A treatment center marketing director called us last quarter for an audit. She had hired a healthcare-broad PR and advertising agency six months earlier on a $35,000 monthly retainer for paid social management. The agency had agency credentials, healthcare references, and a slick pitch deck.
Six months in, the facility had spent $210,000 on paid social. They had produced 47 admits.
Two of the three Meta ad accounts had been restricted. The creative library was 12 ads deep across all campaigns.
The audience targeting was set to “interest in addiction recovery,” which Meta started flagging in early 2026. The cost per admit had climbed from $2,800 to $5,100 month over month.
She asked us what she should have asked the agency before signing. The list was long.
Inside Webserv’s paid social program for treatment centers, we run the question-by-question vetting framework below whenever a multi-facility operator asks us to help evaluate competing agency proposals.
The 15 questions in this article group into four areas: specialization and credentials, compliance and platform policy, performance and measurement, and operational fit.
The questions are not theoretical. Each one is a question whose absence cost a real operator real admits in the last 24 months. This is the buyer’s vetting framework we wish she had when the contract went out.
Key Takeaways
- Hiring a paid social agency for a treatment center is one of the highest-stakes vendor decisions in behavioral health marketing. The right agency compounds across creative library, platform-policy relationships, audience stacks, and reporting integrations. The wrong agency costs 6 to 12 months of compressed admit volume, depleted creative inventory, ad account restrictions, and sometimes a LegitScript strike that follows the facility for years.
- The 15 questions below separate agencies who actually know behavioral health paid social from agencies who will learn on your dime. The questions cluster into four areas: specialization, compliance and platform policy, performance and measurement, and operational fit.
- Specialization is the load-bearing filter. Agencies running paid social for fewer than 3 active behavioral health clients today should be deprioritized regardless of how good their healthcare-broad portfolio looks. Behavioral health paid social is a separate discipline from healthcare PR or pharma paid media.
- Compliance fluency is a dealbreaker. LegitScript advertising eligibility, Meta Conversions API + 42 CFR Part 2 configuration, and Custom Audience SUD-signal handling are all areas where agency mistakes compound into ad account restrictions and platform-policy strikes that take quarters to recover from.
- The 90-day evaluation framework matters as much as the questions you ask up-front. The first 90 days predict the next 12. Set the measurement framework before campaigns go live so you can recognize the right and wrong patterns when they show up.
Why Hiring a Paid Social Agency for a Treatment Center Is Different
Paid social for a treatment center is not the same discipline as paid social for a consumer brand, a healthcare-broad provider, or a SaaS company. The compliance frame, the platform-policy reality, and the audience and creative constraints are all different in ways that compound on each other.
LegitScript advertising eligibility is the gating constraint for any treatment center running paid social. LegitScript Healthcare Merchant Certification is the de facto gatekeeper across Google, Meta, Microsoft, TikTok, LinkedIn, and Nextdoor for addiction treatment advertising.
An agency that doesn’t manage LegitScript application status, renewal cycles, and ad-account-level eligibility flags is an agency that will eventually have your ads pulled.
HIPAA and 42 CFR Part 2 compliance govern how ad data flows between the platforms and the facility’s CRM. 42 CFR Part 2’s February 2026 final compliance deadline tightened the rules on how SUD patient data can be shared.
Meta Conversions API and Custom Audience configurations need to be reviewed against the new compliance frame. Agencies operating on a 2023 compliance checklist are exposing the facility to enforcement risk they may not even recognize, which is the same gap covered in our HIPAA-compliant Facebook Ads guide.
Ad account restrictions happen more frequently in behavioral health than in almost any other vertical. Industry observation suggests 15 to 25 percent of behavioral health ad accounts experience at least one Meta or Google restriction event per year.
Recovery times range from 24 hours to 90+ days depending on the violation tier. An agency without a documented restriction-recovery playbook is an agency you will eventually wait on while your spend sits frozen.
Audience and creative constraints specific to behavioral health include the prohibition on SUD-identifying interest targeting, the requirement to avoid implying patient outcomes in creative, and the LegitScript landing-page standards.
Most healthcare-broad agencies learn these in their first year of behavioral health work, which is the year you will be paying them to figure it out.
This article assumes you understand why most treatment centers fail at Meta ads. The vetting framework below is the upstream work that prevents your facility from being the next case study.
Before the RFP: What to Align On Internally
Before you send the questions to agencies, align internally on five things. Agencies cannot give you good answers to questions you have not yet answered for yourselves.
Your monthly paid social budget and how it relates to your total marketing budget. Most behavioral health paid social retainers run between $5,000 and $25,000 monthly for management fees, with media spend layered on top. Know what you can sustain for 12 months minimum.
Your current performance baseline. What’s the current cost per admit on paid social? What’s the current creative volume per month? What’s the current ad account health status? An agency cannot improve what you cannot measure.
Your in-house capacity. Do you have someone internal who will own the agency relationship, review creative, approve copy, and handle compliance reviews? An agency without an internal counterpart at the facility under-delivers in predictable ways.
Your definition of success. Is success cost per admit, cost per collected dollar, total admits, payer mix shift, or some combination? Different definitions point to different agencies.
Your timeline expectations. Plan for 12 to 18 months minimum with the chosen agency. The first 90 days are ramp. Months 4 through 12 produce the compounding returns. Operators who expect month-one results from paid social agencies will be disappointed by every agency they hire.
The 15 Questions, Grouped
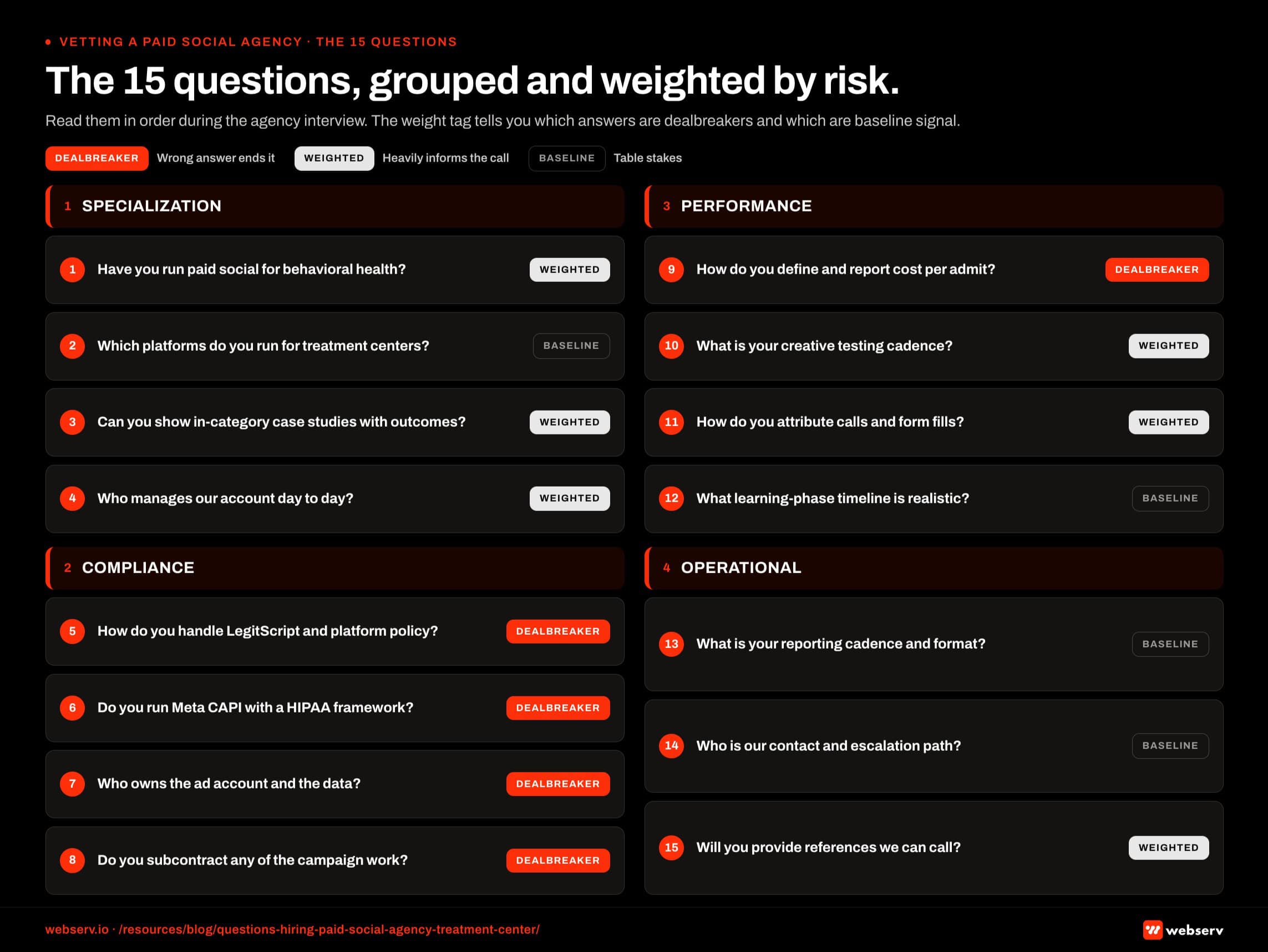
The questions split into four groups. Read them in order during the agency interview. Each question is followed by what a strong answer sounds like, what a weak answer reveals, and a drill-down question to ask if the answer is unclear.
Group 1: Specialization and Credentials
1. How many addiction treatment or mental health clients are you currently running paid social for, and can you name three references?
Why it matters: Behavioral health paid social is a separate discipline from healthcare-broad or consumer paid social. Agencies running fewer than three active behavioral health clients today are agencies who will learn the vertical on your dime.
What a strong answer sounds like: A specific count, with active client names where the agency has reference permission. References that match your facility profile (similar size, similar payer mix, similar geography). Willingness to introduce you to two or three current clients before contract signing.
What a weak answer reveals: Vague counts (“we have a few”), references that are 2+ years old, or references from adjacent verticals (general healthcare, hospitals, urgent care) rather than addiction treatment specifically. Agencies that lead with their consumer or healthcare-broad portfolio are signaling that behavioral health is not their specialization.
Follow-up if unclear: “Of those clients, how many are running active campaigns this week, and what’s the average monthly spend on Meta specifically?”
2. Which platforms do you actively run paid social on for behavioral health clients, and what’s the spend-by-platform breakdown across your book?
Why it matters: A strong behavioral health paid social agency will have differentiated experience across Meta, TikTok, LinkedIn, and increasingly YouTube. The platform mix tells you what they actually know vs. what they will be learning in real time.
What a strong answer sounds like: Specific percentages by platform across the behavioral health book. Discussion of which platforms work for which patient populations. Meta for family-member-driven inquiries, LinkedIn for B2B referral partner outreach, TikTok cautiously for younger demographics. Awareness that Meta still dominates behavioral health paid social spend but the platform mix matters.
What a weak answer reveals: Single-platform answers (“we mostly do Facebook”), no awareness of platform-specific behavioral health dynamics, or a pitch to add platforms you haven’t asked about.
Follow-up if unclear: “Walk me through a specific behavioral health client’s platform mix and why you allocated spend the way you did.”
3. What’s the longest tenure of a behavioral health client on your roster, and what’s the typical engagement length?
Why it matters: Long-tenure clients signal that the agency produces compounding results over time. High client churn signals month-one performance pressure that the agency is failing to convert into year-two retention.
What a strong answer sounds like: At least one client over 24 months, with several over 12 months. Honest discussion of average tenure (typically 18 to 30 months for healthy behavioral health agency-client relationships).
What a weak answer reveals: Average tenure under 12 months, no clients over 24 months, or evasive answers about churn rates.
Follow-up if unclear: “What’s the most common reason clients have churned in the last 12 months, and what changed in your process as a result?”
Group 2: Compliance and Platform Policy
4. How do you handle LegitScript advertising eligibility for clients running Google Ads alongside paid social?
Why it matters: LegitScript certification gates the entire addiction treatment paid advertising market across Google, Meta, Microsoft, TikTok, LinkedIn, and Nextdoor. An agency that doesn’t actively manage LegitScript status is an agency that will eventually have your ads suspended.
What a strong answer sounds like: Specific LegitScript application and renewal workflow. Awareness of the 2025-2026 fee structure ($975 application + $2,150 annual per website, with behavioral-health-facility tiered pricing). Documentation of which client ad accounts are tied to which LegitScript certifications.
What a weak answer reveals: “Your in-house team handles that.” Translation: the agency does not understand the certification system that gates their entire campaign.
Follow-up if unclear: “Walk me through what happens if a client’s LegitScript certification expires while paid campaigns are running.”
5. What’s your HIPAA and 42 CFR Part 2 framework for paid social work, specifically for Meta Conversions API and Custom Audience use?
Why it matters: The February 2026 42 CFR Part 2 compliance deadline tightened the rules on SUD patient data sharing. Meta CAPI server-side events and Custom Audience uploads can expose the facility to enforcement risk if not configured correctly.
What a strong answer sounds like: Specific server-side event configuration that strips PHI before transmission. Custom Audience strategies that avoid uploading any SUD-identifying patient list directly. Documentation of which fields flow from CRM to ad platform and which fields are explicitly filtered.
What a weak answer reveals: “Meta is HIPAA-compliant” (it is not). “We follow the same process as our other healthcare clients” (general healthcare and behavioral health have different compliance frames). “We don’t worry about Custom Audiences because we don’t use them” suggests they don’t know about high-value audience-building tactics.
Follow-up if unclear: “If a client’s CRM contains SUD-identifying records, what specifically does your agency upload to Meta as Custom Audience seed data and how?”
6. How many client ad accounts have been restricted or suspended by Meta or other platforms in the last 12 months, and what was the recovery process?
Why it matters: Behavioral health ad accounts get restricted more frequently than in other verticals. The question is not whether the agency has had restrictions; it’s whether they have a documented recovery playbook.
What a strong answer sounds like: Specific number (likely between 2 and 6 restrictions across the agency’s book in 12 months). Discussion of the recovery process: appeal documentation, alternative ad account spin-up while the primary is in review, creative and landing-page audit before the appeal goes in.
What a weak answer reveals: “We’ve never had a restriction” (either dishonest or signals very limited behavioral health volume). “We just spin up new ad accounts” (high-risk behavior that compounds platform-level scrutiny).
Follow-up if unclear: “What’s the average recovery time for the restrictions you’ve handled, and what’s the longest one took?”
Group 3: Performance and Measurement
7. What’s the typical cost per qualified lead and cost per admit for your behavioral health paid social clients, and how do you define each metric?
Why it matters: Vague metric definitions are how operators end up paying for traffic that does not convert to admits. Definitions matter as much as numbers.
What a strong answer sounds like: Specific cost-per-admit range based on actual client data (typically $1,800 to $5,500 in 2026 across behavioral health paid social depending on payer mix, length of stay, geography). Clear definition of “qualified lead” that excludes form spam and unqualified inquiries. Acknowledgment that cost per admit varies by payer mix and geography.
What a weak answer reveals: Vague ranges (“it varies”), benchmark numbers that don’t match behavioral health reality (“$50 per lead is typical”), or qualified-lead definitions that are not actually qualified.
Follow-up if unclear: “Take your last three behavioral health client engagements. What was the cost per admit at month three vs. month nine for each one?”
8. What’s your reporting and attribution stack, and how does conversion data flow from ad platform to CRM?
Why it matters: Cost per admit cannot be measured if conversion data does not flow cleanly from the ad platform to the CRM. Most agencies have weak attribution stacks.
What a strong answer sounds like: Specific tooling (GA4 + a tag manager + Meta CAPI + CRM integration). Discussion of how lead source attribution survives the funnel from form-fill to VOB to admission. Awareness of the gap between platform-reported conversions and actual collected revenue.
What a weak answer reveals: Reporting dashboards that show only Meta Ads Manager numbers. No CRM integration. No conversation about offline conversion data.
Follow-up if unclear: “Show me a sample weekly report from a current behavioral health client (with PHI redacted), and explain what each metric measures.”
9. How do you handle the gap between cost per admit (reported in 30 days) and cost per collected dollar (lagged 90-180 days)?
Why it matters: Cost per admit is a vanity metric if it does not connect to cost per collected dollar. Behavioral health paid social agencies that report only the upstream number are reporting on a 30-day cycle while the facility’s actual ROI runs on a 120-day cycle.
What a strong answer sounds like: Specific framework for lagged-collection reporting. Monthly or quarterly review that maps cost-per-admit cohorts to actual collected revenue 90 to 180 days later. Discussion of payer mix shifts that compress collected revenue per admit.
What a weak answer reveals: “We just track what Meta gives us.” Translation: the agency does not connect their work back to the bank account.
Follow-up if unclear: “What’s the typical cost per collected dollar for your behavioral health clients, and how does it compare to their cost per admit?”
10. What’s your average ratio of creative concepts produced per month, and how do you decide what to test and what to scale?
Why it matters: Creative is the single highest-impact variable in paid social performance over a 12-month horizon. Agencies producing 2 to 3 creative concepts per month will hit a creative-fatigue wall in 4 to 6 months.
What a strong answer sounds like: Specific monthly creative volume (typically 15 to 30 net-new concepts per month across formats and audiences for an active behavioral health client). Documented testing framework that distinguishes statistical testing from anecdotal testing. Clear scaling logic that promotes winning creative across audiences and ad sets.
What a weak answer reveals: Vague creative-volume answers, no documented testing methodology, no awareness of the creative formats that work best for behavioral health on Meta in 2026.
Follow-up if unclear: “What percentage of your current creative spend is on tests vs. proven-winner concepts, and how do you decide when to retire a creative?”
Group 4: Operational and Relationship Fit
11. Who on your team will actually run my account day-to-day, and what’s their behavioral health paid social experience?
Why it matters: Pitch teams are senior and impressive. Account-management teams are who actually runs your campaigns. The gap between the two predicts most agency failures.
What a strong answer sounds like: Named individuals with verifiable behavioral health paid social experience. Direct introduction to the day-to-day account manager during the sales process. Documented escalation paths to senior leadership when needed.
What a weak answer reveals: “We’ll assign someone after you sign.” “Our team is collaborative” (no named individuals). Senior-led pitch with junior account management revealed only after the contract is signed.
Follow-up if unclear: “Can I meet the specific person who would manage my account, and what’s their direct experience with addiction treatment clients?”
12. What’s your weekly and monthly cadence, including reporting deliverables and response SLA on questions?
Why it matters: Cadence predicts whether the relationship will be reactive (you chasing the agency) or proactive (the agency surfacing issues before you ask). Reactive relationships compound dysfunction.
What a strong answer sounds like: Standing weekly call. Monthly reporting deliverable with consistent format. Documented response SLA (typically 24 hours for non-urgent questions, same-day for urgent). Quarterly strategic review.
What a weak answer reveals: “We’re flexible” (translation: no defined cadence). “Email is best” (translation: no standing relationship structure). No mention of standing meetings.
Follow-up if unclear: “What’s the standing weekly call format, who attends from your team, and what’s the agenda?”
13. What’s the onboarding ramp, and what do you need from us in the first 30 days?
Why it matters: A defined onboarding ramp signals the agency has done this before and has a repeatable process. An ill-defined ramp signals you will be paying retainer during a 90-day exploration period.
What a strong answer sounds like: Specific weeks-to-launch timeline (typically 2 to 4 weeks to first campaign live, 60 to 90 days to optimized cadence). Clear list of what they need from your team in the first 30 days: CRM access, brand assets, compliance documentation, intro to clinical leadership for credentialed source positioning.
What a weak answer reveals: Open-ended ramps (“we’ll see how it goes”), vague asks (“just send us your stuff”), no discussion of clinical or compliance documentation needs.
Follow-up if unclear: “Walk me through the specific milestones in your first 30, 60, and 90 days with a new behavioral health client.”
14. What does off-boarding look like if we end the engagement?
Why it matters: Healthy agencies plan for off-boarding from day one. Unhealthy agencies build dependency that costs the facility time and equity to unwind.
What a strong answer sounds like: Documented off-boarding process. Ad accounts owned by the client (not the agency). Creative assets transferred on engagement end. Reporting infrastructure documented for handoff to in-house or successor agency. Reasonable transition period (30 to 60 days).
What a weak answer reveals: “We don’t really plan for that” (red flag). Ad accounts owned by the agency rather than the client (major red flag). No documented asset-transfer process.
Follow-up if unclear: “If we ended the engagement tomorrow, what specifically would we keep and what would we lose?”
15. What’s the contract structure, including retainer model, contract length, performance clauses, and cancellation policy?
Why it matters: Contract structure either aligns incentives or misaligns them. Long-lockup contracts with no performance clauses favor the agency. Month-to-month with performance terms favor the operator.
What a strong answer sounds like: Reasonable initial term (typically 6 months for the ramp), then month-to-month or shorter terms after that. Performance clauses tied to defined metrics. Reasonable cancellation notice (30 to 60 days). Transparent retainer structure.
What a weak answer reveals: 12-month or longer initial terms with no performance clauses. Steep early-cancellation penalties. Retainer structures that are not clearly documented. Bundled services that make pricing comparison impossible.
Follow-up if unclear: “What’s the cancellation notice period, and what happens to the work in flight at the time of cancellation?”
The single biggest predictor of whether a paid social agency will work out for a treatment center is not the pitch, the references, or the case studies. It is whether they can name the specific behavioral-health-specialist people who will run the account, walk you through their LegitScript and 42 CFR Part 2 framework in detail, and show you a month-nine cohort report from a current client. Agencies that can do all three rarely fail. Agencies that miss any of the three almost always do.
Preston Powell, CEO of Webserv
Red Flags and Dealbreakers
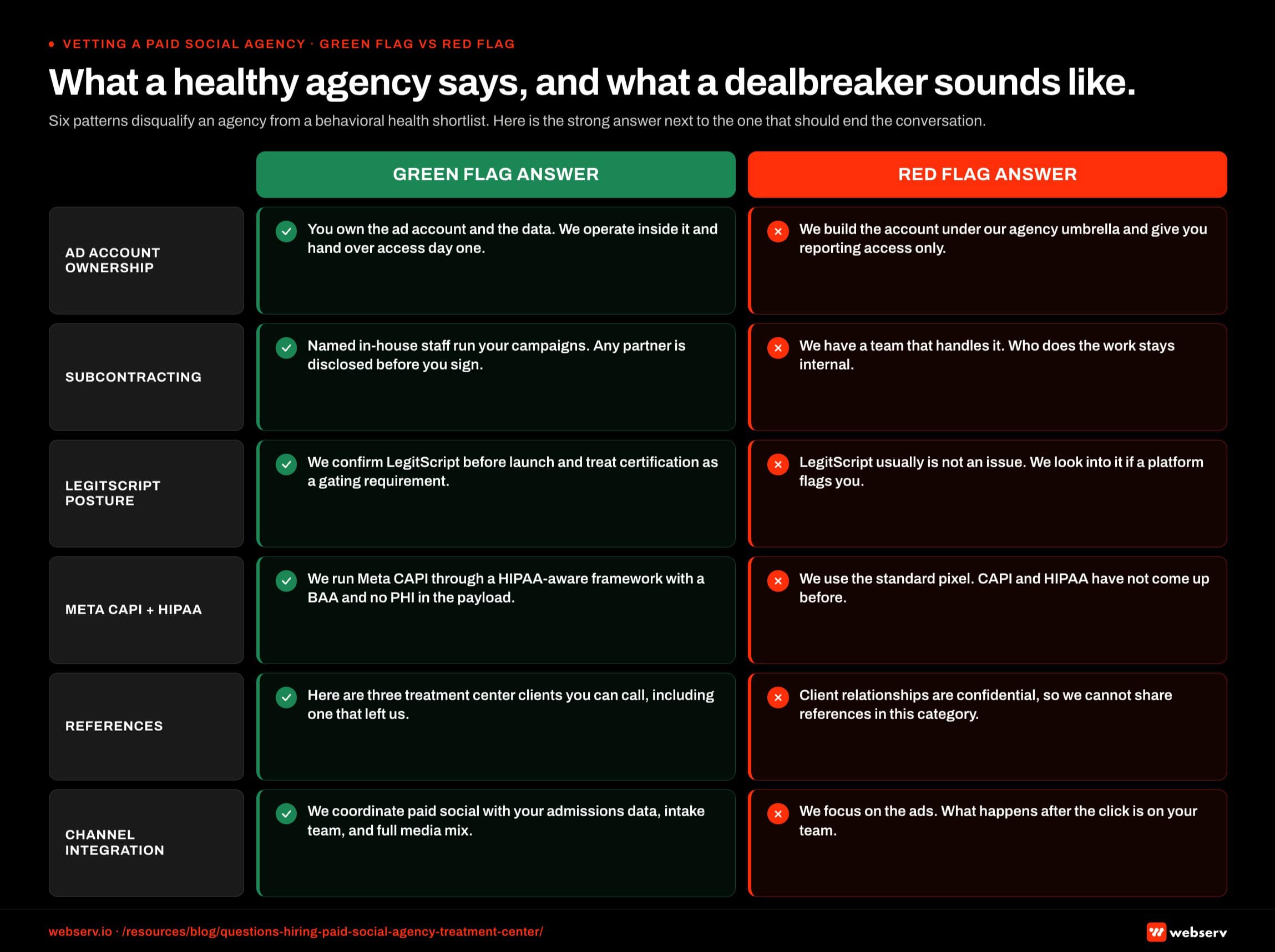
Some answers are not just weak; they should disqualify the agency from your shortlist. Six patterns count as dealbreakers in behavioral health paid social agency selection.
The agency owns your ad accounts rather than the client. Healthy agencies set up ad accounts under the client’s Business Manager and grant the agency partner-level access. Agencies that retain ownership are agencies that hold the facility hostage during off-boarding.
No documented LegitScript and compliance framework. Compliance is not a checkbox. If the agency cannot walk you through how they handle LegitScript renewals, Meta CAPI configuration under 42 CFR Part 2, and ad account restriction recovery, they will eventually cost you a quarter to a year of paid spend during a learning incident.
A pitch team that disappears after the contract signs. The senior pitch deck does not equal the senior account manager. If the agency will not introduce you to the day-to-day account team during the sales process, they are not planning to staff your account with senior people.
Long-lockup contracts with no performance clauses. A 12-month or longer initial term with no performance language and steep cancellation penalties is the contract structure of agencies that produce dependency, not capability.
Vanity-metric reporting. If the reporting deliverable shows only Meta Ads Manager numbers and does not connect to actual admits and collected revenue, the agency is reporting on a metric that does not pay your bills.
No clinical-side coordination. Treatment center marketing fails at the handoff between marketing, admissions, billing, and clinical. Agencies that don’t ask about clinical leadership, admissions team workflow, and billing-to-marketing data connections are agencies that will treat paid social as an isolated channel rather than the front end of an admit pipeline.
The 90-Day Evaluation Framework After You Hire
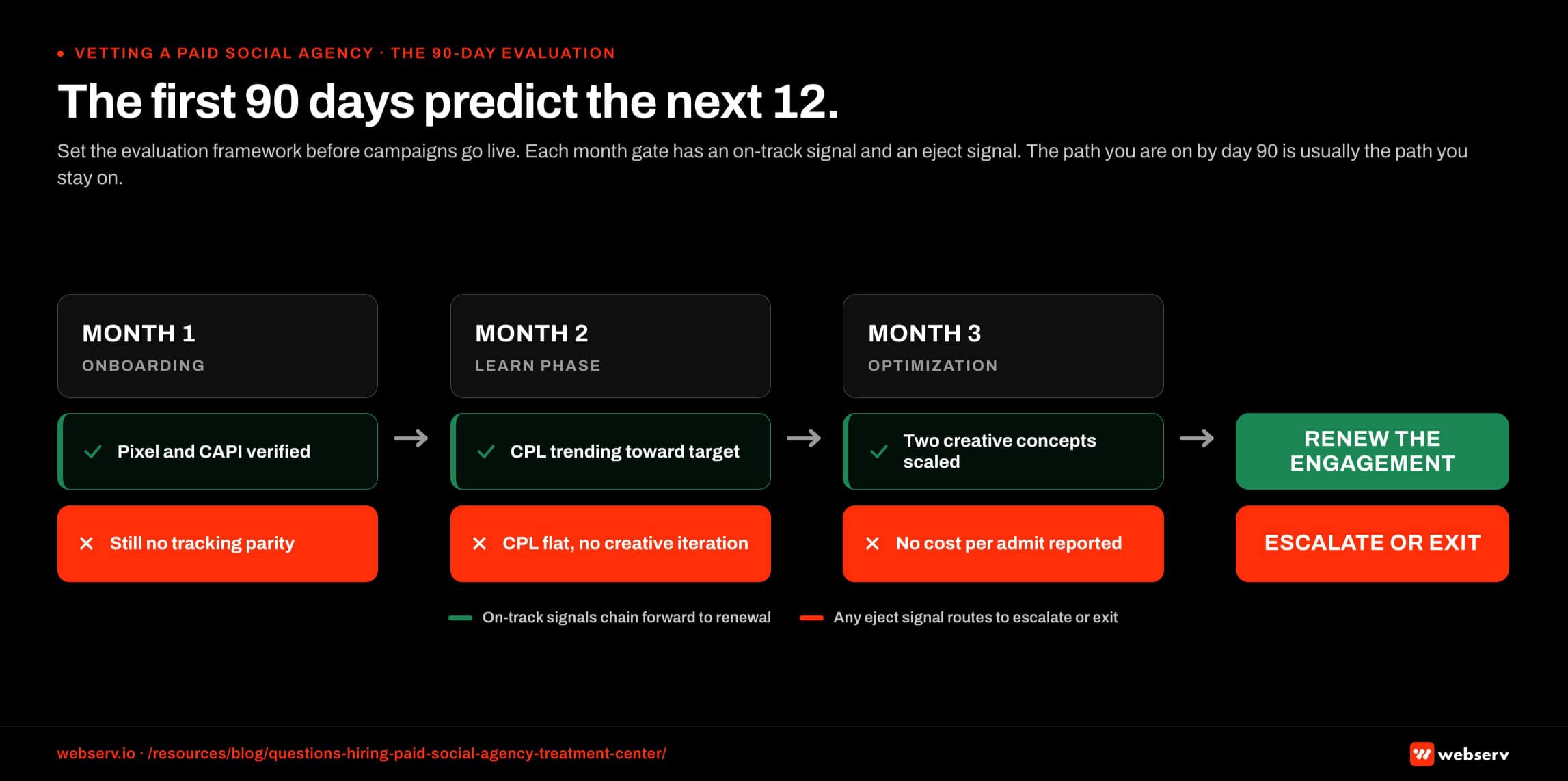
The first 90 days of the engagement predict the next 12. Set the evaluation framework before campaigns go live so you can recognize the right and wrong patterns when they show up.
Month 1: Onboarding and Foundation. Ad accounts set up under your Business Manager with the agency as partner. LegitScript and 42 CFR Part 2 documentation completed. First creative concepts produced and reviewed. Tracking and CRM integration validated. First campaigns live by end of month 1 or early month 2.
By end of month 1, you should have: working ad accounts under your ownership, documented compliance framework, first creative concepts approved, validated tracking from form-fill to CRM, and a standing weekly call cadence with the same account-management team that pitched you.
Month 2: Initial Campaign Performance. Campaigns live across the primary platforms. First conversion data flowing. Initial creative-fatigue patterns visible. Adjustments to audience and creative based on early data.
By end of month 2, you should have: 2 to 3 weeks of campaign data, initial cost-per-lead and cost-per-admit numbers (with the caveat that month-2 numbers will not be representative).
You should also have early creative-winners identified and a clear sense of whether the account team is responding proactively to performance signals.
Month 3: Optimization Cycle. Tested creative and audience patterns produce a stable cost-per-admit benchmark. Reporting cadence established. Cross-functional coordination with admissions and billing teams in place.
By end of month 3, you should have: a stable cost-per-admit number that the agency can defend, plus a documented creative-iteration cycle producing 15 to 30 net-new concepts per month.
You should also have a 30/60/90 day cohort framework showing how earlier-month admits are tracking to collected revenue, and confidence that the relationship cadence supports the work.
Operators who hit these milestones on schedule are working with the right agency. Operators who miss them are working with the wrong agency, and the first 90 days are when the cost of switching is lowest.
Frequently Asked Questions
How long should I expect the agency interview process to take?
Plan for 4 to 8 weeks from initial outreach to signed contract for a substantive paid social agency selection process. Compressing the timeline below 4 weeks usually means skipping reference calls and second-meeting drill-downs, which is when the real signal shows up.
The first round is typically a 60-minute discovery and capabilities pitch. The second round is the question-by-question deep-dive using the 15 questions in this article. The third round is reference calls, contract review, and final negotiations.
Most operators we work with run 3 to 5 agencies through the full process before selecting. Running fewer than 3 means you don’t have a comparison set; running more than 5 means you are not filtering for category fit before the deep interviews.
What’s the right monthly retainer to budget for paid social management?
Realistic management retainer ranges depend on agency tier and scope. Boutique behavioral-health-specialist agencies typically run $5,000 to $15,000 monthly for management fees, often with a media-spend minimum.
Healthcare-broad agencies typically run $15,000 to $40,000 monthly for dedicated paid social scope. Enterprise PR-and-advertising agencies (Real Chemistry, Edelman) typically engage at $40,000 and up monthly when they take behavioral health clients at all.
Media spend layers on top of management fees. For a multi-facility behavioral health operator running serious paid social, expect total monthly investment (management + media) of $20,000 to $100,000+ depending on facility count and admit-volume goals.
Should I require a performance clause in the contract?
Yes, with realistic clause structure. The mistake operators make is writing performance clauses tied to month-one or month-two metrics, which fail to account for the ramp cycle.
A workable performance clause is tied to month-6 cost-per-admit performance against a defined baseline, with a clear definition of what counts as an admit and how it gets attributed to paid social vs. other channels. If the agency misses the month-6 target by more than 20 percent, the contract converts to month-to-month with a 30-day notice.
Performance clauses that are written reasonably and tied to defined metrics signal alignment. Agencies that refuse any performance language are agencies that don’t want accountability. Agencies that propose unrealistic performance language are signaling overpromise habits.
How do I evaluate an agency’s references during the selection process?
Ask the references three specific questions. First, what did the agency promise in the pitch vs. what they delivered in months 3 to 9? The gap between pitch and delivery is the agency’s actual performance signature.
Second, how does the agency handle problems? Every behavioral health paid social engagement runs into ad account issues, creative-fatigue periods, and performance dips. The agency’s behavior during those moments matters more than the behavior during the easy months.
Third, would they sign with this agency again if they were starting over? An evasive answer here is the most important signal in the entire reference process.
Should I hire a behavioral-health-specialist agency or a healthcare-broad one?
For most multi-facility behavioral health operators, behavioral-health-specialist agencies produce better outcomes in the first 24 months. The reason is the learning curve. Healthcare-broad agencies need 6 to 12 months to learn behavioral-health-specific compliance, audience, and creative constraints, and you will be paying full retainer during that learning period.
Healthcare-broad agencies become viable when the operator has very large paid social budgets (over $40,000 monthly in media spend) where the agency’s scale and senior bench compensate for the behavioral-health-specific learning curve. They also become viable when the operator has strong in-house behavioral health paid media leadership that can supplement the agency’s missing specialization.
For most operators in the first 24 months, a behavioral-health-specialist agency from the curated list is the better starting point.
What’s the right cadence to evaluate the agency relationship over the full engagement?
Three evaluation points matter. The 90-day evaluation determines whether to continue past the initial ramp. The 12-month evaluation determines whether to renew or transition. The 24-month evaluation determines whether to bring the function in-house, switch agencies, or maintain the relationship.
At each evaluation point, the question is not just whether performance is acceptable. It is whether the agency’s compounding returns (creative library depth, audience stack maturity, platform-policy relationships, reporting integration quality) are accumulating in your favor or remaining stagnant.
Agencies that compound returns over time are agencies worth renewing for years. Agencies that produce only month-one performance with no compounding are agencies to transition out of when the cost of switching is lowest, which is typically the 12 to 18 month window.
Hire the Right Paid Social Agency the First Time
Hiring a paid social agency for a treatment center is one of the highest-stakes vendor decisions in behavioral health marketing. The 15 questions in this article are the framework Webserv uses internally when treatment center operators ask us to help them evaluate competing proposals.
The questions are not theoretical. Each one surfaces a specific failure mode that has cost a real operator real admits in the last 24 months.
The agencies that answer well are the agencies that produce compounding returns over 12 to 24 months. The agencies that answer poorly are the agencies you should not sign with regardless of how good the pitch deck looks.
Book an intro meeting to walk through your current paid social setup, what the right vetting framework looks like for your facility, and how the broader marketing program connects paid social to admit pipeline and collected revenue.
For the broader picture of how paid social fits inside a full treatment center marketing program, see our paid social ultimate guide and our ultimate guide to behavioral health marketing.
Mitch Marowitz is Director of Paid Media at Webserv, where he leads paid search, paid social, and CRO programs for behavioral health and addiction treatment centers across the U.S. He writes about treatment-center paid media performance, creative testing, and the operational realities of running high-acuity healthcare campaigns.