Most of the treatment center sites that lost traffic in the March 2026 Google algorithm update shared one common characteristic. Clinical content was being published without a real clinical review process.
The article draft would leave the writer’s hands, hit the CMS with minimal editorial oversight, and go live under an unnamed byline or a marketing manager’s name. Google’s ranking systems now weight this pattern heavily against the site.
The rebuild after an update like that is 6 to 12 months of content work, and it requires the exact workflow the site should have been running all along.
Rebuilding cheaply is possible only when the discipline is in place before the article gets written, not after the update penalizes its absence.
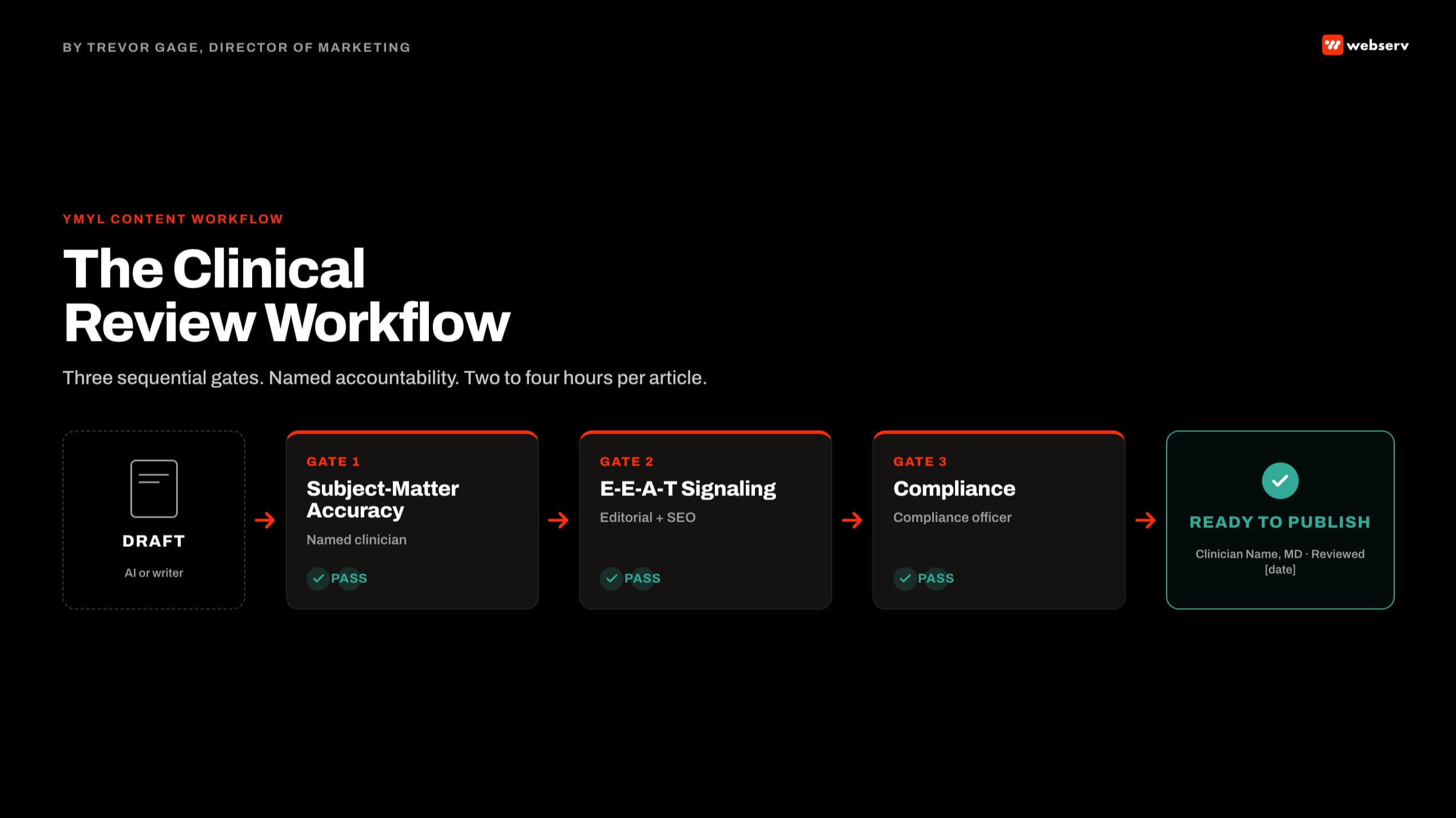
This article walks the clinical review workflow we run inside our authority content program at Webserv. It covers what YMYL actually means for behavioral health content, the three-stage review process every clinical article should pass through, who needs to be involved at each stage, and the realistic time investment required.
The goal is a workflow that adds 2 to 4 hours per article and pays back in ranking, AI citation, and defensibility across the 12- to 24-month content lifecycle.
Key Takeaways
- YMYL (Your Money Your Life) content standards apply strictest to healthcare content, and behavioral health sits at the highest tier of YMYL scrutiny. Every clinical article a treatment center publishes is evaluated by Google against author expertise, publisher authority, and content trustworthiness.
- The March 2026 Google algorithm update was particularly punishing on sites that used AI content production without editorial or clinical review. Treatment centers with unreviewed AI-heavy content lost traffic materially. Sites with disciplined clinical review workflows either held ground or gained share.
- A working clinical review workflow has three sequential stages: subject-matter accuracy (clinician verifies the claims), E-E-A-T signaling (named author, visible credentials, review timestamp, bio structure), and compliance review (42 CFR Part 2, LegitScript, FTC, HIPAA-adjacent claims). Skipping any stage produces a publishable article that will not compound.
- The total time investment is 2 to 4 hours per article across the three stages, on top of the original writing time. Treatment centers that skip the review add zero time to production and lose the ranking, citation, and defensibility that the review would have produced. The math is not close.
- Named clinical authorship is not a nice-to-have. It is a hard requirement for YMYL content at the current standard. The medical director, clinical director, or a credentialed clinician should be named on every clinical article, with verifiable credentials visible and a real bio.
- The most common failure pattern I see on audits is treatment centers where “the clinician reviewed the article” but no clinician is credited, no timestamp exists, and no bio is visible on the page. Google detects this pattern, and it produces the same signal as no review at all.
What YMYL Actually Means
DEFINITION
YMYL (Your Money Your Life)
Google’s category for content topics that could substantially impact a reader’s financial stability, health, safety, or wellbeing if the information is wrong. Healthcare content, including behavioral health and addiction treatment, sits at the highest YMYL tier. Google’s Search Quality Rater Guidelines direct evaluators to apply stricter standards to YMYL content on author expertise, publisher authority, and factual accuracy than they apply to non-YMYL content. Ranking systems then use those quality signals to inform which pages rank on YMYL queries.
Behavioral health is a category where the YMYL standards compound in three directions. The health-impact dimension is obvious: a family choosing a treatment center is making a decision that affects a loved one’s clinical outcome.
The financial dimension applies because treatment is expensive and the wrong facility choice has real financial consequences. The safety dimension applies because behavioral health conditions carry risk of harm when untreated or poorly treated.
The signal Google reads is a composite. Named author with real credentials. Author bio with verifiable background. Review timestamp indicating when a subject-matter expert last examined the content. Citations to authoritative sources.
Content depth commensurate with the query complexity. Publisher-level authority signals from other content on the site. AI assistants like ChatGPT, Claude, and Perplexity increasingly weight the same composite when deciding which sites to cite in their answers.
The Three-Stage Clinical Review Workflow
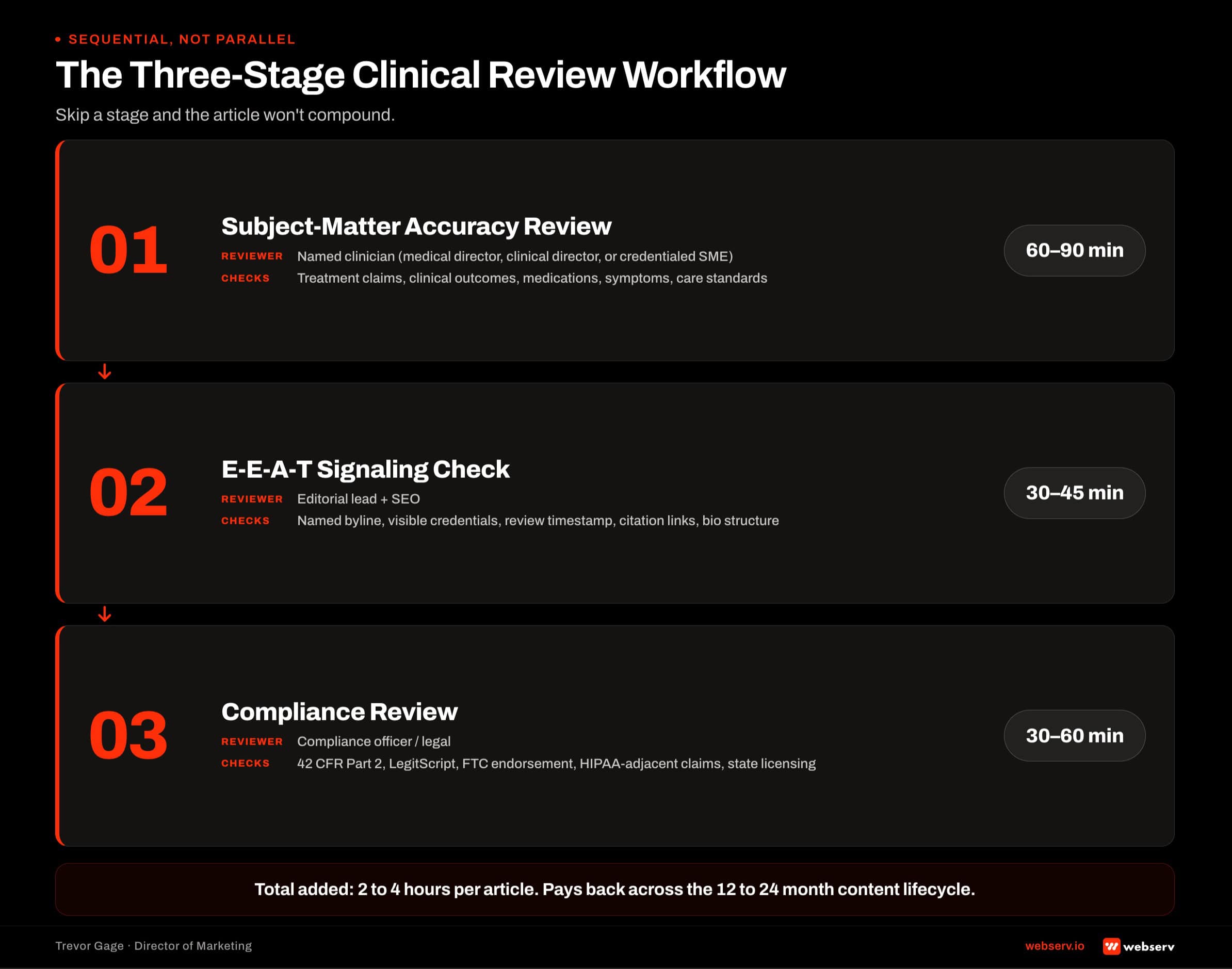
- Subject-Matter Accuracy Review. A named clinician (medical director, clinical director, or credentialed subject-matter expert) reviews the draft article for clinical accuracy. Every claim about treatment approaches, clinical outcomes, medications, symptoms, or care standards gets verified against current clinical understanding. Corrections happen at this stage before anything downstream runs. Time: 60-90 minutes for a typical 2,000-word article.
- E-E-A-T Signaling Check. The article’s byline, author bio, review timestamp, credentials display, citation formatting, and internal link structure all get audited against E-E-A-T standards. Every clinical claim links to a source. The author’s credentials are visible on the page. The review timestamp is current. Missing any of these elements is a failure of this stage. Time: 30-45 minutes.
- Compliance Review. The article goes through compliance review for 42 CFR Part 2 (SUD patient privacy), LegitScript standards, FTC endorsement guidelines, HIPAA-adjacent claims, and state licensing considerations. Any content that could create legal or regulatory exposure gets flagged for revision or removal. Time: 30-60 minutes.
The three stages are sequential, not parallel. Subject-matter accuracy has to pass before E-E-A-T signaling matters. An inaccurate article with perfect E-E-A-T markup is still an inaccurate article.
E-E-A-T has to be in place before compliance review, because the compliance officer needs to see the final structure the article will actually publish in.
Skipping any stage produces a publishable article that will not compound. Missing subject-matter review produces content that erodes trust when readers spot errors. Missing E-E-A-T signaling produces content Google cannot verify. Missing compliance review produces content that creates regulatory exposure or 42 CFR Part 2 disclosure risk.
Who Actually Needs to Be Involved
DEFINITION
The Clinical Reviewer
A named clinician with real credentials who takes editorial responsibility for the clinical accuracy of a specific article. Not “the marketing team consulted with a clinician.” A specific named person whose credentials are visible on the page and whose expertise is relevant to the article’s clinical topic. For a piece on medication-assisted treatment, the reviewer should be an addiction medicine specialist. For a piece on trauma-focused therapy, a licensed clinician with relevant training. The reviewer’s name and credentials appear either as author or as clearly credited “Medically Reviewed By.”
The people involved in a working workflow, by role:
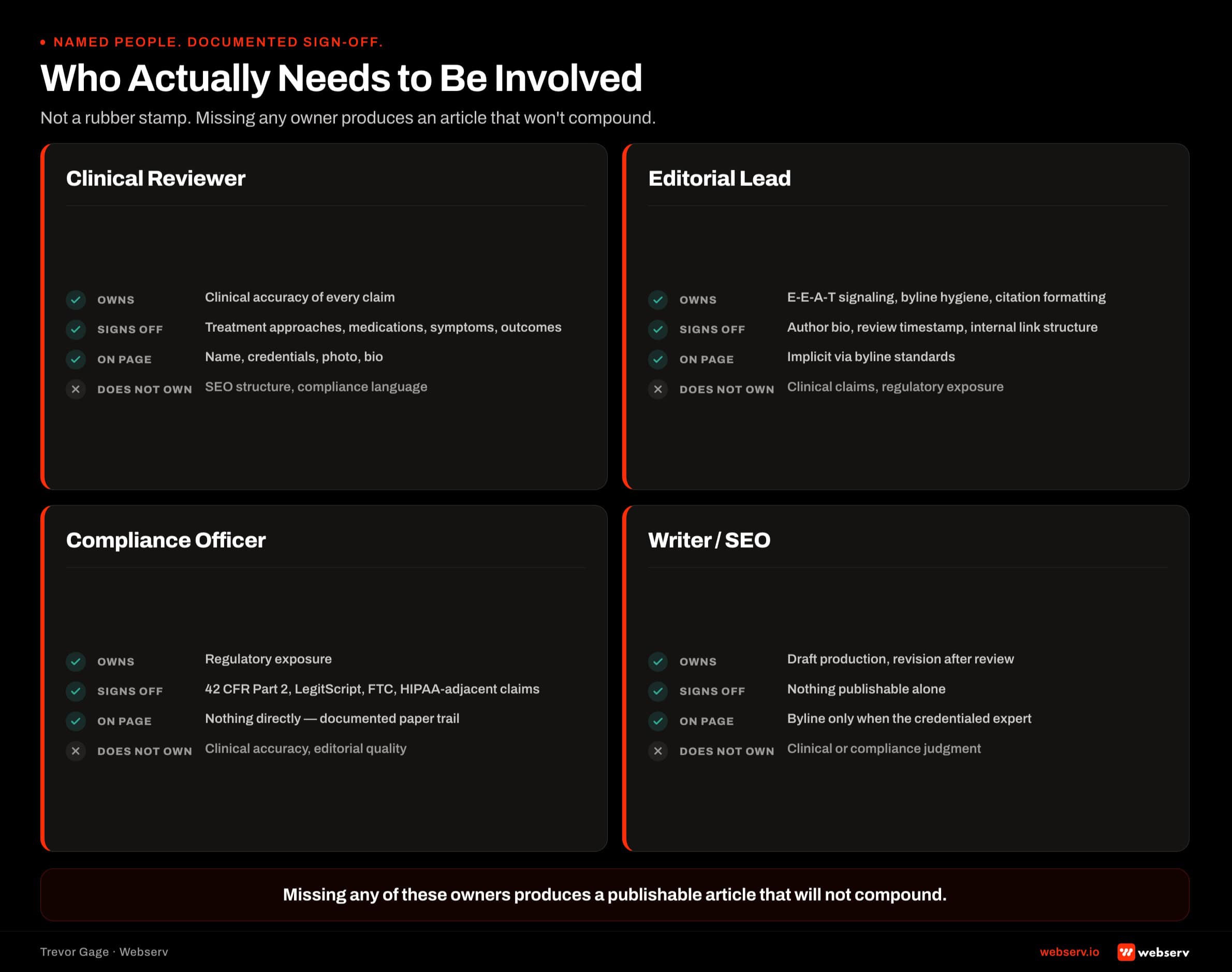
The Writer. Produces the initial draft. May be in-house, contract, or agency. Provides source-of-truth citations for every clinical claim.
The Clinical Reviewer. Named clinician with credentials relevant to the article’s topic. Reviews for accuracy. Signs off with a review timestamp that gets published on the article.
The E-E-A-T Editor. Marketing team member or SEO specialist who audits the byline, bio, credentials display, citations, and structural signaling. This role can rotate but has to be explicitly owned by someone.
The Compliance Reviewer. Compliance officer, legal counsel, or a designated compliance function. Reviews for 42 CFR Part 2, LegitScript, FTC, and HIPAA-adjacent issues. In smaller treatment centers, this can be the executive director wearing the compliance hat.
The Publisher. The person who actually pushes the article to the CMS after all three reviews pass. Usually the marketing team lead. Confirms every element is in place before publishing.
For treatment centers without a medical director or in-house clinical reviewer, the reviewer role can be filled by a credentialed consultant on retainer, a contracted medical writer with clinical credentials, or a rotating panel of clinical staff who cover their specialty areas.
What does not work: a nurse or clinical staff member without publishing-relevant credentials, or a marketing team member with clinical vocabulary but no license.
The Two-to-Four-Hour Article Timeline
THE WORKFLOW ADDS 2 TO 4 HOURS PER ARTICLE ACROSS THE THREE STAGES, ON TOP OF WRITING TIME
Sequential timing looks like: writing (12-16 hours), clinical review (60-90 minutes), E-E-A-T check (30-45 minutes), compliance review (30-60 minutes), writer revision based on all three reviews (60-120 minutes), final publish. The workflow can compress if the clinical reviewer and compliance reviewer engage in parallel late-stage rather than fully sequentially, but the sequential-first cycle is what catches issues before they compound.
The compression tactics that work without breaking the discipline:
Batching. Reviewers examine three or four articles in a single sitting rather than one at a time. Cuts context-switching overhead.
Templates. Standardized E-E-A-T checklists, clinical review checklists, and compliance checklists that the reviewer runs through rather than reinventing each time.
Reusable citations. A curated library of pre-vetted authoritative sources (SAMHSA, ASAM, JCAHO, CARF, peer-reviewed journals) that writers cite from rather than having to research fresh each article.
Staff clinical writers. Writers who are themselves credentialed clinicians (LCSWs, RNs with behavioral health backgrounds, LADCs) can reduce the clinical review time because the accuracy check becomes lighter.
The compression tactics that erode the workflow:
- Skipping the clinical review “just this once” for time pressure.
- Copy-pasting review credit without actual review.
- Publishing without compliance review because the topic “seems safe.”
- Stale review timestamps that suggest the article was reviewed when it was not.
What Passes Post-March-2026 vs What Doesn’t
THE MARCH 2026 GOOGLE ALGORITHM UPDATE SPECIFICALLY DEVALUED UNMOTIVATED AI-GENERATED CONTENT ON YMYL TOPICS
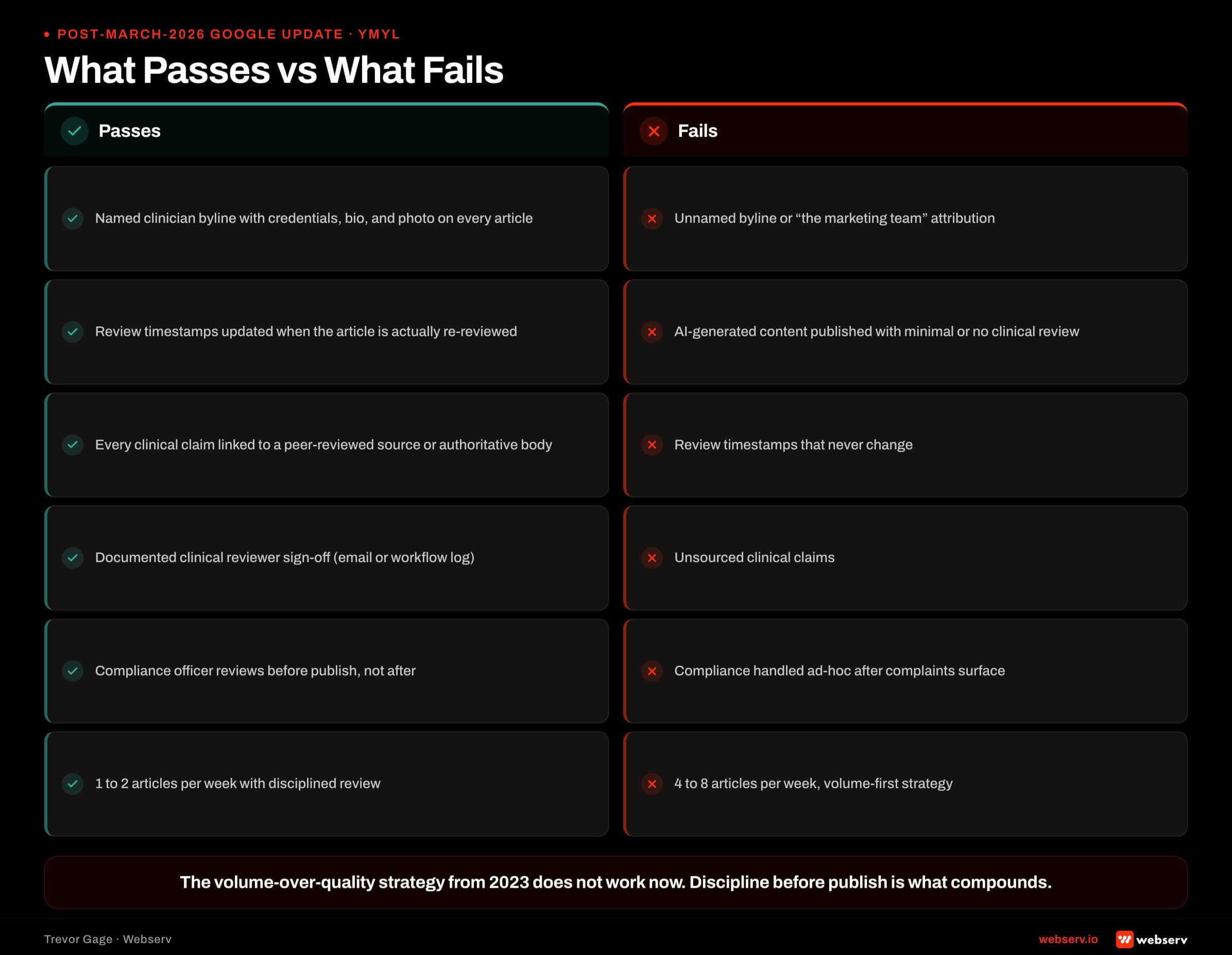
Treatment center sites that were producing 4-8 articles per week with minimal review lost significant traffic. Sites producing 1-2 articles per week with disciplined clinical review either held ground or gained share. The volume-over-quality strategy that worked in 2023 does not work now. AI content itself is not the problem; unreviewed AI content on YMYL topics is.
1-2/wk
sustainable publishing cadence with full clinical review workflow
4-8/wk
typical volume that lost traffic in the March 2026 update
2-4 hrs
added time per article for the three-stage review workflow
The content that passes post-update:
- Named clinician author with credentials visible on the page.
- Content depth of 1,500 to 3,000 words with substantive clinical detail (not fluff to hit a word count).
- Every clinical claim linked to an authoritative source (SAMHSA, peer-reviewed research, government health agencies, credentialed clinical bodies).
- Recent review timestamp indicating the content was examined for accuracy within the last 12 months.
- Author bio that establishes expertise and links to further credentials.
- Internal links to related content on the same site (topical authority signal).
- FAQ sections with substantive answers, not just SEO padding.
The content that fails post-update:
- Missing or unnamed author.
- Generic “medical team reviewed” without a named individual.
- Timestamps that never update, suggesting no ongoing review.
- Claims made without citations.
- Word count achieved through repetition or restatement.
- No internal linking, orphaned pages.
- Thin FAQ sections written to hit schema markup rather than to inform.
The Common Failure Patterns
WORKING CLINICAL REVIEW PATTERNS
- Named clinician byline with credentials, bio, and photo visible on every article
- Review timestamps updated when the article is actually re-reviewed
- Every clinical claim linked to a peer-reviewed source or authoritative body
- Clinical reviewer signs off with a documented paper trail (email, workflow log)
- Compliance officer reviews before publish, especially for patient-adjacent content
FAILURE PATTERNS THAT GOOGLE NOW PENALIZES
- Unnamed ‘medical team’ or generic ‘staff writer’ bylines on clinical content
- Static timestamps from initial publish, never updated, no ongoing review
- Clinical claims presented without citations, treated as common knowledge
- Verbal ‘yeah, looks good’ clinical review with no documentation
- Marketing team publishes without compliance review because ‘it’s just a blog post’
The pattern that surprises operators most often on audits is the missing paper trail. The clinical review may have actually happened; the clinical director may have looked at the article and given approval verbally. But no documentation exists.
When the marketing team lead departs and the compliance officer is asked whether the article was reviewed, the answer is uncertain. That uncertainty is what Google reads as the absence of review, and it is what fails audits when regulatory questions arise.
The paper trail is the workflow. Not the intention. Documented review by a named individual, tied to a specific article version, with a timestamp and any revision notes.
When to Start Building the Workflow
The workflow pays back inside 90 to 120 days on new content and inside 6 to 12 months on backfilled older content. Backfilling older content with retroactive clinical review, updated timestamps, and E-E-A-T signaling is one of the highest-return activities we run in SEO recovery engagements.
The realistic cadence for a treatment center starting from zero:
Month 1. Design the workflow, hire or designate the reviewer, build the templates and checklists, train the marketing team.
Months 2-3. New content flows through the full workflow. Existing content stays as-is temporarily.
Months 4-6. Backfill the top 20-30 most-trafficked older articles with retroactive review, updated bylines, and E-E-A-T signaling.
Months 6-12. Continue backfilling. Extend to lower-trafficked but topically important pieces. Measure ranking and citation recovery.
Most treatment centers can execute this without hiring new staff by reallocating existing clinical, marketing, and compliance capacity into the workflow. The bottleneck is usually clinical reviewer time, which can be planned around a 3-5 hour weekly commitment from a medical director or clinical director. Book an intro meeting if you want to walk your current content review process with our team.
Frequently Asked Questions
Do we need this workflow if we outsource content to an agency?
Yes, and the workflow gets more important, not less. Outsourced content that skips clinical review is a bigger risk than in-house content that skips it, because the writer has less context on the treatment center’s clinical program and is more likely to introduce errors that a clinician would have caught.
The agency should provide the writing and E-E-A-T signaling, but the clinical review has to happen inside the treatment center. Named clinician on staff or on retainer, with editorial authority over what publishes. The article is published under a treatment center author (usually the reviewing clinician), not under the agency writer’s name.
Treatment centers that skip this step and publish agency drafts unchanged tend to end up with generic behavioral health content that Google increasingly does not distinguish from the volume of similar generic content across the category. The clinical review is what makes the content specific enough to compound.
Can a nurse or LCSW be the clinical reviewer?
Depends on the topic. For general behavioral health education, nursing content, care coordination topics, and family-support content, licensed nurses and LCSWs with relevant clinical experience are appropriate reviewers. Their credentials establish expertise on the topics they are qualified for.
For medication-focused content (MAT, psychiatric medications, medical detox protocols), the reviewer should be a physician (typically the medical director or an addiction medicine specialist). For diagnostic content, a licensed clinical psychologist or psychiatrist. For clinical outcome claims, a research-credentialed clinician.
Match the reviewer’s credentials to the article’s clinical claims. A licensed LADC reviewing a piece on MAT medication protocols is not the right fit even if the LADC has clinical experience with those medications. Google’s Search Quality Rater guidelines specifically evaluate whether the reviewer’s expertise matches the content’s topic.
What if we do not have a medical director?
Options in rough order of preference. First, contract with a credentialed clinician on a retainer basis specifically for content review.
Second, partner with a psychiatrist or medical director who consults for the facility on other clinical matters and can add content review to their scope. Third, if the treatment center has a clinical director with clinical credentials (LCSW, LPC, LMFT), that person can review content within their clinical scope.
What does not work as a substitute: a non-credentialed operator serving as reviewer, a marketing team member with clinical vocabulary, or an “anonymous medical team” credit with no named individual behind it. Google reads all three as absence of review.
For treatment centers that genuinely cannot find a reviewer, the honest response is to publish less content until they can. Fewer articles that pass YMYL review compound better than more articles that fail it.
How do we balance content volume with the review overhead?
The answer is fewer, better articles. The 4-8 per week cadence that worked pre-March-2026 was already producing diminishing returns; the update finished that model for treatment centers. The sustainable post-update cadence is 1 to 2 articles per week with full clinical review, plus disciplined distribution through the email, social, and video repurposing workflow.
Treatment centers running the higher-cadence unreviewed model tend to have a large content library that produces disappointing ranking and citation results. Consolidating to fewer, higher-quality articles with proper review typically produces better ranking within 90 to 180 days than the higher-volume approach did.
The math is intuitive once you see it. Google’s ranking systems now measure quality per article, not volume. Publishing 4 articles per week that each get read by 30 visitors is worse than publishing 1 article per week that gets read by 500 and cited by AI assistants in the process.
Trevor Gage is the Director of Marketing at Webserv, a digital marketing agency for treatment centers.