Paid social for behavioral health treatment centers has crossed a threshold in 2026. Meta moved healthcare advertisers into a sensitive category framework, HHS-OCR doubled enforcement activity on tracking technologies, and platform-level audience targeting has narrowed simultaneously. A 2022 paid social playbook applied to a 2026 account produces predictable failure.
The operators winning paid social in this category are running an integrated channel mix, a HIPAA-safe tracking stack, and a creative framework built around family-member voice and platform-specific compliance. Each of those layers connects to the others; an account missing any one of them does not reach scale.
This guide walks through the 2026 landscape, the six platforms in the mix, the family-versus-patient targeting decision, the HIPAA-safe tracking architecture, the common mistakes that get accounts banned, and how to evaluate or audit a paid social agency for behavioral health.
Key Takeaways
- Paid social is still a viable admissions channel for behavioral health, but only with LegitScript certification, Meta addiction treatment certification, and a HIPAA-aware tracking infrastructure built around the Conversions API instead of the Meta pixel.
- The 2026 platform restrictions are stricter than any prior cycle. Meta moved healthcare into a three-tier sensitive category framework starting January 2025, with a second wave hitting lead-generation campaigns in early 2026. HHS-OCR launched civil enforcement of 42 CFR Part 2 on February 16, 2026.
- Family-first targeting outperforms patient-first targeting for residential and PHP admissions. The buyer is rarely the patient. The audience signal layer, household-income tiers, and life-event signals identify family decision-makers better than any zip-list approach.
- Creative compliance is non-negotiable. Before-and-after imagery, exaggerated outcome claims, and emotional manipulation language get accounts disabled in the current enforcement environment. The compliant creative bar is educational, family-focused, and outcome-realistic.
- Budget allocation should weight Meta heavily (60-75% of social spend for most BH operators), with TikTok and Snap as supplements for specific patient demographics, and Reddit and YouTube as long-tail authority surfaces rather than direct-response channels.
A 42-bed residential treatment center came to us in January after Meta disabled their ad account for the third time in 18 months. The first disable was a creative policy violation. The second was an unverified payment source.
The third was the lookalike audience they had built from their Meta pixel, which Meta’s compliance system flagged as PHI exposure under the new healthcare advertising restrictions that started rolling out in 2025.
The facility had spent six months and roughly $180,000 with three different agencies, none of which had explained why the disables kept happening, and all of which had assumed the next one would be the last.
The fix took 60 days. We removed the Meta pixel entirely, rebuilt tracking on the Conversions API with server-side identity matching, restructured creative around compliant family-first messaging, and submitted a new LegitScript-tied addiction treatment certification through Meta’s approval flow.
The account has been live and stable for the 11 months since, running $58,000 a month in social spend at a cost per admission roughly half of what the prior agencies had achieved before the disables started.
That story is the right opener for this guide because it captures the actual problem with paid social for behavioral health in 2026. The platforms are still high-volume admission channels for the operators who run them correctly. They are also a regulatory minefield that gets worse every quarter as Meta, TikTok, and the rest of the stack tighten their healthcare advertising posture.
This paid social guide covers what the 2026 environment actually looks like, what the compliant playbook is across each platform, and how to build the tracking and creative infrastructure that survives the next round of restrictions.
The 2026 paid social landscape for treatment centers
The starting point is that 2026 paid social for behavioral health is harder than it was in 2022, and the trend is toward more restriction, not less. Three structural forces are reshaping what works.
The first is platform compliance tightening. Meta moved healthcare advertisers into a sensitive category framework starting in January 2025, with tiered restrictions on optimization signals, audience targeting, and lead-form mechanics. The second wave landing in 2026 extends those restrictions to healthcare lead-generation campaigns specifically. TikTok and Snap have both narrowed addiction treatment ad eligibility, requiring educational framing rather than direct admission acquisition messaging.
The second is HIPAA enforcement intensification. The HHS Office for Civil Rights imposed $4.18 million in penalties across 13 enforcement actions in the most recent year, nearly double the prior year. OCR launched civil enforcement of 42 CFR Part 2 in February 2026, which means mishandling of substance use disorder records now carries civil money penalties aligned with HIPAA’s tiered structure. Tracking technologies on healthcare sites are explicitly flagged as enforcement targets.
The third is the broader privacy infrastructure shift. iOS 14.5 in 2021, the death of third-party cookies in 2024, and Apple’s continued attribution-window tightening have made the pre-2021 paid social tracking model unworkable. The operators still running on legacy pixel-only setups are getting worse data every quarter and do not realize it.
The combined effect is that paid social for behavioral health requires a higher operational bar than it used to. Treatment centers running paid social in 2026 need compliance infrastructure, a server-side tracking layer, a family-first creative strategy, and a budget posture that survives platform volatility. Operators who try to run the 2020 playbook in 2026 lose ad accounts, miss admissions, and pay agencies to learn what was already published in platform documentation.
HIPAA and platform compliance in 2026
Compliance is the spine of paid social in this category. Two compliance surfaces drive most of the operational reality.
HHS-OCR and HIPAA tracking technologies
The HHS-OCR guidance on online tracking technologies classifies the data flowing through pixels, SDKs, and analytics tools as PHI when the user is engaging with health-related content. A Meta pixel on a page about IOP services that fires on form submission is sending PHI to Meta unless a Business Associate Agreement is in place, which Meta does not sign. The legal exposure for treatment centers running standard pixel setups is real and increasing.
The implication is that the Meta pixel as historically deployed is a HIPAA risk on most treatment center sites.
The compliant replacement is the Meta Conversions API deployed with server-side identity hashing, no PHI in the URL path or event parameters, and an opt-in disclosure on the page that informs users about data collection. The headline is that the pixel-only approach common in 2020 will not survive a 2026 OCR audit.
OCR’s February 2026 enforcement launch under 42 CFR Part 2 specifically targets substance use disorder records, which means the SUD content category carries higher enforcement scrutiny than general healthcare. Treatment centers should assume an audit is more likely in 2026 than in any prior year, and the tracking layer should be built accordingly.
Meta’s addiction treatment policy and LegitScript
The Meta addiction treatment ad policy requires advertisers running addiction treatment ads in the United States to be LegitScript-certified and to apply separately to Meta for permission to advertise in this category. The certification process is the gate for serving ads at all; the permission flow on top of it is what distinguishes addiction treatment from general healthcare advertising on the platform.
Treatment centers without active LegitScript certification cannot run compliant paid social on Meta. The certification process is also the prerequisite for Google Ads and the rest of the major ad ecosystem, so the work is not Meta-specific. The 60-90 day certification timeline should be built into any paid social planning that does not already have the credential.
Meta also assigns healthcare advertisers to one of three sensitive category tiers based on service type. Substance use treatment is in the most restrictive tier, which means reduced access to standard optimization events (Purchase, Lead are blocked or limited), tighter audience targeting constraints, and reduced lookalike eligibility. The optimization workarounds discussed later in this guide are how operators in this tier actually run effective campaigns despite the restrictions.
Other compliance surfaces
LegitScript and Meta are the two big ones. The remaining surfaces are platform-specific:
- Google Ads requires LegitScript and applies its own healthcare advertising policies and compliance mistakes framework, including healthcare advertising compliance constraints that apply across surfaces
- TikTok treats addiction treatment as a restricted category, with educational framing requirements and limited targeting
- Snapchat age-restricts addiction-related ads to users 18+ and requires educational rather than promotional messaging
- Reddit is the least restrictive but still requires honest claims and prohibits exploitative framing
- LinkedIn is generally usable for B2B treatment marketing (referral source acquisition, employee recruitment) without addiction-specific restrictions
The compliance posture across these surfaces is what determines which platforms a treatment center can run on, in what creative shape, and at what budget level.
Beyond platform policies, the FTC’s 2024 Health Products Compliance Guidance and its March 2026 enforcement letters to substance use disorder treatment providers add a federal regulatory layer to the picture. Unsubstantiated outcome claims like “guaranteed recovery” or “85% sobriety rate” without published methodology are actionable at the federal level regardless of which platform they ran on. The compliant default for treatment center paid social is defensible operator-voice claims with documented substantiation behind every quantitative statement.
Platform-by-platform breakdown
Paid social is not one channel. Each platform has its own audience, compliance posture, and economics. The right mix depends on facility, patient demographic, and budget scale.
 Infographic titled ‘Where treatment centers actually advertise in 2026 — and what wins on each platform’ showing a six-platform paid social matrix for behavioral health operators. Meta (Facebook + Instagram): reaches family decision-makers with the broadest behavioral health audience layer, takes 60–75 percent of typical social budget, works on family-perspective creative with a Reels + carousel + static mix optimized through Conversions API on upper-funnel events, killed by Meta pixel on PHI-exposing pages and lookalikes built from PHI. TikTok: reaches young adults 18–29 with a 16–34 audience skew, takes 5–15 percent of budget, works on mental health awareness framing routing to info pages not direct admit flows, killed by direct treatment-acquisition language. Snapchat: reaches young adults with AR-first creative formats, takes 0–5 percent of budget, works on awareness-only campaigns and AR lenses for lower-acuity outpatient, killed by direct-response intent without compliance review. Reddit: reaches self-aware patients researching options and family members in support subreddits, takes 0–10 percent of budget, works on educational copy and transparent operator presence, killed by hard-sell ad copy and subreddit policy violations. YouTube: reaches mid-funnel research with brand authority for family + patient mix, takes 5–15 percent of budget, works on 30–60s testimonial-style video and clinician-led explainers, killed by generic stock-footage rehab ads and Healthcare and Medicines policy violations. LinkedIn: reaches professional referrers like EAPs, PCPs, school counselors, and attorneys for B2B alumni-referral build, takes 0–5 percent of budget, works on clinician-led leadership content and LegitScript-aware partner offers, killed by consumer-direct admission ads. Color legend: green = stable + certifiable, yellow = restricted runs cautious, red = workaround-required. Footer: most operators run 70–80% of budget on Meta, 10–15% on YouTube, 5–10% across one or two of the rest.” class=”wp-image-23996″/>
Infographic titled ‘Where treatment centers actually advertise in 2026 — and what wins on each platform’ showing a six-platform paid social matrix for behavioral health operators. Meta (Facebook + Instagram): reaches family decision-makers with the broadest behavioral health audience layer, takes 60–75 percent of typical social budget, works on family-perspective creative with a Reels + carousel + static mix optimized through Conversions API on upper-funnel events, killed by Meta pixel on PHI-exposing pages and lookalikes built from PHI. TikTok: reaches young adults 18–29 with a 16–34 audience skew, takes 5–15 percent of budget, works on mental health awareness framing routing to info pages not direct admit flows, killed by direct treatment-acquisition language. Snapchat: reaches young adults with AR-first creative formats, takes 0–5 percent of budget, works on awareness-only campaigns and AR lenses for lower-acuity outpatient, killed by direct-response intent without compliance review. Reddit: reaches self-aware patients researching options and family members in support subreddits, takes 0–10 percent of budget, works on educational copy and transparent operator presence, killed by hard-sell ad copy and subreddit policy violations. YouTube: reaches mid-funnel research with brand authority for family + patient mix, takes 5–15 percent of budget, works on 30–60s testimonial-style video and clinician-led explainers, killed by generic stock-footage rehab ads and Healthcare and Medicines policy violations. LinkedIn: reaches professional referrers like EAPs, PCPs, school counselors, and attorneys for B2B alumni-referral build, takes 0–5 percent of budget, works on clinician-led leadership content and LegitScript-aware partner offers, killed by consumer-direct admission ads. Color legend: green = stable + certifiable, yellow = restricted runs cautious, red = workaround-required. Footer: most operators run 70–80% of budget on Meta, 10–15% on YouTube, 5–10% across one or two of the rest.” class=”wp-image-23996″/>Meta (Facebook + Instagram)
Meta is still the dominant paid social channel for behavioral health admissions. It carries 60 to 75% of total social spend for most of the operators we work with, for three reasons.
First, the audience signal layer for family-decision-maker targeting is more developed than any other platform. Household income deciles, parental status, life events, and in-market signals combine to identify family members in a way TikTok or Snap cannot match.
Second, Meta’s creative formats (single image, carousel, Reels, Stories) cover the spectrum from educational long-form to fast direct-response. The same campaign can run a 60-second video about treatment options on Reels and a static image testimonial on the Facebook feed.
Third, despite the compliance restrictions, Meta still allows treatment center advertising with the right certification stack. TikTok and Snap operate at the margin of “can we even run here” for some operators. Meta operates at “what optimization events can we use” for the same operators.
The 2026 reality on Meta is that lower-funnel optimization (Purchase, Lead) is restricted for substance use treatment advertisers. The workaround is to optimize on upper-funnel events (ViewContent, Page View, custom engagement events) and use the Meta Conversions API setup to feed Meta the conversion signal it cannot capture through pixel. This setup recovers most of the optimization quality the restrictions removed, but only for operators who invested in the tracking infrastructure.
TikTok
TikTok runs cautious for addiction treatment ads. The platform’s stated approach is educational mental health awareness rather than direct treatment-acquisition advertising. In practice, treatment centers can run on TikTok with creative framed around mental health support, family resources, and educational content, with calls-to-action that route to information pages rather than direct admission flows.
The audience case for TikTok is specific. The platform’s user base skews 16-34, with the 18-24 demographic over-represented. For treatment centers focused on young adult patients (ages 18-29 specifically), TikTok produces admission inquiries from a demographic Meta reaches less efficiently. For centers focused on older patient populations or where the buyer is the parent of an adult child, TikTok is a less effective channel.
Budget allocation for TikTok in BH typically lands at 5 to 15% of total social spend when it makes sense, scaling up only for centers with strong young-adult patient fit.
Snapchat
Snapchat is similar to TikTok in audience demographic (38% of users are 18-24) but with more aggressive ad restrictions. Addiction treatment ads must be educational, age-gated to 18+, and avoid emotional manipulation framing. The conversion economics on Snap are usually weaker than Meta or TikTok for BH because the user behavior on the platform is fast, light, and not conducive to multi-step admission flows.
Snap fits best as a brand-awareness layer for treatment centers reaching the young adult demographic, with the heavier conversion work happening elsewhere in the funnel. Allocation is typically 0 to 5% of total social spend for most BH operators. The same body-brokering competitive dynamics that distort Meta ad auctions also distort Snap and TikTok auctions in known fraud corridors, which factors into geo allocation.
Reddit is increasingly viable in 2026 for treatment center advertising. The platform’s policy posture is more permissive than Meta or TikTok, and Reddit’s audience includes high-intent communities (r/addiction, r/recovery, r/AlAnon) where treatment-related content has real engagement.
The challenge with Reddit is that the platform’s culture punishes obvious promotional content. Treatment center ads that read as direct-response acquisition fail. Ads that read as informational, with genuine resource value, perform. Reddit also has limited audience signal sophistication relative to Meta, which means the targeting is coarser and the budget efficiency is lower at scale.
Reddit fits best for treatment centers with strong educational content libraries and a willingness to invest in community engagement alongside paid placement. Allocation is typically 3 to 10% of total social spend.
YouTube
YouTube is technically Google’s display network, not paid social, but it functions as a paid social surface for behavioral health. The pre-roll, mid-roll, and in-feed video formats reach a family-decision-maker audience well, especially for residential and high-acuity treatment.
The compliance posture follows Google Ads (LegitScript-gated). The creative requirement is video, which is a higher production bar than static or short-form. For treatment centers with a video creative budget, YouTube is a strong family-targeting channel with stable cost-per-admission economics. The ad group structure principles that govern Google Search campaigns also apply to YouTube video targeting. For centers without video creative capacity, YouTube is premature.
Budget allocation is typically 5 to 15% of total social spend when video creative is available.
LinkedIn is the outlier in the BH paid social stack. The platform is not effective for direct patient acquisition, but it is highly effective for B2B treatment marketing: referral source acquisition (interventionists, therapists, employee assistance programs), employer-EAP partnership development, and clinical recruitment.
For treatment centers with a referral-source or B2B partnership growth objective, LinkedIn carries unique value. For centers focused on direct family acquisition, LinkedIn is a distraction. Allocation depends entirely on the operator’s growth strategy rather than the patient demographic.
Audience strategy: family vs patient targeting
The single most important strategic decision in BH paid social is whether the campaign is targeting the patient or the family member. The economics, creative, and platform fit all change with the answer.
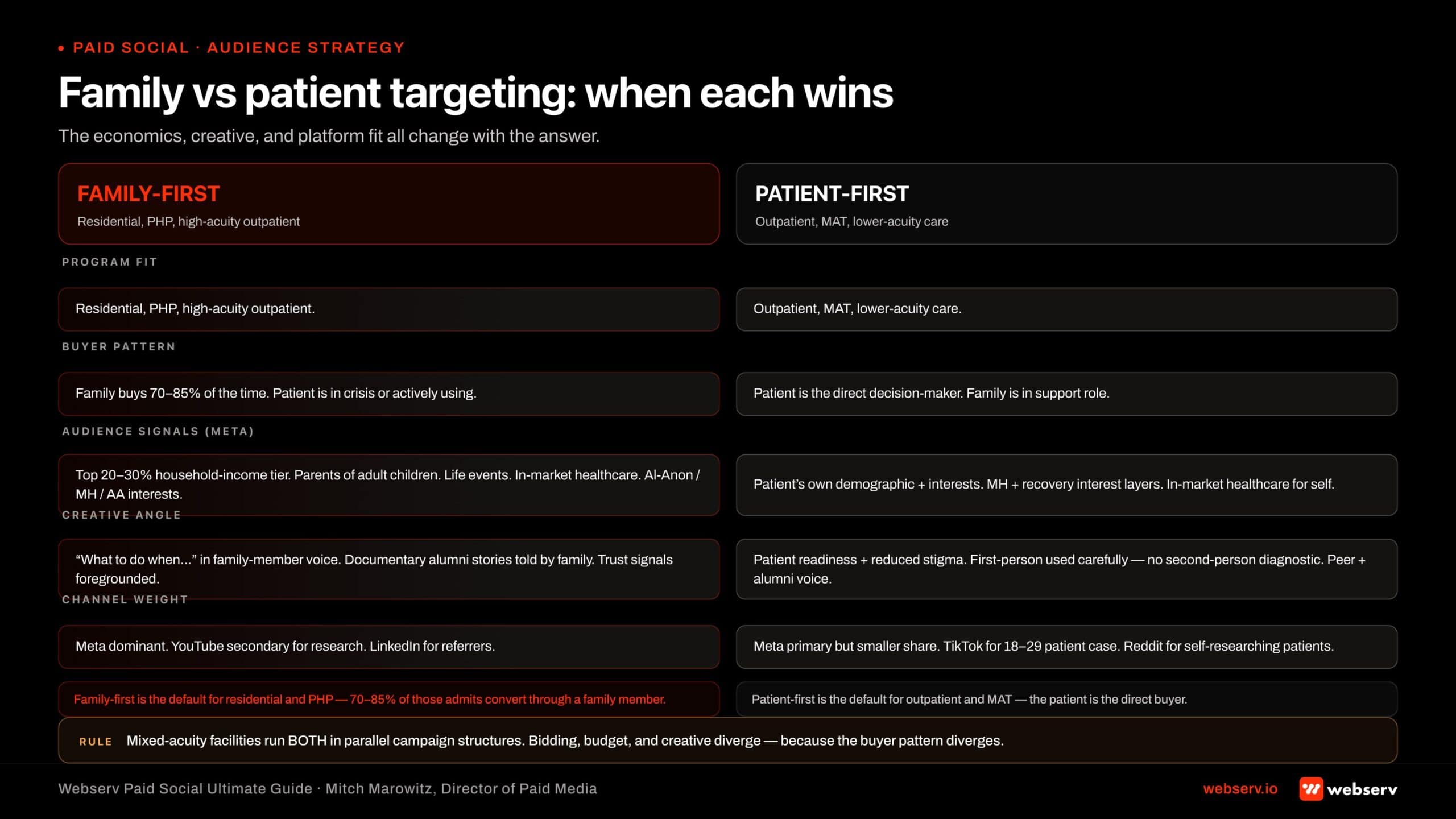 Infographic titled ‘Family vs patient targeting: when each wins.’ Side-by-side comparison of family-first versus patient-first paid social targeting strategies for behavioral health treatment centers. Family-first column applies to residential, PHP, and high-acuity outpatient programs where the family is the buyer 70–85 percent of the time; uses Meta audience signals including household income tier (top 20–30%), parental status for parents of adult children, life events like divorce or recent move, in-market healthcare, and interest layers in family support (Al-Anon, mental health, AA/NA); creative angle is ‘what to do when’ framing in family-member voice with documentary alumni stories told by family and trust signals foregrounded; channel weight is Meta dominant with YouTube secondary for research and LinkedIn for referrers. Patient-first column applies to outpatient, MAT, and lower-acuity care where the patient is the direct decision-maker; uses the patient’s own demographic and interests including mental health and recovery interest layers and in-market healthcare for self; creative angle is patient readiness and reduced stigma with first-person framing used carefully (no second-person diagnostic) and peer + alumni voice; channel weight is Meta still primary but smaller share with TikTok added for the 18–29 patient case and Reddit for self-researching patients. Center band footer: ‘Mixed-acuity facilities run both in parallel campaign structures. Bidding, budget, and creative all diverge because the buyer pattern diverges.’
Infographic titled ‘Family vs patient targeting: when each wins.’ Side-by-side comparison of family-first versus patient-first paid social targeting strategies for behavioral health treatment centers. Family-first column applies to residential, PHP, and high-acuity outpatient programs where the family is the buyer 70–85 percent of the time; uses Meta audience signals including household income tier (top 20–30%), parental status for parents of adult children, life events like divorce or recent move, in-market healthcare, and interest layers in family support (Al-Anon, mental health, AA/NA); creative angle is ‘what to do when’ framing in family-member voice with documentary alumni stories told by family and trust signals foregrounded; channel weight is Meta dominant with YouTube secondary for research and LinkedIn for referrers. Patient-first column applies to outpatient, MAT, and lower-acuity care where the patient is the direct decision-maker; uses the patient’s own demographic and interests including mental health and recovery interest layers and in-market healthcare for self; creative angle is patient readiness and reduced stigma with first-person framing used carefully (no second-person diagnostic) and peer + alumni voice; channel weight is Meta still primary but smaller share with TikTok added for the 18–29 patient case and Reddit for self-researching patients. Center band footer: ‘Mixed-acuity facilities run both in parallel campaign structures. Bidding, budget, and creative all diverge because the buyer pattern diverges.’For residential treatment, PHP, and high-acuity outpatient programs, the family member is the buyer 70 to 85% of the time. The patient is in crisis or actively using and is not the decision-maker for admission. The family member is the parent, spouse, or adult child who is researching options, comparing facilities, and writing the check.
Family-first targeting on Meta uses:
- Household income tier signals (top 20 to 30% for OON economics)
- Life event signals (recently divorced, new homeowner, recently moved correlate with elevated decision-bandwidth)
- Parental status (parents of adult children for adult treatment programs)
- In-market for healthcare signals
- Interest layers (mental health, addiction recovery, family support, AA/NA, Al-Anon) layered with healthcare demographic targeting signals
- Geographic targeting that follows the exclude-zip framework rather than narrow zip inclusion
For outpatient programs, MAT, and lower-acuity care, the patient is more often the direct decision-maker. The patient-first creative speaks to the patient’s own readiness and reduces stigma. The audience targeting shifts to the patient’s own demographic and interests rather than the family member’s.
A mixed-acuity facility (offering residential plus outpatient) typically runs two parallel campaign structures: one family-first for the residential pull, one patient-first for the outpatient pull. The bidding, budget, and creative diverge between the two campaigns because the buyer pattern diverges.
The single most common audience mistake in this category is assuming the patient is the buyer for residential. They are not. Building creative and targeting around the patient when the family is the actual decision-maker is the fastest way to spend $50,000 a month with disappointing admission volume.
Mitch Marowitz, Director of Paid Media, Webserv
Creative strategy
Creative in BH paid social has to do two things at once. It has to emotionally resonate with the family member’s actual experience (which is grief, fear, exhaustion, and hope). And it has to clear platform compliance, which prohibits emotional manipulation, before-and-after imagery, and outcome claims that cannot be substantiated.
The compliant creative bar has five elements that work.
Family-perspective framing. The hero in the ad is the family member, not the patient. The voiceover or copy speaks from the family member’s perspective. The emotional resonance is the family member’s relief at finding the right program, not the patient’s transformation. This framing is compliance-safe because it does not make claims about treatment outcomes for the patient.
Educational, not promotional. The creative explains something the family member needs to understand (the difference between levels of care, what to look for in a residential program, how insurance verification works) rather than directly pitching the facility. Educational creative passes platform review faster, scales further, and converts better in 2026 than direct-pitch creative does.
Family member featured as a presenter, not as a “success story.” Showing a real family member explaining how they navigated a relative’s treatment is highly effective. Showing a “before” picture of a person in active addiction and an “after” of them sober is a creative policy violation on Meta, TikTok, and most other platforms.
Honest framing of treatment realism. Saying “we help families work through the next 90 days” is compliant. Saying “we save lives every day” is not. The closer the language is to the operational reality of what the facility actually does, the safer the creative is to scale.
Native format respect. Reels and TikTok creative should look native to the platform (vertical, 9:16, fast-cut, captioned). Facebook feed creative can be longer-form. LinkedIn creative reads more formal. Reusing the same asset across all formats is a common failure pattern that hurts performance on every platform it runs on.
The compliant ad headlines work we publish on the Google Ads side translates directly to Meta and TikTok creative copy. The principles are the same: no outcome promises, no before-and-after framing, no emotional manipulation, no first-person “I’m a patient” testimonials without consent infrastructure. Within those constraints there is still meaningful creative range.
Tracking infrastructure that survives 2026
The tracking layer is what separates BH operators who actually optimize from operators who pretend to optimize. Three pieces matter.
Server-side conversion API
The Meta Conversions API replaces the browser-side pixel for sending conversion events to Meta. The server-side path has three advantages in 2026: it does not require PHI to flow through the browser, it survives iOS attribution restrictions, and it gives Meta cleaner signal for the optimization layer.
The Conversions API setup for treatment centers covers the implementation in detail. The headline is that without the CAPI infrastructure, paid social in 2026 is running with one hand tied behind its back, and the operators who skipped this work are the operators with disabled ad accounts.
First-party data layer
Treatment centers have rich first-party data: form submissions, phone calls, intake records. Connecting that data to the paid social signal layer (through hashed email and phone matching) recovers most of the conversion attribution that platform restrictions removed.
The pattern is that the intake CRM captures the lead, hashes the contact identifiers, and forwards them to Meta and the other platforms through the CAPI or equivalent. Meta uses the hashed match to attribute the conversion back to the original ad click. The user identity stays on your side. Meta gets the optimization signal it needs without receiving PHI.
This is the same pattern that runs the HIPAA-compliant Facebook ads setup for treatment centers. It is more work than a pixel install, and it is the bar that 2026 compliance and 2026 attribution both require.
Call tracking integrated with the social platforms
Roughly 60 to 75% of behavioral health admission inquiries come in by phone, not by form. A paid social setup that only tracks form fills is missing most of the conversion signal.
The fix is a call tracking platform (CallRail, CallTrackingMetrics, or similar) that assigns dynamic numbers per ad source, captures the call as a conversion event, and feeds the event back to Meta and the other platforms through the same CAPI pipeline.
The conversion tracking work for admission attribution is identical on the paid social side. The single integrated pipeline (CRM + call tracking + CAPI) is what gives Meta and Google enough signal to optimize despite the platform restrictions on healthcare conversion events.
How Profound Treatment drove 31 admits and a 42% drop in cost per viable in one quarter
Broad match pivot, negative keyword management, and intake-level conversion tracking turned a fragmented paid strategy into a predictable admissions engine.
Read the case study →68 viable VOBs at $4,529 cost per viable
Budget allocation framework
The right paid social budget depends on facility size, payer mix, geographic scope, and growth objective. The shape of the allocation is more consistent across operators than the dollar amount.
Total social spend as percent of total marketing. Most BH operators land between 25 and 40% of total marketing budget on paid social, with the rest split across paid search, organic, and referral source development. Operators below 25% are usually under-investing in family acquisition. Operators above 40% are usually over-rotated and missing the search and SEO layer.
Platform mix within social. Meta carries 60 to 75%. YouTube and TikTok combined carry 15 to 25%. Snap, Reddit, LinkedIn carry the remainder. Operators who try to spread evenly across all platforms tend to underperform operators who concentrate on Meta with selective supplementation.
Family vs patient split. For mixed-acuity facilities (residential + outpatient), family-first campaigns typically carry 65 to 75% of social spend with patient-first campaigns at 25 to 35%. The exact split should follow the admission mix the facility actually wants.
Testing budget vs scale budget. A healthy account runs 10 to 20% of monthly spend on creative testing (new audiences, new ad copy, new formats) and the rest on the proven combinations. Operators who run 0% testing budget plateau within 6 months. Operators who run 40% testing budget never reach scale efficiency.
Reserve for compliance disruption. The 2026 environment is volatile. Ad accounts get disabled. Audiences get suspended. Optimization events get restricted. A budget allocation that has no flexibility for compliance disruption breaks during the first incident. Most operators should plan to redeploy 10 to 20% of social spend within 30 days if a platform restriction forces a campaign rebuild.
Common mistakes that get treatment centers banned
Five mistakes account for most of the platform disables we see across BH operators.
ACCOUNT BAN RISK
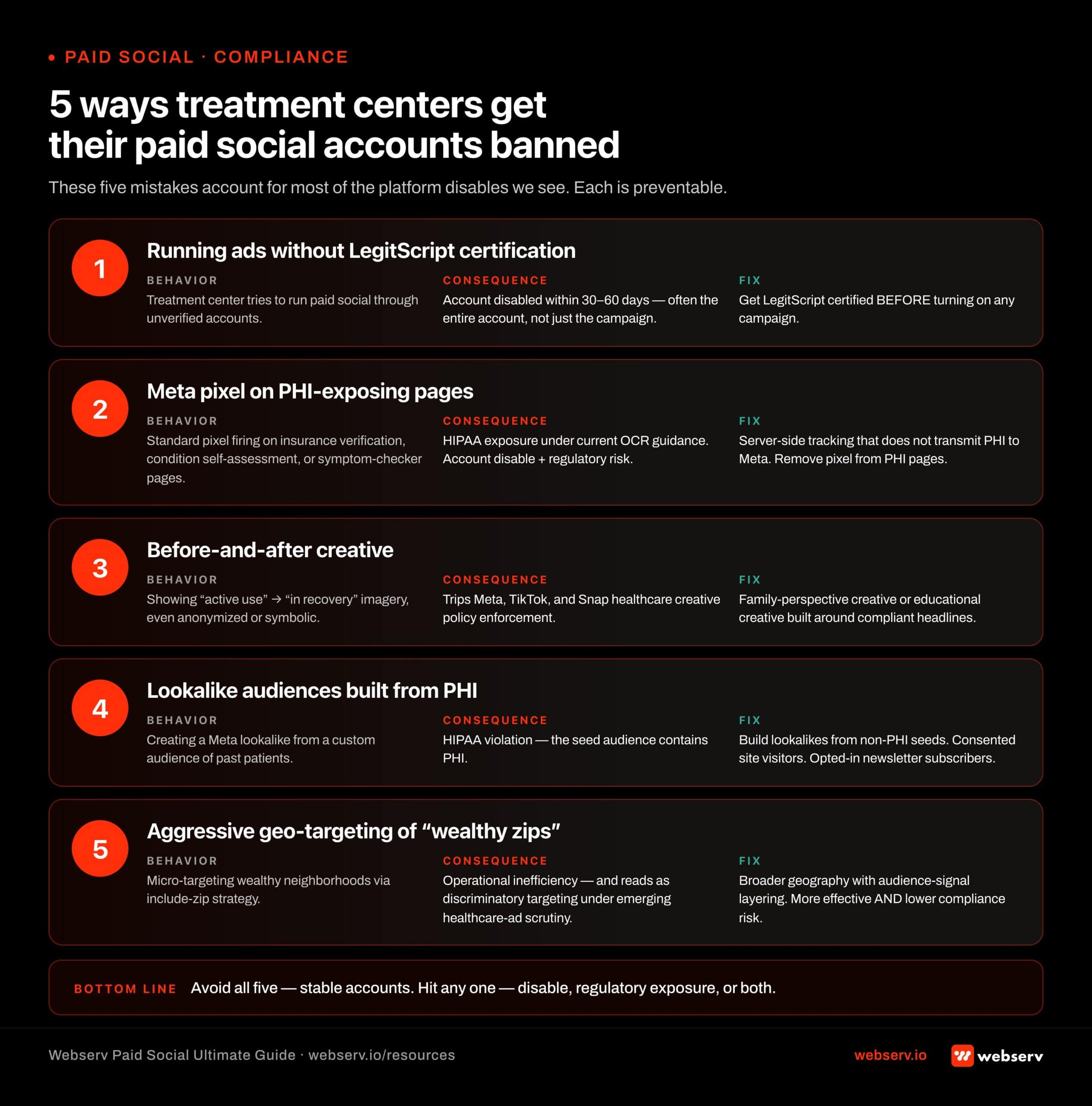
Running paid social ads without LegitScript certification is the fastest way to get a treatment center’s ad accounts disabled across Meta and TikTok. Platform reviews are getting tighter year over year — a single disable typically takes 30-90 days to resolve, and many never come back. Verify certification status before any new campaign goes live.
 Infographic titled ‘5 ways treatment centers get their paid social accounts banned’ showing the five most common compliance mistakes that lead to account disables for behavioral health paid social. Mistake 1: Running ads without LegitScript certification — treatment center tries to run paid social through unverified accounts; consequence is account disable within 30–60 days, often the entire account not just the campaign; fix is get LegitScript certified BEFORE turning on any campaign. Mistake 2: Meta pixel on PHI-exposing pages — standard pixel firing on insurance verification, condition self-assessment, or symptom checker pages; consequence is HIPAA exposure under current OCR guidance, account disable, plus regulatory risk; fix is server-side tracking that does not transmit PHI to Meta and removing pixel from PHI pages. Mistake 3: Before-and-after creative — showing ‘active use’ followed by ‘in recovery’ imagery, even anonymized or symbolic; consequence is tripping Meta, TikTok, and Snap healthcare creative policy enforcement; fix is family-perspective creative or educational creative built around compliant headlines. Mistake 4: Lookalike audiences built from PHI — creating a Meta lookalike from a custom audience of past patients; consequence is HIPAA violation because the seed audience contains PHI; fix is building lookalikes from non-PHI seeds like website visitors who consented to tracking or newsletter subscribers who opted in. Mistake 5: Aggressive geo-targeting of wealthy zips — micro-targeting wealthy neighborhoods through include-zip strategy; consequence is operational inefficiency plus can read as discriminatory targeting under emerging healthcare advertising scrutiny; fix is broader geography with audience-signal layering, which is both more effective and lower compliance risk. Footer: avoid all five and accounts stay stable, hit any one and face disable, regulatory exposure, or both.
Infographic titled ‘5 ways treatment centers get their paid social accounts banned’ showing the five most common compliance mistakes that lead to account disables for behavioral health paid social. Mistake 1: Running ads without LegitScript certification — treatment center tries to run paid social through unverified accounts; consequence is account disable within 30–60 days, often the entire account not just the campaign; fix is get LegitScript certified BEFORE turning on any campaign. Mistake 2: Meta pixel on PHI-exposing pages — standard pixel firing on insurance verification, condition self-assessment, or symptom checker pages; consequence is HIPAA exposure under current OCR guidance, account disable, plus regulatory risk; fix is server-side tracking that does not transmit PHI to Meta and removing pixel from PHI pages. Mistake 3: Before-and-after creative — showing ‘active use’ followed by ‘in recovery’ imagery, even anonymized or symbolic; consequence is tripping Meta, TikTok, and Snap healthcare creative policy enforcement; fix is family-perspective creative or educational creative built around compliant headlines. Mistake 4: Lookalike audiences built from PHI — creating a Meta lookalike from a custom audience of past patients; consequence is HIPAA violation because the seed audience contains PHI; fix is building lookalikes from non-PHI seeds like website visitors who consented to tracking or newsletter subscribers who opted in. Mistake 5: Aggressive geo-targeting of wealthy zips — micro-targeting wealthy neighborhoods through include-zip strategy; consequence is operational inefficiency plus can read as discriminatory targeting under emerging healthcare advertising scrutiny; fix is broader geography with audience-signal layering, which is both more effective and lower compliance risk. Footer: avoid all five and accounts stay stable, hit any one and face disable, regulatory exposure, or both.Running ads without LegitScript certification. This is the single biggest reason accounts get disabled. Meta and Google both require the certification before serving addiction treatment ads. Treatment centers that try to run ads through unverified accounts get caught within 30 to 60 days, and the disable often takes the entire account, not just the specific campaign.
Meta pixel on PHI-exposing pages. The pixel on a page where users enter health information (insurance verification, condition self-assessment, symptom checker) is a HIPAA exposure under the current OCR guidance. The remediation is to remove the pixel from those pages or to deploy server-side tracking that does not transmit PHI to Meta. Pages that are pure informational content (the blog, the homepage) are lower-risk but still benefit from the migration.
Before-and-after creative. Showing a person “in active use” and then “in recovery” violates Meta’s, TikTok’s, and Snap’s healthcare creative policies. Even when the imagery is anonymized or symbolic, the framing trips the policy enforcement. The compliant alternative is family-perspective creative or educational creative built around compliant ad headlines for rehab.
Lookalike audiences built from PHI. Creating a Meta lookalike from a custom audience of past patients is a HIPAA violation, because the seed audience contains PHI. The compliant lookalike is built from non-PHI audiences (website visitors who consented to tracking, newsletter subscribers who opted in for marketing) and is much smaller in seed size but compliance-safe.
Aggressive geo-targeting of “wealthy zips.” Beyond the operational inefficiency of include-zip targeting, micro-targeting wealthy neighborhoods can read as discriminatory targeting under emerging healthcare advertising scrutiny. Broader geography with audience-signal layering is both more effective and lower compliance risk.
The combined cost of these mistakes is roughly equivalent to the value of running the program correctly in the first place. Operators who avoid these five mistakes usually maintain stable accounts. Operators who hit any one of them face account disables, regulatory exposure, or both.
WHAT WORKING REHAB PAID SOCIAL DOES
- Active LegitScript certification verified before any campaign launches
- HIPAA-safe pixel and CAPI deployment with signed BAAs
- Compliance-reviewed ad copy on every creative variant
- Targeting that respects 18+ and no-retargeting health restrictions
- Designated internal owner for platform policy compliance
WHAT BANNED ACCOUNTS DID
- Run paid social through any platform before LegitScript clears
- Standard Meta pixel deployment without HIPAA review
- Outcome claims (“we save lives,” “guaranteed recovery”) in ad copy
- Retargeting audiences built from health-related site visitors
- Compliance treated as an agency-handles-it problem
How to evaluate a paid social agency for behavioral health
If you are hiring or auditing an agency for behavioral health paid social, six questions separate the operators who understand 2026 from the operators who are still running 2020 playbooks.
Operators evaluating agencies should also read our honest review of marketing agencies for rehabs and our Google Ads strategy guide, because most BH treatment center programs cannot run paid social in isolation. The strongest accounts integrate paid social with paid search and organic surfaces. Operators who want to skip the evaluation work can start from our scored ranking of the top paid social ad agencies for rehab marketing, which applies the same six diligence questions to the firms already running 2026 stacks.
- Show me your last LegitScript-certified account onboarding timeline. Real BH paid social agencies onboard certification-aware. Agencies that have not navigated LegitScript should not be running your social.
- Walk me through your Conversions API implementation on a current client. The implementation should be server-side, identity-hashed, and PHI-aware. If the answer involves the Meta pixel as the primary tracking layer, the agency has not updated for 2026.
- Show me a Meta creative that was disabled in the last 90 days and explain why. Agencies that say none of their creative has been disabled either run small enough to fly under enforcement or are not running aggressively enough to scale. The right answer is “here is the one that got flagged, here is what we changed, here is the version that ran.”
- What is your family-vs-patient targeting split for residential programs? Should be 65-75% family-first. Agencies that run patient-first for residential do not understand the buyer.
- How do you handle phone-call conversions for the platforms that do not natively support them? Should involve CallRail or equivalent, server-side CAPI integration, and identity matching. If the answer is “we just use Meta’s lead form,” the attribution layer is incomplete.
- What is your protocol when Meta disables an account? Real agencies have a playbook for this. Most BH accounts get disabled at least once. The agencies that recover accounts inside 14 days are the ones with the relationships, the documentation, and the certification stack already in place.
The agencies that answer all six well are the ones who can actually run BH paid social in 2026. The agencies that fumble even two of the six are usually the ones whose clients are reading this guide because their account just got disabled for the third time.
Frequently asked questions about paid social for treatment centers
Can we still run Meta ads for our treatment center in 2026?
Yes, with the right certification stack. The combination of LegitScript certification, Meta addiction treatment approval, server-side Conversions API tracking, and compliant creative makes BH advertising on Meta both possible and effective. Treatment centers running this stack are scaling on Meta in 2026 at unit economics similar to or better than 2022.
What does not work in 2026 is the pre-2024 setup: pixel-based tracking, direct-pitch creative, narrow lookalike audiences from patient data, and unverified ad account ownership. Operators running that setup get disabled, lose accounts, and pay agencies to rebuild what should have been built right the first time.
The right question is not “can we run Meta ads” but “can we run them with the operational maturity 2026 requires.” If your agency cannot describe the CAPI setup, the LegitScript timeline, and the family-first creative strategy in concrete terms, you are paying for legacy execution at 2026 prices.
How does HIPAA enforcement in 2026 change what we can do on paid social?
The shift is from pixel-based tracking to server-side tracking with strict PHI controls. The Meta pixel and similar browser-side trackers cannot be used on pages that handle protected health information without exposing the operator to HIPAA enforcement risk. The OCR scrutiny of tracking technologies on healthcare sites intensified in 2025 and accelerated in 2026, with $4.18 million in penalties imposed in the most recent enforcement year.
The practical implications: remove the pixel from PHI-exposing pages (insurance verification, condition pages, treatment matching tools). Deploy server-side CAPI for all major paid social platforms. Use hashed identity matching to feed conversions back to the platforms without transmitting PHI. Update Business Associate Agreements with any vendor that touches the tracking layer.
The operators who completed this migration in 2024 are running compliant programs in 2026. The operators who did not are now doing the migration under enforcement pressure, which is more expensive and slower than doing it proactively.
What is the right monthly budget to start with on paid social for a treatment center?
The right answer depends on facility size and admission economics, but the floor is usually $8,000 to $15,000 a month in paid social spend to generate enough data for meaningful optimization. Below $8,000 a month, the platforms cannot serve enough impressions to optimize the campaigns effectively, and the data sparseness mirrors the small-budget Smart Bidding problem in Google Ads max-conversions bidding.
For most residential treatment centers, the working range is $15,000 to $40,000 a month in paid social spend, with 60 to 75% of that on Meta and the rest split across the other platforms. Multi-location operators or higher-volume PHP programs often run $50,000 to $100,000 monthly with stable economics.
The scaling path is to start at the lower end of the range, prove unit economics over 90 days, and increase budget in 25 to 40% monthly increments once the cost per admission is stable. Aggressive scaling without proven economics is the most common way to burn through budget without proportional admission growth.
How do we handle ad accounts that get disabled by Meta?
Plan for it as part of the operational reality. Most BH treatment centers running aggressive paid social on Meta get at least one disable over a 24-month period. The fix has four parts.
First, do not panic. The disable is recoverable for compliant accounts. Pulling spend from the rest of the marketing program in panic mode usually makes things worse. Second, identify the specific policy violation. The Meta notification is sometimes vague. Compare the recently-served creative against the addiction treatment policy and the healthcare advertising policy. Look at the audience configurations. Check whether the LegitScript or Meta certification has lapsed.
Third, submit an appeal with documentation of the certification stack and the policy compliance. The appeal flow is documented but the response times have been slower in 2026 than in prior years. Expect 7 to 21 days for resolution on a clean appeal. Fourth, if the appeal fails, rebuild on a fresh ad account with a different Business Manager structure, with all of the compliance issues from the original account remediated. Most agencies should have a contingency Business Manager already provisioned for clients in this category.
Should we run TikTok and Snap if our patient demographic is older?
Probably not, or only at minimal allocation for brand awareness. TikTok and Snap are most effective for treatment centers focused on 18-29 patient populations. For centers focused on 35+ patients, the audience-fit gap is too large to justify significant spend.
The exception is if the family member is in the younger demographic, which happens for centers treating older patients whose adult children are doing the searching. In that case, TikTok and Snap can have a role at 5 to 10% of social spend, but Meta and YouTube usually still outperform them on family-decision-maker targeting.
Older patient populations (50+) are usually best reached through Meta, YouTube, and selective LinkedIn (for referral sources). The TikTok/Snap allocation should be data-driven from the facility’s actual admission demographics, not from a generic best-practices framework.
What does the compliant content layer look like alongside paid social?
Paid social works better when there is an organic content layer that prospects can land on after the ad click. The landing page is the conversion surface, but the surrounding site content is the trust surface. Operators who try to drive paid social traffic to thin landing pages with no supporting content underneath convert at lower rates than operators with a deep content library.
The implication is to invest in the content layer in parallel with the paid social layer. Service pages, location pages, and a real blog produce the trust signals that make the paid social conversion path work. The commercial layer feeds the conversion, the content layer earns the trust.
For operators with limited content budget, the paid social ROI is much better when even modest content investment runs alongside the ad spend. The two channels are complementary, not competing. If you want a second opinion on whether your paid social setup is configured for 2026 compliance and 2026 optimization, reach out for a social audit and we can walk through your tracking layer, creative library, and platform compliance posture before the next core platform update lands.
The perspective in this article comes from 9 years working exclusively inside behavioral health.
We are a team built by people in recovery who understand that behind every admission is someone asking for help. If that resonates, get to know us.
Mitch Marowitz is the Director of Paid Media at Webserv, a digital marketing agency for treatment centers.