Most treatment centers I audit publish a blog article, hit the button, and watch the article die on the blog page. Traffic sits below 50 sessions in the first month.
The clinical director spent four hours on the reviewing. The writer spent 12 hours on the draft. Nobody sees any of it.
The problem is not the article. The article is usually fine. The problem is that the treatment center has confused publishing with distribution. Publishing takes the content live. Distribution takes the content to the audiences who are not sitting on the blog. That is the work we run inside our authority content program at Webserv.
Families do not read blogs. Referral sources do not read blogs. Alumni do not read blogs. What they do is scroll social, watch video, and check email.
Repurposing the article into email, social, and video surfaces is what turns one investment into eight or ten distinct engagements with different audiences. It is also where treatment centers most consistently underinvest.
This article walks the workflow we run for authority content engagements: the repurposing pyramid, the surface-by-surface mechanics, the 42 CFR Part 2 compliance considerations that shape what you can repurpose safely, and the cadence that produces compounding results.
Key Takeaways
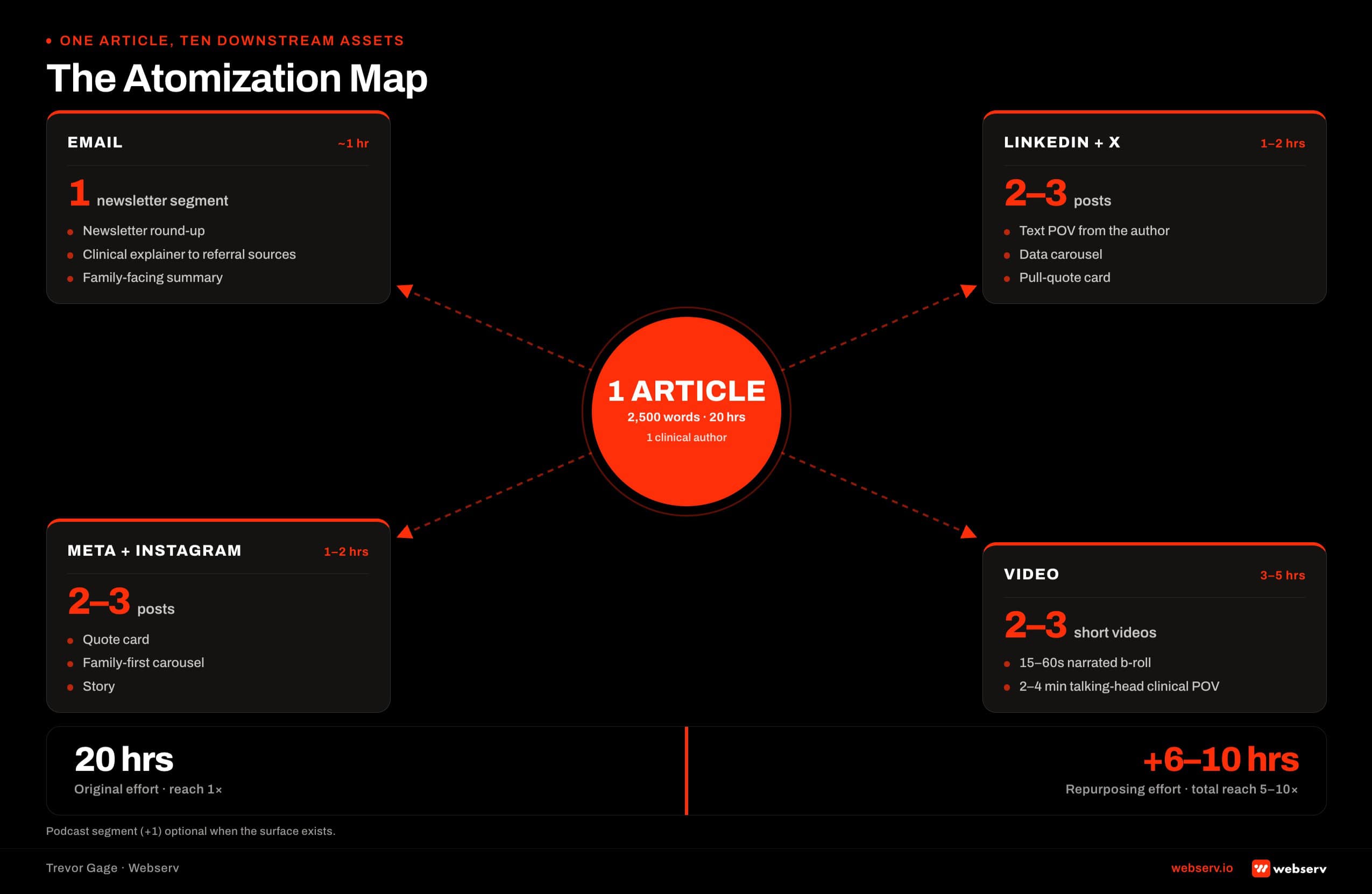
- One well-produced blog article can be repurposed into approximately one email newsletter, four to six social posts across LinkedIn and Meta, two to three short videos, and one podcast segment. The pyramid multiplies the return on the original content investment.
- The repurposing effort takes about 30 to 40 percent of the time the original article took to produce. Skipping the repurposing wastes 60 to 70 percent of the total content ROI available from every article you publish.
- Different surfaces reach different treatment center audiences. Email reaches referral sources, alumni (carefully), and prospects who opted in. LinkedIn reaches other operators, clinicians, and industry stakeholders. Meta and Instagram reach families and prospective patients. Video reaches the broadest audience but requires the most compliance discipline.
- 42 CFR Part 2 shapes what you can repurpose across each surface. Aggregate outcomes, clinical points of view, and operator perspectives translate cleanly. Individual patient stories require written authorization for every format they appear in, not just the original.
- The cadence that compounds is weekly or monthly consistent distribution. Quarterly bursts do not build the audience relationships that turn engagement into admits. Consistency matters more than volume.
- The measurement discipline that separates working programs from wasted ones is downstream tracking. Every repurposed piece should link back to the original article in a way that lets you measure which surfaces produced the traffic and conversions.
Why Repurposing Matters More for Treatment Centers Than for Most Categories
Behavioral health content is YMYL content at the highest tier. Google’s ranking systems, AI search assistants, and prospect trust all reward substantive content produced by named clinicians with real credentials. Google Search Central has documented the standard extensively in its Creating Helpful, Reliable, People-First Content guidance.
The cost of producing that substantive content is high. A well-researched blog article with named clinical authorship, verified citations, and E-E-A-T-appropriate structure typically requires 12 to 20 hours of writer time, 2 to 4 hours of clinical review, and legal or compliance sign-off where the content touches patient-adjacent topics.
That production cost is only worth carrying if the distribution captures the full audience reach available.
The distribution reality for treatment centers spans several audience segments that never converge on the blog. Families researching treatment options are on Instagram and TikTok. Referral sources (therapists, doctors, EAPs) are on email and LinkedIn.
Alumni networks live on email newsletters. Industry stakeholders and clinicians are on LinkedIn and podcast surfaces. AI assistants like ChatGPT and Perplexity ingest content from all of these surfaces, not just the original blog URL. Coverage across surfaces compounds the AI citation eligibility signal.
The Repurposing Pyramid
DEFINITION
The Repurposing Pyramid
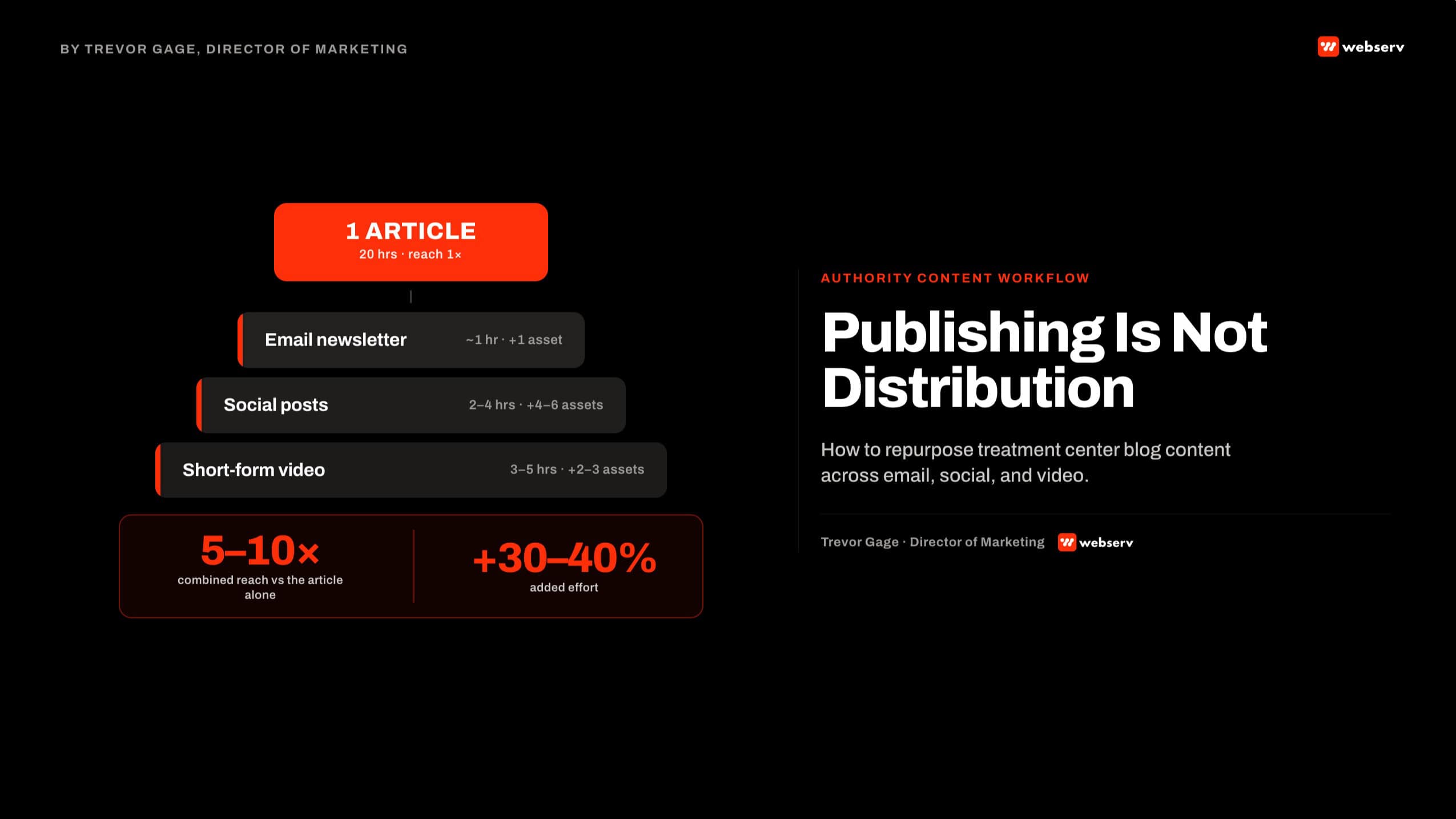
The framework for turning one long-form blog article into a cascade of shorter-form content across email, social, and video surfaces. The pyramid inverts effort against reach: the original article takes the most time to produce and reaches the smallest audience directly, while the repurposed pieces take a fraction of the effort each but collectively reach five to ten times the audience.
The math on repurposing is what makes it worth prioritizing. One 2,500-word article produced at 20 hours of total effort can generate:
1
email newsletter segment (~1 hour to produce from the source article)
4-6
social posts across LinkedIn, Meta, X (2-4 hours total)
2-3
short-form videos for social distribution (3-5 hours total)
The additional 6 to 10 hours of repurposing effort produces content that reaches 5 to 10 times the audience of the original blog article alone. The 30 to 40 percent additional effort captures 70 to 80 percent more total distribution.
The pyramid does not include podcast repurposing in the base cascade because most treatment centers do not have a podcast surface running. When they do, one long-form article generates roughly one podcast segment of 15 to 30 minutes with the clinical author or agency lead as the guest.
From Blog to Email
Email is the treatment center’s most direct channel to referral sources, alumni networks, and prospects who have opted in. It is also the most compliance-sensitive of the repurposing surfaces because alumni lists intersect directly with 42 CFR Part 2.
ALUMNI EMAIL LISTS ARE 42 CFR PART 2 TERRITORY
Any email list that includes patients who received substance use disorder treatment at your facility carries the same confidentiality protections as their clinical records. Sending to alumni without proper authorization can trigger disclosure violations. The safe rule: alumni lists require explicit opt-in with clear authorization language, kept separately from prospect and referral-source lists. Consult your compliance officer before any alumni email campaign uses treatment-related content.
The email formats that repurpose cleanly from blog content:
- Newsletter round-ups that summarize the article in 150 to 300 words with a clear link back to the full piece.
- Clinical explainer emails to referral sources that pull the clinical POV from the article and frame it for other clinicians.
- Family-focused summaries that translate the article’s substance into plain language for prospects and their families.
The formats that fail: generic “we published a new article” announcements with no substance beyond the headline. Referral sources delete these unread.
Segmentation for treatment center email lists is where most operators underinvest. The referral-source list, the alumni list (opt-in only, per compliance), and the prospect list all warrant different content. The same article can serve all three, but the framing, subject line, and call to action should differ.
From Blog to Social
Different platforms reach different treatment center audiences.
LinkedIn reaches other operators, clinicians, industry stakeholders, and investors. The content that lands here is clinical POV, operator perspective on industry issues, data-driven insight, and named-clinician commentary. LinkedIn’s audience does not respond to family-first creative or human-interest angles. It responds to substance, opinion, and industry-shaping stances.
Meta (Facebook and Instagram) reaches families and prospective patients. The content that lands here is family-first creative, hopeful clinical outcomes messaging, and visual assets. LegitScript certification and Meta’s restricted ad category compliance shape what you can advertise, but organic posts are less constrained than paid.
DEFINITION
Family-First Creative
Creative content designed for the family member seeking treatment for a loved one rather than the patient themselves. In behavioral health, roughly 60 to 80 percent of admissions inquiries come from family members, not the patient directly. Family-first creative emphasizes hope, credible outcomes, and clarity about the intake process. It avoids sensationalized recovery narratives, patient-in-crisis imagery, and language that reads as sales pitch. Meta’s ad platform enforces family-first standards for behavioral health advertisers, but the discipline applies equally to organic content.
SAMHSA has published extensively on the family’s role in treatment decision-making through its dedicated Families resource hub, which is a useful reference when the family-first creative direction needs a defensible framing to the clinical team.
TikTok requires the most compliance discipline. Behavioral health content on TikTok can reach large audiences quickly, but the platform’s algorithm surfaces content that generates strong engagement.
For treatment centers that often means dramatic or sensationalized posts that fail LegitScript compliance and Meta-family-first standards. Approach TikTok as a channel that requires purpose-built creative rather than repurposed blog content.
X (Twitter) reaches journalists, policy voices, and industry stakeholders. Repurposed blog content works here as short-form pull quotes with a link back to the original.
Reddit is engagement-only, not amplification. Repurposing blog content by cross-posting will get downvoted or removed. Reddit works for treatment centers only when the operator participates in relevant subreddits as a genuine contributor over time.
The social formats that repurpose cleanly from blog content:
- Carousel posts on LinkedIn or Instagram for data-heavy articles. Each slide covers one data point or takeaway from the article.
- Single-image quote cards for POV articles. Pull the strongest sentence from the article, display it against a branded background, link back in the caption.
- Text-only posts on LinkedIn for policy or operator-perspective articles. LinkedIn’s algorithm currently rewards text-only posts in some formats.
- Short video clips (15 to 60 seconds) for articles with a named clinician on-camera.
From Blog to Video
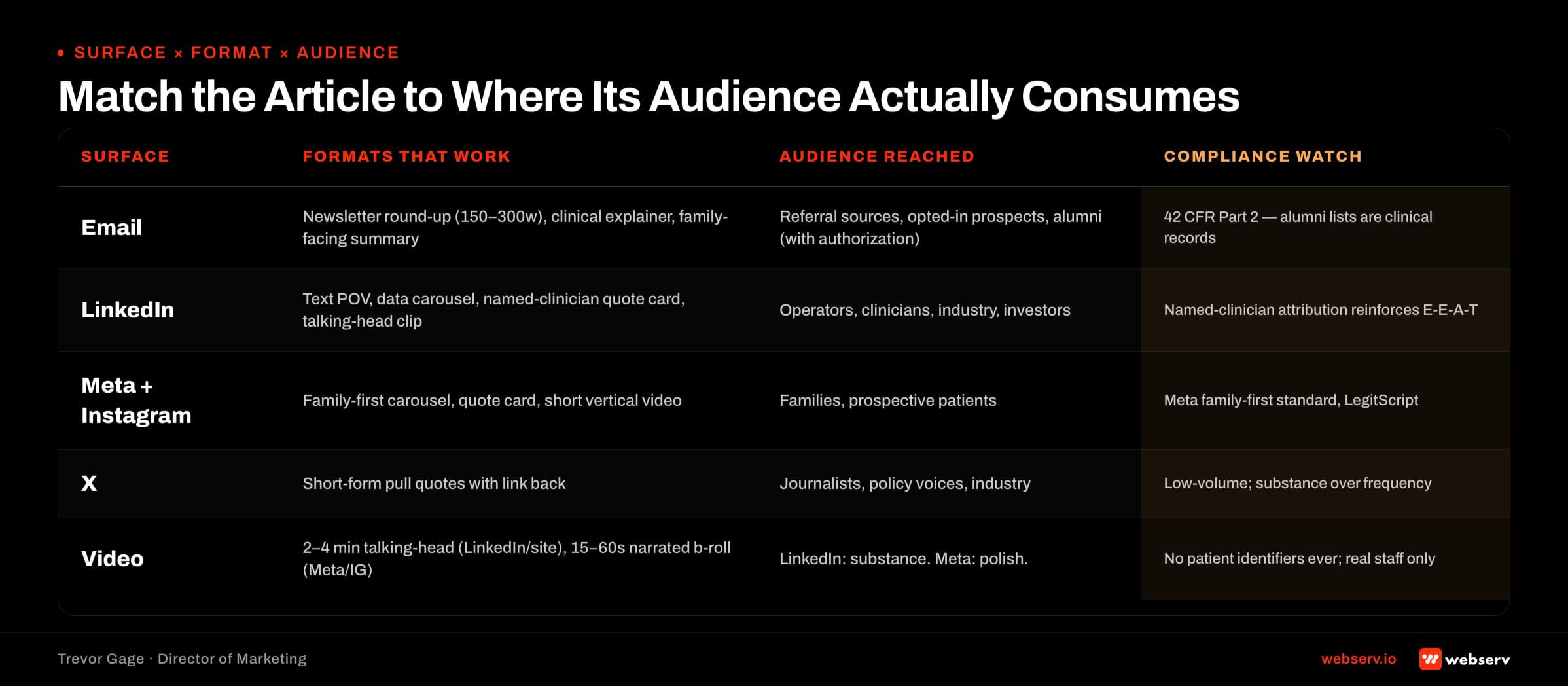
Video is the highest-reach repurposing format and the most production-heavy. The compliance considerations are also the tightest, because video creates identifiable staging that photos and text do not.
Two video categories work for treatment center content:
Talking-head clinical POV. The named clinician who authored or was quoted in the blog article records a 2- to 4-minute video summary of the article’s key argument.
This format performs well on LinkedIn, in email embeds, and on the treatment center’s website. It reinforces the E-E-A-T signal that Google and AI assistants read, because the named author of the article is visible saying the same thing.
B-roll narrated video for social. Shorter format (15 to 60 seconds) built for Meta and Instagram distribution. Voiceover narrates a key point from the article over generic b-roll (facility exteriors, staff at desks, campus scenes) with animated text callouts for the data points.
NAMED CLINICIAN ON CAMERA VERSUS ANIMATED VOICEOVER
The E-E-A-T value comes from having the named author or clinical expert visible on camera. The compliance value of animated voiceover is that it avoids any risk of accidentally showing patients in the background or in staged scenes. Most treatment centers should use both: talking-head video for the authoritative surface (LinkedIn, website), and animated voiceover for the higher-volume social distribution.
Video compliance considerations that matter across formats:
- No patient identifiers in the frame ever, regardless of consent. Patient consent for image use in marketing is legally complex and best avoided as a general policy.
- Staff on camera should be your actual staff, not stock actors. Stock imagery of clinical settings undermines the E-E-A-T signal.
- Facility exteriors, program spaces, and staff work areas are fine to film. Patient-occupied spaces are not.
- Voiceover script should be reviewed against 42 CFR Part 2 the same way blog content is reviewed. The medium changes, the compliance standard does not.
The 5-Step Repurposing Workflow
- Start With the Strongest Article. Not every article warrants repurposing. Focus on articles with named clinical authorship, substantive data, a clear point of view, or a story that resonates across audiences. Weak articles do not become strong repurposed content.
- Extract the Key Assets. Pull the strongest quote (for social cards), the strongest data point (for infographics or carousels), the clinical POV (for LinkedIn), the family-facing angle (for Meta), and the on-camera sound bite (for video). One article can yield 8 to 12 distinct repurposing assets.
- Reformat for Each Surface. Rewrite the key assets in the native language of each platform. LinkedIn opinion posts read differently than Instagram carousel copy. Email newsletter voice differs from social caption voice. Do not copy-paste across surfaces.
- Schedule With the Right Cadence. Distribute across 3 to 6 weeks, not all at once. Email newsletter first (usually within 7 days of the original article), then LinkedIn variants (week 1 to 3), then Meta and Instagram (week 2 to 4), then video (week 3 to 6). Cadence maintains momentum without oversaturating any single audience.
- Measure Downstream. Every repurposed piece links back to the original article with UTM parameters that let you segment traffic by surface. Weekly review of the source-attribution shows which surfaces produced the traffic and which produced the conversions. The measurement is what makes the process defensible over time.
The workflow above produces a repeatable process that a two-person content team can sustain at one to two articles per week. The bottleneck is usually not the original writing; it is the repurposing discipline.
Operators who skip the workflow and post articles to the blog without downstream distribution are leaving 60 to 70 percent of the content ROI unclaimed.
What to Repurpose (and What to Skip)
ARTICLE TYPES THAT REPURPOSE CLEANLY ACROSS SURFACES
- Data-driven articles → excellent for LinkedIn carousels and email newsletters
- Named-clinical-POV articles → excellent for LinkedIn text posts and talking-head video
- Family-focused educational articles → excellent for Meta, Instagram, and family newsletter
- Policy and industry POV → excellent for LinkedIn and X, referral-source email
- How-to and process explainers → excellent for video and email
WHERE THE SAME ARTICLE TYPES FALL SHORT
- Data-driven articles → weak for Meta/Instagram if the audience is family-facing
- Named-clinical-POV articles → weak for email newsletters to families (too clinical)
- Family-focused educational articles → weak for LinkedIn (audience mismatch)
- Policy and industry POV → weak for Meta, Instagram, and consumer video
- How-to and process explainers → weak for LinkedIn (too basic for the audience)
The pattern that emerges: match the article type to the surfaces where its audience actually consumes content. Do not force clinical POV articles onto Instagram or family-focused content onto LinkedIn. The mismatch produces low engagement and no downstream traffic.
The Digital PR side of the content marketing stack applies the same repurposing discipline. Our companion piece on Digital PR tactics for rehab centers walks the earned-media distribution layer that stacks on top of the owned-media distribution described here.
The Cadence Question
Consistency matters more than volume in content distribution. Treatment centers that publish and repurpose one article per week for 12 months build audience relationships that compound. Treatment centers that publish six articles in a single quarter and then go dark for two quarters do not.
The realistic cadence targets for a sustained content marketing program:
- Weekly newsletter to referral sources and prospects. One article per week feeds this cleanly.
- 3 to 5 social posts per week across LinkedIn, Meta, and Instagram. One article per week produces 4 to 6 posts across surfaces, which covers this budget.
- 1 to 2 short videos per week. One article per week yields 2 to 3 videos.
- 1 talking-head video per month. One article per month with a clinical author usually justifies this format.
Operators who cannot commit to weekly cadence should commit to monthly. One article per month with disciplined repurposing across surfaces beats four articles per quarter published in bursts.
What Success Looks Like
5-10x
reach multiplier from repurposed content over the original article alone
30-40%
additional effort required to repurpose one article across surfaces
6-12 mo
compounding window before repurposing produces measurable admit-side lift
The measurable outcomes of a well-run repurposing program show up across multiple channels. Referral-source email engagement lifts within 60 to 90 days as recipients begin recognizing the treatment center’s voice on their preferred surface.
Social reach compounds over 3 to 6 months as the platforms’ algorithms learn to distribute the content to relevant audiences. Video content builds slowly but produces the longest-tail effects, with individual videos continuing to accumulate views for 12 to 24 months.
The admit-side lift shows up latest, usually 6 to 12 months in. Repurposed content is a top-of-funnel and middle-of-funnel investment. It builds the audience relationships that produce inbound inquiries.
The specific attribution back to admits is harder than for paid media, but the compound effect on organic and referral admit volume is real over the 12- to 24-month window. Book an intro meeting if you want to walk your current content distribution with our team.
Frequently Asked Questions
How much staff time does a repurposing program require?
A sustained program producing one article per week with full repurposing across email, social, and video typically requires 15 to 25 hours per week of staff time. That includes writing (10 to 14 hours), design and social production (3 to 5 hours), video production (2 to 4 hours), and scheduling and measurement (1 to 2 hours).
A slower cadence (one article every two weeks) scales down proportionally. Operators without in-house content staff can outsource the entire workflow at $8,000 to $18,000 per month depending on scope and volume.
The cost is real but pays back durably. Content compounds over 12 to 24 months in ways that paid media does not. Treatment centers that sustain content distribution for two years typically end that period with substantially lower cost per admit than they started with, driven by improved organic and referral pipeline.
Do we need a dedicated video producer, or can we handle this in-house?
For talking-head clinical POV videos, in-house is fine if you have quality audio equipment (a lapel or shotgun microphone, not a laptop mic) and a well-lit space. The clinician does not need studio production; they need clean audio and clear framing.
Total production cost per video: $200 to $500 in equipment amortized across many videos, plus 30 to 60 minutes of clinical time.
For b-roll narrated video for social distribution, a dedicated video producer or an outsourced production partner produces materially better results than in-house. The narrative pacing, animated text, and audio design require craft that most in-house teams cannot match. Budget: $500 to $2,000 per finished video from an outsourced producer.
The distinction matters because the audiences are different. Talking-head video reaches LinkedIn and industry audiences that reward substance over polish. Social b-roll reaches Meta and Instagram audiences that reward polish over substance. Match the production level to the audience.
How do we handle repurposing when a clinical author leaves the organization?
Historical articles stay under the original author’s byline. Do not retroactively re-attribute; Google detects authorship shifts and the E-E-A-T signal degrades. When repurposing older articles across surfaces, the byline stays as originally published, but the treatment center voice on the repurposed asset can be attributed to the current team.
For example: an article from 2024 authored by a departed medical director stays under that byline on the blog. The LinkedIn post repurposing that article can reference “our clinical team” or “our leadership” as the voice on the current LinkedIn feed, with the blog article linked for the original authorship.
Video is the trickiest surface. Talking-head video with a departed clinician should typically not be re-promoted after their departure. Animated voiceover video repurposed from the article’s content can continue running, since the voiceover is not tied to a specific person.
What is the fastest single improvement we can make to our content distribution?
The email newsletter, if you do not already have one running. Most treatment centers publish blog articles and never send them to the referral sources and prospects who opted in to hear from them. Adding a weekly newsletter that summarizes the week’s article and links back typically produces the largest single lift in article visibility inside 60 days.
The setup cost is modest. A basic newsletter tool (Mailchimp, Klaviyo, Beehiiv) at $50 to $300 per month, list segmentation for referral sources and opted-in prospects (a few hours of setup), and a template that supports the newsletter format cleanly.
The lift is real because the audience is captive. Anyone who opted in to your list is a warm prospect or a referral source who has already indicated interest. Sending them the substantive content you are already producing is one of the highest-impact moves in a content marketing program.
Trevor Gage is the Director of Marketing at Webserv, a digital marketing agency for treatment centers.