Behavioral health SEO is the most constrained version of SEO in any consumer-facing category. A treatment center sits at the intersection of YMYL ranking standards, HIPAA-restricted tracking, LegitScript certification gates, FTC enforcement on outcome claims, and Google’s Healthcare and Medicines policy.
Operators who apply general SEO playbooks built for ecommerce or local services lose ranking position, waste content budget, and sometimes get manual actions for E-E-A-T failures that would never trigger in another vertical.
A working SEO program for a treatment center is built around the constraints, not despite them. The seven operational layers below describe what a 2026 program actually looks like inside, and how the layers compound on each other to produce admit volume that paid-only competitors cannot match.
Here is what changed, what to build, and what to ask any agency selling SEO services in this category.
Key Takeaways
- Drug rehab SEO is structurally different from general SEO. The category sits at the YMYL, HIPAA, LegitScript, and FTC enforcement intersection. General SEO playbooks miss most of what matters in this vertical and waste budget on tactics that produce ranking without admissions.
- Seven operational layers compound on each other. Technical foundation, keyword strategy, local SEO, content with E-E-A-T, authority and earned media, AI search optimization, and admit-tied measurement. Skip a layer and the layers above it underperform.
- AI search has moved the front page. ChatGPT, Perplexity, Claude, and Google AI Overviews are now primary discovery surfaces for treatment center queries. Operators not investing in AEO are losing share on a metric most marketing teams are not measuring.
- The timeline is 12 to 18 months for compounding. First measurable lift typically lands at month 3. Compounding admit volume starts month 9 to 12. Operators expecting paid-media-speed results from organic will quit too early and lose the position they paid to build.
- Cost ranges by tier. Tier 1 ($3K to $5K monthly) is foundational maintenance. Tier 2 ($7K to $12K monthly) is the floor for compounding programs. Tier 3 ($15K to $25K monthly) is multi-state or multi-facility operator territory. Tier 4 ($30K+ monthly) is national operators with multi-location footprints.
- The agency selection decision is upstream of everything. Operators who pick the wrong SEO agency lose 6 to 12 months before they realize the program is not compounding. The diligence framework matters more than the agency’s portfolio.
- Measurement has to tie to admits, not rankings. Programs that report on rankings and traffic without admit attribution cannot defend their budget. The right measurement layer connects GA4 to the CRM and reports cost per admit by content cluster.
Why drug rehab SEO is structurally different from general SEO
The conventional SEO playbook was built for ecommerce, local services, and B2B SaaS. Each of those categories has its own constraints, but none of them face the constraint stack that addiction treatment does. Five specific constraints define the behavioral health SEO operating environment.
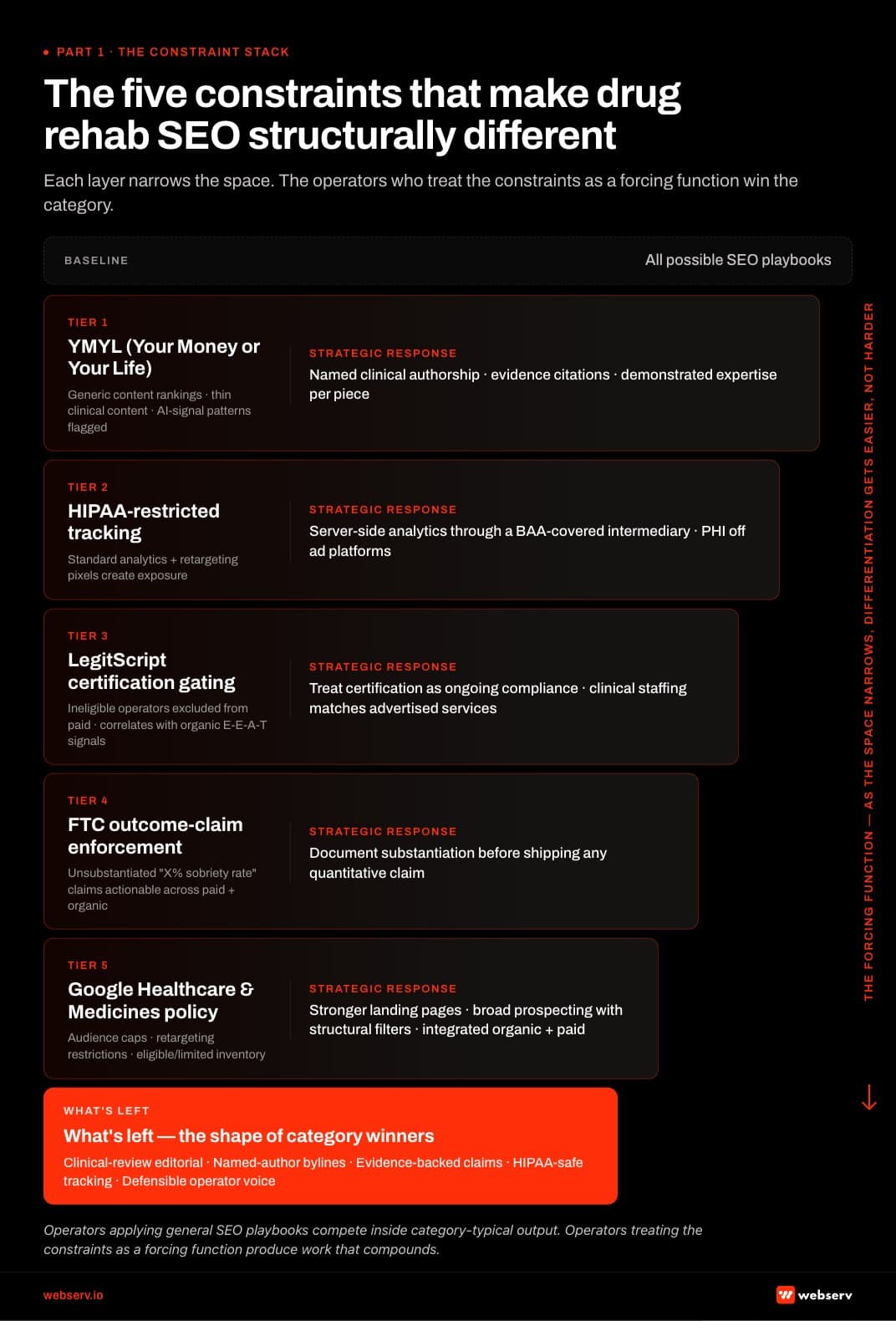 Infographic titled ‘The five constraints that make drug rehab SEO structurally different.’ Vertical five-tier stack showing each compliance constraint narrowing the SEO space available to addiction treatment marketers. Tier 1 (widest) represents all possible SEO playbooks. Tier 2 YMYL (Your Money or Your Life) restricts generic content rankings, thin clinical content gets buried, AI-signal patterns are flagged; strategic response is named clinical authorship, evidence citations, and demonstrated expertise on every piece. Tier 3 HIPAA-restricted tracking restricts standard analytics and retargeting pixels that create exposure; strategic response is server-side analytics through BAA-covered intermediaries with PHI kept off ad platforms. Tier 4 LegitScript certification gating excludes ineligible operators from paid and correlates with organic E-E-A-T signals; strategic response is treating LegitScript as ongoing compliance, not one-time setup. Tier 5 FTC enforcement on outcome claims restricts unsubstantiated ‘X% sobriety rate’ claims as actionable across paid and organic; strategic response is documenting substantiation before shipping any quantitative claim. Tier 6 Google Healthcare and Medicines policy applies audience caps, retargeting restrictions, and eligible/limited inventory; strategic response is stronger landing pages, broader prospecting with structural filters, and integrated organic plus paid program. Survivor band at the bottom: clinical-review editorial discipline, named-author bylines, evidence-backed claims, HIPAA-safe tracking, defensible operator voice.
Infographic titled ‘The five constraints that make drug rehab SEO structurally different.’ Vertical five-tier stack showing each compliance constraint narrowing the SEO space available to addiction treatment marketers. Tier 1 (widest) represents all possible SEO playbooks. Tier 2 YMYL (Your Money or Your Life) restricts generic content rankings, thin clinical content gets buried, AI-signal patterns are flagged; strategic response is named clinical authorship, evidence citations, and demonstrated expertise on every piece. Tier 3 HIPAA-restricted tracking restricts standard analytics and retargeting pixels that create exposure; strategic response is server-side analytics through BAA-covered intermediaries with PHI kept off ad platforms. Tier 4 LegitScript certification gating excludes ineligible operators from paid and correlates with organic E-E-A-T signals; strategic response is treating LegitScript as ongoing compliance, not one-time setup. Tier 5 FTC enforcement on outcome claims restricts unsubstantiated ‘X% sobriety rate’ claims as actionable across paid and organic; strategic response is documenting substantiation before shipping any quantitative claim. Tier 6 Google Healthcare and Medicines policy applies audience caps, retargeting restrictions, and eligible/limited inventory; strategic response is stronger landing pages, broader prospecting with structural filters, and integrated organic plus paid program. Survivor band at the bottom: clinical-review editorial discipline, named-author bylines, evidence-backed claims, HIPAA-safe tracking, defensible operator voice.The YMYL classification. Google explicitly designates “Your Money or Your Life” content as the highest-stakes category for ranking evaluation. YMYL content covers medical, financial, legal, and safety topics where bad information can cause real-world harm.
Addiction treatment sits squarely inside the most scrutinized version of YMYL because the content is medical, financial (treatment is expensive), and life-safety (the wrong choice can lead to death).
Google’s quality raters evaluate YMYL pages against a different bar than non-YMYL pages, with credential signals, citation depth, and reviewer authority weighted heavily.
HIPAA-restricted tracking. Treatment center websites cannot deploy standard analytics and ad tracking the same way ecommerce sites can. The HHS-OCR guidance on online tracking technologies treats pixel data from health-related pages as protected health information when combined with identifying signals.
The implication for SEO is that the standard GA4 setup most agencies deploy is not compliant on a BH site without server-side tracking, BAA-covered intermediaries, and PII-scrubbing layers in place.
LegitScript certification. LegitScript is the paid certification that gates Google Ads and Meta ads for addiction treatment. The certification is widely understood as a paid-search compliance gate, but its less-discussed effect is that it also functions as an organic E-E-A-T signal.
Sites that hold valid LegitScript certification accumulate trust signals that Google’s quality raters and AI engines treat as a verifiable third-party endorsement. The LegitScript certification process is now part of the organic playbook, not just the paid one.
FTC enforcement on outcome claims. The Federal Trade Commission’s Health Products Compliance Guidance and the March 2026 enforcement letters on substance use disorder advertising raised the bar on outcome claims in treatment center content.
Claims about success rates, completion rates, or treatment efficacy now require substantiation that meets FTC’s competent and reliable scientific evidence standard. Generic claims like “evidence-based treatment” or “industry-leading recovery rates” are now active liability exposure when published without specific citation backup.
Google’s Healthcare and Medicines policy. Google’s healthcare advertising policies extend into organic content scoring through E-E-A-T signals. The same restrictions that govern paid search ads (no testimonials without consent, no before-and-after imagery, no unsubstantiated outcome claims) flow into organic ranking criteria for treatment center content.
Operators who treat the paid and organic constraints as separate concerns produce content that hits one constraint and trips the other.
The compound effect of these five constraints is what makes the category different. Each constraint narrows the creative and operational space; the operators who treat the constraints as a forcing function (rather than as obstacles to work around) win the category.
The right framing is not “general SEO with healthcare modifications.” It is “a different game with different rules where the operators who write the new playbook lap the operators trying to retrofit the old one.”
Trevor Gage, Director of Earned & Owned Media, Webserv
The broader healthcare advertising compliance and compliance mistakes frameworks govern how these constraints play out across paid and organic.
 Infographic titled ‘The 7 layers of behavioral health SEO’ showing the operational stack that produces compounding inbound admissions for treatment centers. Layer 1 Technical foundation includes mobile-first indexing, schema markup, Core Web Vitals, site architecture, and HIPAA-compliant analytics; failure mode is pages not getting crawled or indexed. Layer 2 Keyword strategy by intent tier covers high-intent commercial, mid-funnel informational, and brand defense queries segmented by level of care, insurance, and population; failure mode is bidding against irrelevant traffic. Layer 3 Local SEO and Google Business Profile includes map pack ranking factors, location pages, review acquisition, and NAP consistency; failure mode is being invisible on ‘near me’ queries. Layer 4 Content and E-E-A-T requires clinical-review editorial workflow, named author plus medical reviewer, citation cadence, and topic cluster architecture; failure mode is generic content that decays. Layer 5 Authority and earned media includes digital PR, healthcare journalism pitching, SAMHSA and Psychology Today directory listings, and brand mentions; failure mode is thin backlink profile. Layer 6 AI search optimization (AEO) requires the 7-layer AEO playbook including Reddit and community presence, structured citations, and named clinical authorship; failure mode is being cited by zero AI engines. Layer 7 Measurement tied to admit attribution requires GA4 plus CRM plus call tracking integrated stack reporting cost per admit by content cluster and AI citation share; failure mode is reports that cannot defend the budget. Bottom band: operators running all 7 layers produce 2-4x admit volume versus operators running layers 1-3 only.
Infographic titled ‘The 7 layers of behavioral health SEO’ showing the operational stack that produces compounding inbound admissions for treatment centers. Layer 1 Technical foundation includes mobile-first indexing, schema markup, Core Web Vitals, site architecture, and HIPAA-compliant analytics; failure mode is pages not getting crawled or indexed. Layer 2 Keyword strategy by intent tier covers high-intent commercial, mid-funnel informational, and brand defense queries segmented by level of care, insurance, and population; failure mode is bidding against irrelevant traffic. Layer 3 Local SEO and Google Business Profile includes map pack ranking factors, location pages, review acquisition, and NAP consistency; failure mode is being invisible on ‘near me’ queries. Layer 4 Content and E-E-A-T requires clinical-review editorial workflow, named author plus medical reviewer, citation cadence, and topic cluster architecture; failure mode is generic content that decays. Layer 5 Authority and earned media includes digital PR, healthcare journalism pitching, SAMHSA and Psychology Today directory listings, and brand mentions; failure mode is thin backlink profile. Layer 6 AI search optimization (AEO) requires the 7-layer AEO playbook including Reddit and community presence, structured citations, and named clinical authorship; failure mode is being cited by zero AI engines. Layer 7 Measurement tied to admit attribution requires GA4 plus CRM plus call tracking integrated stack reporting cost per admit by content cluster and AI citation share; failure mode is reports that cannot defend the budget. Bottom band: operators running all 7 layers produce 2-4x admit volume versus operators running layers 1-3 only.LAYER 1 · TECHNICAL FOUNDATION
Layer 1: The technical foundation
The technical foundation is the substrate underneath every other SEO layer. A site with broken technical SEO produces poor results regardless of how strong the content, authority, or AI optimization layers are. For treatment center sites in 2026, five technical priorities matter most.
Mobile-first indexing. Google has crawled from a mobile-first index since 2019, and in 2026 roughly 92% of treatment-seeking research traffic originates on mobile devices. Sites that render poorly on mobile lose ranking position even when desktop performance is strong.
The mobile-first indexing reality for rehab websites shapes every other technical decision: site architecture, page speed thresholds, image optimization, schema deployment. Operators with desktop-prioritized sites built in 2018 to 2020 need a mobile audit before any other technical work.
Schema markup deployment. Three schema types form the foundation for treatment center sites: MedicalBusiness (or LocalBusiness, depending on facility type), FAQPage (for the Rank Math FAQ blocks that surface in AI Overviews), and Article (for blog content).
The schema deployment needs to validate without warnings, render consistently across page templates, and include the credentialed author signal through Person schema with knowsAbout, jobTitle, and sameAs properties. Schema deployment is one of the highest-ROI technical investments because it shapes both organic ranking eligibility and AI engine citation eligibility.
Core Web Vitals. Google’s Core Web Vitals (Largest Contentful Paint, Interaction to Next Paint, Cumulative Layout Shift) are direct ranking signals. The 2024 INP replacement of FID raised the bar for interactive responsiveness. Treatment center sites typically fail on LCP because of large hero images and unoptimized clinical photos.
They fail on INP because of script-heavy chat widgets, retargeting pixels, and contact form widgets. The audit identifies the failure modes and the technical team prioritizes fixes by ranking impact, not by engineering simplicity.
Site architecture for hub-and-spoke clusters. The 2026 ranking environment rewards topical depth more than topical breadth. Sites that organize content into hub-and-spoke clusters (a pillar piece linking to deep cluster Micros, with clean internal linking between Micros) rank better on cluster topics than sites that publish 200 disconnected blog posts.
The architecture decision is upstream of content production: pillars first, cluster Micros after, with the URL structure reflecting the cluster hierarchy.
HIPAA-compliant analytics. Standard GA4 deployment on treatment center sites is a HIPAA exposure when combined with identifiable user signals on health-related pages.
The compliant alternative is server-side tracking through a BAA-covered intermediary (Segment with BAA, Freshpaint, RudderStack with the appropriate configuration), with PII scrubbing applied before data hits the analytics layer. Operators running standard pixel-only setups are creating compliance risk that compounds quietly until an OCR audit forces remediation.
The deeper coverage on the technical foundation lives in our technical SEO playbook, and the technical fixes most sites need covers the audit pattern that surfaces the high-priority gaps.
Operators starting from scratch should expect 4 to 8 weeks of technical foundation work before the content and authority layers can compound on top.
LAYER 2 · KEYWORD STRATEGY
Layer 2: Keyword strategy by intent tier
Keyword strategy in BH is not a list of high-volume queries to rank for. It is a segmentation of the addressable query space by buyer intent, level of care, payer, and population, with explicit prioritization of the queries that produce admissions over the queries that produce traffic.
Intent tiers. Three intent tiers structure the strategy. High-intent commercial queries with direct admission-purchase intent (“[City] residential rehab,” “[insurance] PHP near me,” “alcohol detox accepting Aetna”) have the highest economics because the buyer is already in the funnel.
The right pages targeting these queries are service pages and location pages, not blog posts. Mid-funnel informational queries (“Difference between PHP and IOP,” “what to expect in residential treatment,” “how to support a family member in recovery”) feed the commercial layer through internal linking and brand authority development.
Brand defense queries containing the facility name or its competitors are usually low-volume but high-intent and need to be defended against competitor poaching.
Level-of-care segmentation. Residential, PHP, IOP, detox, MAT, outpatient, and any specialty programs the facility offers each warrant dedicated keyword targeting. The buyer searching “detox near me” is a different buyer from the buyer searching “outpatient drug treatment with telehealth,” and the content that serves each should be different.
Insurance-specific keywords. Payer queries (“Anthem residential treatment,” “Aetna BHC coverage rehab,” “Tricare drug rehab”) are high-intent commercial queries that most BH operators underweight.
The insurance verification call is often the first real conversion event in the funnel, and the keyword strategy should map these queries to dedicated insurance-page content that surfaces verification CTAs.
Population-specific keywords. Veteran-specific, adolescent-specific, LGBTQ+-specific, dual-diagnosis-specific, women-only, men-only, and professional-population programs each have distinct query patterns. Operators serving these populations should treat the population-specific content as its own cluster, not as a footnote inside the general residential cluster.
Geographic modifiers. “Near me” queries, city-specific queries, and metro-area queries shape local SEO strategy. The keyword research should distinguish between queries that map to a local pack result (city-specific) and queries that produce a hybrid pack-plus-organic result (broader regional queries).
The keyword strategy work for providers covers the segmentation framework in operational detail.
The output of the keyword strategy phase is a tiered query map (roughly 200 to 400 prioritized queries for a mid-sized treatment center), grouped by intent tier, level of care, payer, and population, with target page assignments for each cluster.
The keyword map becomes the operating document for content planning, technical optimization, and measurement.
LAYER 3 · LOCAL SEO
Layer 3: Local SEO and Google Business Profile
For multi-location operators and any facility serving a defined regional market, local SEO is the highest-ROI layer after the technical foundation.
The local pack (the three-result map block at the top of city-specific results) drives a meaningful share of treatment-seeking discovery, and Google Business Profile optimization is the operational lever underneath local pack ranking.
Map pack ranking factors. The three primary factors are proximity (distance from the searcher), relevance (how well the GBP listing matches the query), and prominence (review volume, review quality, citation depth across third-party directories). Treatment center operators have limited control over proximity but meaningful control over relevance and prominence.
Location pages. A treatment center serving multiple markets needs dedicated location pages for each market.
The location pages must carry distinct, market-specific content (not templated content with the city name swapped), reference the specific clinical offerings available at that location, include map embeds and verifiable NAP (Name, Address, Phone) data, and link back to the relevant service pages.
Generic location pages that swap a city name into a template produce no ranking lift and may trip duplicate content flags.
NAP consistency. Name, address, and phone number must match exactly across the facility website, Google Business Profile, third-party directories (Yelp, Healthgrades, Psychology Today, Yellow Pages), and any aggregator data feeds. Inconsistencies degrade local ranking through trust signal dilution.
Review acquisition workflows. Google reviews, Yelp reviews, and Healthgrades reviews carry differential weight in the local pack ranking algorithm.
Treatment centers face a unique constraint: HIPAA prevents the facility from directly soliciting reviews from former patients without explicit consent, and even with consent the review content cannot reference specific clinical conditions or treatments without further consent.
The workflow that works is a consent-first review request integrated into the discharge planning process.
Google Business Profile optimization. Services, attributes, photos, posts, Q&A, and Justifications all factor into GBP ranking. The optimization is operational rather than strategic: identify the GBP fields that are blank or weak, fill them with accurate facility-specific content, and maintain the content with regular updates.
Posts (the GBP equivalent of a brand timeline) should be updated weekly with operational content that reflects active facility programming.
Our local SEO playbook for rehab centers covers the structural decisions, and local SEO tactics that fill beds covers the operational rhythms that produce admit lift.
LAYER 4 · CONTENT + E-E-A-T
Layer 4: Content strategy and E-E-A-T
DEFINITION
Your Money or Your Life (YMYL)
Google’s classification for content that can materially affect a reader’s health, finances, or safety. Addiction treatment sits inside the most scrutinized version of YMYL because the content is medical, financial, and life-safety. YMYL pages face the strictest E-E-A-T threshold of any vertical Google evaluates.
Content is where most treatment center SEO programs underperform. The constraint stack from Layer 1 limits what content can be published without triggering compliance or E-E-A-T issues, which means generic content production approaches do not work in this category.
The content strategy has to be built around credentialed clinical authorship, topic cluster architecture, and the helpful content guidance Google publishes for YMYL content.
The clinical-review editorial workflow. Every published piece in 2026 should carry a named author and a named clinical reviewer when the author is not themselves clinically credentialed. The author byline is the E-E-A-T signal Google’s quality raters and AI engines look for first.
The clinical reviewer adds the medical authority that YMYL content requires. The workflow operationalizes both: the writer drafts based on clinician interviews and source material, the clinical reviewer signs off on accuracy, the published piece carries both names with verified credentials linked through Person schema.
Topic cluster architecture. Content is organized into clusters, not lists. A cluster has one pillar piece (3,000 to 5,000 words covering the broad topic) and 5 to 12 supporting Micros (1,500 to 3,000 words each, drilling into specific sub-topics).
The pillar links to every Micro and every Micro links back to the pillar. The cluster carries the topical depth that AI engines reward for citation, and the internal linking structure carries the authority signal that traditional Google ranking rewards.
Content depth for YMYL queries. Thin content fails in YMYL. A 700-word piece on dual diagnosis treatment cannot compete with a 3,000-word piece written by a credentialed clinician with citation depth and operational specificity.
The depth requirement is operational: each piece needs to answer the underlying question completely, cite authoritative sources where claims are made, and demonstrate the clinical or operational expertise of the author. Operators chasing volume with shallow content produce libraries that consume budget without generating admits.
The “anonymous content fails” pattern. In 2024 and 2025, AI engines and Google’s quality systems began discounting content with anonymous bylines, generic agency attribution, or “Editorial Team” labels. The 2026 retrieval reality is that anonymous content is a discount signal regardless of the content’s underlying quality.
Content cadence and freshness. Treatment center content benefits from a publication cadence of 4 to 12 pieces per month at the cluster level, with quarterly refreshes on existing pillars and annual refreshes on supporting Micros.
Freshness signals are weighted in 2026 for YMYL content because clinical guidance, regulatory frameworks, and treatment standards change. The published date and the last-reviewed date should both appear on every piece.
The healthcare content creation framework covers the cadence model that works at the treatment center operator scale, and our healthcare blog and article writing primer covers the editorial standards underneath each piece.
The Client Brain framework. Most agencies producing BH SEO content do not actually know the client they are writing for.
The Client Brain is the operating layer underneath effective agency content production: a structured representation of the facility’s clinical voice, operational reality, payer mix, population focus, and admission workflow that the agency uses to produce content that sounds like the operator rather than like the agency.
The Client Brain operating system is the diligence framework that separates agencies producing compounding work from agencies producing category-typical filler.
The content layer also pulls our authority content capability into operating relevance: the editorial standards, credentialed author infrastructure, and topic cluster discipline are what turn the SEO program from a content marketing line item into an admit-producing engine.
LAYER 5 · AUTHORITY
Layer 5: Authority and earned media
The authority layer is where most BH SEO programs go wrong. Traditional link building strategies that work in ecommerce and B2B SaaS (guest posting, link exchanges, content marketing for backlinks) either fail or actively damage rankings in behavioral health. The right alternative is digital PR with verticalized targeting.
Why traditional link building fails. Three failure modes recur in BH. First, guest posts on low-authority sites flag the E-E-A-T evaluation negatively because the site association reduces perceived credibility rather than enhancing it.
Second, reciprocal link schemes trigger Google’s link spam detection, which is more aggressive in YMYL than in other categories. Third, broad outreach to non-healthcare sites produces low-quality links that are increasingly treated as ranking-neutral or ranking-negative under the 2024 and 2025 spam updates.
Digital PR as the right answer. The earned media strategy that works in BH targets verticalized healthcare publications, treatment industry directories, and authoritative community resources.
SAMHSA’s treatment locator and Single State Agency listings, Psychology Today provider listings, ASAM and JCAHO directory placements, state and local recovery community resource lists, and healthcare journalism placements in publications like STAT, Behavioral Health Business, and Addiction Professional.
Each placement is a trust signal that the AI engines and Google’s quality raters can verify, and the cumulative authority compounds across the cluster.
Healthcare journalism pitching. Treatment centers with named clinical leaders, published research, or distinctive operational approaches can earn media coverage that produces backlinks alongside brand exposure.
The pitch is not “promote our facility” but “here is a credentialed clinician who can speak to a current trend or development.” The pitching cadence is 4 to 8 well-targeted pitches per month, with hit rates of 15 to 30% producing real coverage.
Brand mention monitoring. Mentions of the facility name across the web carry brand authority value even when they do not include backlinks. Monitoring tools surface mentions across publications, podcasts, social platforms, and review sites. The mentions feed the brand-defense keyword strategy and identify reputation issues before they compound.
What to avoid. Paid links are an E-E-A-T flag and a Google penalty risk. Reciprocal exchanges are flagged. Irrelevant guest posts (on sites unrelated to behavioral health or healthcare) produce no authority signal and waste production budget. Private blog networks (PBNs) are an active manual action risk.
The authority strategy works by addition (new high-quality placements) not by subtraction (cleaning up bad links from prior agencies), though sometimes both run in parallel. The authority layer connects to the broader digital PR capability and pulls the credentialed author signal from Layer 4 into wider distribution.
How SoCal Sunrise generated 85 admissions and 2,297% ROI from SEO in 6 months
A ground-up SEO rebuild using the Pathfinder Parents Methodology turned an invisible online presence into a top-ranking admissions engine.
Read the case study →85 admits and 3,152 leads attributed to organic
LAYER 6 · AI SEARCH
Layer 6: AI search optimization (AEO)
The 2026 reality is that AI search engines (Google AI Overviews, ChatGPT, Perplexity, Claude, Gemini) are now primary discovery surfaces for treatment center queries. Treatment-seeking research that previously routed through traditional Google search now increasingly routes through AI engines that synthesize answers from cited sources.
The implication is that organic ranking is no longer the only goal; citation share inside AI engine responses is now an equally important metric.
The seven-layer AEO playbook. Our AI Overviews and ChatGPT guide covers the operational details. The short version is that AEO is built on seven layers. First: entity SEO so the engines can identify and verify the facility. Second: passage-level optimization so the engines can extract citable passages from longer content.
Third: named clinical authorship so the credential signal is legible to the engines. Fourth: Reddit and community citation building because Reddit is now Google’s largest external citation source. Fifth: FAQ structuring so the engines can extract Q-A pairs cleanly. Sixth: source diversification across the citation graph.
Seventh: measurement of citation share through specialized tooling.
Reddit citations as the largest AI citation source. Google’s 2024 Reddit partnership and the AI engines’ independent reliance on Reddit content have made Reddit the single largest external citation source for treatment center queries in 2026.
Treatment centers that develop a discipline around Reddit presence (without violating Reddit’s anti-promotional rules) capture citation share that competitors miss. The discipline is operator-direct participation (real clinicians and operators answering questions) rather than promotional content.
Named clinical authorship. AI engines preferentially cite content with named credentialed authors. The Person schema deployment from Layer 1, the editorial workflow from Layer 4, and the authority placements from Layer 5 all feed the AI engine’s preference for credentialed sources.
Anonymous content is cited at much lower rates than credentialed content in 2026.
The 12-week measurable lift cycle. AEO investments typically produce measurable citation share lift in 12 to 16 weeks. The lift compounds as more credentialed content publishes, more entity signals strengthen, and the cluster’s overall authority compounds.
Operators expecting paid-media-speed AEO results will be disappointed; operators who run the program for 6 to 12 months will see the compounding pattern that defines the next decade of treatment center marketing.
Query fan-out architecture. Modern AI search uses query fan-out where a user’s question gets decomposed into 8 to 15 sub-queries that the engine retrieves independently before synthesis.
The fan-out query architecture shapes content structure: passages that answer specific sub-queries clearly get cited, while passages that cover the broad topic without sub-query specificity do not.
The AEO layer is the most actively evolving SEO discipline in 2026. Operators investing now are positioning for the next phase of discovery; operators waiting until the layer is fully mature will be too late to catch the early-mover citation share that compounds into category leadership.
Our AEO capability page covers the service-level operational frame.
LAYER 7 · MEASUREMENT
Layer 7: Measurement tied to admit attribution
The measurement layer is where the budget defense lives.
Programs that report on rankings and traffic without admit attribution cannot defend their cost to operator leadership; programs that connect the SEO work to actual admit volume through CRM and call tracking integration become the most defensible line items in the marketing budget.
Why rankings and traffic alone underperform as measurement. Rankings move for reasons unrelated to program performance (algorithm updates, competitor activity, seasonal volatility). Traffic correlates with rankings but does not reliably correlate with admits because not all traffic intent is commercial.
Operators reporting on rankings and traffic without admit data are reporting on intermediate metrics that may or may not connect to revenue.
The integrated measurement stack. The right measurement layer integrates GA4 (or a privacy-compliant alternative), call tracking software (CallRail or equivalent), and the facility’s CRM through a clean data pipeline.
The pipeline tracks the searcher’s first touch (which keyword, which page, which AI engine citation if applicable), the conversion event (form submission or phone call), and the eventual admit outcome (admitted, evaluated and referred, scheduled but did not show).
The connected data set lets the operator report cost per admit by content cluster, by keyword tier, by location, and by AI citation source.
Cost per admit by content cluster. The most defensible budget metric is cost per admit segmented by the content cluster that produced the lead. The residential cluster might produce admits at $400 cost per admit; the dual-diagnosis cluster at $250; the veteran-specific cluster at $180.
The segmentation lets the operator increase budget allocation to high-performing clusters and de-prioritize underperforming clusters. The granularity is impossible without the integrated measurement stack.
AI citation tracking. Specialized tools (Otterly, Profound, Surfer’s AI tracking, and a small handful of others as of 2026) track citation share inside AI engine responses for a defined keyword set.
The metric is new, the tooling is imperfect, but the directionality is reliable: programs that increase citation share over 6 to 12 months produce admit lift that lags by 2 to 4 months.
The reporting cadence that wins budget defense. Monthly reports that include traffic, rankings, citation share, conversion volume, and cost per admit by cluster. Quarterly reports that include cluster-level admit attribution, comparative benchmarking against the prior quarter, and a forecast for the next quarter.
Annual reports that include the full cost-per-admit picture, the agency’s contribution to brand value and authority, and the strategic recommendation for the following year.
The measurement layer connects upstream to the admission operations capability that runs the back-end of the funnel. Marketing and admissions teams that share the measurement framework produce more coordinated growth than teams running independent metrics.
Cost benchmarks by tier
Operators new to behavioral health SEO usually ask the budget question first. The honest answer is that BH SEO costs more than general SEO because the constraint stack from Layer 1 requires specialized expertise, credentialed clinical workflows, and a higher baseline level of compliance work.
Four tiers cover the working range for most operators.
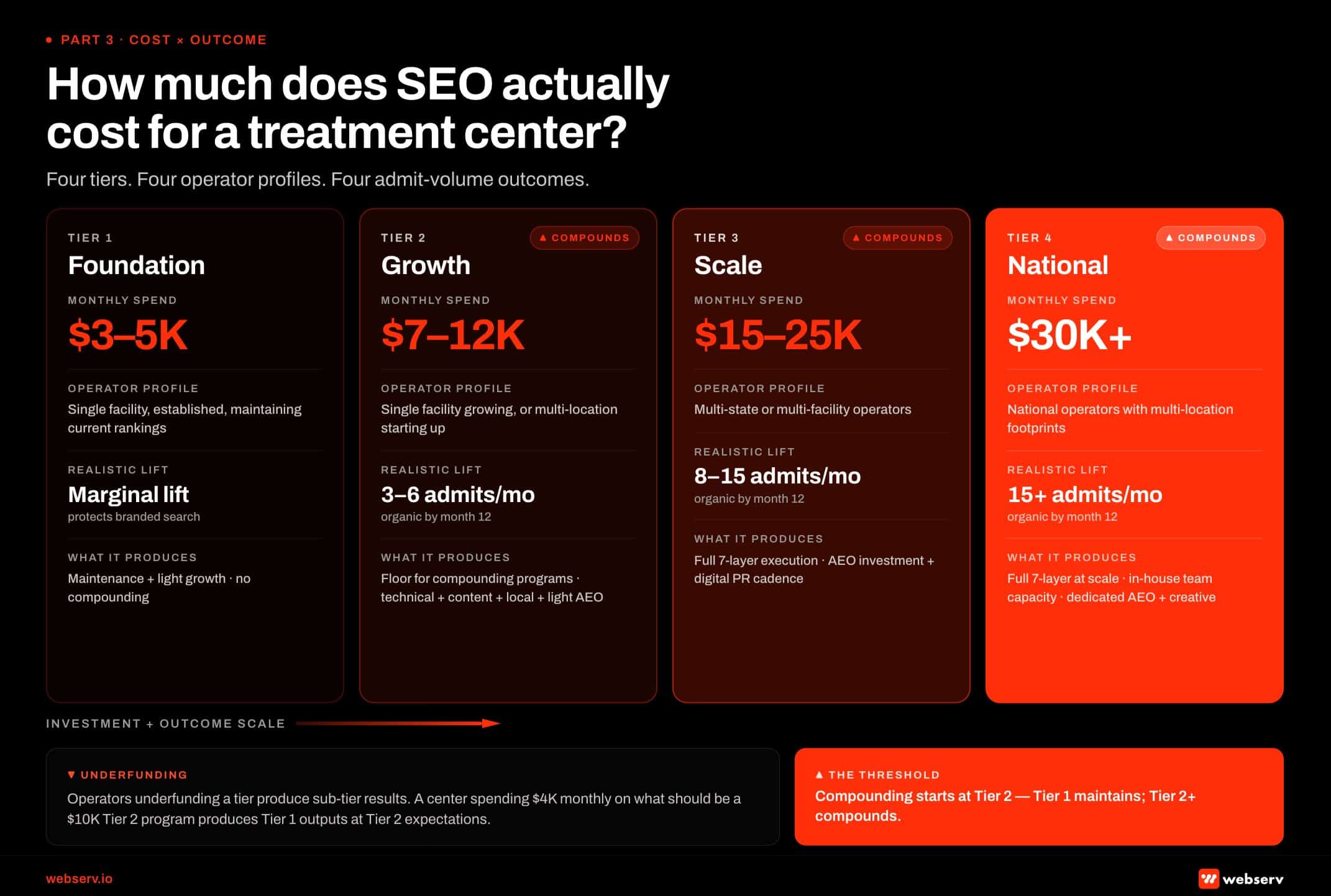 Infographic titled ‘How much does SEO actually cost for a treatment center?’ showing the four-tier SEO investment framework for behavioral health treatment centers. Tier 1 Foundation: $3,000 to $5,000 monthly spend, applies to single-facility established operators maintaining current rankings, produces marginal lift that protects branded search, runs as maintenance plus light growth without compounding. Tier 2 Growth: $7,000 to $12,000 monthly, applies to single-facility operators growing or multi-location operators starting up, produces 3-6 admits per month organic by month 12, represents the floor for compounding programs covering technical foundation, content production, local SEO, and light AEO. Tier 3 Scale: $15,000 to $25,000 monthly, applies to multi-state or multi-facility operators, produces 8-15 admits per month organic by month 12, runs full 7-layer execution including AEO investment and digital PR cadence. Tier 4 National: $30,000 plus monthly, applies to national operators with multi-location footprints, produces 15 plus admits per month organic by month 12, runs full 7-layer at scale with in-house team capacity and dedicated AEO plus creative production. Bottom callout: operators underfunding a tier produce sub-tier results, so a center spending $4K monthly on what should be a $10K Tier 2 program produces Tier 1 outputs at Tier 2 expectations.
Infographic titled ‘How much does SEO actually cost for a treatment center?’ showing the four-tier SEO investment framework for behavioral health treatment centers. Tier 1 Foundation: $3,000 to $5,000 monthly spend, applies to single-facility established operators maintaining current rankings, produces marginal lift that protects branded search, runs as maintenance plus light growth without compounding. Tier 2 Growth: $7,000 to $12,000 monthly, applies to single-facility operators growing or multi-location operators starting up, produces 3-6 admits per month organic by month 12, represents the floor for compounding programs covering technical foundation, content production, local SEO, and light AEO. Tier 3 Scale: $15,000 to $25,000 monthly, applies to multi-state or multi-facility operators, produces 8-15 admits per month organic by month 12, runs full 7-layer execution including AEO investment and digital PR cadence. Tier 4 National: $30,000 plus monthly, applies to national operators with multi-location footprints, produces 15 plus admits per month organic by month 12, runs full 7-layer at scale with in-house team capacity and dedicated AEO plus creative production. Bottom callout: operators underfunding a tier produce sub-tier results, so a center spending $4K monthly on what should be a $10K Tier 2 program produces Tier 1 outputs at Tier 2 expectations.Tier 1 ($3,000 to $5,000 monthly). Foundational maintenance for single-location operators with existing baseline rankings. This tier covers technical SEO maintenance, monthly content production at 2 to 4 pieces (with credentialed authorship), GBP optimization, and basic monthly reporting.
Tier 1 maintains the ranking position the operator already has but does not produce the compounding lift that defines a working SEO program.
Tier 2 ($7,000 to $12,000 monthly). The floor for compounding programs.
This tier covers technical work including ongoing audits, 4 to 6 pieces of content per month, local SEO with active review acquisition, digital PR at 2 to 4 placements per month, light AEO investment, and reporting that connects rankings to leads.
Tier 2 produces measurable admit lift starting at month 6 to 9 and compounding through month 18 to 24.
Tier 3 ($15,000 to $25,000 monthly). Multi-state or multi-facility operators running the full seven-layer execution.
This tier covers everything in Tier 2 plus location-page production at scale, expanded content production (8 to 12 pieces monthly), full AEO investment including Reddit and community citation strategies, advanced measurement infrastructure including AI citation tracking, and quarterly strategic planning aligned with the operator’s expansion plans.
Tier 4 ($30,000+ monthly). National operators with multi-location footprints, expanded creative production capacity, and full AEO investment.
This tier covers everything in Tier 3 plus dedicated brand and authority investment, expanded location coverage, advanced clinical content production (including video, podcasts, and original research where applicable), and strategic planning at the corporate level.
What each tier produces in admit terms. Tier 1 maintains the current admit baseline. Tier 2 produces 15 to 30% admit growth from organic at month 18 versus the baseline. Tier 3 produces 40 to 80% admit growth at month 24.
Tier 4 produces the category-leading positions that depend more on duration than dollar amount.
Why operators who underfund Tier 2 produce Tier 1 results. The most common budget mistake is committing to a Tier 2 budget but cutting it during the first 6 months when the compounding has not yet appeared.
Programs cut at month 4 to 6 produce Tier 1 outcomes because the compounding layers require runway to produce results. Operators who commit to 18 months at the Tier 2 budget level reliably outperform operators who run the same budget for 6 months before cutting back.
Timeline: what to expect at 3, 6, 9, 12 months
The most common reason BH SEO programs fail is impatience. Operators expecting paid-media-speed results from organic quit at month 4 to 6, before the compounding has appeared. The realistic timeline for a Tier 2 or Tier 3 program runs across 18 months with distinct phases.
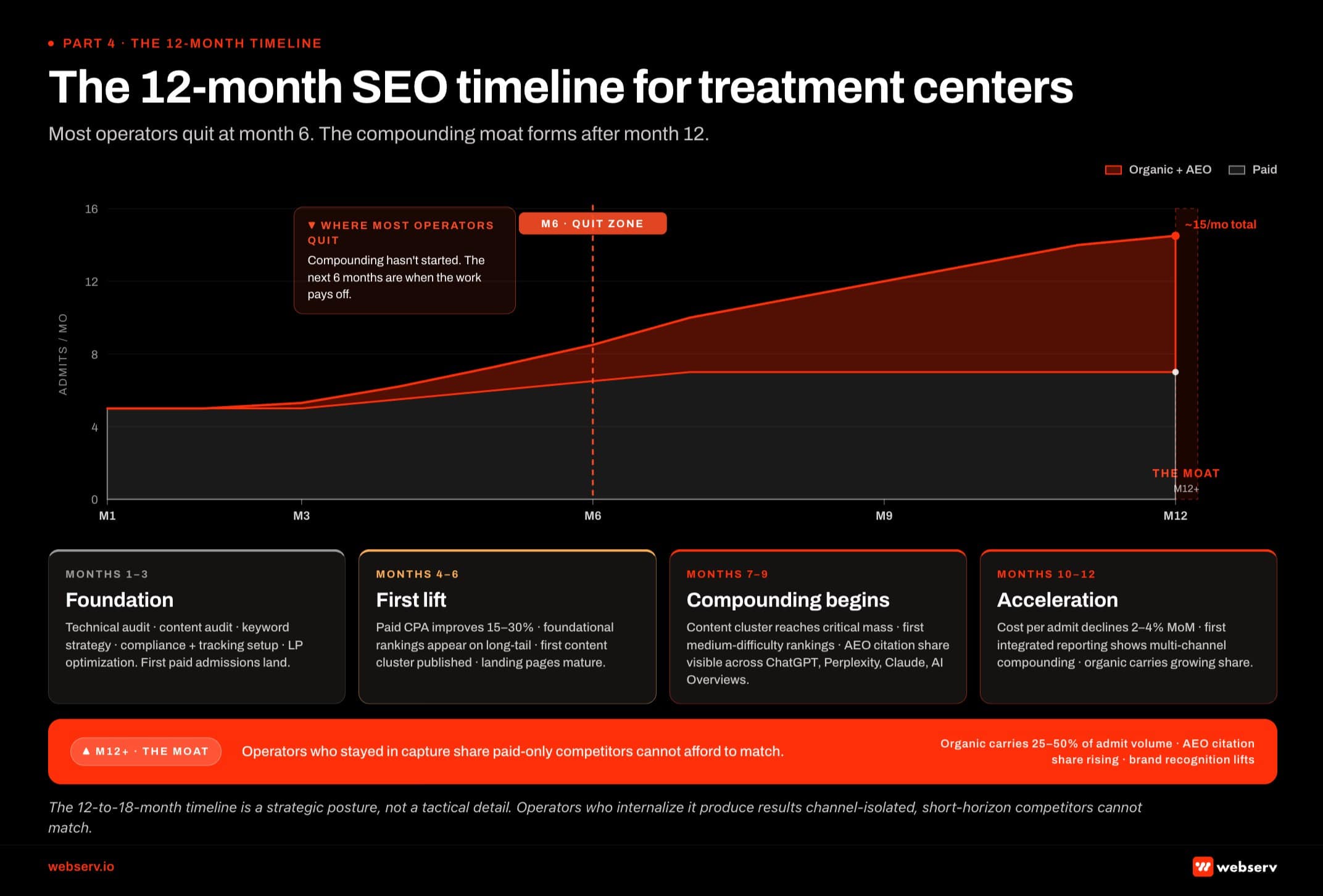 Infographic titled ‘The 12-month SEO timeline for treatment centers’ showing what compounds when across a year of an integrated SEO program for behavioral health treatment centers. Months 1-3 (Foundation): technical audit, content audit, keyword strategy, compliance and tracking setup, landing page optimization; first paid admissions land but organic is still building. Months 4-6 (First lift): paid CPA improves 15-30 percent, foundational rankings start appearing on long-tail queries, first content cluster published, landing pages mature; organic still pre-compounding. Red dashed warning band at Month 6: most operators who quit do so right before compounding starts. Months 7-9 (Compounding begins): organic content cluster reaches critical mass, first medium-difficulty rankings appear, AEO citation share becomes visible across ChatGPT, Perplexity, Claude, and Google AI Overviews. Months 10-12 (Acceleration): cost per admit declines 2-4 percent month over month, first integrated reporting shows multi-channel compounding, organic carries growing share of total admits. Month 12+ (The moat): organic carries 25-50 percent of admit volume, AEO citation share continues rising, brand recognition lifts in service geographies, operator now defends category position rather than building it.
Infographic titled ‘The 12-month SEO timeline for treatment centers’ showing what compounds when across a year of an integrated SEO program for behavioral health treatment centers. Months 1-3 (Foundation): technical audit, content audit, keyword strategy, compliance and tracking setup, landing page optimization; first paid admissions land but organic is still building. Months 4-6 (First lift): paid CPA improves 15-30 percent, foundational rankings start appearing on long-tail queries, first content cluster published, landing pages mature; organic still pre-compounding. Red dashed warning band at Month 6: most operators who quit do so right before compounding starts. Months 7-9 (Compounding begins): organic content cluster reaches critical mass, first medium-difficulty rankings appear, AEO citation share becomes visible across ChatGPT, Perplexity, Claude, and Google AI Overviews. Months 10-12 (Acceleration): cost per admit declines 2-4 percent month over month, first integrated reporting shows multi-channel compounding, organic carries growing share of total admits. Month 12+ (The moat): organic carries 25-50 percent of admit volume, AEO citation share continues rising, brand recognition lifts in service geographies, operator now defends category position rather than building it.Month 1 to 3: Foundation work. Technical audit and remediation, schema deployment, content audit identifying gaps and underperforming pieces, keyword strategy development, baseline measurement setup, credentialed author onboarding, GBP audit and optimization. No measurable ranking lift yet; the program is building the substrate.
Month 4 to 6: Content cluster expansion and first publishing cycle. The first 8 to 16 content pieces publish, local SEO work produces initial review velocity, digital PR launches with 4 to 8 placements landing, first technical optimizations show measurable Core Web Vitals improvement.
Early ranking movement appears on long-tail and lower-competition queries by month 6.
Month 7 to 9: Citation building, AEO development, first measurable lift.
The content cluster has 20 to 30 pieces published with strong internal linking, citation share in AI engines shows initial lift, authority signals strengthen through accumulated PR placements, organic traffic shows measurable month-over-month growth, first commercial-intent queries start ranking on page one.
The compounding effect is now visible but admit attribution lags 60 to 90 days.
Month 10 to 12: Compounding gains, citation share rising, first admit attribution data.
The content library has 35 to 50 pieces, organic traffic is 50 to 100% above the baseline, citation share in AI engines is producing measurable referral traffic, commercial-intent queries are stable in the top three results for the most-targeted keywords, and the integrated measurement layer is producing reliable cost-per-admit data.
Month 13 to 18: Discipline becomes the moat. The compounding pattern accelerates. Content production cadence stabilizes. Citation share in AI engines reaches steady state at a category-competitive level. Authority signals plateau at a defensible level.
The operator’s organic traffic and admit volume from organic are 2 to 4 times the baseline. The competitive advantage is now structural.
Why programs that quit at month 6 produce nothing. The compounding has not appeared yet at month 6.
Operators who pull the plug at this stage do not just lose the months they invested; they leave the cluster authority half-built, which means restarting later costs more than continuing the original program would have.
The math of quitting at month 6 is the worst version of the SEO investment decision.
Building SEO in-house versus hiring an agency
The build-versus-buy decision depends on the operator’s annual marketing budget, content production capacity, and strategic priorities. Three configurations work for different operator profiles.
When in-house works. Operators with $1 million-plus annual marketing budgets, dedicated content production capacity, and strong internal clinical leadership can build an in-house SEO team that outperforms most agencies.
The internal team includes an SEO director (with BH-specific experience), 2 to 3 content writers, a clinical content reviewer, a technical SEO specialist, and a measurement analyst. The all-in cost for this team runs $400,000 to $800,000 annually.
When an agency works. Most Tier 1 and Tier 2 operators (and many Tier 3 operators) benefit from agency engagement.
The agency model concentrates BH-specific expertise that operators cannot recruit individually, provides the technical depth and content production capacity at a lower cost than building it in-house, and operationalizes the seven-layer playbook through established workflows.
The hybrid model. Some operators run a hybrid model where the agency handles paid-adjacent technical work and content production, and the operator owns brand voice and clinical leadership.
This model works well for Tier 3 operators with strong internal teams who want to scale beyond what the internal team can produce alone.
Our list of top SEO agencies for behavioral health covers the operators who work specifically in this category and the diligence framework for evaluating them, and the broader best marketing agencies for rehabs lens covers integrated agency relationships beyond SEO alone.
How to evaluate an SEO agency for behavioral health
Operators picking an SEO agency without a diligence framework usually pick the wrong one. For an operator-side ranking of behavioral health SEO agencies, see our scored shortlist.
The wrong agency costs 6 to 12 months before the operator realizes the program is not compounding, and the recovery from a failed agency engagement costs more than picking the right one initially. Six diligence questions separate the agencies producing compounding work from the agencies producing category-typical filler.
Question 1: What is your clinical review workflow? The right answer describes named clinical reviewers, documented review cadence, citation depth requirements, and how the agency handles the credentialed author signal. The wrong answer is “we have clinical reviewers on staff” without specifics.
Question 2: How do you handle LegitScript compliance and HIPAA-restricted tracking? The right answer covers both: LegitScript as an organic E-E-A-T signal in addition to a paid gate, HIPAA-compliant analytics through server-side tracking and BAA-covered intermediaries, PII scrubbing in the measurement layer.
The wrong answer treats both as paid-search concerns rather than organic concerns.
Question 3: Can you walk me through your AEO playbook? The right answer covers the seven-layer AEO framework, entity SEO infrastructure, Reddit citation strategy, AI citation tracking tooling, and the measurable 12-week lift cycle.
The wrong answer is “we are watching the AI search space” or “we deploy schema for AI Overviews.”
Question 4: Show me a recent client’s measurement report. The right answer is a redacted version of a real client report that connects rankings, traffic, conversion volume, AI citation share, and cost per admit by content cluster.
The wrong answer is a generic ranking and traffic report that does not connect to admits.
Question 5: What does your content production look like operationally? The right answer covers the writer pool (credentials, experience, BH-specific knowledge), the clinical reviewer relationship, the editorial workflow including author byline assignment, the content cadence, and the citation discipline.
The wrong answer focuses on volume (“we produce 30 pieces per month”) without describing the editorial infrastructure that turns volume into quality.
Question 6: How do you onboard a new client’s voice and operational reality? The right answer describes a structured Client Brain or equivalent framework: clinical voice capture, operational interviews with admissions and clinical leadership, payer mix documentation, population focus documentation, and brand standards translation into content guidelines.
Our Client Brain operating system covers the full diligence framework that operators should run before signing any SEO agency contract.
Common SEO mistakes treatment centers make
Eight patterns recur across BH SEO programs that underperform. Each one is structurally fixable but expensive to address after the fact, which makes the diagnostic worth running before the program is well underway.
Generic content written without clinical review. The most common failure mode. Content that passes the SEO checklist (target keyword, internal links, recommended word count) but fails the clinical and editorial bar. The fix is the credentialed editorial workflow from Layer 4.
MOST COMMON FAILURE MODE
Generic content written without clinical review. Content that passes the SEO checklist (target keyword, internal links, recommended word count) but reads like every other rehab site explainer. The 184-post commodity library is what most operators inherit from their previous agency, and it is the single biggest source of E-E-A-T drag we audit.
Stock photography and stock language. “Compassionate care.” “Evidence-based treatment.” “Personalized recovery.” Stock language signals to AI engines and to skeptical readers that the content is generic, not specific to the operator. Stock photos compound the signal. The fix is operator-specific language and original photography that captures the actual facility.
Listicles without expert depth. “Top 10 signs of opioid addiction.” Listicle content can work when written with real clinical depth, but most agency-produced listicles in BH are surface-level aggregations that do not earn AI citation and do not produce admit lift.
The fix is either expert-depth listicles or different content formats entirely.
Bought links and link schemes. Paid links flag YMYL E-E-A-T issues, link schemes trigger Google’s anti-spam systems, and both produce ranking damage that takes 6 to 12 months to recover from. The fix is the digital PR strategy from Layer 5.
HIPAA-noncompliant tracking. Standard pixel-only GA4 deployment is a HIPAA exposure on treatment center sites. The fix is the server-side tracking infrastructure from Layer 1.
Population-specific content treated as interchangeable. Veteran-specific, adolescent-specific, and dual-diagnosis-specific content cannot be produced from the same template. Each population has distinct clinical considerations, search intent patterns, and editorial requirements. The fix is dedicated cluster planning for each population the operator serves.
Site rebuilds that lose rankings. Operators rebuilding their websites without SEO migration planning regularly lose 30 to 60% of their organic traffic during the rebuild. The damage takes 4 to 9 months to recover from, if it recovers at all.
Our why rebuilds hurt rankings piece covers the migration planning that prevents the damage.
Forgetting AEO entirely. Operators who built their SEO programs in 2022 to 2023 often have not updated their playbook for the AI search reality. Sites that rank well in traditional Google search but earn zero AI citations are leaving the next wave of discovery on the table.
The fix is the AEO investment from Layer 6.
WHAT WORKING REHAB SEO PROGRAMS DO
- Named clinical author + reviewer on every YMYL article
- Original research and named-clinician perspective in content
- Earned editorial placements from healthcare journalists
- Server-side, BAA-covered tracking on the conversion stack
- SEO migration planning before any site rebuild
WHAT BROKEN REHAB SEO PROGRAMS SKIP
- “Editorial Team” bylines on clinical YMYL articles
- Generic listicles built off keyword tools and competitor scrapes
- Bought links and PBN-style link schemes
- Standard Meta pixel + GA4 with no HIPAA review
- Rebuild the site, then realize 50 percent of rankings vanished
What changed in 2025 and 2026
The behavioral health SEO landscape shifted sharply across 2025 and into 2026. Five changes matter operationally for any treatment center running an SEO program now.
DEFINITION
Helpful Content Update (HCU)
Google’s algorithmic system, rolled out across 2024 and 2025, that demotes content created primarily for search engines rather than for human readers. For treatment center sites, HCU specifically punishes commodity-keyword listicles, AI-generated explainer content without clinical review, and scaled-content patterns.
The Helpful Content Update for treatment center content. Google’s Helpful Content Update (HCU) implementation across 2024 and 2025 raised the bar for content quality across all YMYL categories.
Treatment center sites that had been ranking on thin or generic content lost positions, and the recovery for affected sites requires substantive content rewrites rather than minor optimizations.
The AI Overviews rollout and citation pattern shifts. Google AI Overviews rolled out widely across 2024 and 2025, and the citation patterns shifted across 2026 as the engine matured.
The early citation patterns favored Reddit and authoritative third-party sources; the 2026 patterns increasingly include treatment center sites that hold strong entity signals and named clinical authorship.
LegitScript audit pattern shifts. LegitScript’s audit cadence increased across 2025 with more frequent re-certification reviews and tighter operational standards. The implication for organic SEO is that LegitScript-related E-E-A-T signals are now more dynamic; operators must maintain certification continuously rather than treating it as a one-time gate.
Google’s increasing reliance on Reddit and community signals. Google’s 2024 Reddit partnership and the broader AI engine reliance on community sources made Reddit the single largest external citation source for treatment center queries by 2026.
The operational implication is that operators who engage authentically with Reddit communities (real clinicians and operators answering real questions in r/addiction, r/recovery, r/AlAnon, and similar) capture citation share that competitors miss.
FTC’s March 2026 enforcement letters on substance use disorder advertising. The FTC issued enforcement letters in March 2026 targeting treatment centers making unsubstantiated outcome claims (success rates, completion rates, treatment efficacy comparisons).
The FTC Health Products Compliance Guidance provides the framework operators should use to vet their content claims before publication.
The cumulative effect of these five shifts is that the 2024 BH SEO playbook does not work in 2026.
The operators winning their markets are operators who updated their playbook continuously, treated AEO as a primary discipline rather than an experimental sideline, and ran their content production through editorial infrastructure that meets the 2026 bar.
What this means for treatment center operators
The pattern across this guide repeats: BH SEO is structurally different, the seven operational layers compound on each other, the timeline rewards patience over urgency, and the agency selection decision is upstream of everything.
The skip-a-layer pattern is what produces most BH SEO failures. Programs that cover the technical foundation but skip credentialed content production underperform. Programs that produce content but skip the authority and earned media layer underperform. Programs that build authority but skip AEO underperform against operators investing in AI search.
Programs that run all six operational layers but skip the integrated measurement layer cannot defend their budget and get cut before the compounding appears.
The competitive reality in 2026 is that the operators winning their markets started 18 months ago and have continued executing through the timeline. The operators starting now can still catch up, because the discipline is more important than the head start, but the runway compresses every quarter.
Operators waiting another 12 months to commit will find themselves competing against established positions that paid-only strategies cannot dislodge.
The next step for operators evaluating SEO investment is to read the deeper cluster pieces this guide links to: the technical SEO playbook, the keyword strategy framework, the local SEO playbook, the AEO operational guide, and the agency evaluation framework.
Operators whose billing operations are not yet producing predictable cash flow should also read the shortlist of BH-specialized RCM vendors before scaling SEO investment, because marketing spend compounds only when billing operations are reliable.
Operators ready to evaluate Webserv’s SEO program directly can reach out for a strategy session to walk through their specific operator situation and the right tier of investment for their stage.
Most in-house teams hit a wall not because they lack knowledge, but because they lack bandwidth.
When you are ready to hand it off, Webserv has spent 9 years executing exactly this for treatment centers nationwide.
Frequently asked questions about SEO for drug rehab centers
How is SEO for drug rehab centers different from general SEO?
Drug rehab SEO sits at the intersection of YMYL ranking standards, HIPAA-restricted tracking, LegitScript certification gates, FTC enforcement on outcome claims, and Google’s Healthcare and Medicines policy. The constraint stack means general SEO playbooks built for ecommerce or local services miss most of what matters in this vertical.
The right playbook is built around the constraints rather than despite them. Credentialed clinical authorship is required where general SEO treats authorship as optional. Server-side HIPAA-compliant analytics is required where general SEO uses standard pixel tracking. Outcome claims require FTC-grade substantiation where general SEO operates with marketing-grade claims.
Operators who treat the constraints as a forcing function win the category, because the operators who write the new playbook lap the operators trying to retrofit the old one. The seven operational layers above describe the working version.
How long does SEO take to work for a treatment center?
Realistic timeline is 3 months for first measurable lift, 9 to 12 months for compounding admit volume, and 12 to 18 months for category-leading positions. The compounding pattern is the most important variable: operators who quit at month 4 to 6 see no admit lift because the compounding has not appeared yet, while operators who commit to 18 months reliably outperform paid-only competitors.
The phases are predictable. Month 1 to 3 builds the foundation. Month 4 to 6 sees first content cluster expansion and early ranking movement on long-tail queries. Month 7 to 9 produces measurable AI citation share lift and the first commercial-intent queries reaching page one. Month 10 to 12 produces the first admit attribution data and the compounding effect becomes visible.
Operators who expect paid-media-speed organic results will be disappointed. The math of quitting at month 6 is the worst possible outcome because it loses the months invested without producing the compounding the investment was designed to capture.
How much should a treatment center budget for SEO?
Four tiers cover the working range. Tier 1 at $3,000 to $5,000 monthly is foundational maintenance for single-location operators with existing rankings. Tier 2 at $7,000 to $12,000 monthly is the floor for compounding programs and the appropriate tier for most single-location operators. Tier 3 at $15,000 to $25,000 monthly is multi-state or multi-facility operator territory with full seven-layer execution. Tier 4 at $30,000+ monthly is national operators with multi-location footprints.
The most common budget mistake is committing to a Tier 2 budget but cutting it during the first 6 months when the compounding has not yet appeared. Programs cut at month 4 to 6 produce Tier 1 outcomes because the compounding layers require runway.
The right framing is that SEO budget is a strategic investment with an 18-month payback window. Operators thinking about it as a month-to-month marketing line item produce mismatched expectations against the timeline reality, and the mismatched expectations are what cause programs to fail.
Can I do SEO for my rehab in-house, or do I need an agency?
Most operators benefit from agency engagement. The agency model concentrates BH-specific expertise that operators cannot recruit individually, provides technical depth and content production capacity at lower cost than in-house team building, and operationalizes the seven-layer playbook through established workflows.
In-house teams work for operators with $1 million-plus annual marketing budgets, dedicated content production capacity, and strong internal clinical leadership. The all-in cost for a competent in-house SEO team runs $400,000 to $800,000 annually, which only makes sense for operators with the budget to support it.
The hybrid model splits the work: agency handles technical and production capacity, operator owns brand voice and clinical leadership. This model works well for Tier 3 operators with strong internal teams who want to scale beyond what the internal team can produce alone.
Does LegitScript certification affect organic SEO rankings?
Yes, more than most operators realize. LegitScript was originally designed as a paid advertising gate, but the certification now functions as an organic E-E-A-T signal that Google’s quality raters and AI engines treat as a verifiable third-party endorsement. Sites that hold valid LegitScript certification accumulate trust signals that flow into organic ranking and AI citation eligibility.
The implication is that LegitScript maintenance is now part of the organic SEO playbook, not just the paid playbook. The cross-channel effect also tightened across 2025: a LegitScript audit that surfaces operational issues affects both paid eligibility and organic ranking authority.
The 2026 best practice is continuous LegitScript maintenance with internal audit cadence aligned to the external re-certification reviews, and explicit documentation of the certification status in schema markup and on-page trust signals. The full operational picture lives in our LegitScript compliance guide.
Should treatment centers invest in AI search optimization (AEO)?
Yes, urgently. AI search engines are now primary discovery surfaces for treatment center queries. Treatment-seeking research that previously routed through traditional Google search now increasingly routes through AI engines that synthesize answers from cited sources. Operators not investing in AEO are losing share on a metric most marketing teams are not measuring.
AEO is structured around seven operational layers: entity SEO, passage-level optimization, named clinical authorship, Reddit and community citation building, FAQ structuring, source diversification, and citation share measurement. The investments compound in the same pattern as traditional SEO but with a faster lead time (typically 12 to 16 weeks for measurable citation share lift versus 6 to 12 months for measurable organic ranking lift).
The bigger picture is that 2026 is the year AEO becomes a primary discovery layer. Operators investing now position for the next phase; operators waiting until the layer is fully mature will be too late to catch the early-mover citation share that compounds into category leadership.
What are the most common SEO mistakes treatment centers make?
The eight recurring patterns include generic content without clinical review, stock photography and stock language, listicles without expert depth, bought links and link schemes, HIPAA-noncompliant tracking, population-specific content treated as interchangeable, site rebuilds that lose rankings, and forgetting AEO entirely. Each pattern is individually fixable but cumulatively expensive when allowed to compound.
The mistakes share a common root: the operator (or the agency) is running general SEO with healthcare modifications instead of running BH-specific SEO. The constraint stack and the operational reality of the category require a different playbook.
The diagnostic worth running is the annual SEO audit. Operators running annual audits identify the patterns before they compound; operators who run their programs without audit cadence accumulate damage that surfaces only when the program is failing. The audit should cover all seven operational layers, with explicit checks for the eight failure patterns above. If you want a second opinion on your current SEO program, reach out for a strategy session and we can walk through where your site sits in the seven-layer build.
The perspective in this article comes from 9 years working exclusively inside behavioral health.
We are a team built by people in recovery who understand that behind every admission is someone asking for help. If that resonates, get to know us.
Trevor Gage is the Director of Earned & Owned Media at Webserv, a digital marketing agency for treatment centers.