A treatment center founder asked me two weeks ago which paid channel he should start with. He had $18,000 a month in marketing budget for the first time, a clean 32-bed residential facility, a JCAHO accreditation, and a partial LegitScript application sitting on his desk.
He wanted to know whether to put the budget into Google Ads or Facebook Ads. The agency he had been talking to had pitched a 50-50 split across both, with the implication that more channels meant more admissions.
I told him to put $15,000 into Google Ads first, hold the remaining $3,000 in reserve, and let Facebook Ads wait three to six months. The reasoning is what this piece is about. The answer is not always Google first.
The answer is Google first for roughly 85 percent of behavioral health treatment centers, with specific exceptions worth understanding. The 50-50 split his agency had pitched was the wrong starting point. It ignored what each channel actually does in the admission funnel and how the channels feed each other.
If you are running a treatment center with a fixed paid media budget and you are trying to decide which channel to launch first, the next 2,000 words are the framework I use across every new client engagement at Webserv’s paid search practice.
It is opinionated, and the opinion is informed by 18 months of comparative spend data across roughly 40 behavioral health accounts.
Key Takeaways
- For most treatment centers, Google Ads should launch first. The buyer in this category is searching with high commercial intent, the conversion path is short, and the unit economics are cleaner at small budgets than Facebook Ads can match.
- Facebook Ads belongs in the program, but most operators benefit from waiting three to six months after Google Ads launches before adding Meta. The Google Ads conversion data feeds Meta’s audience signals, and the Meta compliance setup takes longer than Google’s anyway.
- The 2026 compliance environment makes the sequencing matter more than it used to. Meta’s healthcare advertising restrictions, the HHS-OCR tracking technology enforcement, and the Conversions API infrastructure requirements push Meta’s time-to-launch from 4 weeks to 8 to 12 weeks.
- Three specific exceptions argue for launching Facebook Ads first: facilities with mature commercial infrastructure already running, brand-awareness campaigns for new modalities or new markets, and operators focused on adolescent or young adult patient populations.
- The right framing is not “Google or Facebook.” It is “Google first, then Facebook, with both eventually carrying weight.” The wrong framing is the 50-50 split most agencies pitch.
What each channel actually does in the admission funnel
The comparison only makes sense if both channels are doing the job they are designed for. The mistake most operators inherit from agency pitches is treating Google Ads and Facebook Ads as interchangeable tools that both produce admissions. They are not interchangeable.
Vetting specialists is often faster than refereeing the split yourself; our roundup of Google Ads agencies for treatment centers screens for exactly this discipline.
They produce different things at different stages of the buyer funnel.
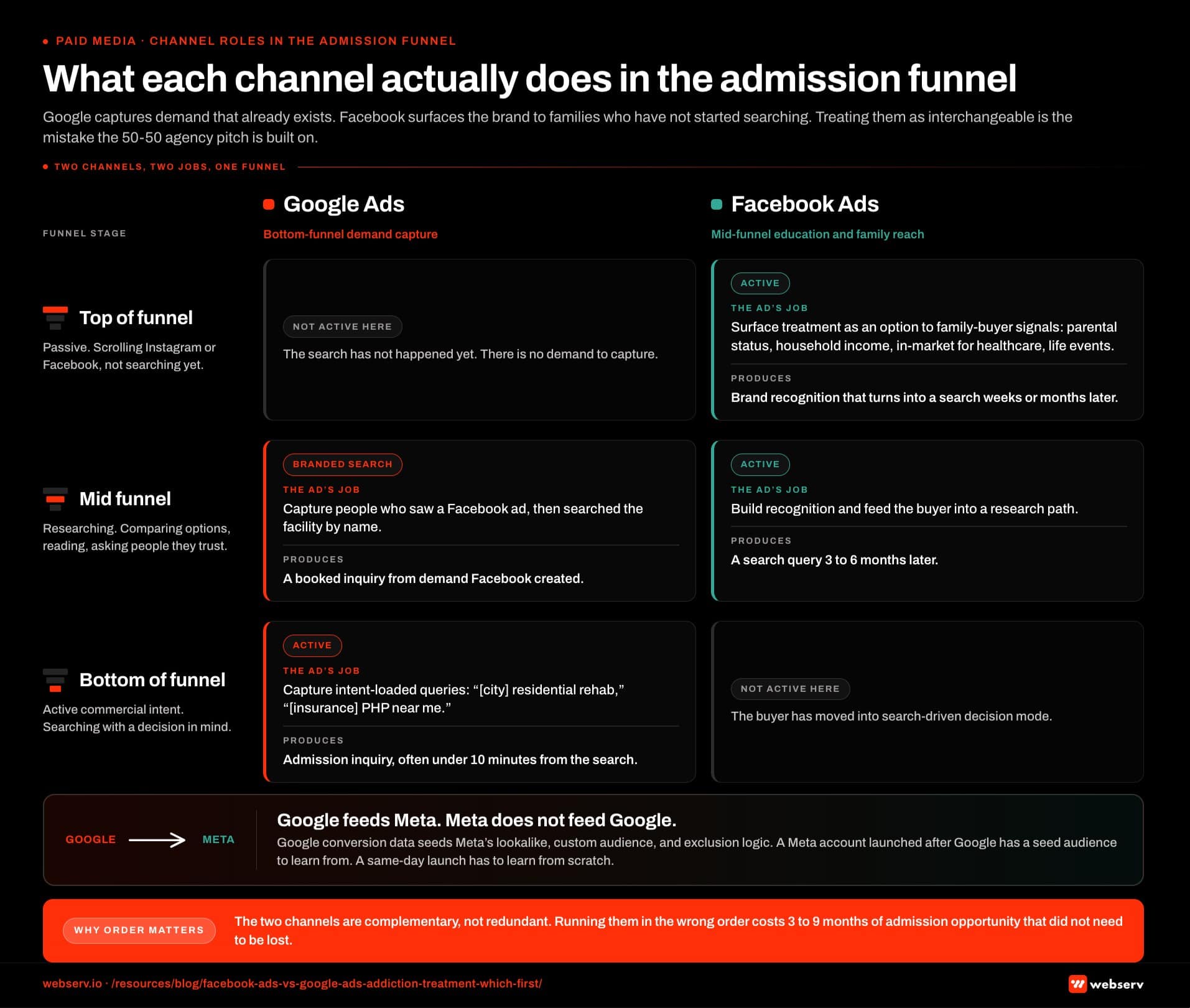 Infographic titled ‘What each channel actually does in the admission funnel’ showing a two-track funnel diagram comparing Google Ads on the left as a bottom-funnel commercial intent capture channel and Facebook Ads on the right as a mid-funnel education and family-member targeting channel. Top of funnel passive awareness stage: Google Ads is not active because the search has not happened yet, while Facebook Ads is active and surfaces treatment as an option to family-buyer audience signals including parental status, household income, in-market for healthcare, and life events, reaching a buyer who is scrolling rather than searching. Mid-funnel research stage: Google Ads captures branded search from users who saw a Meta ad and searched the facility name, while Facebook Ads builds brand recognition and feeds the user into a research path that produces a search query three to six months later. Bottom of funnel commercial intent stage: Google Ads is active and captures city-residential-rehab and insurance-PHP-near-me queries with a path from query to admission inquiry often under ten minutes, while Facebook Ads is not active because the user has moved into search-driven decision mode. Channel-feeds-the-other layer: Google conversion data seeds Meta’s lookalike, custom audience, and exclusion logic, while Meta data does not import into Google so the data flow is one-way. Left-track Google callout: the buyer is already in the funnel and Google Ads makes sure the facility is in the consideration set. Right-track Facebook callout: the buyer is not yet in the funnel and Facebook Ads pulls them toward it with a longer conversion path and an admission inquiry that happens weeks or months after the first ad exposure. Center bridge callout: Google feeds Meta and Meta does not feed Google, which is why the sequencing matters. Bottom strip callout: the two channels are complementary not redundant, and running them in the wrong order costs the operator three to nine months of admission opportunity that does not need to be lost.
Infographic titled ‘What each channel actually does in the admission funnel’ showing a two-track funnel diagram comparing Google Ads on the left as a bottom-funnel commercial intent capture channel and Facebook Ads on the right as a mid-funnel education and family-member targeting channel. Top of funnel passive awareness stage: Google Ads is not active because the search has not happened yet, while Facebook Ads is active and surfaces treatment as an option to family-buyer audience signals including parental status, household income, in-market for healthcare, and life events, reaching a buyer who is scrolling rather than searching. Mid-funnel research stage: Google Ads captures branded search from users who saw a Meta ad and searched the facility name, while Facebook Ads builds brand recognition and feeds the user into a research path that produces a search query three to six months later. Bottom of funnel commercial intent stage: Google Ads is active and captures city-residential-rehab and insurance-PHP-near-me queries with a path from query to admission inquiry often under ten minutes, while Facebook Ads is not active because the user has moved into search-driven decision mode. Channel-feeds-the-other layer: Google conversion data seeds Meta’s lookalike, custom audience, and exclusion logic, while Meta data does not import into Google so the data flow is one-way. Left-track Google callout: the buyer is already in the funnel and Google Ads makes sure the facility is in the consideration set. Right-track Facebook callout: the buyer is not yet in the funnel and Facebook Ads pulls them toward it with a longer conversion path and an admission inquiry that happens weeks or months after the first ad exposure. Center bridge callout: Google feeds Meta and Meta does not feed Google, which is why the sequencing matters. Bottom strip callout: the two channels are complementary not redundant, and running them in the wrong order costs the operator three to nine months of admission opportunity that does not need to be lost.Google Ads captures existing commercial demand. The user searching “[city] residential rehab” or “[insurance] PHP near me” is in active treatment-seeking mode. They have a specific need. They are clicking results to find a facility to call.
The ad’s job is to be one of the results they click and to route them to a service page where they convert. The buyer is already in the funnel. Google Ads makes sure your facility is in the consideration set.
Facebook Ads creates demand or accelerates research-stage demand. The user scrolling Instagram or Facebook is not actively searching for treatment. They are reached because their audience signals (in-market for healthcare, parental status, life events, household income) match a family-buyer profile.
The ad’s job is to surface treatment as an option, build brand recognition, and feed the user into a research path that may produce a search query weeks or months later. The buyer is not yet in the funnel. Facebook Ads pulls them toward it.
The two channels are complementary, not redundant. A treatment center running both well has Google capturing the high-intent searches and Facebook surfacing the brand to families who have not yet started searching. The compound effect is meaningful, which is why most mature programs eventually run both.
The sequencing question is different from the question of whether to run both. Sequencing matters because the channels have different time-to-launch, different time-to-positive-economics, and different data dependencies on each other.
Running them in the wrong order costs the operator 3 to 9 months of admission opportunity that does not need to be lost.
“Running them in the wrong order costs the operator 3 to 9 months of admission opportunity that does not need to be lost.”
Preston Powell, Chief Executive Officer, Webserv
Why Google Ads first for most treatment centers
GOOGLE FIRST WHEN
- Median commercial-intent operator with existing brand and payer relationships
- Sub-$25K/month budget and a short runway to prove ROI
- Intake team ready to answer “[insurance] residential rehab in [city]” calls today
- Service pages and location pages already in place and tracking properly
FACEBOOK FIRST WHEN
- Alumni and family-of-user awareness campaigns where demand does not exist yet
- Modality launches (TMS, ketamine, IOP virtual) that families are not searching for by name
- Reactivation of past inquiries with warm audiences and long consideration windows
- Established brand with a content library that can carry the longer conversion path
Five reasons drive the “Google first” recommendation for the median behavioral health operator.
The demand already exists. The SAMHSA 2023 National Survey on Drug Use and Health found 48.5 million Americans aged 12 or older met criteria for a substance use disorder in the prior year, with only about 12.8 million receiving any substance use treatment.
That treatment gap of roughly 73 percent is mostly searching at the commercial end of the funnel, not browsing social media. Capturing existing demand on Google is faster economics than creating demand on Facebook.
The conversion path is shorter. A family member searching “[insurance] residential rehab in [city]” clicks a result, lands on a service page, calls the intake line. The path from query to admission inquiry is often under 10 minutes.
Facebook’s conversion path is longer. The user has to be moved from passive scrolling to active research, then through several touches, before the admission inquiry happens. Short conversion paths are more forgiving of small budgets, less data, and earlier-stage account maturity.
The compliance gate is the same but better documented. Both Google Ads and Meta require LegitScript certification for addiction treatment advertising. Google’s policy is more documented, with clearer setup instructions, more agency familiarity, and a faster review cycle for newly certified advertisers.
Meta’s policy adds an additional in-house review on top of LegitScript that can push time-to-launch from 4 weeks to 8 to 12 weeks. The LegitScript certification process is identical for both platforms, but the operational ramp on Google is faster.
The tracking infrastructure is simpler. Google Ads conversion tracking via tag manager and call tracking integration is a well-trodden setup that most agencies can deploy in a week. Meta’s server-side Conversions API setup is more complex and takes 3 to 6 weeks to deploy correctly.
Operators running Meta without the CAPI infrastructure are running with degraded signal in the 2026 environment, which is a worse position than not running Meta at all.
The unit economics are cleaner at small budgets. Below $15,000 a month in spend, Google Ads tends to produce more predictable cost-per-admission economics than Meta.
Meta’s optimization layer needs more conversion volume to learn from than Google’s manual CPC or thin-data Smart Bidding setups. Small-budget Meta accounts often run at $400 to $800 cost-per-conversion variance while Google runs at $200 to $400 variance.
The cleaner economics matter when the budget is small enough that variance becomes existential.
When Facebook Ads goes first instead
Three specific exceptions argue for launching Meta before Google.
The facility already has mature commercial infrastructure running. A treatment center with an established Google Ads account (12+ months of conversion data), strong organic search visibility, and a working service-page conversion path is past the foundation work. For that operator, the next paid channel is Meta, not more Google.
The Google account is already capturing the demand that exists. The Meta account adds the brand-awareness layer that creates new demand.
Brand-awareness for a new modality or new market. A facility launching a new clinical specialty (TMS, ketamine-assisted therapy, EMDR-led residential) or opening in a new geographic market often does not have enough commercial search volume yet to make Google Ads productive.
The search demand has to be created before it can be captured.
Meta Ads with educational creative on the new modality or market can build the awareness layer that produces search queries 3 to 6 months later. This is a brand investment, not a direct-response one, and the unit economics are different.
Adolescent or young adult patient acquisition. Facilities focused on patients ages 18 to 29 (residential adolescent programs, college-aged early-intervention, young-adult dual-diagnosis) have a buyer who is reached more efficiently on Instagram, TikTok, and Snap than on Google.
The family member in this segment is also younger (often a sibling or peer, not a parent), and the search behavior is less mature than the adult-treatment segment. Meta and the rest of the social stack carry more weight in the channel mix from day one for these operators.
For operators outside these three exceptions, the Google-first recommendation holds. Operators inside one of these exceptions should still run Google Ads eventually, but the launch order can flip to Meta first.
The complete Google Ads strategy guide and the ultimate guide to social advertising for rehabs cover the channel-specific playbooks once the sequencing decision is made.
The 2026 compliance environment changed the math
Two factors in the 2026 environment made the Google-first recommendation stronger than it was in 2022.
The first is the tightening of Meta’s healthcare advertising posture. Per the Meta Transparency Center policy on drug and alcohol addiction treatment advertising, substance use treatment sits in the most restrictive sensitive category, with the 2026 wave adding restrictions on lead-generation campaigns specifically.
 Infographic titled ‘The 2026 compliance math: time to launch’ showing two horizontal timelines comparing Google Ads time-to-launch of roughly four weeks against Meta Ads time-to-launch of eight to twelve weeks. Top timeline Google Ads: week zero kickoff to week four through six optimized campaigns live, with a single compliance gate marker for LegitScript certification at roughly week two; LegitScript runs in parallel with account build and rarely blocks the Google launch window. Bottom timeline Meta Ads: week zero kickoff to week eight through twelve optimized campaigns live, with three stacked compliance gates along the bar; Meta healthcare advertising in-house review overlaps weeks two through six, HHS-OCR tracking technology remediation overlaps weeks two through eight, and Conversions API server-side infrastructure deploys across weeks three through eight. Top-timeline callout: LegitScript certification is the gate underneath both channels, with the sixty to ninety day application running in parallel with account build. Bottom-timeline callout: three stacked compliance gates on Meta drive the eight to twelve week launch, including Meta healthcare advertising in-house review, HHS-OCR tracking technology remediation, and Conversions API server-side deploy, each taking weeks of operational work that did not exist in 2022. Gate-specific callout on HHS-OCR: the Meta pixel on a PHI-handling page is a HIPAA exposure under current OCR guidance, and remediation requires server-side CAPI plus confirmation that no PHI flows to Meta in URLs or event parameters. Bottom strip callout: operators launching Meta in 2026 with a four-week timeline are launching with degraded signal, blocked optimization events, or HIPAA exposure, and the eight to twelve week timeline is the floor for compliant launch not the ceiling.
Infographic titled ‘The 2026 compliance math: time to launch’ showing two horizontal timelines comparing Google Ads time-to-launch of roughly four weeks against Meta Ads time-to-launch of eight to twelve weeks. Top timeline Google Ads: week zero kickoff to week four through six optimized campaigns live, with a single compliance gate marker for LegitScript certification at roughly week two; LegitScript runs in parallel with account build and rarely blocks the Google launch window. Bottom timeline Meta Ads: week zero kickoff to week eight through twelve optimized campaigns live, with three stacked compliance gates along the bar; Meta healthcare advertising in-house review overlaps weeks two through six, HHS-OCR tracking technology remediation overlaps weeks two through eight, and Conversions API server-side infrastructure deploys across weeks three through eight. Top-timeline callout: LegitScript certification is the gate underneath both channels, with the sixty to ninety day application running in parallel with account build. Bottom-timeline callout: three stacked compliance gates on Meta drive the eight to twelve week launch, including Meta healthcare advertising in-house review, HHS-OCR tracking technology remediation, and Conversions API server-side deploy, each taking weeks of operational work that did not exist in 2022. Gate-specific callout on HHS-OCR: the Meta pixel on a PHI-handling page is a HIPAA exposure under current OCR guidance, and remediation requires server-side CAPI plus confirmation that no PHI flows to Meta in URLs or event parameters. Bottom strip callout: operators launching Meta in 2026 with a four-week timeline are launching with degraded signal, blocked optimization events, or HIPAA exposure, and the eight to twelve week timeline is the floor for compliant launch not the ceiling.Lower-funnel optimization events (Purchase, Lead) are blocked or limited for the sensitive category. Meta accounts have to optimize on upper-funnel events and feed conversion signal through the Conversions API instead of the pixel.
The setup work for this is significant. Operators launching Meta in 2026 should expect 8 to 12 weeks from kickoff to optimized campaigns, versus 4 to 6 weeks for Google. The compliance overhead has shifted the time-to-launch calculus in Google’s favor.
The second factor is HHS-OCR’s intensified enforcement of HIPAA tracking technology rules. Per the HHS guidance on HIPAA-regulated online tracking, the Meta pixel on a page that handles protected health information is a HIPAA exposure under current OCR guidance.
The remediation (remove the pixel from PHI pages, deploy server-side CAPI, confirm no PHI flows to Meta in URLs or event parameters) takes weeks and requires careful technical work.
Operators that need a deeper playbook on the compliant setup can see HIPAA-compliant Facebook Ads for addiction treatment centers for the full breakdown.
Google’s tracking layer carries similar exposure but is somewhat less scrutinized because Google’s conversion tagging defaults are more compatible with HIPAA controls when configured correctly. The compliance posture across both platforms needs careful attention regardless. The operational lift to get Meta compliant is heavier.
The combined effect is that “Google first” is now both a strategic recommendation (capture demand before creating it) and an operational one (Meta takes longer to launch correctly).
What the channels actually feed each other
The sequencing recommendation is also informed by how the two channels feed each other when both are running.
Google Ads produces clean conversion data: form fills, phone calls, admission inquiries with full attribution. That data is the seed audience for Meta’s optimization layer.
A Meta account launched 6 months after Google has access to a custom audience of converters that the algorithm can use to find similar prospects, build lookalikes from, and exclude from creative variants. A Meta account launched alongside Google has no such seed audience and has to learn from scratch.
The 6-month Google-first head start gives Meta a much better launch position than a same-day launch does.
Operators who sequence in this order see Meta CPA stabilize 3 to 5 weeks faster than operators who launch both at once. The Meta algorithm has real conversion data to learn from on day one of the Meta launch.
The reverse direction does not work the same way. Meta data does not feed Google’s optimization layer because Google does not import Meta conversion events. Meta-first does not produce a Google launch advantage. Google-first produces a Meta launch advantage. This asymmetry is part of why the sequencing matters.
How Profound Treatment drove 31 admits and a 42% drop in cost per viable in one quarter
Broad match pivot, negative keyword management, and intake-level conversion tracking turned a fragmented paid strategy into a predictable admissions engine.
Read the case study →68 viable VOBs at $4,529 cost per viable
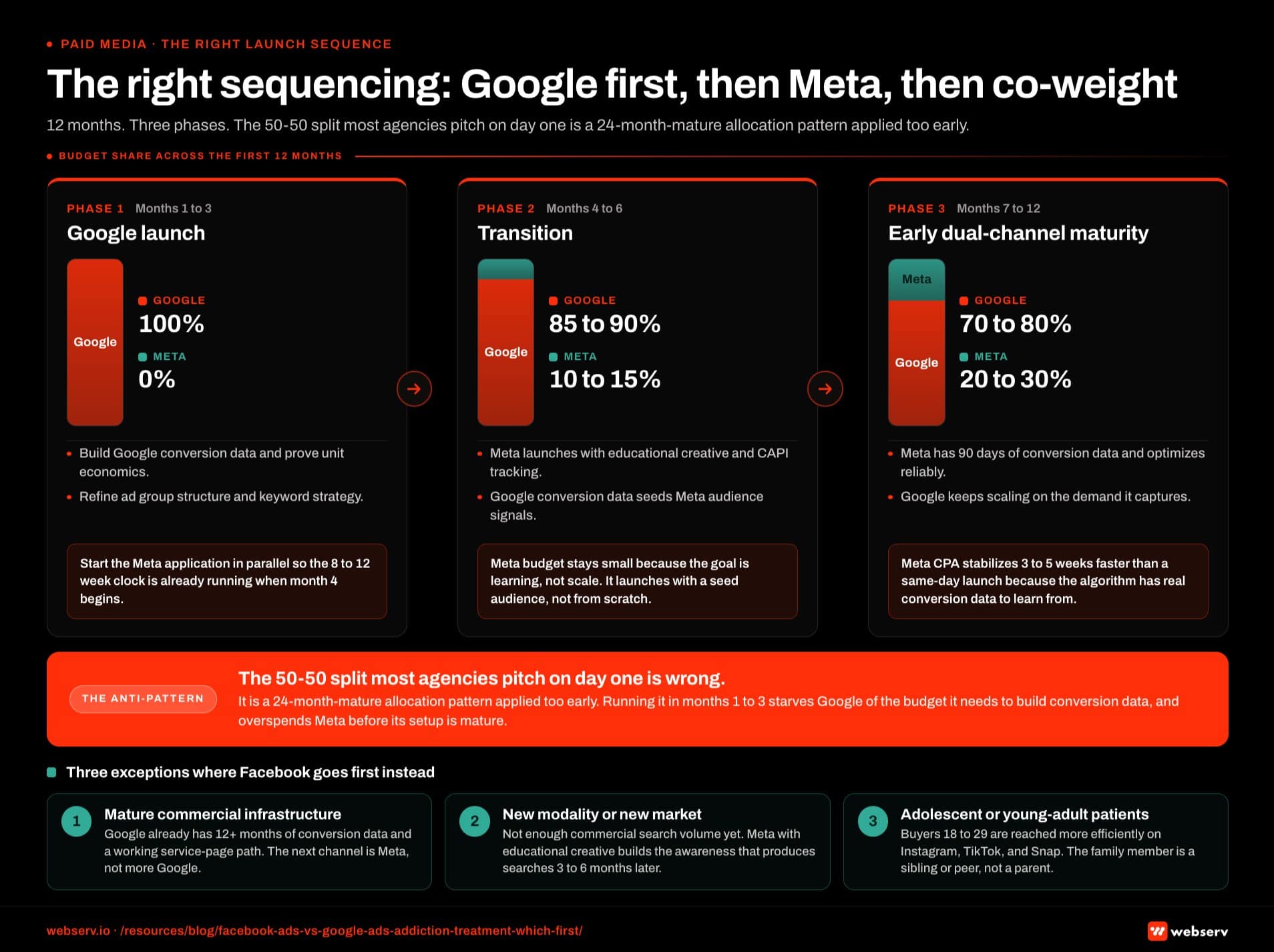 Infographic titled ‘The right sequencing: Google first, then Meta, then co-weight’ showing a three-phase horizontal timeline of the right paid media launch sequence across the first twelve months, with a budget-share stacked bar at each phase. Phase one Google launch in months one to three: 100 percent Google and zero percent Meta; the operator builds Google conversion data, proves unit economics, refines ad group structure and keyword strategy, finalizes LegitScript certification, and starts the Meta application in parallel. Phase two transition in months four to six: 85 to 90 percent Google and 10 to 15 percent Meta; Meta launches with educational creative, audience signals layered including parental status, household income, and in-market for healthcare, and conversion tracking via the Conversions API; the Meta budget is small because the goal is learning rather than scale, and Google conversion data feeds Meta audience signals. Phase three early dual-channel maturity in months seven to twelve: 70 to 80 percent Google and 20 to 30 percent Meta; Meta has ninety days of conversion data, the algorithm is optimizing reliably, the budget can grow, Google continues to scale on the demand it captures, and the two channels are now mutually reinforcing. Phase one in-bar callout: 100 percent Google for months one to three to build conversion data, prove unit economics, and start the Meta application in parallel so the eight to twelve week clock is running when month four begins. Phase two in-bar callout: Meta launches at ten to fifteen percent of budget, the goal is learning not scale, and Google conversion data seeds Meta’s audience signals on day one of the Meta launch. Phase three in-bar callout: Meta cost-per-acquisition stabilizes three to five weeks faster for operators who sequenced Google first than for operators who launched both at once, because the Meta algorithm has real conversion data to learn from. Anti-pattern callout strip in brand red along the bottom: the fifty-fifty split most agencies pitch on day one is wrong because it is a twenty-four-month-mature allocation pattern applied prematurely, and running it in months one to three starves Google of the budget it needs to build conversion data while overspending Meta before its setup is mature. Sidebar block with three exceptions where Facebook goes first instead: facilities with mature commercial infrastructure already running, brand-awareness campaigns for new modalities or new markets, and operators focused on adolescent or young adult patient populations.
Infographic titled ‘The right sequencing: Google first, then Meta, then co-weight’ showing a three-phase horizontal timeline of the right paid media launch sequence across the first twelve months, with a budget-share stacked bar at each phase. Phase one Google launch in months one to three: 100 percent Google and zero percent Meta; the operator builds Google conversion data, proves unit economics, refines ad group structure and keyword strategy, finalizes LegitScript certification, and starts the Meta application in parallel. Phase two transition in months four to six: 85 to 90 percent Google and 10 to 15 percent Meta; Meta launches with educational creative, audience signals layered including parental status, household income, and in-market for healthcare, and conversion tracking via the Conversions API; the Meta budget is small because the goal is learning rather than scale, and Google conversion data feeds Meta audience signals. Phase three early dual-channel maturity in months seven to twelve: 70 to 80 percent Google and 20 to 30 percent Meta; Meta has ninety days of conversion data, the algorithm is optimizing reliably, the budget can grow, Google continues to scale on the demand it captures, and the two channels are now mutually reinforcing. Phase one in-bar callout: 100 percent Google for months one to three to build conversion data, prove unit economics, and start the Meta application in parallel so the eight to twelve week clock is running when month four begins. Phase two in-bar callout: Meta launches at ten to fifteen percent of budget, the goal is learning not scale, and Google conversion data seeds Meta’s audience signals on day one of the Meta launch. Phase three in-bar callout: Meta cost-per-acquisition stabilizes three to five weeks faster for operators who sequenced Google first than for operators who launched both at once, because the Meta algorithm has real conversion data to learn from. Anti-pattern callout strip in brand red along the bottom: the fifty-fifty split most agencies pitch on day one is wrong because it is a twenty-four-month-mature allocation pattern applied prematurely, and running it in months one to three starves Google of the budget it needs to build conversion data while overspending Meta before its setup is mature. Sidebar block with three exceptions where Facebook goes first instead: facilities with mature commercial infrastructure already running, brand-awareness campaigns for new modalities or new markets, and operators focused on adolescent or young adult patient populations.The right framework for budget allocation as both channels mature
After 6 to 12 months of running Google Ads alone, most BH operators are ready to layer Meta on top. The allocation framework that works in my experience is:
Months 1-3 (Google launch): 100 percent of paid budget on Google Ads. Build conversion data, prove unit economics, refine the ad group structure and keyword strategy. LegitScript certification finalized, Meta application started in parallel.
Months 4-6 (transition): 85 to 90 percent Google, 10 to 15 percent Meta. Meta launches with educational creative, audience signals layered (parental status, household income, in-market for healthcare), conversion tracking via CAPI. The Meta budget is small because the goal is learning, not scale.
Months 7-12 (early dual-channel maturity): 70 to 80 percent Google, 20 to 30 percent Meta. Meta has 90 days of conversion data, the algorithm is optimizing reliably, and the budget can grow. Google continues to scale on the demand it captures. The two channels are now mutually reinforcing.
Months 12+ (mature dual-channel): 60 to 70 percent Google, 30 to 40 percent Meta. Both channels are at scale, with Meta carrying meaningful share of the family-buyer awareness layer and Google capturing the resulting search demand plus the existing demand.
Operators at this stage often expand to TikTok, Snap, Reddit, or YouTube depending on patient demographics, and the broader paid media program can absorb the new channels with the Google and Meta foundations in place.
The 50-50 split that agencies often pitch on day one is a 24-month-mature allocation pattern applied prematurely. Running it in months 1-3 starves Google of the budget it needs to build conversion data while overspending Meta before its setup is mature.
The shared infrastructure that supports both
Some setup work is shared across both channels and matters regardless of which launches first.
LegitScript certification. Both platforms require it. The application process takes 60 to 90 days, and the cost is roughly $3,000 to $5,000 annually depending on facility size. This is the gate underneath both channels.
Operators trying to run either Google Ads or Meta without it eventually face account disables, and the recovery is slower than the original setup.
Conversion tracking with phone-call integration. Roughly 60 to 75 percent of BH admission inquiries come in by phone. A tracking layer that only captures form submissions misses most of the signal. The conversion tracking setup with CallRail feeds both Google and Meta and is foundational to either channel.
Service page conversion infrastructure. Both channels send traffic to landing pages. If the landing pages are thin, the channels both underperform regardless of which launches first. The service-page work that drives admission inquiries is the same regardless of which channel sends the traffic.
Compliant creative library. Compliant ad headlines across both platforms follow similar principles even though the formats differ.
Operators who invest in a compliant creative library early can deploy it across both channels as each launches, and the paid social work inherits the same creative discipline as the Google account when Meta does launch.
The implication is that some of the launch-prep work for Meta happens during the Google launch period and does not have to wait for the Meta launch window.
The 6-month Google-first sequence is not 6 months of idle Meta planning. It is 6 months of foundational work that benefits Meta when it does launch.
For operators thinking about how this paid sequencing fits inside the broader behavioral health marketing program, paid is one of five disciplines that compound. The sequencing inside paid is what this piece is about. The sequencing across organic, paid, content, admissions ops, and creative is a longer conversation.
Frequently Asked Questions
Will we miss admissions by waiting on Facebook Ads?
Some, but less than most operators fear. The admissions that come from Meta tend to lag the ad exposure by weeks to months because the buyer funnel is longer. A 3-to-6-month wait on Meta delays the start of that pipeline, but the Google Ads program is capturing the high-intent demand that would have converted faster anyway.
The net admission opportunity lost in the waiting period is usually 8 to 15 percent of what Meta would eventually produce. That pool is largely recovered in months 7 to 12 once Meta launches with stronger fundamentals.
The framing that helps operators think about this clearly is that the cost of waiting is measured in delayed pipeline, not in lost demand. The demand is still there 6 months from now. The Meta program will reach it then. Running Meta early with weak fundamentals captures less of the demand than running it later with strong fundamentals. The exceptions where waiting hurts more are the three scenarios covered above.
What if we already have Google Ads running but underperforming?
Fix Google before adding Meta. Adding a second channel on top of a broken first channel does not improve the first channel and gives the second channel weaker conversion signal to learn from.
The diagnostic order is to audit the Google account first (campaign structure, bidding strategy fit to conversion volume, conversion tracking quality, keyword and match-type discipline), fix what is broken, prove unit economics for 60 to 90 days, then layer Meta on top. Most underperforming Google accounts can be remediated in 4 to 8 weeks with focused work on structure and tracking.
Operators who skip that remediation and add Meta tend to end up with two underperforming channels instead of one. The “add another channel to fix the broken one” pattern is one of the most common agency-driven mistakes in this category. If the Google account is genuinely well-run and still underperforming, the issue is usually further upstream (service page conversion, geographic targeting, or compliance posture). Fix the upstream issue, not the channel mix.
What is the minimum monthly budget to run both channels effectively?
Roughly $20,000 a month combined is the threshold where both channels can carry meaningful weight. Below $20,000, the budget is usually better concentrated on one channel (Google for most operators) because spreading it thin starves both of the signal volume they need.
The split at $20,000 typically lands around $14,000 to $16,000 on Google and $4,000 to $6,000 on Meta in early dual-channel maturity. As budget scales above $30,000, the Meta share grows toward 30 to 40 percent of total.
Below $15,000 a month, single-channel concentration on Google is almost always the right call for the first 6 to 12 months. The framework operators should use is to start with the channel that captures the highest-intent demand first, prove it works, then add channels as the budget allows incremental investment without starving the first channel.
How does the answer change for outpatient programs?
Outpatient (IOP, PHP, MAT) shifts the calculus somewhat but does not change the order. The patient is more often the direct decision-maker for outpatient than for residential, which means patient-first targeting carries more weight than family-first. Google captures the patient’s own commercial search queries efficiently, which keeps Google as the first channel.
Meta’s role for outpatient is different (reaching the patient directly through interest and life-event signals rather than reaching the family member) but the sequencing logic is the same: Google first, Meta after 3 to 6 months.
The exception is short-duration low-acuity outpatient (single counseling sessions, brief MAT consultations) where the conversion economics differ enough that the comparison framework above does not transfer directly. Those operators usually run a fundamentally different channel mix that includes more local SEO and less paid media at all.
Is the answer different for a brand-new facility with no track record?
The recommendation is the same but the execution is slower. A facility with no existing brand, no completed website, and no service pages is not ready to run either channel productively. Most facilities in this position need 60 to 90 days of foundational work (service pages, LegitScript application, conversion tracking, compliance posture audit) before paid media of any kind makes sense.
After that foundation is in place, the Google-first sequence applies the same way. The premature-launch failure mode is common: operators who launch Google Ads on a site with thin service pages produce traffic that does not convert, conclude the channel does not work, and try Meta as a “different approach” without fixing the underlying problem.
The fix is to slow down the launch by a quarter, fix the foundation, then launch correctly.
When should we start hiring or replacing the paid media agency?
If your current agency is recommending a 50-50 day-one split across Google and Meta for a small treatment center, the framework they are using is wrong for this category. That alone is grounds to evaluate alternatives.
Other warning signs: the agency cannot describe your LegitScript status, the agency has not deployed CAPI infrastructure on the Meta side, the agency is recommending Smart Bidding on Google campaigns with under 30 conversions a month, or the agency is targeting narrow zip lists instead of broader geography with smart exclusions.
The good news is that the BH paid media agency space is smaller than the general agency space, and the operators who work specifically in this category are easier to identify than the generalists. Look for agencies with documented LegitScript onboarding experience, a CAPI implementation on a current client they can walk you through, and a clear position on Google-first sequencing. Those three filters narrow the field fast.
The perspective in this article comes from 9 years working exclusively inside behavioral health.
We are a team built by people in recovery who understand that behind every admission is someone asking for help. If that resonates, get to know us.
Mitch Marowitz is Director of Paid Media at Webserv, where he leads Google Ads, Meta, and emerging paid channel strategy for behavioral health treatment centers. He has overseen more than $45M in managed media spend across the addiction treatment category and writes about paid acquisition for treatment operators.