
I took over a residential treatment center’s paid search account last year. The campaign had been built around a list of 47 zip codes the prior agency had labeled “high-value out-of-network targets.” Westchester County. Greenwich, Connecticut. Bel Air. Beverly Hills. Brentwood. Pacific Palisades.
The zips where wealthy families “obviously” live and where the agency had decided the facility’s ideal patient pool came from. Spend was $42,000 a month. The CPA on admissions was running $1,200.
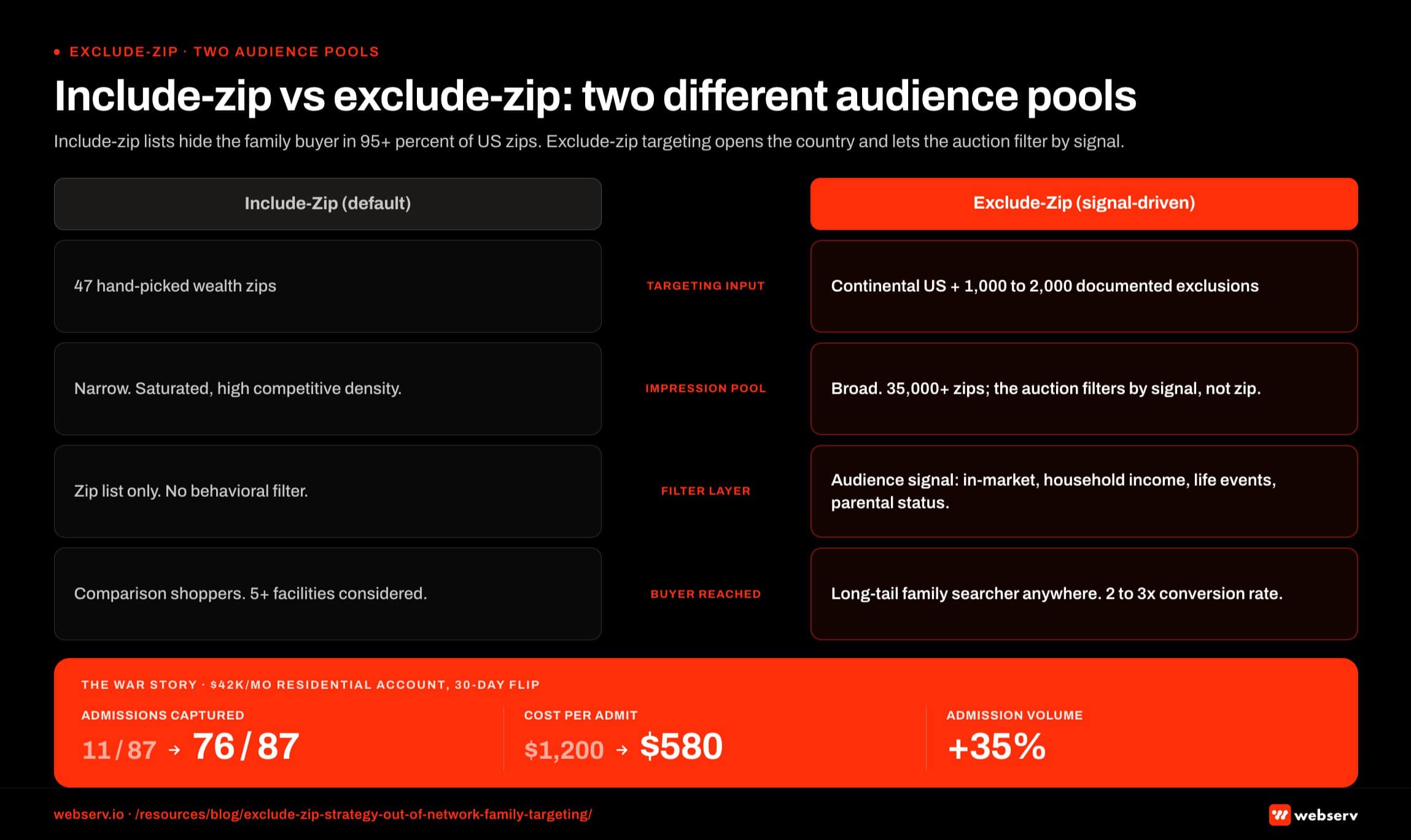
I pulled the prior 12 months of admissions data and matched the patient records against the family member’s actual home zip code. Of the 87 admissions the facility had taken in that period, 11 of them came from the 47 zips the campaign was targeting.
The other 76 came from zips like Cleveland, Akron, Sacramento, Albuquerque, St. Paul, Tucson, and 60 more that the campaign had been actively excluding. The agency had spent $504,000 the prior year chasing 13 percent of the addressable market and pretending the rest did not exist.
We rebuilt the account on an exclude-zip framework inside 30 days. The exclusion list had 1,200 zips on it. The inclusion was the entire continental United States. CPA dropped to $580 in the first 60 days. Admission volume grew 35 percent because the campaign finally reached the buyer pool the agency’s zip list had been hiding from it.
This is one of the most consistent mistakes I see in behavioral health paid search. Operators (and the agencies that serve them) assume they know where the high-value out-of-network family lives, build campaigns around that assumption, and miss most of the market. The fix is not better zip targeting. The fix is letting Google’s audience signals find the family while you exclude the few places you know are not worth your money. Our paid search practice runs every account on this framework from day one.
Key Takeaways
- Out-of-network families are not zip-clustered. High-net-worth families with rich PPO plans are statistically distributed across thousands of zip codes. Including a curated “wealthy zip” list excludes 70 to 90 percent of your addressable family market.
- The buyer in this category is often not the patient. Family members search from their own home zip, often in a different state, with a different demographic profile than the patient. Inclusion-based geo targeting has no way to know that.
- The exclude-zip strategy inverts the assumption. Run the campaign nationally (or across the largest geography you can serve). Exclude only the zips you have specific reasons to avoid: low historical conversion, documented body-broker fraud corridors, low-income zips with no realistic OON volume.
- The remaining 95+ percent of US zips become available to Google’s audience signal layer, which has more accurate household-income, life-event, and intent data than any zip list a media buyer can build manually.
- Patient brokering and body brokering corridors are still real. Targeted exclusion of known fraud zips is responsible, not contradictory to letting data find the buyer.
Why family targeting breaks the include-zip habit
The default playbook for paid search geo targeting was built for businesses where the buyer lives near the service. A dentist in Cleveland wants to reach people in Cleveland. A used-car lot in Tucson wants to reach people in Tucson. Inclusion targeting works for those businesses because the buyer’s geography matches the service’s geography.
Residential treatment centers do not work that way, and out-of-network admissions especially do not work that way.
The buyer for a 30-day residential treatment program in California is rarely the patient. The buyer is the patient’s parent, spouse, or adult child, and that family member is searching from their own home, which is statistically anywhere in the country. A mother in Boise looking for a residential program for her son is the same buyer profile as a father in Tampa looking for one for his daughter.
The geography of the family is independent of the geography of the facility, and it is independent of the geography of the patient.
Out-of-network economics make this gap more expensive. An OON admission in residential treatment typically runs $30,000 to $80,000 in collected revenue across a 25 to 40 day stay, compared to $8,000 to $18,000 in-network. The unit economics of OON admissions justify reaching the family member wherever they are, not just where a zip list says wealthy families “should” be.
The include-zip habit is built on three assumptions, all of which are wrong in this category. First, that high-net-worth families cluster in specific zips. They don’t. Second, that the facility’s local market is the relevant market. For residential, it isn’t. Third, that a media buyer building a zip list has better targeting data than Google’s audience signals. They don’t, and the gap has widened every year since 2020.
What the exclude-zip strategy actually does
The mechanic inverts the default. Instead of saying “show this ad to people in these zips,” you say “show this ad nationally, but exclude these specific zips for these specific reasons.” The remaining audience is everywhere else, and Google’s audience signal layer picks who gets served based on intent, demographics, and behavior.
Here is what makes it work.
Google’s signal layer is better than your zip list. Per Google Ads location targeting documentation, the system uses user setting, device, IP, search and behavioral signals to determine relevance. On top of that, audience signals like “in-market for healthcare,” household income deciles, life events, parental status, and search history feed into the auction.
A wealthy household in Cleveland with a teenager who searched “how to help a relative with addiction” three times in the last week is a stronger signal than any of the 47 zips on the original Westchester list.
Negative signal beats positive signal at scale. When you tell the system “do not serve here,” the system honors it absolutely. When you tell the system “serve only here,” you are excluding the long-tail signal that produces most of the conversions. Negative geo targeting is permission to let everything else through, which lets the algorithm work the way it is designed to work.
The remaining pool is larger and qualifies through behavior, not assumption. Excluding 1,200 to 1,500 specific zips leaves you with 35,000+ remaining US zips. Google’s auction layer decides which of those 35,000 actually gets impressions based on who is searching, what they are searching, what intent and demographic signals they carry. That is a better filter than any zip list you can build by hand.
What to exclude (and why)
The exclude list is not arbitrary. It comes from three specific sources, and any zip on the list should have a documented reason for being there.
Source 1: Your own historical conversion data. Pull 18 months of conversion data from your account. Bucket the conversions by family-member zip (not facility zip). Any zip that produced 8+ impressions and zero conversions over that window goes on the exclude list. This is your account’s empirical “no-go” set, and it is more accurate than any third-party data.
Source 2: Documented body-broker and patient-brokering corridors. Per New York OASAS guidance on patient brokering, federal and state authorities have prosecuted brokering rings in specific geographic clusters. The Florida coastal corridor from Delray Beach through Boca to Boynton is the most documented. The southern California “rehab row” through Newport Beach and Costa Mesa. Parts of Las Vegas, parts of Texas.
These corridors have higher fraud risk per impression because the local operator economics favor body-broker behavior, and ads served there compete with brokers paying $500 to $5,000 per referral. Your CPA does not survive that auction. Exclude the corridors. The body-brokering competitive dynamic is a separate problem worth its own treatment.
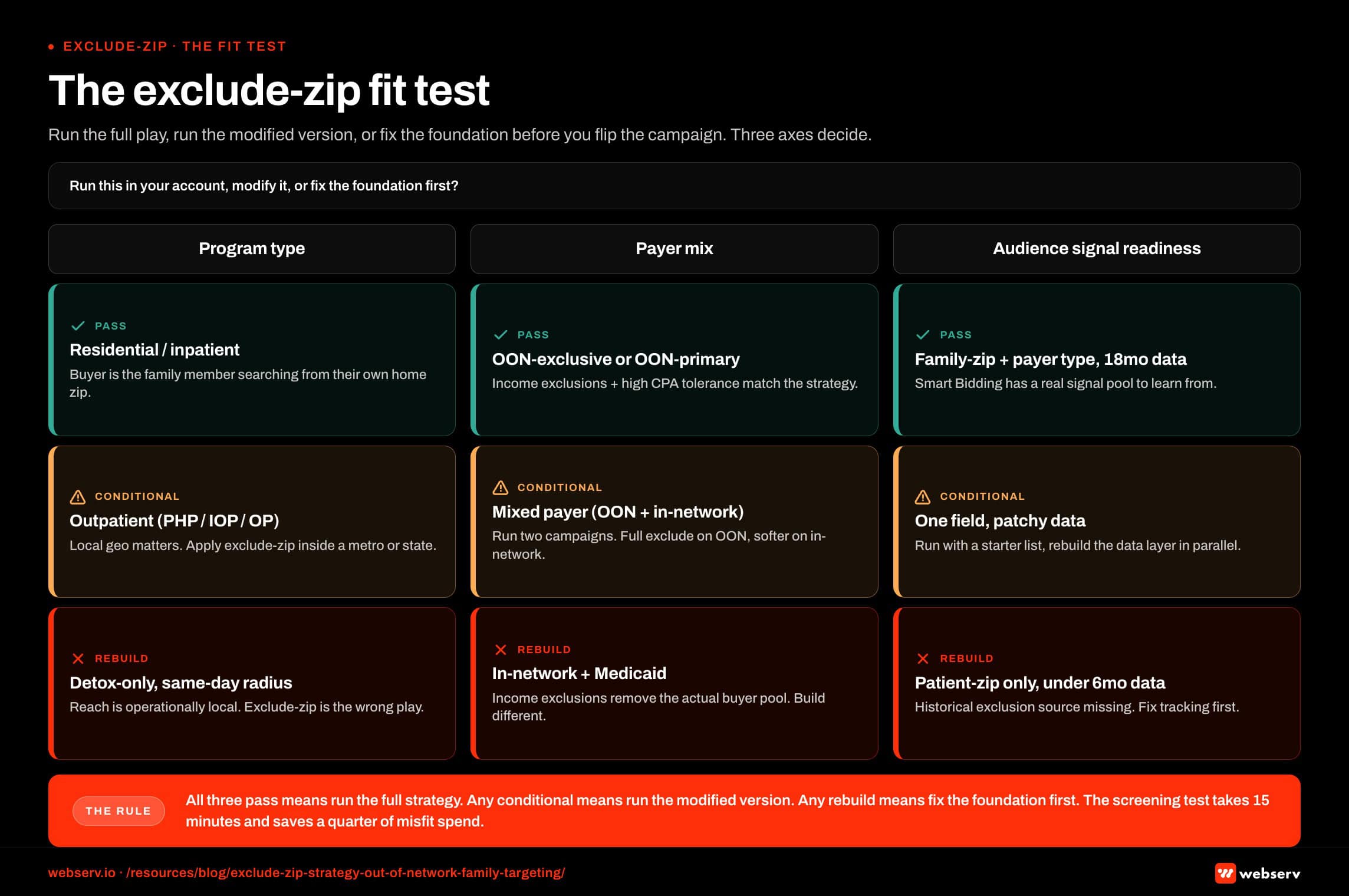
Source 3: Documented low-OON zips. Census-tract median household income under $35,000 with no documented PPO penetration is a poor signal for the OON family buyer. These zips will sometimes produce admissions, but those admissions will skew Medicaid or in-network low-margin, which is a different unit economics than the OON family this strategy is built around. If your facility takes both, run two separate campaigns with different geo settings. If your facility is exclusively OON or primarily OON, the low-income zip exclusion is appropriate.
The exclusion list typically lands at 1,000 to 2,000 zips after applying all three sources. That is 3 to 5 percent of US zips excluded, with 95+ percent of the country available for the auction.
What the inclusion-targeting alternative actually costs
The math behind the include-zip mistake compounds across three layers.
Impression starvation. A campaign targeting 47 zips runs out of impression inventory in those zips fast, especially in competitive BH markets. The campaign either underspends (good for budget pacing, terrible for volume) or bids up beyond economics to win the limited inventory available. Either way, the impression-to-conversion funnel narrows below what the budget should support.
Adverse selection in the included zips. The zips most agencies pick (Bel Air, Greenwich, Pacific Palisades) are also the zips every other behavioral health competitor is targeting. The auction in those zips is saturated, the CPCs are elevated, and the actual buyers in those zips are sophisticated about the category. A family in Pacific Palisades typing “best residential treatment near me” is comparing five facilities before they call any of them, which collapses your effective close rate even on the impressions you do win.
The long-tail signal goes unused. A mother in Albuquerque searching “how to get my son into rehab” is a high-intent searcher whose conversion rate to admission is often 2 to 3 times higher than the comparison shopper in Pacific Palisades. The include-zip list cannot reach her because Albuquerque is not on the list. She becomes a competitor’s admission.
When I pull conversion data on accounts that ran the include-zip pattern for 12 months before I took them over, the consistent finding is that the actual paying admissions came from a long tail of unexpected zips, while the included “wealthy” zips produced impressions but few admissions. The cost per admission in the include-zip campaigns is almost always 2 to 4 times what it becomes once we flip the campaign to exclude-zip.
How Profound Treatment drove 31 admits and a 42% drop in cost per viable in one quarter
Broad match pivot, negative keyword management, and intake-level conversion tracking turned a fragmented paid strategy into a predictable admissions engine.
Read the case study →68 viable VOBs at $4,529 cost per viable
How to set this up in Google Ads (the actual mechanics)
The setup in Google Ads is straightforward, but the defaults work against you. Three configuration steps matter.
Set location targeting to the largest geography you can serve. For most residential treatment centers, this is “United States.” For outpatient programs, it is the metro or state where the facility operates plus the surrounding region. Set it broad, then exclude.
Configure advanced location options correctly. The default “Presence or interest” setting includes people who are physically present, regularly present, OR show interest in the targeted location. For OON family targeting, you want “Presence” (people physically in the targeted area). The interest setting muddies the signal and serves impressions to people researching the location without being in your market.
Build the exclusion list as a single bulk paste. Google Ads accepts bulk uploads of negative locations. Paste your 1,200+ exclude list as a single operation, not as 1,200 individual entries. The interface for this is under Locations → Excluded → Add → Bulk paste. After the exclusions are in, the audience signal layer does the work.
Layer in audience segments for “Healthcare → In-market for healthcare services,” household income tiers (top 10 percent and top 11-20 percent for OON economics), life events (“starting a new job” and “new homeowner” correlate with elevated PPO purchase decisions), and parental status. The combination of broad geography with audience signals is what reaches the long-tail family buyer your zip list was excluding.
For Paid Social, the equivalent pattern runs on Meta and X with their own audience-signal layers. The HIPAA-compliant Facebook ads setup governs what you can and cannot target by audience type, but the geography logic is the same: broad targeting plus thoughtful exclusion beats narrow zip-list inclusion.
“If your agency hands you a 47-zip target list and tells you those are your buyers, the agency is showing you their geography assumptions, not your customer data. The data is in your CRM. The list is hiding it from you.”
Preston Powell, Chief Executive Officer, Webserv
The pull quote is uncomfortable because it implies the agency built the wrong campaign. In most cases, that is exactly what happened. Agencies build include-zip campaigns because the campaign looks like SEO work to the client, not because the math supports it.
The 2026 wrinkle that makes this matter more
Two changes in 2026 made the exclude-zip strategy more important, not less.
The first is Google’s continuing investment in audience signal accuracy. The signal layer in 2026 is much better at identifying OON-eligible households than it was in 2022, but only if the campaign gives the signal layer room to work. Narrow geo targeting starves the algorithm of the signal pool it needs to identify the OON family buyer.
The second is the platform’s tightening of healthcare advertising compliance in ways that make zip-level micro-targeting more scrutinized. Zip-code targeting cannot be used for housing, employment, or credit ads in the US and Canada, and while behavioral health does not fall under those categories directly, the scrutiny on healthcare ad targeting has increased in parallel.
An exclude-only strategy carries less compliance surface area than an aggressive include-zip strategy that micro-targets specific high-net-worth neighborhoods, which can look like discriminatory targeting under emerging scrutiny.
The combination of those two pressures is that the exclude-zip strategy is now both more effective and lower-risk than the include-zip default. Neither change argues for narrower targeting. Both argue for broader targeting with thoughtful exclusion.
What this means for the rest of your account
The exclude-zip move is one specific tactical change, but it cascades into the rest of the campaign structure.
The ad-group structure should reflect family-searcher intent, not facility-local intent. Your ad group structure probably has groups built around “residential treatment in [city]” type queries. If 70 percent of your conversions come from out-of-state family searchers, those city-keyword ad groups are misaligned with your actual buyer. Reweight toward queries like “how to help my brother with addiction” and “find a residential program for adult child.”
Conversion tracking has to capture family-zip data. The default Google Ads conversion tracking captures the searcher’s location. Your CRM or call-tracking layer needs to capture the family member’s home zip on the intake form or in the post-call notes. Without that data, you cannot build the historical exclusion list in step 1 of the strategy. The Meta Conversions API setup on the Paid Social side has the same requirement.
Bidding strategy interacts with this. Smart Bidding (Max Conversions, Target CPA) works better with a larger geography because the algorithm has more signal pool to learn from. The Max Conversions vs Max Clicks decision for small budgets covers when each makes sense. Max Clicks works fine in this configuration too. The combination of exclude-zip plus the right bidding strategy is the lift.
The negative keyword discipline compounds with the geographic exclusion work. Both are filters that protect the budget from low-quality auction inventory. The broader behavioral health marketing program only compounds when the paid foundations are configured correctly.
Frequently Asked Questions
Are we wasting impressions if we run the campaign nationally?
No, because impressions are not the cost. Clicks are the cost, and clicks are gated by the auction. Running national geography with a thoughtful exclude list means the auction serves your ad to high-intent searchers anywhere in the country who match your audience signals. The auction will not show your ad to a low-income searcher in a non-relevant zip with no in-market signal, because that searcher loses the auction to lower-bidding advertisers competing for them.
The pattern when operators run this test is that total impressions go up (because the geography is larger) while wasted impressions stay flat (because the auction filters by signal, not by zip alone). The net is more qualified impressions per dollar, not more total impressions per dollar.
The CPC also tends to drop slightly because the campaign is no longer competing in the most saturated wealth zips against five other BH advertisers. The long tail of qualified searchers has lower competitive density, so the cost per click on those auctions is lower.
What if our facility is regional and we cannot accept patients from outside our state?
The strategy still works at a regional scale. For a state-licensed facility that can only admit residents of the home state plus a few neighboring ones (or that prefers not to advertise out-of-state for LegitScript compliance reasons), set the geography to the licensed region and apply the exclude list within that geography.
The same logic applies. Inside a state, the wealth zips most agencies pick are not where most of the OON family buyers live. Statewide targeting with thoughtful exclusion will outperform 12-zip targeting within the same state, every time.
The geography boundary is set by your operational reality (licensing, intake capacity, payer mix). The exclude logic operates inside whatever boundary your operations set.
What zips actually go on the exclusion list?
The list is account-specific because it draws from your conversion data. There is no universal “exclude these zips” list because each operator’s historical conversion footprint is different. What is universal is the methodology: 18 months of conversion data bucketed by family-zip, plus documented brokering corridors, plus low-OON zips by income proxy.
For a starting point, most accounts I work with end up excluding approximately 1,000 to 1,500 zips after the methodology runs through. The largest blocks are typically: South Florida coastal (200-300 zips), parts of LA/OC (100-200 zips), low-income census tracts across the South and Rust Belt (400-800 zips), and a long tail of low-converting individual zips from the account’s own data.
Build the list once with the methodology. Refresh quarterly as new conversion data accumulates. Drop zips off the list if 12 months pass with no signal that they should still be excluded.
Does this work for in-network admissions or only out-of-network?
The strategy is shaped around OON economics because that is where the family-buyer pattern is most pronounced and where the income-based exclusions are most defensible. For in-network programs, the family-buyer pattern still exists (the buyer is still the family member, not the patient), but the income-based exclusions matter less because lower-income family members can produce in-network admissions just as profitably.
For mixed-payer facilities, run two campaigns. One for OON-targeted family acquisition with the full exclude-zip strategy. One for in-network with a softer exclusion list (brokering corridors and low-converting zips only, no income-based exclusions).
The bidding strategies and CPA targets should also differ between the two campaigns because the per-admission economics differ. The conversion tracking layer needs to capture payer type on the lead so you can attribute correctly to the right campaign.
What about Meta and other paid social channels?
The same pattern applies on Meta, X (formerly Twitter), and the rest of the paid social stack. Build broad geography, apply audience signals, exclude specific known-bad geographies and adverse audience segments. The technical setup is different per platform but the strategic logic is the same.
Meta in particular has stronger audience-signal data on parental status, life events, and household composition than Google does for some segments. That data feeds the OON family identification work directly.
The compliance posture for HIPAA-compliant Facebook ads constrains some audience segments but does not block the geographic logic of exclude-only targeting.
What is the single highest-impact change to make first?
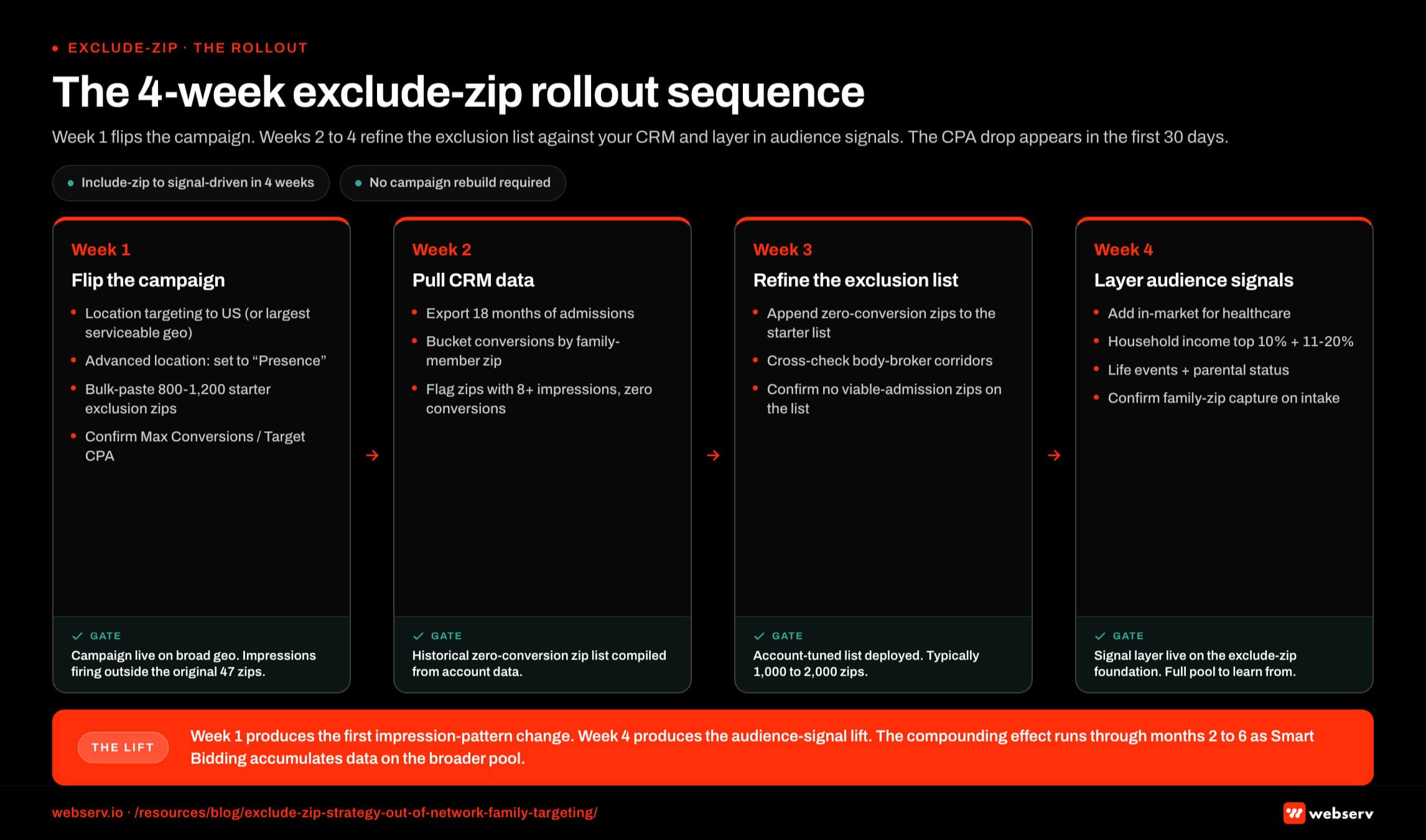
Flip the campaign from include-zip to exclude-zip targeting in week one. Geography setting to the largest serviceable region, location options set to Presence (not Presence-or-Interest), and a starter exclusion list of 800 to 1,200 known body-broker corridors plus low-income census tracts. The lift typically appears in the first 30 days as the algorithm starts reaching the long-tail family searcher pool.
The follow-up move in weeks 2 to 4 is to pull your CRM data, bucket past admissions by family-member zip (not patient zip, not facility zip), and add zips with 8+ impressions and zero conversions over 18 months to the exclusion list. This refines the exclusion list against your account’s actual signal, which is the strongest data source available.
The compounding lift through months 2 to 6 comes from layering audience signals (in-market for healthcare, household income tiers, parental status, life events) on top of the broad-geo exclude-zip foundation. The combination is what drops CPA into the range the unit economics support.
If you want a second opinion on whether your account is leaving OON family admissions on the table because of an include-zip configuration, request an account review and we can pull the historical conversion tracking data against your current targeting to size the gap.
The perspective in this article comes from 9 years working exclusively inside behavioral health.
We are a team built by people in recovery who understand that behind every admission is someone asking for help. If that resonates, get to know us.
Mitch Marowitz is Director of Paid Media at Webserv, where he leads Google Ads, Meta, and emerging paid channel strategy for behavioral health treatment centers. He has overseen more than $45M in managed media spend across the addiction treatment category and writes about paid acquisition for treatment operators.





