families. Their queries are clinical and operational: “ASAM criteria placement levels,” “PHP vs IOP outcomes,” “MAT-friendly residential treatment near me,” “facility for co-occurring eating disorders and SUD.”
Referral-source content is a different writing register and a different topic depth. It uses clinical terminology fully, cites peer-reviewed outcome research, and addresses operational questions the family-member content does not need to cover.
Treatment centers ignoring the referral-source segment leave a high-value, low-volume traffic source on the table.
The high-volume, high-intent searches that 2026 keyword research surfaces for behavioral health include phrases like “how to help someone with depression” (18,000+ monthly searches), “what to expect in rehab” (12,000+ monthly searches), and “online therapy covered by insurance” (22,000+ monthly searches).
All three use patient or family vocabulary rather than clinical terminology. Content built around these phrases, written by named clinicians, reviewed for accuracy, and addressed to the actual audience asking, earns both ranking and conversion.
Pillar 3: The E-E-A-T System Google Rewards
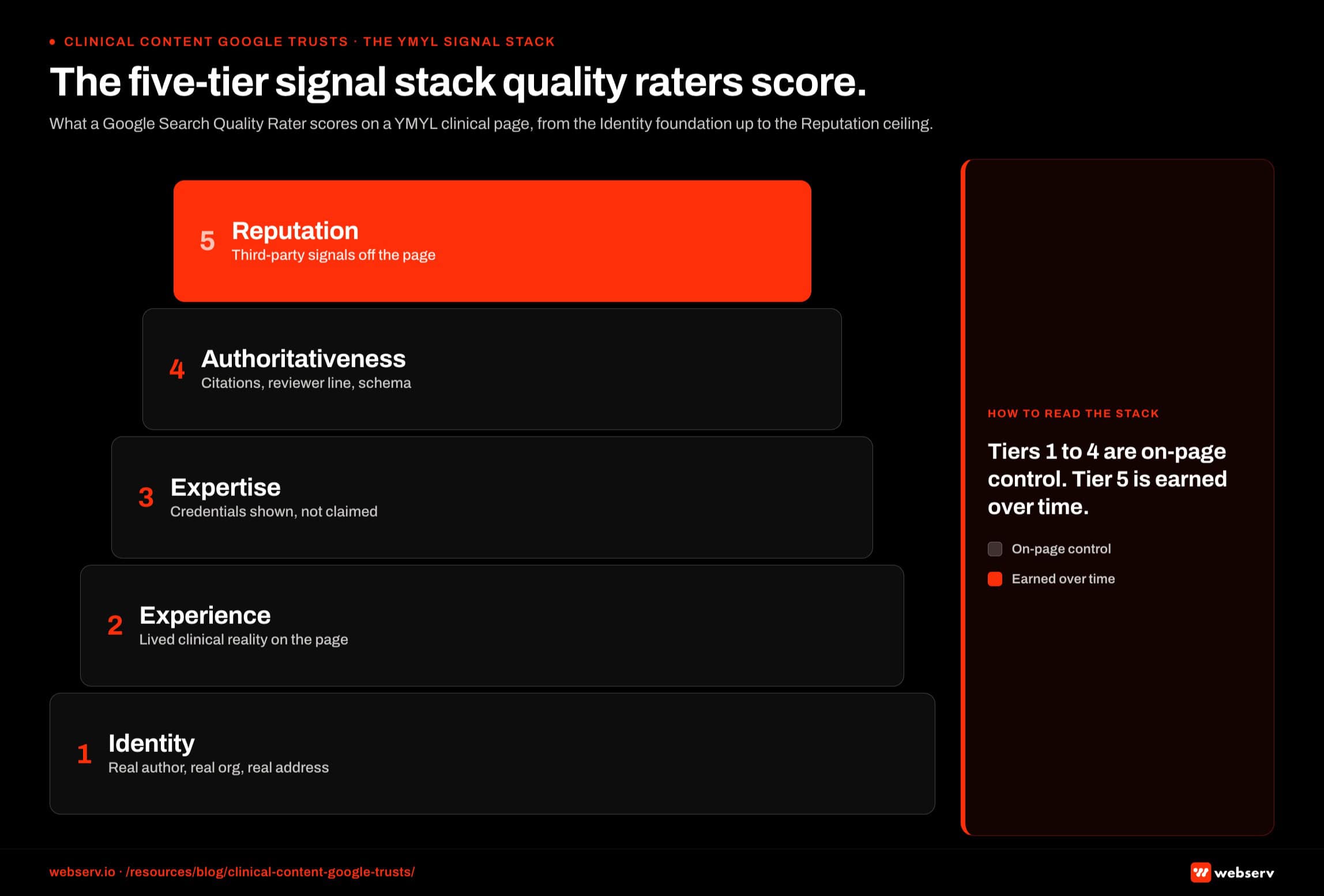
Building clinical content that Google trusts requires a system rather than a single tactic. Five components combine to produce the E-E-A-T signal Google evaluates.
Named clinical authorship. Every YMYL page on the site needs a named, credentialed author attached. The clinical director, chief medical officer, lead clinical therapist, or named subject-matter clinician at the facility should be the byline on clinical content, not “the editorial team” or the marketing director.
The author byline links to a structured bio page that includes credentials, licensing, sameAs links to professional registries (NPI, state licensing boards, professional society memberships), and a list of topics the author writes about.
Bylines that read “by Editorial Team” or “by [Facility Name] Staff” actively undermine E-E-A-T evaluation. Google’s quality raters explicitly look for named, credentialed authors on YMYL content. The absence of an attributable human author is a negative signal at scale.
Clinical reviewer credit. Every clinical content piece should have a second named credentialed reviewer alongside the author.
The reviewer signs off on clinical accuracy, with a visible “Clinically Reviewed by [Name, Credentials] on [Date]” line on the page. The reviewer’s bio page is structured the same way as the author’s.
The author-reviewer pairing serves three functions. It produces redundant clinical accuracy review. It signals to Google’s quality raters and AI search systems that the facility takes clinical credibility seriously.
It also spreads the credentialing surface area across more named clinicians, which compounds the entity-level E-E-A-T signal over time.
Peer-reviewed citations. Clinical claims need citations to peer-reviewed sources. SAMHSA, NIDA, NIMH, JAMA Psychiatry, peer-reviewed clinical journals, government data, and ASAM publications all carry citation weight.
Citations from non-peer-reviewed sources (other blog posts, press releases, undocumented stats) carry less weight and can undermine the page’s E-E-A-T evaluation if they replace peer-reviewed sources.
The citation format matters. Inline citations with hyperlinks to the source carry more weight than reference lists at the bottom of the page.
Citations attributing specific claims to specific sources carry more weight than general “according to research” framing. Direct quotes from named clinical researchers carry the most weight of any citation format.
Structured author and reviewer bios. Each named clinician on the site needs a dedicated bio page with structured information: education, credentials, licensing, areas of expertise, professional society memberships, sameAs links to NPI Registry and state licensing board records, headshot, and a list of articles authored or reviewed.
The bio pages are themselves YMYL content that Google evaluates for E-E-A-T signals.
The bio page strategy spreads E-E-A-T signal across the site. A treatment center with 6 to 10 named credentialed clinicians, each with a structured bio page, accumulates more topical authority than a treatment center with one CEO bio and no clinical attribution.
The bio pages also feed into AI search citation eligibility, since AI systems use named clinician bios as authority signals, which connects directly to the clinician-as-AEO-moat work.
Visible signals on every YMYL page. Author and reviewer attribution at the top of the page (not buried in the footer). Last-reviewed date visible. Citation links to peer-reviewed sources. Accreditation badges (JCAHO, CARF, LegitScript) in or near the hero area. Privacy and compliance notices accessible from the footer.
Each of these is an individual signal; their combined presence produces the trust gestalt Google rewards.
Pillar 4: The Content Architecture That Compounds
Building clinical content that Google trusts and patients find requires architectural discipline, not just individual page quality. The architecture that compounds for treatment centers follows a condition × modality × level of care × geography matrix.
Condition pillar pages anchor the architecture. A condition pillar (alcohol use disorder, opioid use disorder, anxiety disorders, depression, co-occurring disorders, eating disorders) is a 3,500 to 6,000 word page that covers the condition end-to-end.
That includes clinical definition, symptoms, prevalence data, common patient and family questions, treatment approaches, what to expect, and how the facility treats it. The condition pillar is the topical authority anchor for everything else.
Modality cluster pages sit one level below the condition pillars. Modality pages cover treatment approaches: medication-assisted treatment (MAT), cognitive behavioral therapy (CBT), dialectical behavior therapy (DBT), EMDR, trauma-informed care, family therapy, and group therapy.
Each modality page links back to relevant condition pillars and forward to specific level-of-care pages where the modality is delivered.
Level-of-care pages anchor the operational layer. Detox, residential, partial hospitalization (PHP), intensive outpatient (IOP), outpatient, sober living, and aftercare each get a dedicated page.
Each page covers what the level of care involves, who it fits, what the typical day looks like, and how insurance covers it, plus the facility-specific operational details.
Geographic and intent-modifier pages extend the architecture for local SEO. “Alcohol rehab in [city],” “PHP in [state],” “MAT-friendly residential in [region]” all become legitimate content targets when paired with real facility presence in the geography.
The intent-modifier pages link back through the modality and condition pillars to keep the topical authority signal coherent. Operators building thin geographic pages without real facility presence run into the doorway pages problem, which is a measurable ranking drag rather than a theoretical risk.
The architecture compounds because each new page strengthens the connected pages. A new piece on “EMDR for substance use disorder” links to the EMDR modality page, the substance use disorder condition pillar, the residential and PHP level-of-care pages where EMDR is delivered, and the relevant geographic pages.
Internal linking density rises across the cluster, which signals to Google that the site has topical authority across the behavioral health category rather than thin coverage of disconnected topics.
Topical authority for treatment centers is the broader cluster strategy this architecture lives inside. The connection between architecture and authority is the multiplier that converts individual page quality into category-level competitive advantage.
Operators who skip the architecture and publish one-off pages tied to whatever the marketing team felt like writing that quarter produce content that does not compound.
The same operator with the same writers producing the same volume but organized inside a condition-modality-level matrix produces 3 to 5 times the organic search traffic and AI citation share over a 24-month horizon.
Treatment centers that treat clinical content as a marketing exercise and skip the YMYL frame produce content that fails on both ranking and conversion. Treatment centers that treat clinical content as a clinical credibility statement that happens to also serve a marketing function produce content that compounds across years. The frame is the lever; the volume is downstream.
Preston Powell, CEO of Webserv
Pillar 5: AI Citation Eligibility for Clinical Content
The 2026 reality is that traditional Google ranking is no longer the only measurement that matters. ChatGPT, Perplexity, Claude, Gemini, and Google AI Overviews now intercept a real share of the queries that used to drive organic clicks.
Healthcare YMYL pages in particular are evaluated against an AI citation eligibility frame that overlaps with but is distinct from organic ranking.
Three mechanisms drive AI citation eligibility for clinical content.
The institutional citation lean. Per Profound’s 27-million-citation analysis from January 2026, the Healthcare and Life Sciences vertical citation mix runs 52 percent brand, 15 percent media, 30 percent institution, and 3 percent social.
The 30 percent institutional share is the highest of any tracked vertical. AI systems answering healthcare queries pull disproportionately from government sources, academic institutions, medical society publications, and peer-reviewed journals.
For treatment centers, this means clinical content that cites institutional sources (SAMHSA, NIDA, NIMH, ASAM) and is itself cited by institutional sources earns AI citation share at higher rates than content that lives only in the brand citation tier.
Building citation relationships with institutional sources (through Wikipedia mentions, peer-reviewed journal appearances, SAMHSA grant program visibility, and academic collaboration) compounds with the on-site authorship work.
Schema-driven entity verification. AI systems use structured data to disambiguate entities and verify the authority signals on a page. The deeper read on entity disambiguation lives in what entity SEO actually is and how it helps treatment centers get found in AI search.
Organization schema with stable @id, MedicalOrganization schema on the homepage, FAQPage schema on clinical content, and Speakable schema for assistant-tier queries all feed into the AI citation evaluation.
Pages with strong FAQ schema get cited 4 to 5 times more often than identical content without it based on 2026 measurement data.
The schema layer is the technical infrastructure that makes the authorship and citation work readable to AI systems. Operators who skip the schema layer leave authority signals on the table even when the human-readable content is strong.
Question-shaped content structure. AI systems extract the sentence that most cleanly answers the user’s query.
Clinical content that opens each section with a direct question-shaped answer in the first 40 to 60 words gets pulled into AI Overview citations at higher rates than content that buries the answer in context.
The structural change is not stylistic. It is the extraction pattern AI systems use to decide what to cite.
A page on “what to expect in detox” that opens with “Detox typically lasts 5 to 7 days for alcohol and 3 to 10 days for opioids, depending on use history” gets extracted into AI answer cards.
A page that opens with “When patients arrive at our facility for detoxification, they undergo a thorough intake process…” does not.
The full system for getting cited by ChatGPT, Perplexity, Claude, and Google AI Overviews extends the clinical content work into the AI citation eligibility frame specifically.
Pillar 6: The Production System That Scales
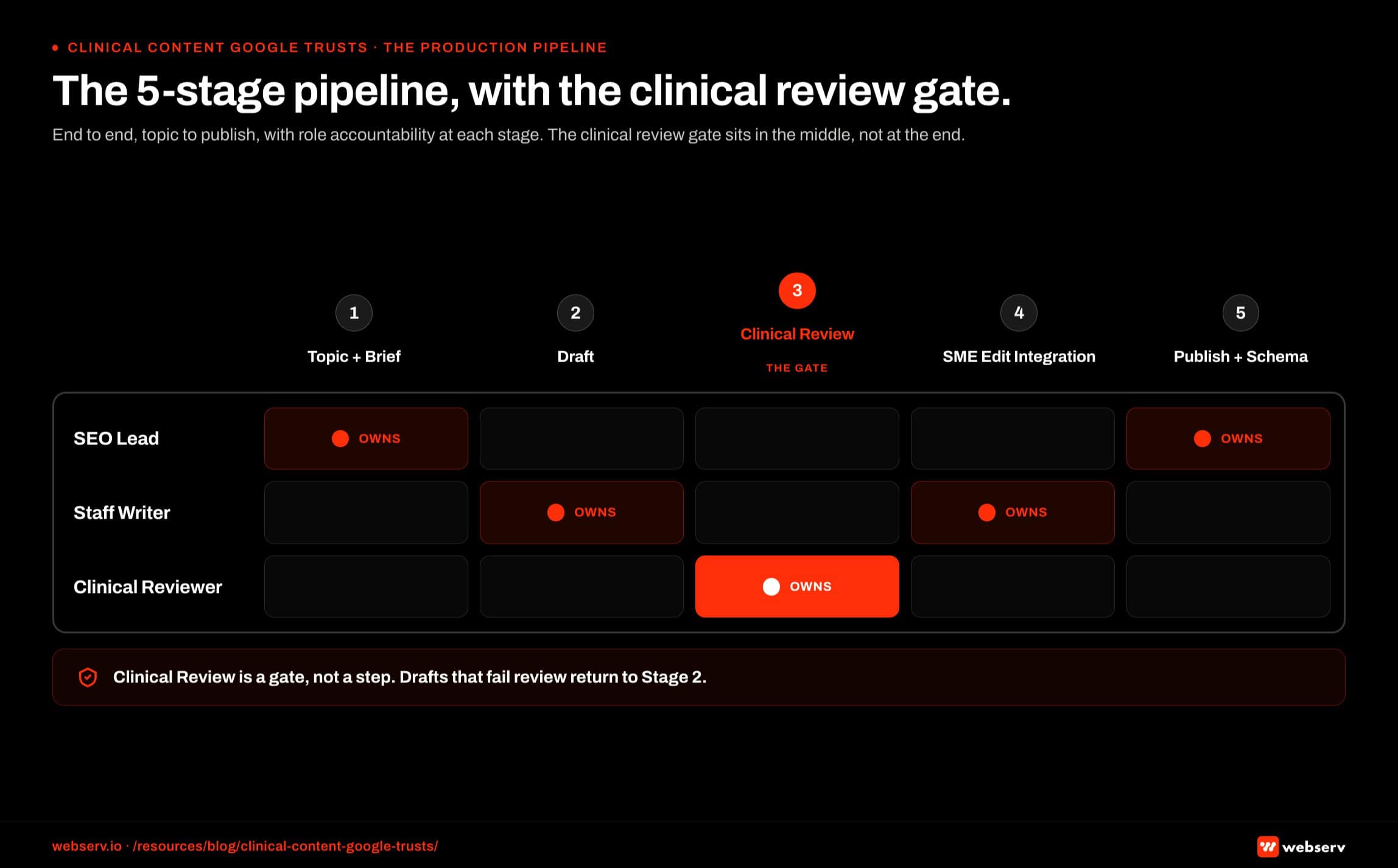
Building clinical content at the quality and cadence that produces ranking and AI citation requires a production system. The system has five components that work as a cohesive whole rather than as parallel work streams.
Editorial calendar grounded in keyword research and search intent. The calendar maps content topics to search volume, search intent, current ranking position, audience segment (patient, family, referral), and architecture position (condition pillar, modality cluster, level-of-care leaf, geographic intent).
Each piece on the calendar has a clear position in the architecture and a clear audience.
The calendar runs on a 90-day rolling horizon with quarterly strategic review. Topics are prioritized against three criteria: search volume opportunity, topical authority gap (what cluster pages need to be filled), and recent algorithm or AI search shifts.
The calendar does not optimize for volume; it optimizes for compound authority. The content gap analysis methodology is the input that keeps the calendar tied to actual cluster gaps rather than topic-of-the-week pitches.
Brief and outline framework for every piece. Every clinical content piece starts with a structured brief: target keyword, search intent, primary audience (patient, family, or referral), word count target, required citations, and required author and reviewer assignments.
The brief also names internal linking targets within the cluster, schema requirements, and success metrics. It is co-authored by the SEO lead and the clinical reviewer.
Outlines extend the brief into section-by-section structure. Each section gets a question-shaped answer, supporting evidence requirements, citation needs, and an internal link target.
The outline is the bridge between strategy (the brief) and execution (the draft), and it eliminates the back-and-forth that kills content production cadence.
Named clinical authorship with structured workflow. Each piece is assigned to a named clinician author and a named clinician reviewer.
The author drafts the clinical claims directly or works from a writer’s draft that the clinician then revises into clinically-accurate, voice-authentic prose. The reviewer signs off on clinical accuracy after the author approves the final draft.
The author-reviewer workflow requires clinician time, which is the primary production constraint for most treatment centers. Operators who try to scale clinical content without clinician participation produce content with “Editorial Team” bylines that underperform.
Operators who allocate 2 to 4 hours per piece of clinician time produce content that compounds in traffic, AI citation share, and admit-attributed conversion.
Compliance and clinical-accuracy review built into the workflow. Every clinical content piece passes through three review gates before publication: the author for clinical accuracy and voice, the reviewer for clinical accuracy second-pass, and the marketing or operations lead for brand voice, compliance language, and internal link integrity.
Each gate has a defined SLA and a documented sign-off.
The compliance review checks for 42 CFR Part 2 alignment (no identifiable patient stories, no implied patient testimonials), Meta and Google healthcare advertising policy alignment (no outcome promises, no claims that exceed evidence), and LegitScript landing-page standard alignment for any pages tied to paid traffic.
Measurement against admit-attributed conversions, not just sessions. The success metrics for clinical content are not session counts. They are admit-attributed conversions traced from content visit to inquiry to admission, with attribution lagged 60 to 120 days to allow for the behavioral health conversion cycle.
Sessions, time-on-page, and bounce rate are diagnostic metrics. Admits are the metric the system optimizes against.
Operators measuring content marketing on sessions alone optimize for volume that does not pay back. Operators measuring on admit attribution refine the architecture and the editorial calendar against the specific topics and audience segments that actually produce admits.
The measurement framework feeds back into the calendar for the next quarter, which is how the system compounds across years.
How to Sequence the Build

The six pillars are not parallel work streams. They sequence in five phases across the first 12 months of program build, with the work continuing past month 12 as compounding takes over.
Months 1-2: Author and reviewer infrastructure. Identify the 6 to 10 clinicians who will serve as named authors and reviewers across the cluster. Build their structured bio pages with credentials, sameAs links, and topic assignments. Stand up the author-reviewer workflow with defined SLAs and sign-off documentation.
This phase produces no published content, which is the part most operators want to skip. Skipping it means the content published in months 3 onward carries weaker E-E-A-T signals than it should and compounds slower.
Months 2-4: Condition pillar pages. Build the 4 to 6 condition pillar pages that anchor the architecture for the facility’s primary service lines. These are the longest, highest-investment pages on the site, typically 3,500 to 6,000 words each with the full author-reviewer workflow and peer-reviewed citation discipline.
The pillar pages take 30 to 45 days to build at quality. Publishing them too fast (before clinician review is complete) produces ranking and citation drag that takes a year to recover from.
Months 3-6: Modality cluster pages and level-of-care pages. Once the condition pillars are live, the modality and level-of-care pages can build out in parallel. Each new page links back to the relevant condition pillar and into the level-of-care and geographic pages where appropriate.
By end of month 6, the cluster typically has 15 to 25 pages live, with the architecture coherent enough that internal linking density starts producing meaningful topical authority compounding.
Months 4-8: Schema infrastructure and AI citation eligibility work. Organization schema with stable @id, MedicalOrganization on the homepage, FAQPage schema on every clinical page with FAQ blocks, Speakable schema for assistant-tier queries.
This phase also includes the question-shaped first-paragraph rewrites for the top pages, which produces measurable AI citation share lift within 4 to 8 weeks.
Months 6-12: Blog content cadence and measurement loop. Once the architectural pages are in place, the blog content cadence (4 to 6 pieces per month) fills out the cluster with longer-tail topics, family-vocabulary searches, and referral-source content.
The measurement loop (admit attribution, AI citation share tracking, organic ranking review) feeds back into the editorial calendar quarterly. By month 12, the system is producing compounding returns rather than linear output.
Quarter 4 and beyond: Refresh cycle and content gap closure. Existing pillar and cluster pages get refreshed on a 12 to 18 month cycle. Content gap analysis runs quarterly to identify cluster pages that should be added.
The system at this stage is not building from scratch. It is compounding what was built in months 1-12 by closing gaps and refreshing pages where new clinical data, AI search shifts, or competitive movement warrant it.
Operators who try to skip the early phases (start publishing blog content in month 2 before the author infrastructure is in place) produce content that does not compound. Operators who follow the sequence produce systems that pay back for years.
Frequently Asked Questions
How long should clinical content pieces be for treatment center websites?
Condition pillar pages run 3,500 to 6,000 words because they cover the condition end-to-end (definition, symptoms, prevalence, treatment approaches, what to expect, how the facility treats it). Modality cluster pages run 2,000 to 3,500 words to cover the treatment approach in depth without duplicating the condition pillar.
Level-of-care pages run 1,500 to 2,500 words. Geographic and intent-modifier pages run 1,000 to 2,000 words when they are tied to a real facility presence in the geography. Word count is the byproduct of complete answers, not the goal.
Pages that hit the word count by padding underperform pages that hit a shorter count with tight, named-clinician-authored prose. Pages that miss the word count by skipping sections underperform pages that fully cover the topic at length. Length follows substance.
How often should treatment centers publish new clinical content?
Four to six pieces per month is the operator-tested cadence sweet spot for treatment centers in 2026. That works out to 50 to 70 pieces annually across condition pillars, modality clusters, level-of-care pages, and blog content tied to the architecture.
Below 4 pieces per month, the content cadence does not produce enough topical authority compounding to outpace organic content drift. Above 6 pieces per month, clinician review bandwidth becomes the limiting constraint and content quality starts dropping, which produces content that underperforms even at higher volume.
The 4-to-6 cadence assumes clinical author and reviewer time is available at 2 to 4 hours per piece. Operators without that clinician bandwidth should reduce cadence to match available time rather than publish “Editorial Team” content to hit a volume target.
Should treatment centers use AI to write clinical content?
For drafting and outlining, yes. For final clinical claims, no. Google’s September 2025 Quality Rater Guidelines update explicitly treats AI-generated medical content with no human clinician review as a YMYL safety issue. AI-generated paragraphs making clinical claims without named clinician authorship disqualify the page from citation eligibility.
The right framing is that AI tools assist a credentialed clinician’s production. A clinician can use AI to draft an outline, generate first-pass prose for a section, or rewrite a passage in plainer language. The clinician then revises the AI output into clinically accurate, voice-authentic prose under their own byline.
Operators using AI to replace the clinician produce content that loses ranking position and AI citation share within 90 days. Operators using AI to amplify clinician productivity scale clinical content to the cadence that compounds across years.
What’s the realistic ROI timeline for clinical content marketing in 2026?
Six to nine months for organic ranking to start moving on new content. Twelve to 18 months for topical authority across a condition cluster to produce ranking on competitive head terms. Eighteen to 24 months for admit-attributed conversions from organic content to compound into a primary admit channel.
The timeline runs longer than most operators expect because behavioral health is a stricter YMYL category than most. New pages take longer to earn trust signals, and existing pages take longer to build the topical authority that lifts the whole cluster.
The SEO timeline reality for rehab websites covers the cycle in more detail. Operators planning content marketing on a 6-month ROI expectation are setting up for disappointment; operators planning on a 18-to-24-month compounding horizon produce content that pays back for years.
How do we measure whether our clinical content is actually working?
Three measurement layers matter. First, organic search performance: ranking position on target keywords, organic sessions, organic traffic to the cluster, and impression share on AI Overviews where it’s measurable.
Second, AI citation share: how often the facility’s domain or named clinicians appear in citations across ChatGPT, Perplexity, Claude, Gemini, and Google AI Overviews on prompts in the cluster. Most operators measure this with a monthly manual sampling protocol against 15 to 20 representative prompts plus a citation-tracking tool subscription.
Third, admit-attributed conversions: form-fills and phone calls from content visitors traced through the CRM to actual admits, lagged 60 to 120 days for the behavioral health conversion cycle. Sessions and time-on-page are diagnostic; admits are the metric the system optimizes against.
Do we need a content marketing agency to build this system, or can we run it in-house?
For most multi-facility operators, a hybrid model produces better outcomes than either pure in-house or pure agency for the first 24 months. The agency handles strategy, editorial calendar, briefs, SEO architecture, and AI citation work. The facility’s clinical team handles authorship and review.
The hybrid model lets the agency move at the cadence the architecture requires while keeping clinical credibility anchored in the facility’s own clinicians. Pure in-house works for operators with a senior SEO leader already on staff plus the clinician bandwidth to author and review. Pure agency without clinician participation produces “Editorial Team” content that underperforms.
After 24 months of compounding work, many operators converge on bringing more of the strategy and architecture in-house while keeping the agency on AI citation strategy, digital PR, and refresh cycles. The transition is normal and signals that the system is producing results.
Build a Clinical Content System That Compounds Across Years
Clinical content for treatment centers in 2026 is not a marketing exercise. It is a clinical credibility statement that happens to also serve a marketing function, evaluated by Google and AI search systems at the strictest YMYL threshold and read by family members in crisis at 11 PM.
The six-pillar system in this article produces clinical content that ranks on Google, earns AI citation share across ChatGPT, Perplexity, Claude, and Google AI Overviews, and converts inquiry traffic into admit-attributed pipeline that compounds over a 12 to 24 month horizon.
The 184-vs-23 case framing at the top of this article is not unusual. Operators publishing high volumes of “Editorial Team” content consistently underperform operators publishing fewer pieces of named-clinician-authored, peer-reviewed, architecturally-coherent content. The system is the lever; volume without the system is wasted effort.
We work with treatment center operators across the U.S. on the full clinical content production system: author infrastructure, condition cluster architecture, AI citation eligibility, schema infrastructure, editorial calendar, and the measurement loop that ties content back to admit pipeline.
Book an intro meeting to walk through your current clinical content profile, where the system gaps are likely costing you ranking and admit-attributed conversions, and what the first 12 months of system build would produce for your facility.
For the broader picture of how clinical content fits inside a full treatment center marketing program, see our ultimate guide to behavioral health marketing and our clinicians-as-AEO-moat framework for the deeper read on credentialed authorship as a competitive advantage.
Trevor Gage is the Director of Earned and Owned Media at Webserv, where he leads SEO, AEO, and digital PR for behavioral health and addiction treatment centers across the U.S. He writes about the cross-platform visibility work that earns treatment centers citation share in AI search alongside organic rankings and earned media coverage.