A mother of a 22-year-old in active opioid use called a treatment center after her son overdosed for the second time in six months. She had spent the previous 90 minutes searching for residential treatment. She landed on five facility websites in that window.
She closed the first one in 8 seconds. The site had a stock photo of a smiling family on a beach as the hero image. The headline promised “your journey to recovery starts here.” The form asked for 14 fields. The phone number was buried in the footer.
She did not close it because she was a sophisticated marketing critic. She closed it because some signal her crisis-state brain processed in two seconds told her this place was not serious.
She called the third facility she visited. Their site had a clinical director’s name and credentials in the hero section. The phone number was the first thing she could see. The intake form asked for five fields. The accreditation logos were visible without scrolling.
That facility admitted her son three hours later. The first facility never got the call.
Inside Webserv’s web design practice for treatment centers, we work with operators on websites that do two jobs at once.
The marketing job (drive inquiries, convert visitors, support paid traffic) is what most operators budget for.
The clinical trust signal job, the job that determines whether the mother on a crisis call keeps the tab open or closes it in eight seconds, is the job most websites get wrong because nobody is responsible for it.
This article makes the case for treating design as a clinical trust signal alongside its marketing function, names the specific design elements that telegraph clinical credibility, and gives operators a framework for getting marketing and clinical leadership aligned on the website without producing thrash.
Key Takeaways
- 75 percent of users judge a business’s credibility based on website design. For treatment centers, that percentage is materially higher because the decision being made carries life-stakes weight and is often made by a family member in active crisis.
- A treatment center website does two jobs at once: marketing (drive inquiries) and clinical trust signaling (telegraph credibility to a family member who may be deciding in 8 seconds whether to keep the tab open). The two jobs overlap in some elements and diverge in others.
- Behavioral health sits inside Google’s YMYL framework at a stricter threshold than most categories. The December 2025 Core Update produced significant ranking changes on 67 percent of health-related websites, with E-E-A-T (Experience, Expertise, Authoritativeness, Trustworthiness) signals as the load-bearing differentiator.
- Eight specific design elements function as clinical trust signals: named clinical authorship, NAP consistency, encryption, accreditation visibility, leadership team photos, facility imagery, response-time signals, and accessibility. Most rehab sites get three or four right and miss the rest.
- The design brief should be co-authored by marketing and clinical leadership. Sites where marketing owns the brief alone tend to over-index on conversion and miss clinical credibility. Sites where clinical owns the brief alone tend to look like academic literature and miss the family-decision psychology.
The Dual-Function Frame
Every other website in the operator’s universe does one job. The ecommerce site converts visitors into orders. The SaaS site converts visitors into trials. The hospital marketing site converts visitors into appointments. Single function, single objective.
Treatment center websites do two jobs that pull in different directions.
The marketing job is the one most operators budget for. Drive inquiries from paid traffic. Convert organic search visitors. Support the family member who arrives via referral. Lower cost per admit. Reduce bounce rate. Optimize the form.
The clinical trust signal job is the one most operators do not budget for explicitly. Telegraph to the family member that this facility is serious enough to entrust someone’s life to.
Demonstrate clinical credentials. Show that the program is real, not a marketing front. Pass the YMYL evaluation that Google’s quality raters apply at a stricter threshold than they apply to almost any other category.
The two jobs overlap in some elements. A clean visual hierarchy serves both. Fast page load serves both. Mobile-responsive layout serves both. Clear navigation serves both.
The two jobs diverge in other elements. A marketing-optimized hero image of a smiling family on a beach might convert better than a clinical-credibility-optimized photo of the actual clinical director.
The marketing-optimized testimonial section might emphasize outcome promises that the clinical-credibility-optimized version would never make. The marketing-optimized form might ask for fewer fields than the clinical-credibility-optimized version needs for safe intake.
Sites that solve only the marketing job tend to convert well in the short term and erode credibility over time. Sites that solve only the clinical trust signal job tend to be credible but un-discoverable and difficult to convert. Sites that solve both jobs at once compound over years.
What a Family Member in Crisis Reads in the First 5 Seconds
The family member arriving at a treatment center website is rarely in the patient demographic. They are often a mother, father, sibling, or spouse who has just learned about an overdose, an arrest, a relapse, or a dangerous use pattern.
They are searching at 11 PM, in tears, on mobile, with a phone battery at 14 percent.
Their crisis-state cognition is making a fast trust decision based on signals that operate below conscious awareness. The signals are not the headline or the marketing copy. They are the visual gestalt: does this look like a real place with real people who know what they are doing?
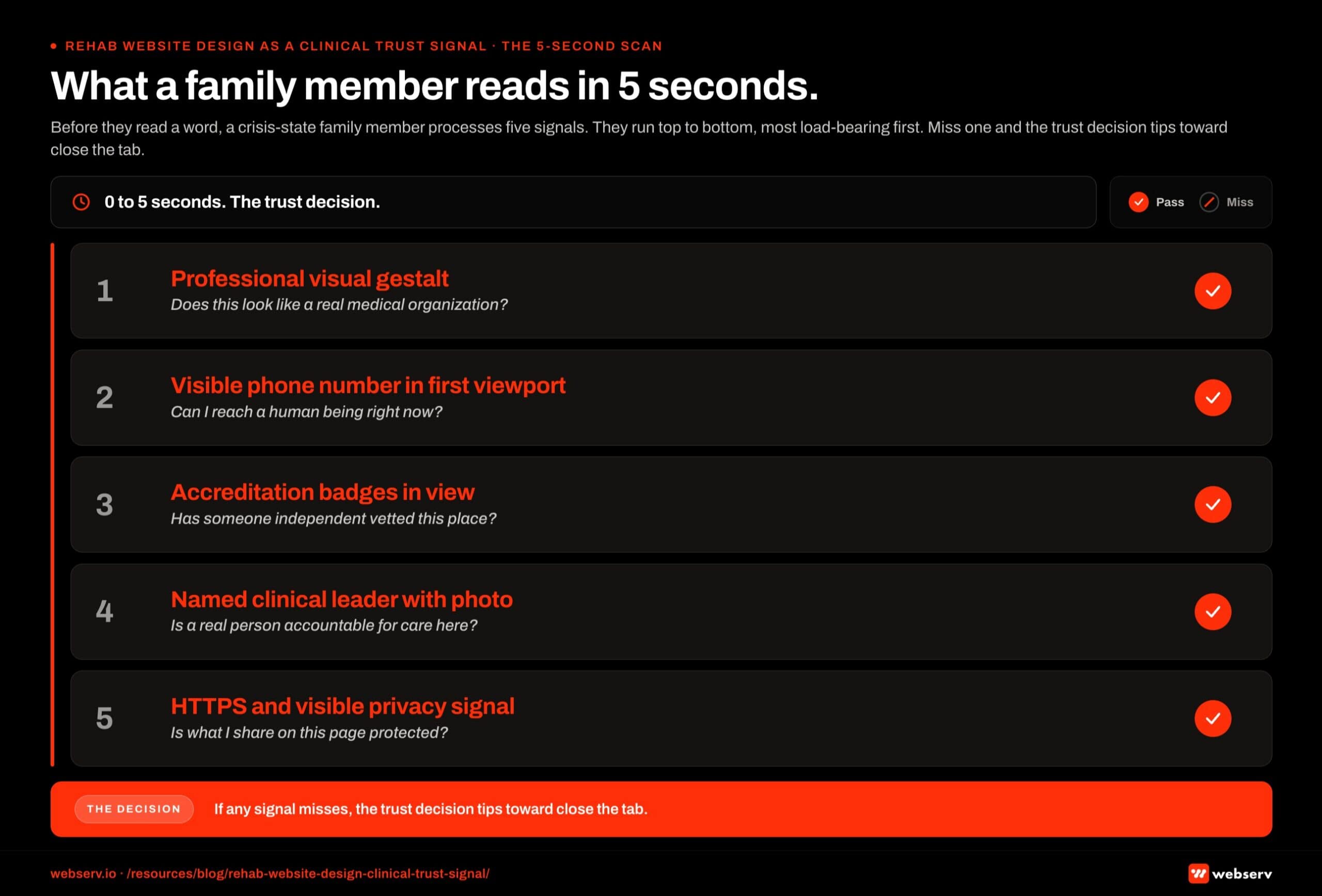 Vertical stacked hierarchy infographic titled ‘What a family member reads in 5 seconds.’ Five subconscious trust signals processed by a crisis-state family member in the first five seconds on a treatment center website. Ranked by impact: visual gestalt (overall design quality and professionalism), visible phone number in the header, accreditation badges in view above the fold, named clinical leader with credentials, and HTTPS encryption with a privacy-conscious header. Each row carries a pass-fail diagnostic icon so an operator can self-score their own homepage.
Vertical stacked hierarchy infographic titled ‘What a family member reads in 5 seconds.’ Five subconscious trust signals processed by a crisis-state family member in the first five seconds on a treatment center website. Ranked by impact: visual gestalt (overall design quality and professionalism), visible phone number in the header, accreditation badges in view above the fold, named clinical leader with credentials, and HTTPS encryption with a privacy-conscious header. Each row carries a pass-fail diagnostic icon so an operator can self-score their own homepage.Five-second signals that family members process whether they realize it or not:
Does the site look professional? Stock photos, generic templates, broken layouts, and outdated styling all telegraph “this is not a serious place.” The family member does not consciously think this; they just feel an instinct to close the tab.
Is there a phone number visible? Not buried in the footer. Not behind a “contact us” click. In the first viewport, large, with an immediate call-to-action posture.
Are credentials visible? Accreditation badges (JCAHO, CARF, LegitScript), state licensing references, ASAM alignment statements. The family member does not know what these are, but their presence signals “this place is recognized by authorities.”
Is a clinical leader named and pictured? A real human with real credentials, attached by name and headshot to the front-facing parts of the site. Anonymous treatment centers do not pass the trust test.
Does the site look secure? Browser security icon. HTTPS encryption. Visible privacy notice. Family members handling sensitive information about a loved one are exquisitely sensitive to “this place looks sketchy.”
If any of these five signals is missing or wrong, the trust decision tips toward “close the tab.”
Google’s Search Quality Rater Guidelines apply YMYL evaluation at a higher threshold to healthcare than to almost any other category, and the human family member is applying their own version of the same evaluation in the first five seconds.
The Design Elements That Telegraph Clinical Credibility
Eight specific design elements function as clinical trust signals in 2026. Most rehab websites get three or four of them right and miss the others.
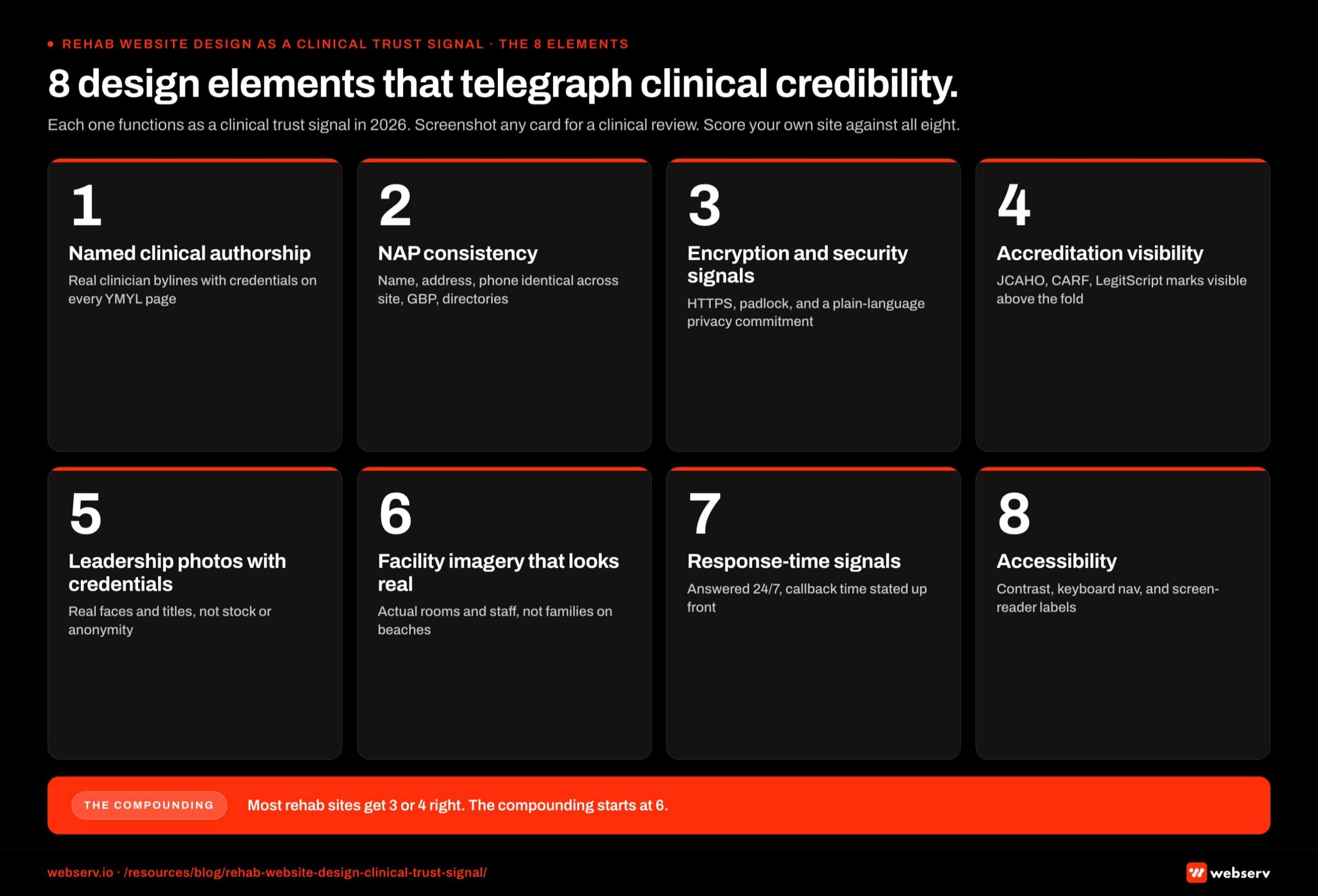 Numeric card grid infographic titled ‘8 design elements that telegraph clinical credibility.’ Eight numbered cards arranged in a 2 by 4 grid covering the design elements that function as clinical trust signals: named authorship with credentials, NAP consistency across the web, HTTPS encryption and privacy policy, accreditation badges (JCAHO, CARF, LegitScript), clinical leadership photos with real names, real facility imagery (not stock), visible response time and contact channels, and accessibility compliance. Footer band reads: ‘Most rehab sites get 3 or 4 right. The compounding starts at 6.’
Numeric card grid infographic titled ‘8 design elements that telegraph clinical credibility.’ Eight numbered cards arranged in a 2 by 4 grid covering the design elements that function as clinical trust signals: named authorship with credentials, NAP consistency across the web, HTTPS encryption and privacy policy, accreditation badges (JCAHO, CARF, LegitScript), clinical leadership photos with real names, real facility imagery (not stock), visible response time and contact channels, and accessibility compliance. Footer band reads: ‘Most rehab sites get 3 or 4 right. The compounding starts at 6.’Named clinical authorship. Every YMYL page on the site should have a named, credentialed author attached. The clinical director or chief medical officer should be the face of the facility’s clinical content, not “the editorial team” or a marketing director.
Per Google’s 2026 YMYL framework, authorship is the single highest-impact compliance signal for healthcare content, which is why clinicians function as the AEO moat for treatment centers.
NAP consistency. Name, address, phone number consistent across the site, Google Business Profile, SAMHSA Treatment Locator, state licensing records, LegitScript listing, and any directory listings.
NAP mismatches signal to Google quality raters and to AI search systems that the entity is not verifiable, and they undermine local SEO performance. Entity SEO work for treatment centers starts here.
Encryption and visible security signals. HTTPS everywhere. Visible privacy notice and HIPAA disclosure. Cookie consent banners that work properly. An unencrypted healthcare site in 2026 signals to Google that patient data is not handled with care, and signals to family members that this facility does not take privacy seriously.
Accreditation visibility. JCAHO, CARF, LegitScript, state licensing, ASAM alignment, SAMHSA listing. The badges and references should appear in the first viewport on every primary page, not buried in the footer or hidden in an about page. The family member needs to see them while the trust decision is still open.
Leadership team photos with credentials. Real photos of real people with their names, titles, and credentials visible. Clinical director, chief medical officer, executive director, founder. Anonymous teams or stock-photo “team members” actively undermine credibility.
Facility imagery that looks real. Photos of the actual facility, not stock interior shots. Real rooms, real common areas, real treatment spaces. The family member is trying to imagine their loved one in this physical place. Stock photos make that imagination harder, not easier.
Response-time signals. “Available 24/7,” “we will call you within 1 hour,” “live chat with admissions counselor” framed as commitments. Family members in crisis are time-pressured. Sites that signal response speed convert them at higher rates than sites that don’t.
Accessibility. WCAG-compliant color contrast, alt text on every image, keyboard navigation, screen reader compatibility. Beyond the legal compliance angle, accessible design signals that the facility cares about all patients and families, including those with disabilities. The signal compounds.
The Design Failures That Destroy Clinical Trust
COSTLIEST MISTAKE
Stock photos of smiling families on beaches, paired with outcome-promise testimonials. The family member in crisis reads the photo as “nobody at this facility looks like this” and the testimonial as marketing copy — the clinical trust signal collapses in the first five seconds. The testimonials also risk 42 CFR Part 2 exposure and trigger Meta and Google ad-review rejections. Swap to real facility photography and de-identified outcome data with named clinical review.
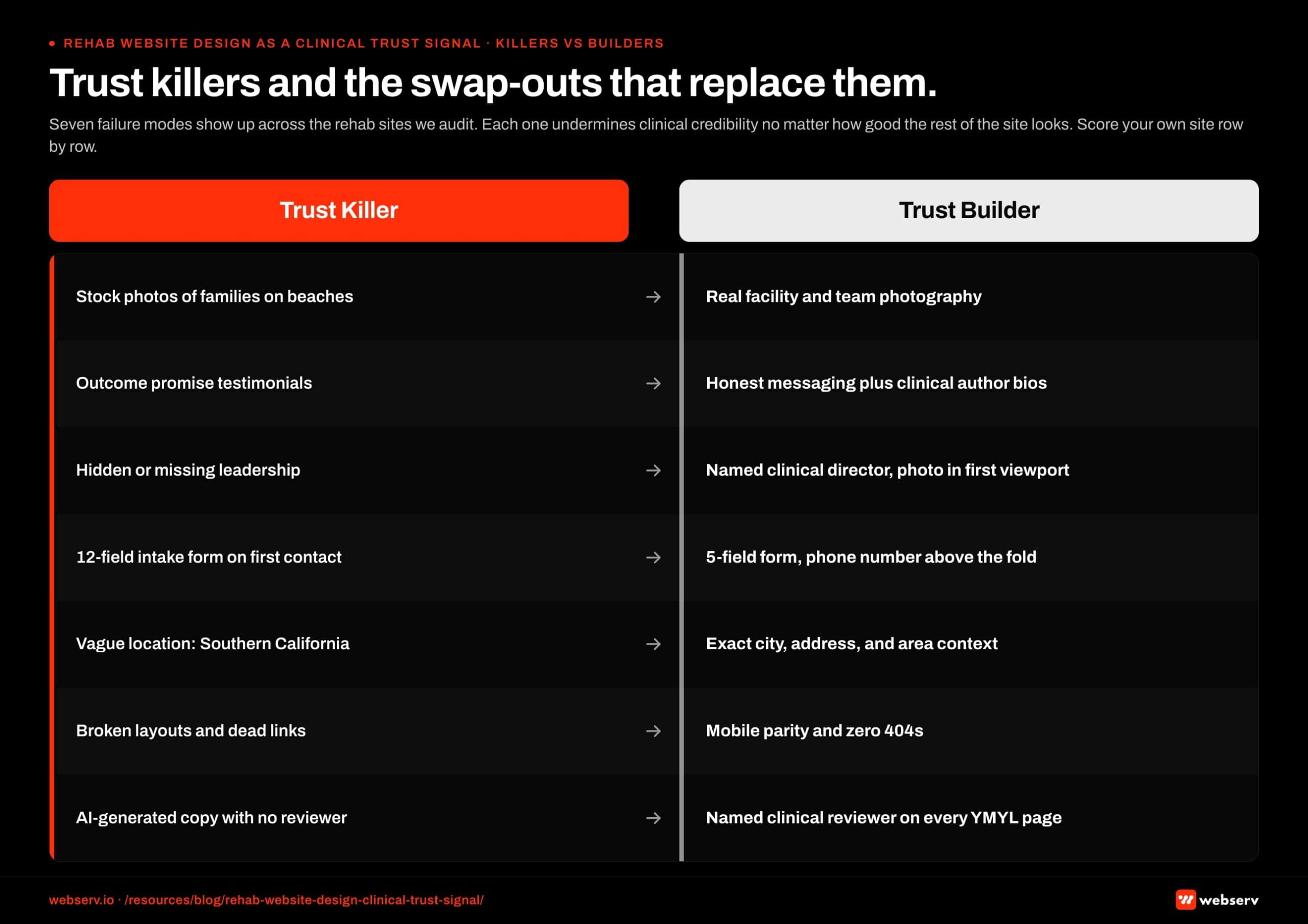 Two-column comparison infographic titled ‘Trust killers and swap-outs that replace them.’ Red Trust Killer column on the left vs black Trust Builder column on the right. Seven paired rows invert each failure mode into its operator-friendly swap-out: stock medical photos to real facility photography, generic ‘About Us’ text to named clinical leadership with credentials, Lorem-style placeholder testimonials to verified outcome stories, missing accreditation badges to JCAHO and CARF logos in view, hidden phone number to header-pinned phone number, outdated copyright year to current year with last-updated stamp, and mismatched NAP across pages to NAP consistency across every page and Google Business Profile.
Two-column comparison infographic titled ‘Trust killers and swap-outs that replace them.’ Red Trust Killer column on the left vs black Trust Builder column on the right. Seven paired rows invert each failure mode into its operator-friendly swap-out: stock medical photos to real facility photography, generic ‘About Us’ text to named clinical leadership with credentials, Lorem-style placeholder testimonials to verified outcome stories, missing accreditation badges to JCAHO and CARF logos in view, hidden phone number to header-pinned phone number, outdated copyright year to current year with last-updated stamp, and mismatched NAP across pages to NAP consistency across every page and Google Business Profile.Seven failure modes show up across the rehab websites we audit. Each one actively undermines clinical credibility regardless of how the rest of the site looks.
Failure 1: Stock photos of smiling families on beaches. The single most common rehab website design failure. The family member knows immediately that nobody at this facility looks like this. The implied promise is false. The trust signal collapses.
Failure 2: Outcome-promise testimonials. “I was an addict, now I have a life.” Visible patient testimonials with identifiable faces violate 42 CFR Part 2 confidentiality requirements.
They also trigger Meta and Google ad-review rejections, and signal to clinically-literate family members that this facility is willing to compromise patient privacy for marketing.
Failure 3: Missing or hidden leadership team. No clinical director named. No medical staff visible. No founder. A treatment center without visible leadership is a treatment center the family member assumes is hiding something. The trust signal collapses.
Failure 4: Long forms that suggest the facility does not understand crisis. Twelve-field intake forms on the primary contact page. Required fields for insurance details, demographics, and family history before the conversation has even started.
The family member in crisis bounces. Trimming intake forms from 12 fields to 5 produces 40 percent more inquiries, but the failure mode is not just conversion: the form length signals the facility does not understand the crisis context.
Failure 5: Vague or generic location information. “Located in beautiful Southern California.” “Serving the New England area.” Family members need to know exactly where the facility is, what city, what amenities the surrounding area provides, what the actual address is. Vague location signals that the facility is hiding something.
Failure 6: Outdated or broken design elements. Pages that render differently on mobile vs. desktop. Images that fail to load. Forms that submit nothing. Links to pages that don’t exist. Each broken element compounds the “this place is not serious” trust collapse.
Failure 7: AI-generated content with no clinical reviewer credit. Healthcare YMYL content in 2026 requires named clinical authorship and reviewer credit.
AI-generated medical copy with no human credentialed author is disqualifying per Google’s quality rater guidelines, and is increasingly recognizable to sophisticated family members who have been on enough treatment center websites to spot the pattern.
The treatment center website is the only marketing asset the operator owns that is also a clinical credibility statement. Every design decision either reinforces the clinical credibility or undermines it. The operators who hold the dual frame in their head while building the site produce websites that compound trust over years. The operators who treat design as a marketing exercise alone produce websites that convert in the short term and erode in the long term.
Preston Powell, CEO of Webserv
Who Owns the Design Brief
Most rehab website redesigns produce thrash because the design brief has a single author.
When marketing owns the brief alone, the site over-indexes on conversion mechanics and misses clinical credibility. When clinical owns the brief alone, the site looks like a peer-reviewed journal article and misses the family-decision psychology.
The right answer is co-authorship. The design brief should have two named owners: the marketing director (for conversion mechanics, paid traffic support, and brand voice) and the clinical director or chief medical officer (for clinical credibility, named authorship strategy, and the YMYL trust signal layer).
The co-authorship model has a specific workflow. Marketing drafts the brief from the conversion side. Clinical reviews and adds the trust-signal layer. The two leads jointly approve the final brief before it goes to the design and development team. Mid-project changes also require joint approval.
Operators who try to skip the clinical involvement to save time produce sites that need to be partially rebuilt within 18 months once the clinical credibility issues become visible. Operators who include clinical leadership from the start produce sites that compound credibility and conversion together.
For multi-facility operators, the clinical signoff should come from the clinical leader who actually appears on the site. If the chief medical officer is the named author and trust-signal anchor, the CMO should be in the design review meetings, not delegating to a junior clinical team member.
Frequently Asked Questions
How much does it cost to redesign a treatment center website with clinical credibility in mind?
Realistic budget ranges for a full treatment center website redesign run between $25,000 and $150,000 depending on facility count, content scope, and design complexity. Single-facility operators typically land in the $25,000 to $60,000 range. Multi-facility national operators typically run $80,000 to $150,000.
The clinical credibility layer adds 10 to 20 percent to the project cost relative to a pure marketing-focused redesign. The added cost comes from the clinical reviewer time, the content development for named clinical authors, and the additional design iteration to surface trust signals correctly.
That added cost is recovered within 6 to 12 months on a typical operator’s paid media budget through improved cost per admit. Operators who skip the clinical layer save the up-front cost and pay it back over 18 to 36 months in lower trust-driven conversion.
Should we use stock photos or custom photography on a rehab website?
Custom photography of the actual facility, the actual leadership team, and the actual physical environment beats stock photography on every dimension that matters for clinical credibility. The investment in a half-day photo shoot at the facility plus a half-day headshot session for leadership runs $2,000 to $8,000 and produces years of usable assets.
The exception is patient imagery. Real patient photos are prohibited by 42 CFR Part 2 confidentiality requirements and create both legal and clinical-credibility risk. For situations where you need a “patient” image, use clearly-labeled stock with diverse, non-identifying composition (back-of-head shots, distance shots, hands-only shots).
Avoid stock photos of smiling families on beaches, generic recovery imagery, and any “patient” stock that looks too polished. These actively undermine the trust signal the rest of the design is trying to build.
How do we evaluate whether our current website is functioning as a clinical trust signal?
Run a five-test audit. First, the eight-second test: have someone unfamiliar with the facility land on the homepage on mobile, and ask them within eight seconds whether they would trust this place with a family member’s life. Their gut answer is the signal. Second, the named-leader test: can a family member find the clinical director’s name and credentials within two clicks? If not, the trust signal is broken.
Third, the credentials test: are accreditation badges visible in the first viewport on the homepage and primary service pages? If they’re in the footer, family members are not seeing them. Fourth, the form test: how many fields does the primary contact form require? If it’s more than 7, the form is signaling that the facility does not understand the crisis-state user.
Fifth, the security test: does the URL show HTTPS? Is there a visible privacy notice? Does the site feel like it handles sensitive information appropriately? Sites that pass all five tests are functioning as clinical trust signals. Sites that miss any are leaving trust signals on the table.
Does design quality actually affect SEO rankings for behavioral health?
Yes, more so in 2026 than in any prior year. Google’s December 2025 Core Update produced sizable ranking changes on 67 percent of health-related websites, with E-E-A-T signals (Experience, Expertise, Authoritativeness, Trustworthiness) as the load-bearing differentiator. Design quality feeds directly into the E-E-A-T evaluation that Google’s quality raters apply to YMYL content.
The specific design elements Google’s raters evaluate include named clinical authorship visible on pages, accreditation references displayed prominently, NAP consistency across the site and across external listings, encryption status, accessibility compliance, and overall design quality as a proxy for operator seriousness.
Treatment centers that invest in design as a trust signal produce websites that perform better on both organic search and AI citation share over 12 to 24 months than treatment centers that treat design as a pure marketing exercise.
What’s the difference between a rehab website that converts well and one that builds clinical trust?
A high-converting rehab website optimizes for the form-fill or phone call. Short forms, prominent CTAs, urgent copy, conversion-focused hero sections. These elements can be done in ways that also build clinical trust, or in ways that undermine it.
A clinical-trust-building rehab website signals to the family member that the facility is serious, credentialed, and safe. Named clinical leadership, accreditation visibility, real facility imagery, encryption, clinical author bios, and outcome-honest messaging.
The right site does both. The form is short but the surrounding context tells the family member why this facility is the right call. The hero section converts but the imagery is real and the leadership is named. The intake CTA is prominent but the credentials are visible alongside it. Sites that prioritize one over the other produce predictable failures.
How often should a rehab website be redesigned to maintain clinical credibility?
Major redesigns every 4 to 6 years for most operators. The pace is driven less by design trends than by clinical leadership changes, accreditation updates, service line additions, and Google algorithm shifts that change what trust signals matter.
Minor refreshes every 12 to 18 months: leadership photos, clinical author updates, accreditation logo updates, new service page additions, design pattern adjustments based on conversion data. These maintenance refreshes preserve clinical credibility between major redesigns.
The operators who let their sites age 7+ years without major redesign typically see clinical credibility erode in measurable ways. Family-member trust decisions tip toward “close the tab” more often. Paid media costs climb. AI citation share stagnates. The compound effect of an aging site on a YMYL category is meaningful.
Build a Website That Does Both Jobs at Once
A treatment center website is the only marketing asset you own that is also a clinical credibility statement. Every design decision either reinforces the clinical credibility or undermines it.
The operators who hold both jobs in their head while building the site produce websites that compound trust and conversion together over years.
We build websites for treatment centers across the U.S. that are co-authored by marketing and clinical leadership, structured around the YMYL E-E-A-T framework, and designed to do both the marketing job and the clinical trust signal job at the same time.
Book an intro meeting to walk through your current website’s clinical credibility profile, where the trust signals are missing, and what a co-authored redesign would produce for your facility.
For the broader picture of how design fits inside a full treatment center marketing program, see our ultimate guide to behavioral health marketing and our rebuild vs. optimize framework for deciding whether your current site warrants a full rebuild.
Trevor Gage is the Director of Earned and Owned Media at Webserv, where he leads SEO, AEO, and digital PR for behavioral health and addiction treatment centers across the U.S. He writes about the cross-platform visibility work that earns treatment centers citation share in AI search alongside organic rankings and earned media coverage.