Most behavioral health SEO agencies sell SEO output without the operating system underneath that makes the output compound. The output looks competent and is brand-interchangeable. Three months in, the operator notices the content sounds nothing like their facility. Six months in, the strategist who knew the account leaves and institutional knowledge leaves with them. Twelve months in, the engagement has produced a lot of content and very little compounding.
The agencies whose engagements actually compound run a documented operating system we call the Client Brain. It captures positioning, clinical leadership, audience documentation, voice, trust signals, content gap maps, performance history, and operator-stated constraints. It lives in a system that survives team turnover.
This guide breaks down the eight components of a functional Client Brain, the diligence questions to ask before signing with any SEO agency, what the output looks like when the system is working, and the failure patterns to watch for.
Key Takeaways
- A Client Brain is the internal operating system that captures everything an agency knows about a specific facility and makes that knowledge available to every team member doing work for the account.
- Most agencies do not have one because building it costs more than it bills, junior-team turnover destroys the institutional knowledge, and operators do not know to ask for it during the buying process.
- The system has eight components: positioning, clinical leadership and credentials, audience documentation, voice guide, trust signal inventory, topic and content gap map, past content performance, and operator-stated constraints.
- Six diligence questions surface whether the agency has one before you sign. Eight operator checks audit whether your current agency is running on a working system.
- The Client Brain is the only piece of infrastructure that makes content compound. Output volume is downstream of the system that produces it. Operators evaluating only on price and deliverable count select for agencies that ship volume without compounding effect.
Most treatment center operators evaluate SEO and content agencies on outputs. The number of blog posts shipped per month. The keywords on the tracker. The dashboard’s traffic line going up. The agency that produces the most stuff wins the pitch.
The problem is that outputs are downstream of a decision the operator never gets to inspect. The decision is: what does this agency actually know about my facility?
Without an answer to that question, every blog post, service page rewrite, and content brief is a guess wearing a brand template. Some land. Most do not.
The agencies that consistently produce authority content for treatment centers have built something most operators have never been shown: an internal operating system that captures, organizes, and operationalizes everything the team has learned about a specific facility.
We call it a Client Brain. The name is unremarkable. The system is the work.
The reason most rehab content is interchangeable has nothing to do with the agencies being lazy. They do not have a system for remembering anything specific about the client they are writing for. The client brain is the only piece of infrastructure that makes content compound.
Trevor Gage, Director of Marketing, Webserv
This article is the operator-facing version of the Client Brain methodology we use at Webserv. It is written as a buying guide for treatment center operators who are either evaluating a new SEO or content agency, or auditing the one they have. The framework holds whether the agency calls it a Client Brain, a Brand Hub, an Account Knowledge Base, or something else entirely. The name matters less than the system.
The seven sections cover what a Client Brain actually is, why most agencies do not have one, and the eight components that make one functional. It then covers the diligence questions to ask before signing, what good output looks like when the system is working, the common failure modes, and the operator checklist for auditing your current agency against the framework.
DEFINITION
The Client Brain Operating System
Webserv’s framework for what an SEO agency should know about a client at the operating level: program structure, payer mix, current keyword inventory, prior agency history, content cluster status, and ranking baselines. The Client Brain is the difference between agencies running the same playbook for every client and agencies running a playbook calibrated to the operator’s actual situation.
What a Client Brain actually is
A Client Brain is the internal document, system, or knowledge base that captures everything the agency knows about a specific client and makes that knowledge available to every team member doing work for that client. It is the answer to the question “what does this agency know about us that nobody else knows?”
In a working Client Brain, an editor writing a blog post for a treatment center can look up the medical director’s published positions, the facility’s specific accreditation history, the payer mix targets the operator has shared, and the brand voice rules the team has documented. The same writer can look up the audiences the program is built for, the topics the operator does not want covered, and the previous content that has worked or failed.
The output of the system is content that sounds like the operator’s facility. The byproduct of the system is content that compounds, because each new piece references and builds on what the agency has already established.
The opposite of a Client Brain is what most operators experience when they hire an agency: a kickoff call, a brand questionnaire, three months of generic content, and a quarterly business review where everyone tries to remember what the strategy was supposed to be. The work resets every time a new editor or strategist joins the team because nothing was actually captured in a usable format.
Why most agencies do not have one
Three reasons most SEO and content agencies operate without a Client Brain:
Treatment center operators evaluating agencies should look at the SEO program structure first, because the Client Brain is the operating layer underneath an agency’s SEO output. Without that underlying system, even well-funded SEO programs ship category-typical content that fails to compound.
Building one costs more than it bills. A serious Client Brain takes 20 to 40 hours of agency time to build at the start of the engagement and continuous maintenance after that. Most agencies are operating on retainers that do not have room for that upfront investment. They skip it and ship faster output.
The team turnover model breaks it. Agencies with high junior-team turnover cannot maintain a Client Brain even if they build one. The system requires institutional knowledge held by senior team members who stay on the account. Agencies that route work through a rotating cast of contractors lose the knowledge between handoffs.
Most operators do not know to ask. If the operator does not specifically evaluate the Client Brain during the buying process, the agency has no incentive to build one. Operators evaluating only on price, deliverable count, and dashboard polish select for agencies that optimize for those variables. The Client Brain becomes the dropped requirement.
The compound effect is that most operators hire agencies that do not have the operating infrastructure to produce content that consistently sounds like their facility. The agency ships volume. The volume reads as generic. The CPL on owned content underperforms the paid channel because the content does not differentiate.
The eight components of a functional Client Brain
A working Client Brain has eight discrete components. The components are documented, version-controlled, and accessible to every team member doing work for the account. Each one feeds a specific category of decision the agency has to make on a recurring basis.
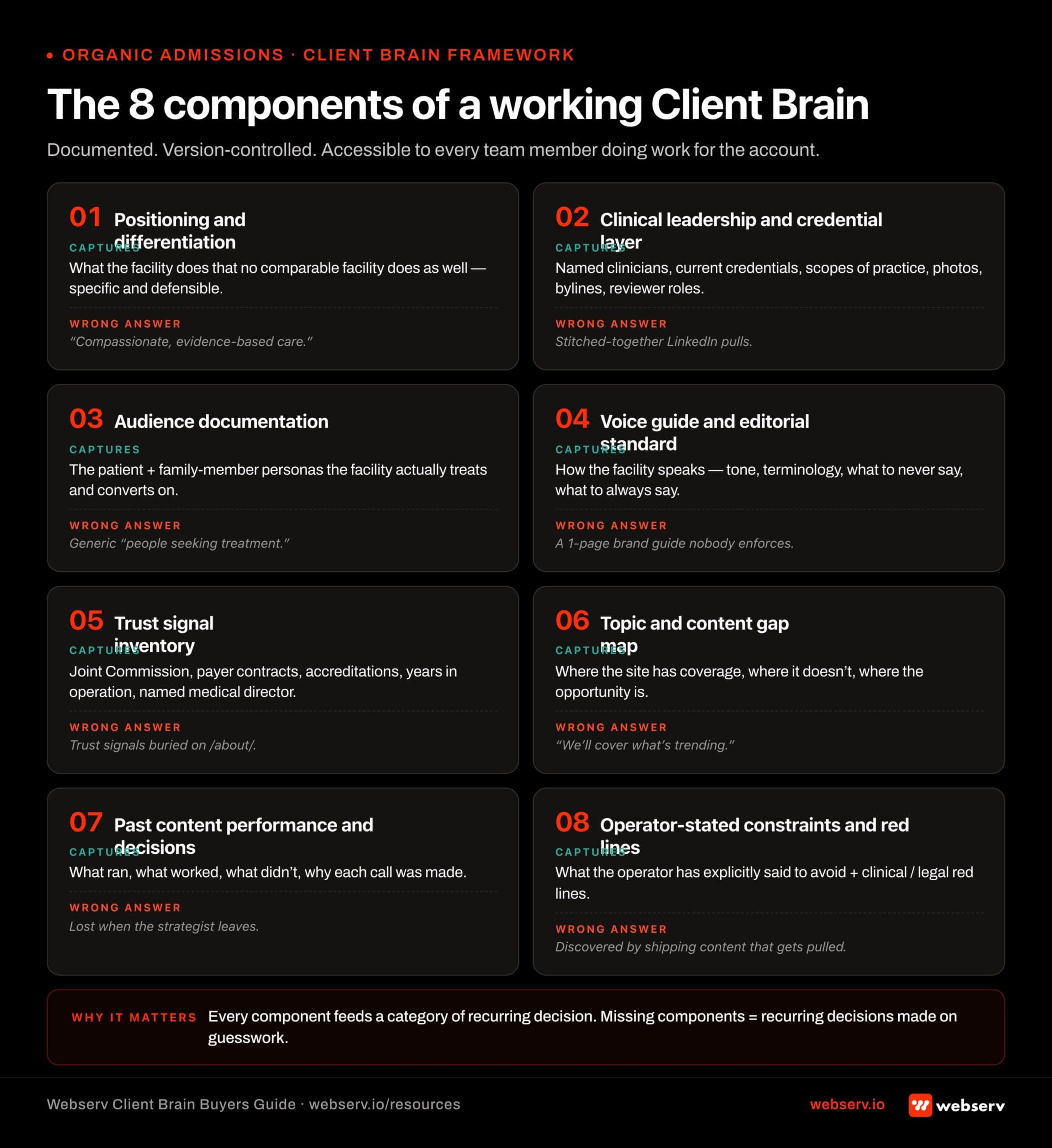 Infographic titled ‘The 8 components of a working Client Brain’ showing the documented, version-controlled operating system every SEO agency should maintain for a behavioral health client. Component 1 Positioning and differentiation: captures what the facility does that no comparable facility does as well, specific and defensible; wrong answer is ‘compassionate, evidence-based care.’ Component 2 Clinical leadership and credential layer: captures named clinicians with current credentials, scopes of practice, photos, bylines, and reviewer roles; wrong answer is stitched-together LinkedIn pulls. Component 3 Audience documentation: captures the patient and family-member personas the facility actually treats and converts on; wrong answer is generic ‘people seeking treatment.’ Component 4 Voice guide and editorial standard: captures how the facility speaks including tone, terminology, what to never say, and what to always say; wrong answer is a one-page brand guide nobody enforces. Component 5 Trust signal inventory: captures Joint Commission, payer contracts, accreditations, years in operation, and named medical director; wrong answer is trust signals buried on the about page. Component 6 Topic and content gap map: captures where the site has coverage, where it doesn’t, and where the opportunity is; wrong answer is ‘we’ll cover what’s trending.’ Component 7 Past content performance and decisions: captures what ran, what worked, what didn’t, and why each call was made; wrong answer is institutional knowledge lost when the strategist leaves. Component 8 Operator-stated constraints and red lines: captures what the operator has explicitly said to avoid plus clinical and legal red lines; wrong answer is discovered by shipping content that gets pulled. Footer: ‘Every component feeds a specific category of recurring decision. Missing components = recurring decisions made on guesswork.’
Infographic titled ‘The 8 components of a working Client Brain’ showing the documented, version-controlled operating system every SEO agency should maintain for a behavioral health client. Component 1 Positioning and differentiation: captures what the facility does that no comparable facility does as well, specific and defensible; wrong answer is ‘compassionate, evidence-based care.’ Component 2 Clinical leadership and credential layer: captures named clinicians with current credentials, scopes of practice, photos, bylines, and reviewer roles; wrong answer is stitched-together LinkedIn pulls. Component 3 Audience documentation: captures the patient and family-member personas the facility actually treats and converts on; wrong answer is generic ‘people seeking treatment.’ Component 4 Voice guide and editorial standard: captures how the facility speaks including tone, terminology, what to never say, and what to always say; wrong answer is a one-page brand guide nobody enforces. Component 5 Trust signal inventory: captures Joint Commission, payer contracts, accreditations, years in operation, and named medical director; wrong answer is trust signals buried on the about page. Component 6 Topic and content gap map: captures where the site has coverage, where it doesn’t, and where the opportunity is; wrong answer is ‘we’ll cover what’s trending.’ Component 7 Past content performance and decisions: captures what ran, what worked, what didn’t, and why each call was made; wrong answer is institutional knowledge lost when the strategist leaves. Component 8 Operator-stated constraints and red lines: captures what the operator has explicitly said to avoid plus clinical and legal red lines; wrong answer is discovered by shipping content that gets pulled. Footer: ‘Every component feeds a specific category of recurring decision. Missing components = recurring decisions made on guesswork.’1. Positioning and differentiation
What the facility does that no other comparable facility does as well.
Not “compassionate care.” Specific: “Only adolescent residential program in California with on-site academic credit for high school.” “Veteran-built program with the only TRICARE West contract in the regional service area.” “Boutique residential program with 24-hour direct access to the medical director.”
The positioning has to be true, defensible, and useful for the family member doing the comparison. If the operator cannot articulate the positioning in one paragraph, the Client Brain captures the work the agency does to surface it.
2. Clinical leadership and credential layer
Every named clinician with verifiable credentials, schools, licenses, specialties, publication history, and current scope of practice at the facility. Photographs that meet the brand visual standard. Quote-ready bio paragraphs at three different lengths (one-sentence, one-paragraph, full).
This component is the load-bearing wall for EEAT, AEO citation, and trust-signal placement across the site. Google’s own E-E-A-T helpful content guidance is explicit that healthcare content without named, credentialed authorship is structurally disadvantaged in YMYL ranking. Our Topical Authority for Treatment Centers explainer covers the architecture this connects to.
3. Audience documentation
The specific audiences the facility serves, ranked by share of admit volume. Family-member personas (the spouse, the parent, the adult child, the sibling). Patient personas where applicable. Professional referrer personas (EAP coordinator, primary care, school counselor, interventionist).
For each audience, the Client Brain captures the questions they ask, the vocabulary they use (and do not use), the platforms where they look for treatment, the trust signals they respond to, the friction points that prevent them from calling. The audience-research discipline pairs with the content production patterns we cover in our healthcare content creation guide.
4. Voice guide and editorial standard
Tone calibration. Default emotional register. Vocabulary the brand uses. Vocabulary the brand avoids. Punctuation conventions. Sentence-length defaults. Banned phrases (clichés, marketing tone, regulatory red flags). Approved framings for sensitive topics.
The voice guide is granular enough that a writer who has never worked on the account can produce on-brand copy from the guide alone. The standard we hold our voice guides to is that a senior editor reviewing a draft can identify voice violations without needing to consult anyone. Practical examples of what a well-built voice guide enables show up in our healthcare blog and article writing primer.
5. Trust signal inventory
Every credible thing the facility carries that should appear in the content. Accreditation badges. State licensing numbers. Payer contracts. Joint Commission designations. CARF status. ASAM affiliation. Years in operation. Patient volume. Peer-reviewed publications by clinical staff. Awards. Media features.
Each trust signal has a documented placement: which pages it belongs on, what visual treatment it gets, what schema markup it produces. The signals do not live exclusively on /about/. They live on the pages where families convert.
6. Topic and content gap map
The cluster taxonomy the facility’s content is organized into. Service pages, level-of-care pages, population pages, condition pages, modality pages. Active content gaps the agency has identified. Topics the operator has explicitly asked to cover. Topics the operator has asked to avoid.
The map is cross-referenced against keyword research, competitor coverage, and AI citation share by query. The agency uses it to allocate quarterly content investment. The keyword-research foundation under this work is detailed in our keyword strategy guide for rehab and mental health providers, and the technical site-architecture layer is covered in our technical SEO guide for treatment center websites.
7. Past content performance and decisions
Every piece of content the agency has produced for the facility, tagged with performance data, the strategic decision it was meant to serve, and what the team learned from how it performed.
The cumulative output is institutional memory. A writer six months into the engagement can look up “what did we try for the dual-diagnosis cluster” and find both the assets and the lessons.
8. Operator-stated constraints and red lines
Topics the operator does not want covered. Phrasings the operator dislikes. Competitive sites the operator does not want referenced. Legal sensitivities. Investor or partnership considerations. Internal politics the agency needs to respect.
Every operator has a list of red lines that the agency learns about through painful violations if they are not documented in advance. The Client Brain captures them at the start of the engagement and updates them as the relationship evolves.
How SoCal Sunrise generated 85 admissions and 2,297% ROI from SEO in 6 months
A ground-up SEO rebuild using the Pathfinder Parents Methodology turned an invisible online presence into a top-ranking admissions engine.
Read the case study →85 admits and 3,152 leads attributed to organic
The diligence questions to ask before signing
Six questions surface whether the agency you are evaluating has a Client Brain or is selling output without the underlying system.
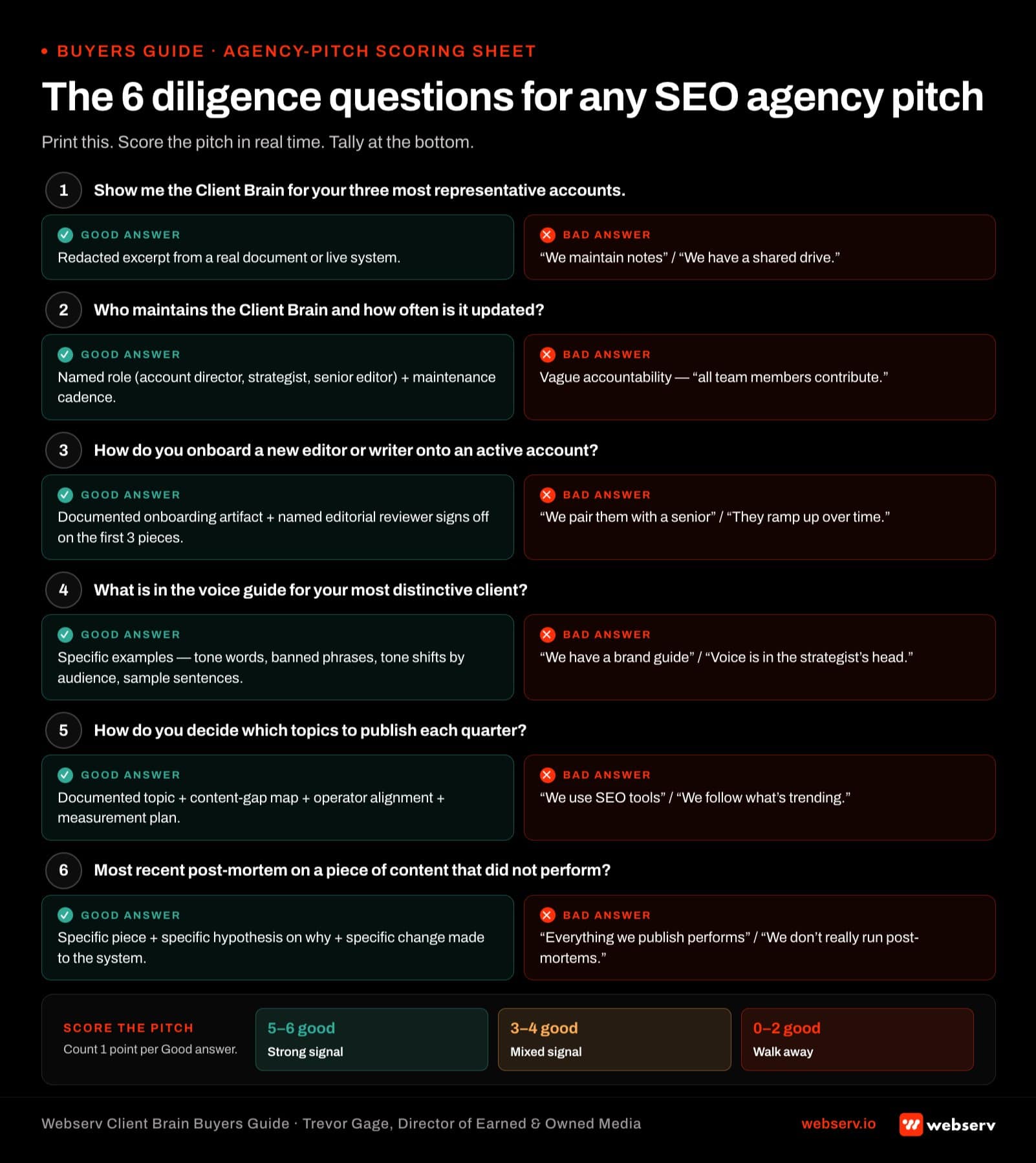 Infographic titled ‘The 6 diligence questions for any SEO agency pitch’ designed for behavioral health operators to score agency pitches in real time. Each question shows the good answer and the bad answer side by side. Question 1: Show me the Client Brain for your three most representative accounts. Good answer: redacted excerpt from a real document or live system. Bad answer: ‘we maintain notes’ or ‘we have a shared drive.’ Question 2: Who maintains the Client Brain and how often is it updated? Good answer: a named role plus a maintenance cadence. Bad answer: vague accountability or ‘all team members contribute.’ Question 3: How do you onboard a new editor or writer onto an active account? Good answer: documented onboarding artifact plus named editorial reviewer signing off on the first three pieces. Bad answer: ‘we pair them with a senior’ or ‘they ramp up over time.’ Question 4: What is in the voice guide for your most distinctive client? Good answer: specific examples including tone words, banned phrases, tone shifts by audience, and sample sentences. Bad answer: ‘we have a brand guide’ or ‘voice is captured in the strategist’s head.’ Question 5: How do you decide which topics to publish each quarter? Good answer: documented topic and content gap map plus operator alignment plus measurement plan. Bad answer: ‘we use SEO tools’ or ‘we follow what’s trending.’ Question 6: What is in your most recent post-mortem on a piece of content that did not perform? Good answer: specific piece plus specific hypothesis on why plus specific change made to the system. Bad answer: ‘everything we publish performs’ or ‘we don’t really run post-mortems.’ Tally band: count one point per good answer. 5-6 strong signal, 3-4 mixed, 0-2 walk away.
Infographic titled ‘The 6 diligence questions for any SEO agency pitch’ designed for behavioral health operators to score agency pitches in real time. Each question shows the good answer and the bad answer side by side. Question 1: Show me the Client Brain for your three most representative accounts. Good answer: redacted excerpt from a real document or live system. Bad answer: ‘we maintain notes’ or ‘we have a shared drive.’ Question 2: Who maintains the Client Brain and how often is it updated? Good answer: a named role plus a maintenance cadence. Bad answer: vague accountability or ‘all team members contribute.’ Question 3: How do you onboard a new editor or writer onto an active account? Good answer: documented onboarding artifact plus named editorial reviewer signing off on the first three pieces. Bad answer: ‘we pair them with a senior’ or ‘they ramp up over time.’ Question 4: What is in the voice guide for your most distinctive client? Good answer: specific examples including tone words, banned phrases, tone shifts by audience, and sample sentences. Bad answer: ‘we have a brand guide’ or ‘voice is captured in the strategist’s head.’ Question 5: How do you decide which topics to publish each quarter? Good answer: documented topic and content gap map plus operator alignment plus measurement plan. Bad answer: ‘we use SEO tools’ or ‘we follow what’s trending.’ Question 6: What is in your most recent post-mortem on a piece of content that did not perform? Good answer: specific piece plus specific hypothesis on why plus specific change made to the system. Bad answer: ‘everything we publish performs’ or ‘we don’t really run post-mortems.’ Tally band: count one point per good answer. 5-6 strong signal, 3-4 mixed, 0-2 walk away.1. Show me the Client Brain for your three most representative accounts.
The right answer is a redacted excerpt from a real document or system. The wrong answer is “we maintain notes” or “we have a shared drive.” If the agency cannot produce a Client Brain artifact at the buying stage, they do not have one in production.
2. Who maintains the Client Brain and how often is it updated?
The right answer names a specific role (account director, strategist, senior editor) and a maintenance cadence (every quarterly review, after every strategy call, continuous). The wrong answer is vague accountability or “all team members contribute.”
3. How do you onboard a new editor or writer onto an active account?
The right answer references the Client Brain as the primary onboarding asset. The wrong answer is a shadowing or hand-off model that depends on a specific senior team member transferring knowledge informally. Knowledge that lives in one head does not survive turnover.
4. What is in the voice guide for your most distinctive client?
The right answer is specific. Vocabulary rules. Banned phrases. Tone calibrations. The wrong answer is a one-page brand summary that could have been written about any treatment center.
5. How do you decide which topics to publish each quarter?
The right answer references the topic and content gap map (Component 6 above), keyword research, competitor coverage, and operator priorities. The wrong answer is “our editorial team picks topics based on industry trends.”
6. What is in your most recent post-mortem on a piece of content that did not perform?
The right answer is a specific document or system entry that names the piece, the hypothesis it tested, the actual performance, the lesson the team captured, and how that lesson updated the Client Brain. The wrong answer is “we look at analytics quarterly.”
If the agency cannot answer all six questions specifically and credibly, they are selling content output without the underlying knowledge infrastructure. The output may still be acceptable. The compounding will not happen.
What good output looks like when the Client Brain is working
The visible result of a working Client Brain is content that reads as if the agency understands the facility better than most internal team members do. The output traits operators consistently report:
The output traits below pair with the standards covered in our AI search citation guide and our honest review of marketing agencies for rehabs. Operators who recognize the patterns above in their current engagement have a working system. Operators who do not are paying for output without the infrastructure that compounds it.
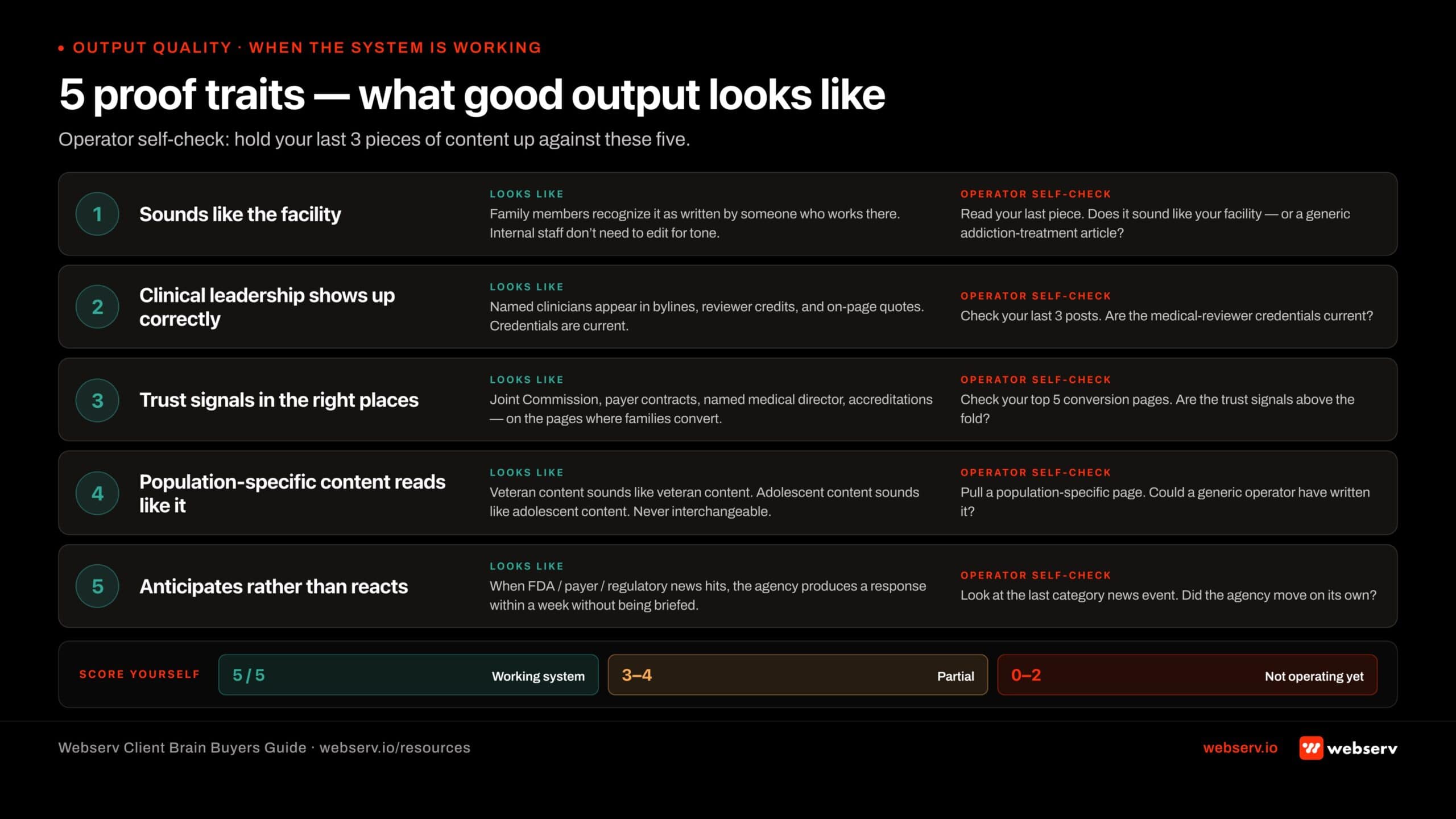 Infographic titled ‘5 proof traits — what good output looks like when the Client Brain is working’ showing the visible markers that an SEO agency’s Client Brain operating system is actually being executed against behavioral health content. Trait 1: The content sounds like the facility — family members reading it would recognize it as being written by someone who works there, and internal staff do not need to edit for tone, terminology, or facility-specific accuracy; operator self-check: read your last piece and ask whether it sounds like your facility or like a generic addiction treatment article. Trait 2: The clinical leadership shows up correctly — named clinicians appear in author bylines, medical reviewer credits, on-page quotes, and bios with the correct credentials and current scope; operator self-check: are the medical reviewer credentials on your last 3 posts current? Trait 3: Trust signals appear in the right places — Joint Commission, payer contracts, named medical director, accreditations, and years in operation surface on the pages where families actually convert, not buried on the about page; operator self-check: are the trust signals on your top 5 conversion pages above the fold? Trait 4: Population-specific content reads like it was written for that population — veteran content sounds like veteran content, adolescent content sounds like adolescent content, mental health content is not treated as interchangeable with addiction content; operator self-check: could a generic operator have written your last population-specific page? Trait 5: The agency anticipates rather than reacts — when a news event hits the category like FDA enforcement, payer policy change, or regulatory shift, the agency produces a relevant response within a week without needing the operator to brief them; operator self-check: did the agency move on the last category news event without being briefed? Tally guidance: 5 of 5 means the system is working, 3 to 4 partial, 0 to 2 the agency does not have the Client Brain operating yet.
Infographic titled ‘5 proof traits — what good output looks like when the Client Brain is working’ showing the visible markers that an SEO agency’s Client Brain operating system is actually being executed against behavioral health content. Trait 1: The content sounds like the facility — family members reading it would recognize it as being written by someone who works there, and internal staff do not need to edit for tone, terminology, or facility-specific accuracy; operator self-check: read your last piece and ask whether it sounds like your facility or like a generic addiction treatment article. Trait 2: The clinical leadership shows up correctly — named clinicians appear in author bylines, medical reviewer credits, on-page quotes, and bios with the correct credentials and current scope; operator self-check: are the medical reviewer credentials on your last 3 posts current? Trait 3: Trust signals appear in the right places — Joint Commission, payer contracts, named medical director, accreditations, and years in operation surface on the pages where families actually convert, not buried on the about page; operator self-check: are the trust signals on your top 5 conversion pages above the fold? Trait 4: Population-specific content reads like it was written for that population — veteran content sounds like veteran content, adolescent content sounds like adolescent content, mental health content is not treated as interchangeable with addiction content; operator self-check: could a generic operator have written your last population-specific page? Trait 5: The agency anticipates rather than reacts — when a news event hits the category like FDA enforcement, payer policy change, or regulatory shift, the agency produces a relevant response within a week without needing the operator to brief them; operator self-check: did the agency move on the last category news event without being briefed? Tally guidance: 5 of 5 means the system is working, 3 to 4 partial, 0 to 2 the agency does not have the Client Brain operating yet.The content sounds like the facility. Family members reading it would recognize it as being written by someone who works there. Internal staff reading it do not need to edit for tone, terminology, or facility-specific accuracy.
The clinical leadership shows up correctly. Named clinicians appear in author bylines, medical reviewer credits, on-page quotes, and bios with the correct credentials and current scope. The credentials are not stitched together from a stale LinkedIn pull.
Trust signals appear in the right places. Joint Commission, payer contracts, named medical director, accreditations, and years-in-operation surface on the pages where families convert. The signals are not buried on /about/.
Population-specific content reads like it was written for that population. Veteran content sounds like veteran content. Adolescent content sounds like adolescent content. Mental health content does not get treated as interchangeable with addiction content.
The agency anticipates rather than reacts. When a news event hits the category (FDA enforcement, payer policy change, regulatory shift), the agency produces a relevant response within a week without needing the operator to brief them on what the response should be.
The work compounds. Each new piece of content references and builds on the existing library. The site reads as a coherent topical authority rather than a sequence of disconnected blog posts.
The compound effect on commercial performance: cost per organic-attributed admit declines quarter over quarter, AI citation share rises on the queries that matter, and the operator’s internal team spends less time on revisions because the agency is producing content that lands the first time.
Common failure modes when the Client Brain breaks down
Five patterns we see when an engagement is producing content but not the compounding effect a Client Brain should deliver.
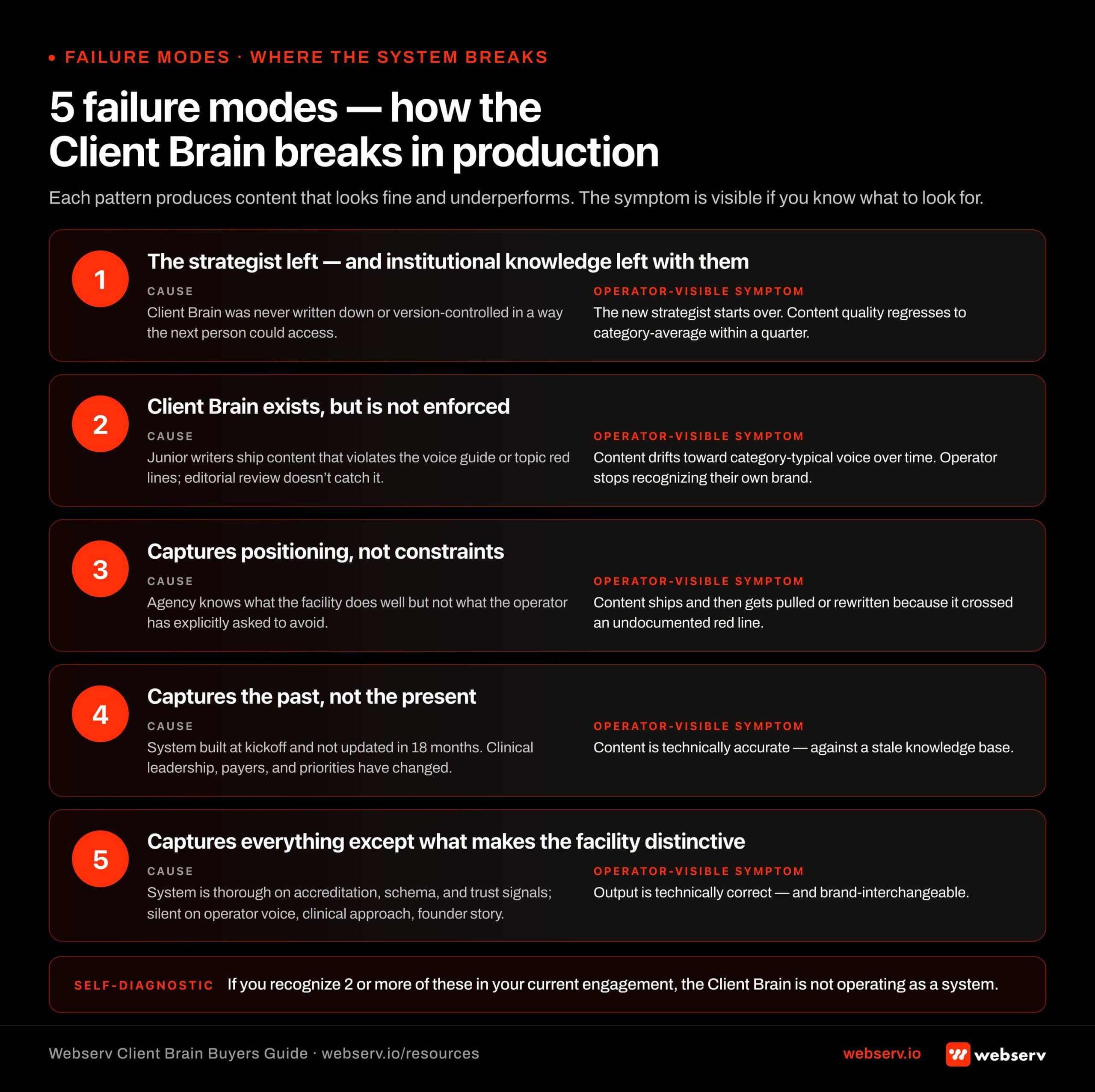 Infographic titled ‘5 failure modes — how the Client Brain breaks down in production’ showing the patterns where an SEO agency’s Client Brain operating system fails to compound. Failure 1: The strategist left and institutional knowledge left with them — caused by the Client Brain never being written down or version-controlled in a way the next person could access; symptom is the new strategist starts over and content quality regresses. Failure 2: Client Brain exists but is not enforced — caused by junior writers shipping content that violates the voice guide or topic red lines while editorial review doesn’t catch the violations; symptom is content drifts toward category-typical voice over time. Failure 3: Captures positioning but not constraints — caused by the agency knowing what the facility does well but not what the operator has explicitly asked to avoid; symptom is content ships and then gets pulled or rewritten because it crossed an undocumented red line. Failure 4: Captures the past but not the present — caused by the system being built at kickoff and not updated in 18 months while clinical leadership, payer contracts, and strategic priorities have all changed; symptom is content technically accurate against a stale knowledge base. Failure 5: Captures everything except what makes the facility distinctive — caused by the system being thorough on accreditation, schema, and trust signals while silent on operator voice, differentiating clinical approach, and founder story; symptom is output that is technically correct and brand-interchangeable. Footer guidance: if you recognize two or more of these in your current engagement, the Client Brain is not operating as a system.
Infographic titled ‘5 failure modes — how the Client Brain breaks down in production’ showing the patterns where an SEO agency’s Client Brain operating system fails to compound. Failure 1: The strategist left and institutional knowledge left with them — caused by the Client Brain never being written down or version-controlled in a way the next person could access; symptom is the new strategist starts over and content quality regresses. Failure 2: Client Brain exists but is not enforced — caused by junior writers shipping content that violates the voice guide or topic red lines while editorial review doesn’t catch the violations; symptom is content drifts toward category-typical voice over time. Failure 3: Captures positioning but not constraints — caused by the agency knowing what the facility does well but not what the operator has explicitly asked to avoid; symptom is content ships and then gets pulled or rewritten because it crossed an undocumented red line. Failure 4: Captures the past but not the present — caused by the system being built at kickoff and not updated in 18 months while clinical leadership, payer contracts, and strategic priorities have all changed; symptom is content technically accurate against a stale knowledge base. Failure 5: Captures everything except what makes the facility distinctive — caused by the system being thorough on accreditation, schema, and trust signals while silent on operator voice, differentiating clinical approach, and founder story; symptom is output that is technically correct and brand-interchangeable. Footer guidance: if you recognize two or more of these in your current engagement, the Client Brain is not operating as a system.Pattern 1: The strategist on the account left and the institutional knowledge went with them. The new strategist starts over. The Client Brain was never written down or was version-controlled in a way that the next person could not access.
Pattern 2: The agency has a Client Brain but does not enforce it. Junior writers ship content that violates the voice guide or the topic red lines because the editorial review process does not catch the violations. The system exists. The execution does not.
Pattern 3: The Client Brain captures positioning but not constraints. The agency knows what the facility does well but not what the operator has explicitly asked to avoid. The result is content that ships and then gets pulled or rewritten because it crossed an undocumented red line. Constraint-aware editorial discipline is the same posture our healthcare advertising compliance overview covers on the paid side.
Pattern 4: The Client Brain captures the past but not the present. The system was built at kickoff and has not been updated in 18 months. The clinical leadership has changed. The payer contracts have changed. The operator’s strategic priorities have changed. The agency is still producing content against a stale knowledge base.
Pattern 5: The Client Brain captures everything except what makes the facility distinctive. The system is thorough on accreditation, schema, and trust signals, and silent on the specific operator voice, the differentiating clinical approach, or the founder story. The output is technically correct and brand-interchangeable.
Each failure mode is recoverable. The recovery work is recognizable as Client Brain maintenance and rebuild. Agencies that do this work treat the Client Brain as a continuous deliverable rather than a one-time setup. Agencies that do not are running on accumulating drift.
The operator checklist for auditing your current agency
If you are running an existing engagement and want to assess whether the agency has a working Client Brain, the eight checks below produce a clear read inside two weeks.
Operators running this audit will benefit from the comparison frameworks in our honest review of rehab marketing agencies and the strategic context in our AI search citation guide. An agency that fails this audit on two or more dimensions is not running a Client Brain in production, regardless of what the pitch deck claimed.
1. Ask for the document. Request the Client Brain or equivalent knowledge base as a deliverable. The response tells you whether one exists in production. If it does, the document tells you how mature it is.
2. Run the voice test. Pull three pieces of content the agency has produced in the last 90 days. Read them side by side with three pieces of content the agency produced for a different client. If you cannot distinguish your content from the other client’s content without checking the bylines, the voice system is not working.
3. Run the trust signal audit. Pull a level-of-care page or a population page the agency has built. Check whether the Joint Commission seal, named medical director, payer list, and accreditation badges appear above the fold. If they do not, the trust signal inventory is not driving placement decisions.
4. Run the clinical accuracy test. Pull three blog posts that reference your facility’s clinical approach. Have your medical director review them for accuracy without first telling them the agency wrote them. If the medical director catches more than one accuracy issue per post, the clinical leadership component of the Client Brain is weak.
5. Run the new-team-member test. Ask the agency to assign a new writer or editor to your account. Tell them you want to see the first three pieces that writer produces. The quality of those three pieces tells you whether the Client Brain is documented well enough to onboard new team members.
6. Run the post-mortem test. Pull a piece of content that underperformed in the last six months. Ask the agency what they learned and how the lesson updated their approach. A specific answer with a documented update is the right answer. “We are still looking into it” is not.
7. Run the cross-cluster test. Look at content the agency has produced across SEO, content marketing, paid media, and any other channel they handle. Check whether the voice, positioning, and trust signals are consistent. If the same agency is producing content that reads as if it was written for different brands, the Client Brain is not propagating across teams.
8. Run the compounding test. Pull your content performance over the last 12 months. If your cost per organic-attributed admit is flat or rising, the content is not compounding. The Client Brain is either absent, drifting, or not being used to drive content decisions. The Content Marketing Institute’s annual B2C research consistently shows that documented strategy is the single largest predictor of program effectiveness, which maps to the same operational discipline a Client Brain enforces.
Two or three failures across the eight checks suggest the engagement is producing output without the underlying infrastructure. Five or more failures suggest the agency does not have a Client Brain at all and is producing content against generic templates with your facility’s name pasted in.
Frequently asked questions about evaluating an SEO agency for behavioral health
Is the Client Brain something every SEO agency should have, or only larger ones?
Every SEO agency claiming behavioral health specialization should have a Client Brain regardless of size. The category-specific knowledge (LegitScript, HIPAA tracking, OCR enforcement, ASAM levels of care, payer mix realities) requires a documented internal system to capture and pass between team members. Agencies relying on the founder’s head as the only Client Brain are one departure away from losing it.
Smaller agencies sometimes argue the Client Brain is overhead for their size. That argument breaks down in practice. The smaller the agency, the more concentrated the institutional knowledge is in a few people, and the higher the risk to clients if those people leave. A documented Client Brain protects the client against agency-side staff transitions more than it protects the agency itself.
The diligence test is whether the agency can produce examples of their Client Brain documentation in a sales conversation. Specific named client examples with redacted contents is the right answer. Vague references to internal systems is the wrong answer.
How do we audit whether our current agency has a real Client Brain?
Ask the agency to walk you through five specific items they have documented about your facility: your full payer mix with reimbursement patterns, your top 20 admissions queries with current rank and content gap, your competitive set with content depth comparison, your clinical authorship credentials and licensing footprint, and your historical ranking data with the change patterns explained.
A specialist agency with a working Client Brain can produce all five in under 30 minutes. A generalist agency typically struggles past the first two. The gap is not effort or willingness, it is whether the underlying system exists. Without documented capture, the agency has been operating on what its current account manager remembers about your facility, which is a fragile state.
If the audit surfaces gaps, the right next conversation is not termination. It is whether the agency can document what they have inside 30 days and demonstrate the working system at day 60. Most agencies that genuinely understand the vertical can pass that test. Agencies that cannot are revealing a structural problem worth knowing about.
Can a new agency build a Client Brain in the first 90 days?
Yes, when the agency operates a documented Client Brain framework as standard intake. The first 30 days typically focus on payer mix documentation, content audit, competitive mapping, and clinical authorship inventory. Days 30 to 60 add historical ranking analysis, query-set prioritization, and partner-system documentation. Days 60 to 90 close the loop with reporting infrastructure that surfaces what the Client Brain knows back to the operator.
Agencies without a Client Brain framework do not build one inside 90 days even when they say they will. The framework is the institutional system, not the documentation. Operators can usually tell within the first 30 days of a new engagement whether the agency is following a documented intake process or improvising. The signal is whether the agency asks the right questions in the right order versus asking generic onboarding questions.
The diligence question to ask any agency before signing: what does day 1, day 30, day 60, and day 90 look like in your Client Brain build process. A specialist answers with named deliverables per phase. A generalist answers in vague timelines and goal-setting language.
Should we ask to see the Client Brain documentation directly?
Yes, in redacted form. A real Client Brain contains client-specific information that the agency cannot share verbatim, but the structure and depth of the documentation can be demonstrated against an anonymized example. Agencies refusing to show any version of the Client Brain documentation are signaling either that it does not exist or that they are protecting weak documentation from inspection.
The right ask in a sales conversation is to see the table of contents or section headers of a client Client Brain plus one or two redacted excerpts that show depth. A specialist agency provides this readily. A generalist agency typically redirects to capability decks or case studies, which are different artifacts.
If you are already in an engagement with an agency, the request is even more direct. Ask your account manager to walk you through your facility’s Client Brain in your next call. The walkthrough itself reveals whether the system exists and is current, or whether it is an aspirational document that has not been maintained.
What is the difference between a Client Brain and a typical agency project management system?
A project management system tracks what work is happening on your account: tasks, deadlines, deliverables, status updates. The Client Brain is upstream of that. It captures what the agency knows about your facility that informs the decisions about what work should happen. The project management layer is execution. The Client Brain is the strategic context that execution should be calibrated against.
Most agencies have functional project management. Fewer have a Client Brain. The gap shows up in the quality of strategic decisions: which content topics to prioritize, which queries to target, which competitors to learn from, which payer-specific content gaps to fill first. Without the Client Brain, those decisions get made on the account manager’s intuition rather than on documented knowledge of your facility.
When evaluating an agency, the diligence test is to ask the same strategic question to two different people on the account team. If you get the same well-informed answer from both, the Client Brain is operational. If you get different answers, or one of the answers is clearly improvised, the institutional knowledge is concentrated in a single person rather than distributed through a documented system.
What this means for treatment center operators
The Client Brain is the most under-evaluated component of an SEO or content engagement. Operators evaluate agencies on output volume, dashboard polish, and case studies. The output volume is downstream of the system that produces it. The system is the only thing that determines whether the content compounds over time or resets every quarter.
If you are buying a new SEO or content engagement, the diligence questions in this guide are the questions to ask before you sign. The agency that can answer them specifically is the agency whose work will hold up over a 12-month engagement. The agency that cannot is the agency you will fire in nine months when the CPL on owned content has not moved. For a working shortlist of agencies that operate at this standard, see our review of the top healthcare SEO agencies for 2026.
If you are auditing an existing engagement, the eight-check operator audit produces a clear read on whether the agency has the infrastructure to produce content that compounds. The fixes for a broken Client Brain are recognizable and recoverable. The cost of not fixing it is a year of content that does not compound.
We run the Client Brain methodology on every Webserv treatment center account because we audited too many client engagements with previous agencies where the missing system was the proximate cause of underperformance. The work is unglamorous post-positioning operational discipline most agencies do not invest in because clients rarely ask to see it.
If you want help auditing your current agency against the framework above, or talking through what a Client Brain rebuild would look like for your facility, our authority content team handles that work. Get in touch to schedule a discovery call. The audit is free. The honest assessment is the deliverable.
The perspective in this article comes from 9 years working exclusively inside behavioral health.
We are a team built by people in recovery who understand that behind every admission is someone asking for help. If that resonates, get to know us.
Trevor Gage is the Director of Marketing at Webserv, a digital marketing agency for treatment centers.