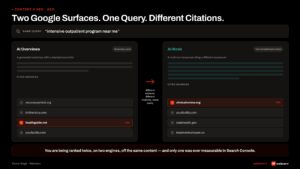
I have been on the same call ten times in the last six months. A treatment center operator opens the conversation with a number. Medicaid is now paying them $260 a day. Or $310. Or $440. Whatever the number is, it is below their operating cost.
They have already done the math on what closes the gap. They need to fill commercial beds, and they need to do it without sacrificing the Medicaid census that is keeping the lights on while the pivot lands.
The marketing implications of that pivot are larger than most operators expect. A commercial admit and a Medicaid admit are functionally different products. The keyword targeting is different. The geographic distribution is different. The creative is different. The admissions intake conversation is different. The reporting architecture needs to be different. This is the operator-facing playbook we walk through across 200+ engagements inside our paid media program for treatment centers.
This article walks the pivot from the operator’s seat, drawing on the paid media and admissions operations work we have run across 200+ treatment center engagements.
If you are reading this with one eye on your monthly P&L and the other on your reimbursement spreadsheet, you are the audience we wrote it for.
The Reimbursement Reality
Key Takeaways
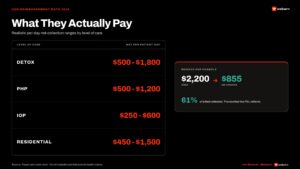
- State Medicaid reimbursement rates for residential addiction treatment have fallen to $250 to $500 per day in many states, below the operating cost of most facilities. The variance across states is large but the direction is consistent. Treatment centers heavily dependent on Medicaid census are pivoting toward commercial payers as a survival strategy.
- A commercial admit and a Medicaid admit are functionally different products from the marketing side. Different keywords, different geographic targeting, different creative messaging, different admissions intake conversation, different reporting architecture. The marketing strategy that produced the Medicaid census is rarely the strategy that produces commercial admits.
- Most pivots fail in the runway gap. Operators who cut Medicaid marketing before commercial is producing watch census drop while the new pipeline ramps. The correct posture is two concurrent campaign tracks: Medicaid moves to maintenance budget, commercial gets built as a parallel program with its own creative, audiences, and intake handling.
- The pivot is a 12 to 18 month operational shift. The first 90 days are foundation work: contract audit, catchment mapping, account architecture, content rebuild, admissions retraining. The next 6 to 9 months are calibration and scale. Operators who try to compress to 90 days usually break the runway.
- What stays the same: the clinical program, the brand, the compliance frameworks. What changes: positioning, geography, intake handling, and reporting. Operators who pivot well preserve the brand voice and rebuild the marketing strategy around it. Operators who pivot poorly create two facilities and end up with operational drag instead of commercial admits.
The financial gap is the forcing function. State Medicaid programs that once reimbursed residential treatment at $700 to $900 per day have moved to rates that no longer cover the cost of running a facility.
The Medicaid and CHIP Payment and Access Commission (MACPAC) tracks state Medicaid policy on behavioral health services, and the variance across states is large. The Kaiser Family Foundation has separately documented widespread state Medicaid behavioral health coverage tightening.
Operators in states that cut rates aggressively are running the same math we keep hearing on intro calls.
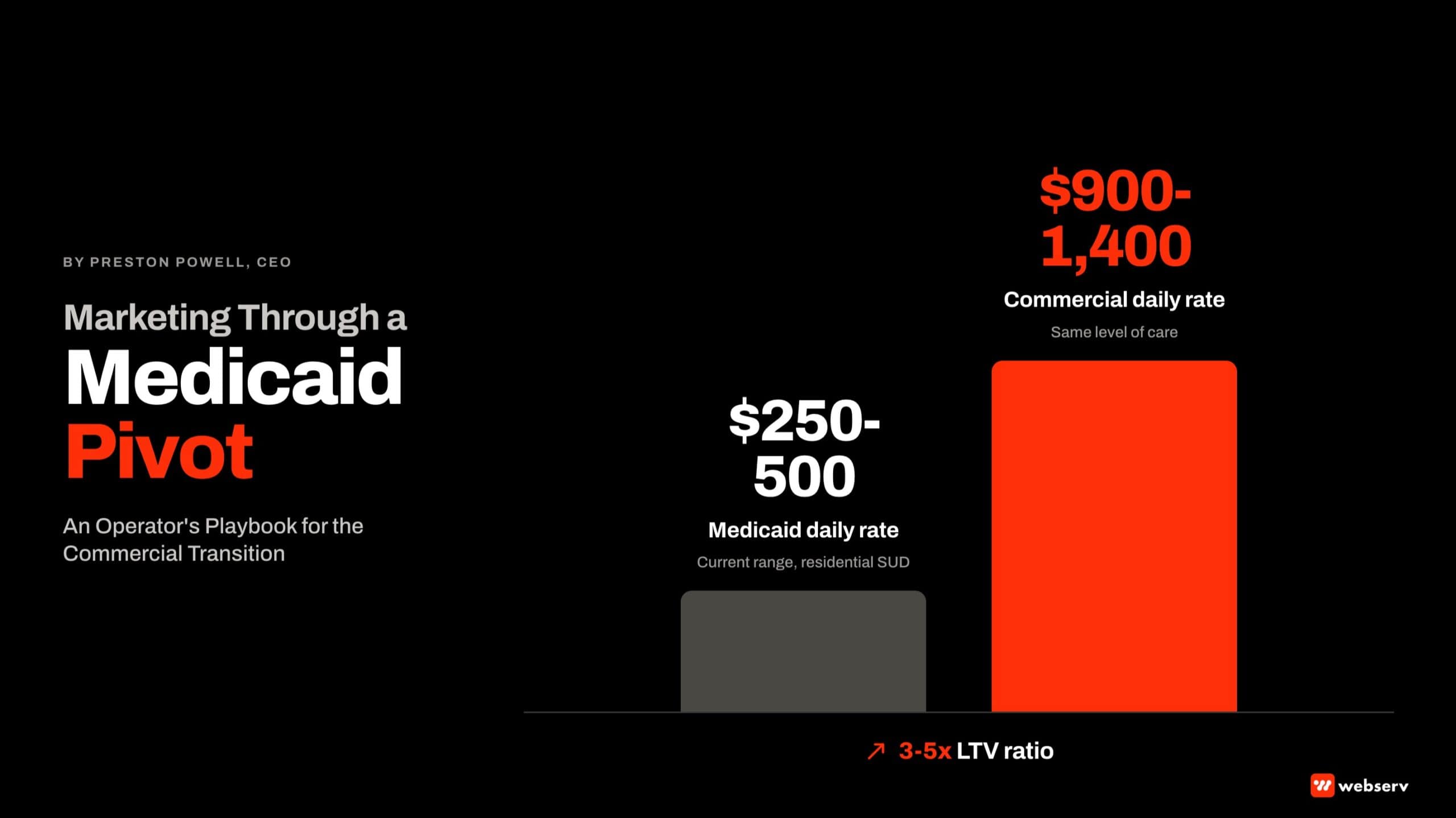
$250-500
Current Medicaid daily rate range for residential SUD
$900-1,400
Average commercial daily rate for the same level of care
3-5x
LTV ratio of a commercial admit to a Medicaid admit
The three options at this point are familiar to every operator. Option one: pivot the payer mix toward commercial insurance and accept that the marketing program has to be rebuilt.
Option two: narrow the level-of-care offering to the programs where Medicaid still pencils, typically outpatient and IOP. Option three: close beds or close the facility.
Most operators we talk to choose option one. They have a clinical program they believe in, a referral network they have built over years, and a team they want to keep employed. The pivot becomes the work.
The math is the easy part. Every operator has done the math. The hard part is the runway: how do you build commercial volume without sacrificing the Medicaid census paying for the facility while the new pipeline ramps.
Preston Powell, CEO of Webserv
The marketing strategy that produced the Medicaid census is rarely the strategy that produces commercial admits. The mistake most operators make is assuming it should be.
 Six things that change when a treatment center pivots from Medicaid to commercial. One, geographic targeting: commercial-insured prospects pull from a broader catchment that follows employer footprints, not the Medicaid enrollment zip codes. Two, keyword and audience targeting: commercial-intent search uses qualifying language like insurance verification, in-network providers, out-of-network benefits, and PPO coverage. Three, creative messaging: commercial prospects respond to in-network status with specific carriers, family-first messaging for adult dependents on employer plans, and clinical credentialing. Four, admissions team conversation: commercial intake requires rigorous benefits verification, in-network versus out-of-network conversations, and financial responsibility discussions. Five, reporting architecture: cost per VOB, viable VOB rate, and cost per admit reported separately by payer track. Six, compliance posture: LegitScript certification, 42 CFR Part 2 handling, and Meta family-first creative guidelines do not change between tracks; what changes is the paid media volume moving through certified accounts.
Six things that change when a treatment center pivots from Medicaid to commercial. One, geographic targeting: commercial-insured prospects pull from a broader catchment that follows employer footprints, not the Medicaid enrollment zip codes. Two, keyword and audience targeting: commercial-intent search uses qualifying language like insurance verification, in-network providers, out-of-network benefits, and PPO coverage. Three, creative messaging: commercial prospects respond to in-network status with specific carriers, family-first messaging for adult dependents on employer plans, and clinical credentialing. Four, admissions team conversation: commercial intake requires rigorous benefits verification, in-network versus out-of-network conversations, and financial responsibility discussions. Five, reporting architecture: cost per VOB, viable VOB rate, and cost per admit reported separately by payer track. Six, compliance posture: LegitScript certification, 42 CFR Part 2 handling, and Meta family-first creative guidelines do not change between tracks; what changes is the paid media volume moving through certified accounts.What Changes When You Pivot to Commercial
DEFINITION
Payer Mix
The distribution of admitted patients across payment sources (Medicaid, specific commercial carriers, self-pay). The composition of a treatment center’s payer mix determines its revenue per admit, its underwriting profile, and the marketing strategy that produces sustainable census. Webserv tracks payer mix as a primary marketing-strategy input.
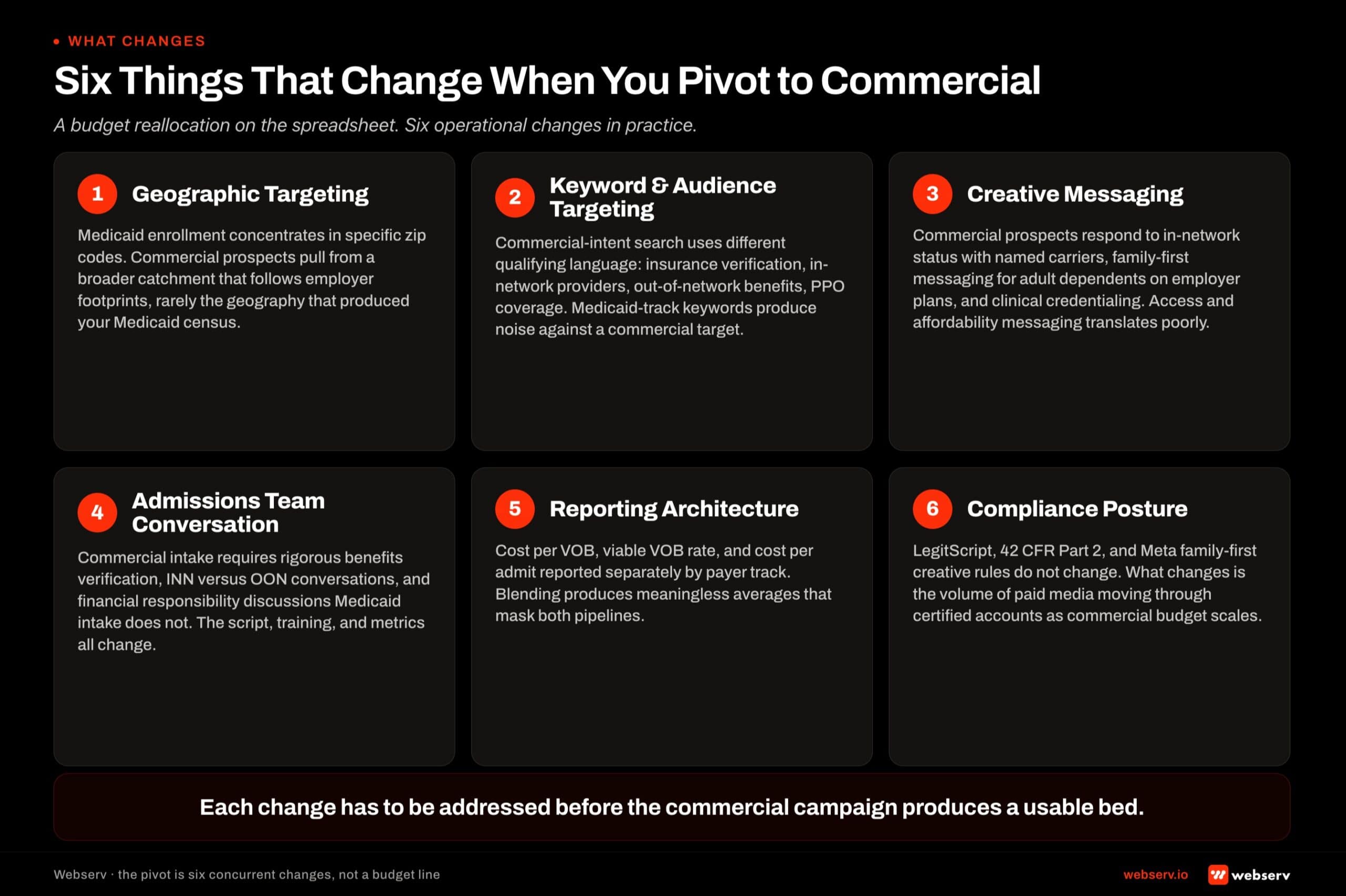
The pivot looks like a budget reallocation on a spreadsheet. In practice, six things change at the operational level, and each one has to be addressed before the commercial campaign produces a usable bed.
Geographic targeting. Commercial insurance flows differently than Medicaid. Medicaid enrollment is geographically concentrated in specific zip codes, while commercial-insured prospects pull from a broader catchment that follows employer footprints. The metropolitan area you pulled Medicaid census from is rarely the same area that produces commercial admits at the same volume.
Keyword and audience targeting. Commercial-intent search behavior includes different qualifying language. Searches that mention insurance verification, in-network providers, out-of-network benefits, and PPO coverage signal commercial intent.
Searches that mention Medicaid by name, sliding-scale fees, or specific state programs signal the opposite. The keyword and audience strategy that worked for Medicaid will produce noise against a commercial target.
Creative messaging. Commercial prospects respond to different proof points: in-network status with specific carriers, family-first messaging that addresses adult dependents covered under employer plans, clinical credentialing language, and verification confidence. Medicaid creative that worked on access and affordability frames does not move commercial prospects.
Admissions team conversation. The intake call is a different conversation. Commercial intake requires more rigorous benefits verification, payer-specific INN versus OON conversations, and financial responsibility discussions that Medicaid intake does not require. The script has to change. The training has to happen before commercial volume lands.
Reporting architecture. Cost per VOB, viable VOB rate, and cost per admit all need to be reported separately by payer track. Blending them produces meaningless averages.
The team needs to see commercial CPL trending up while Medicaid CPL stays flat, or the opposite, without one masking the other.
Compliance posture. LegitScript certification, 42 CFR Part 2 patient privacy handling, and Meta family-first creative guidelines do not change between Medicaid and commercial campaigns. The compliance baseline stays the same. What changes is the volume of paid media moving through certified accounts as commercial scales.
Don’t Tank Your Medicaid Census on the Way
RUNWAY RISK
The pivot fails most often when operators cut Medicaid marketing before commercial is producing. Medicaid census is paying for the facility while commercial ramps. Cut the Medicaid marketing too aggressively and the building empties before the new pipeline produces an admit. The right posture is two concurrent tracks with separate budgets.
The temptation in any pivot is to redirect all of the budget toward the new strategy and let the old one wind down. In a marketing pivot, this destroys the runway.
Medicaid census is paying for the facility while commercial ramps. Cut the Medicaid marketing too aggressively and the building empties before the new pipeline produces an admit.
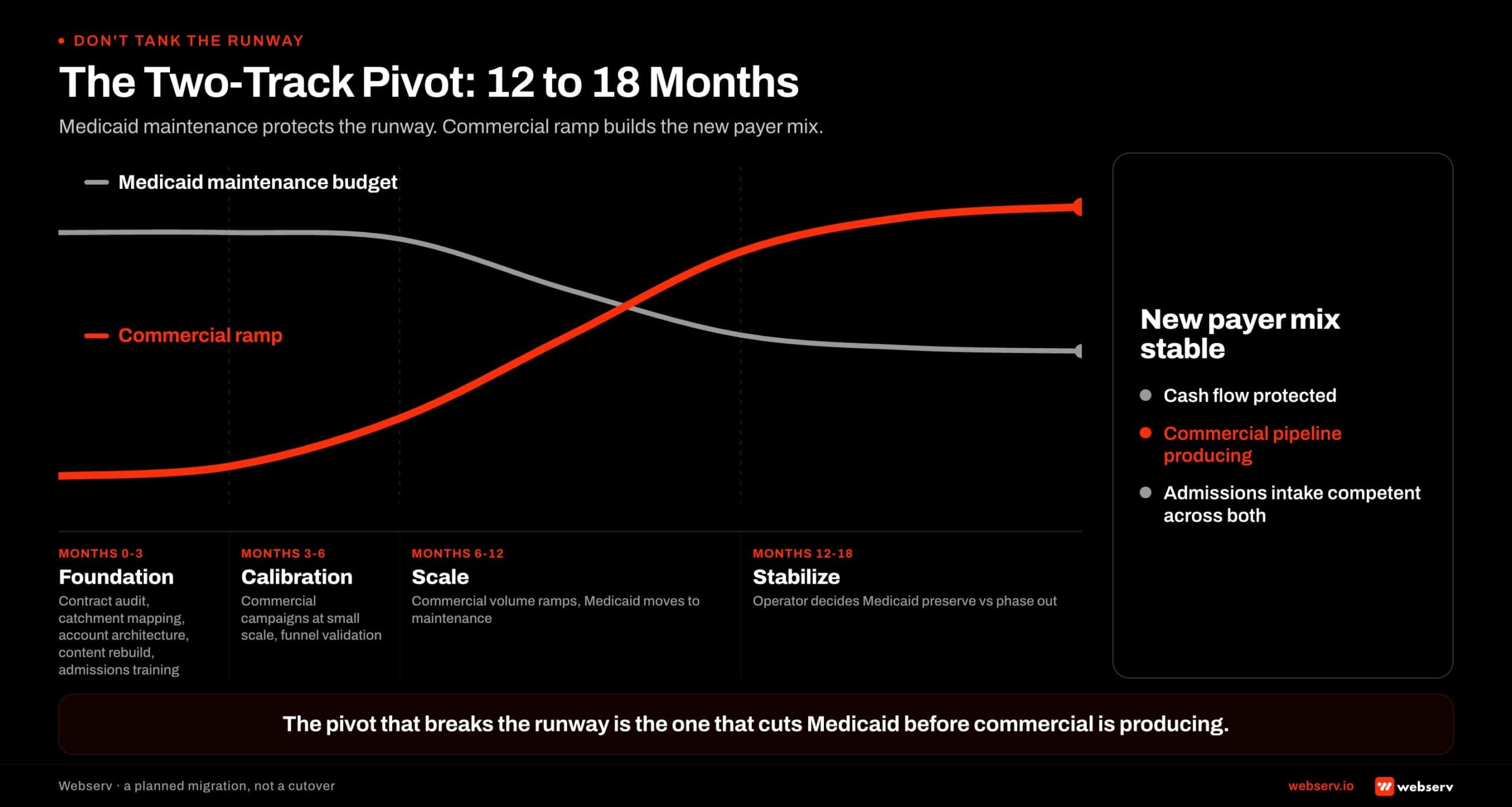 The two-track pivot timeline for treatment centers transitioning from Medicaid to commercial reimbursement. Phase one foundation runs months zero to three for contract audit, catchment mapping, account architecture, content rebuild, and admissions training. Phase two calibration runs months three to six for commercial campaigns at small scale and funnel validation. Phase three scale runs months six to twelve for commercial volume ramp while Medicaid moves to maintenance budget. Phase four stabilize runs months twelve to eighteen for the operator to decide how much Medicaid census to preserve versus phase out. The Medicaid track holds a maintenance budget through the full window while the commercial track ramps from near zero to target volume. The two tracks coexist concurrently rather than a hard cutover. The pivot that breaks the runway is the one that cuts Medicaid before commercial is producing.
The two-track pivot timeline for treatment centers transitioning from Medicaid to commercial reimbursement. Phase one foundation runs months zero to three for contract audit, catchment mapping, account architecture, content rebuild, and admissions training. Phase two calibration runs months three to six for commercial campaigns at small scale and funnel validation. Phase three scale runs months six to twelve for commercial volume ramp while Medicaid moves to maintenance budget. Phase four stabilize runs months twelve to eighteen for the operator to decide how much Medicaid census to preserve versus phase out. The Medicaid track holds a maintenance budget through the full window while the commercial track ramps from near zero to target volume. The two tracks coexist concurrently rather than a hard cutover. The pivot that breaks the runway is the one that cuts Medicaid before commercial is producing.The right posture is two concurrent tracks. The Medicaid track moves to a maintenance budget: enough to preserve referral relationships, sustain GBP and local visibility, and protect the assets that bring the existing census in.
The commercial track is built up as a separate parallel program with its own budget, its own creative, its own keywords, and its own admissions intake handling.
The runway lengthens substantially if you do this. The pivot stops being a race against a closing facility and becomes a planned migration. We have seen operators take eighteen months to fully complete the transition and end up healthier than the ones who tried to do it in six.
The Pivot Playbook
- Audit Current Payer Mix and Contracts. Pull your last 90 days of admits by payer. Pull your in-network and out-of-network contract list. Identify which commercial carriers you are actually credentialed with at which level. The contract reality determines what is possible downstream.
- Identify Commercial-Heavy Catchment. Map your INN commercial carriers to their geographic concentration. Pull employer footprint data where available. The geographic catchment of commercial-insured prospects is rarely the same as the Medicaid catchment and has to be mapped from real data, not from intuition.
- Restructure Paid Campaigns by Payer Intent. Separate the Medicaid track and the commercial track into different campaigns with different audiences, different keywords, different creative, and different conversion actions. Build the two tracks as parallel programs, not as one campaign with split budget.
- Rebuild Content for Commercial Verification Language. The treatment center’s pages need to address commercial intent: in-network status with named carriers, verification confidence language, clinical credentialing detail, family-first messaging for adult dependents covered under employer plans. Medicaid-era messaging on access and affordability does not move commercial prospects.
- Retrain Admissions on Commercial Intake. Commercial intake requires different verification, different payer conversations, and different financial responsibility discussions than Medicaid intake. The script has to change. The training has to happen before paid budget scales, not after.
The sequence matters. Step one cannot be skipped because the contract reality determines everything downstream.
We have watched operators launch commercial campaigns against carriers they were not actually credentialed with and burn three months of budget before catching it. The intake team verifies benefits, finds the operator is OON with no useful out-of-network rate, and the prospect drops.
Step two cannot be skipped because the wrong geography produces wrong-payer leads regardless of how well the campaign is targeted. The geographic catchment of commercial-insured prospects has to be mapped from real data, not from intuition about where the operator’s existing referrals come from.
Steps three through five are concurrent. The campaigns, the content, and the intake training have to land together or the early commercial admits get lost in the gap between marketing producing prospects and operations being ready to convert them.
What Stays the Same Across the Pivot
The pivot rewrites a lot of the marketing program. It does not rewrite the clinical program or the brand.
The clinical excellence, the staffing model, the family-first ethical posture, and the mission alignment that brought the facility into existence are the same across Medicaid and commercial admissions. The marketing strategy has to reflect this honestly rather than chasing whatever pays best.
Operators who pivot well preserve the brand voice. They do not become a different facility on the website to chase commercial prospects. The treatment is the same. The clinical credentialing is the same.
The compliance frameworks (LegitScript, 42 CFR Part 2, state licensing) are the same. What changes is how the program is positioned, where it is positioned, and how the intake conversation handles the payer dynamics.
Operators who pivot poorly look like two different facilities. They run separate websites, separate brands, sometimes separate phone numbers. This usually fails because the team operating both is the same team. The two-website pivot creates more operational drag than it produces commercial admits.
What Goes Wrong: Common Pivot Mistakes
DEFINITION
INN vs. OON
In-network versus out-of-network reimbursement status. Treatment centers carry different INN and OON contracts with different commercial payers. INN status produces predictable per-day rates at lower margins; OON status produces higher rates but with verification friction. The pivot to commercial requires the operator to know exactly which carriers they are credentialed with at which level.
The mistakes we see most often during pivots:
WHAT A WORKING PIVOT LOOKS LIKE
- Two concurrent tracks (Medicaid maintenance + commercial ramp) with separate budgets and reporting
- Geographic targeting aligned to the operator’s actual INN commercial carrier footprint
- Commercial creative built around in-network verification and family-first proof points
- Admissions team retrained on commercial intake before paid budget scales
- Reporting separated by payer track with cost per viable VOB tracked independently
WHAT A BROKEN PIVOT LOOKS LIKE
- One blended campaign targeting both populations, with averaged metrics that mask both pipelines
- Geographic targeting copied from the Medicaid campaign with budget reallocated
- Commercial creative recycled from Medicaid messaging on access and affordability
- Commercial campaigns launched with the existing Medicaid intake script in place
- One reporting dashboard blending both pipelines into a single CPL number
The blended-campaign mistake is the most common. Operators who try to save management overhead by running both populations against one campaign end up with metrics that look fine on the dashboard but produce neither pipeline at the volume needed.
The Medicaid lead rate masks the commercial conversion problem. The commercial admit rate masks the Medicaid pipeline drying up. Neither team can act on the data because the data is averaging two different products.
The recycled-creative mistake is the second most common. Commercial prospects do not respond to access and affordability messaging the way Medicaid prospects do.
The proof points that move commercial intake are clinical credentialing, in-network status with specific carriers, and the verification confidence that comes from a competent intake team. Creative that worked on the Medicaid track needs to be rebuilt for the commercial track from scratch.
How Webserv Approaches the Pivot
TIMING THE CUTOVER
Timing the cutover matters more than aggression on either side. The pivot we see succeed is the one that holds the Medicaid maintenance posture until commercial volume reaches predictable weekly cadence. Operators who try to time it on month boundaries usually time it wrong. The cutover should be triggered by the commercial pipeline crossing a volume threshold, not by the calendar.
Webserv’s pivot work for treatment center operators starts with the contract audit and the geographic catchment analysis, not with the marketing plan. The contract reality determines what is possible. The catchment determines where the budget should go. Both have to be settled before the campaigns are rebuilt.
We then build the two-track media architecture inside the operator’s own ad accounts: separate campaigns, separate audiences, separate creative, separate conversion actions.
The admissions operations workstream runs in parallel with the media build, because the intake team has to be ready before commercial volume lands. The reporting architecture separates the two pipelines from day one so the operator can see what each is doing in isolation.
The companion piece to this article, What Is Payer Mix and Why Does It Determine Your Treatment Center’s Revenue Strategy, walks the contract and credentialing side of the pivot in more detail. The payer mix piece is the foundation. This playbook is the operational sequence on top of it.
The pivot is hard work that produces a healthier facility on the other side. We have watched operators come out of it with a payer mix that the original P&L could not have produced, and with admissions teams that are better at intake across both populations than they were before.
The work is worth it. The sequencing is what determines whether the work lands. Book an intro meeting if you want to walk your pivot timing with us live.
Frequently Asked Questions
How long does a Medicaid-to-commercial pivot take to complete?
The full pivot typically takes 12 to 18 months from the decision point to the new payer mix being stable. The first 90 days are foundation work: contract audit, catchment mapping, account architecture, content rebuild, admissions training. The next 90 days are calibration: commercial campaigns running, intake working, reporting separated.
The 6-to-12 month window is where commercial volume scales while Medicaid moves to maintenance budget. The 12-to-18 month window is where the operator decides how much Medicaid census to preserve versus phase out, based on the new commercial volume.
Operators who try to compress the pivot into 90 days usually break the runway. The Medicaid census drops before commercial volume lands, and the facility’s cash flow takes a hit that creates pressure to make worse decisions downstream.
Can we keep running Medicaid and commercial as one campaign to save on management cost?
We strongly recommend against this. The two populations respond to different keywords, different creative, different geography, and different intake conversations. Running them as one campaign produces blended metrics that mask which pipeline is actually working.
The operational overhead of running two tracks is real but small relative to the budget being moved through them. The cost of running them blended is much larger: wasted spend, lost attribution, and an inability to course-correct because the dashboard cannot tell you which track is the problem.
If management overhead is the constraint, the answer is structuring the two tracks for parallel operation with shared reporting infrastructure, not collapsing them into one campaign. The reporting separation is the load-bearing part.
What should we cut from our Medicaid marketing during the pivot?
The right cut depends on what is producing the existing Medicaid census. Operators whose Medicaid census comes primarily from referral relationships, GBP visibility, and word-of-mouth can reduce paid spend on the Medicaid track substantially while preserving the local SEO and GBP investment that maintains those channels.
Operators whose Medicaid census comes primarily from paid search need to be more careful. The paid track has to stay on a maintenance budget until commercial volume is producing. Cutting paid Medicaid to zero before commercial ramps is the most common cause of pivot failure.
The audit on the front end of the pivot answers this question for the specific facility. Without the audit, the cuts are guesses, and the wrong cut drops Medicaid census faster than commercial ramps.
How do we know if our commercial campaigns are working before they produce admits?
The leading indicators land before admits. Cost per VOB and viable VOB rate are the two metrics to watch in the first 60 days of a commercial campaign. A commercial VOB rate above 45 percent and a cost per VOB inside the operator’s pre-modeled range signal that the campaign is producing the right prospects.
If the VOB rate is below 30 percent or the cost per VOB is double the model, the campaign needs targeting work before more budget moves into it. The admit number lags by 30 to 60 days because of the assessment-to-admit cycle.
Watching only the admit number for the first 90 days of a commercial campaign means flying blind. The viable VOB rate tells you whether the campaign is healthy long before the admit number does.
Preston Powell is the CEO at Webserv, a digital marketing agency for behavioral health and addiction treatment centers.