Most A/B tests on treatment center contact forms fail before they start. The setup looks reasonable, the platform is configured correctly, and the agency reports lifts at the end of the test window.
The problem is that the metric being lifted is not the metric the operator cares about, and the test window is too short to produce meaningful data at behavioral health volumes.
A real conversion rate optimization practice for behavioral health treats the contact form as one stage of a multi-step funnel, not as a standalone conversion event. The test that matters is whether the variant produces more admission inquiries, not more form fills.
This piece covers the specific tests behavioral health operators should be running on contact forms and CTAs, how to size the tests for the volume profile of a typical treatment center, what HIPAA-compliant testing actually looks like, and the five mistakes that show up consistently in tests we audit.
Key Takeaways
- The right primary metric for a BH A/B test is admission inquiries, not form fills. Form-fill optimization can produce 25 to 40% lifts in form-fill rate that translate to zero or negative lifts in actual admissions, which is the metric the operator cares about.
- Statistical significance in small-volume BH accounts requires longer test windows than agencies usually run. A typical treatment center landing page produces 200 to 800 form fills a month. Real significance on a 15% lift hypothesis requires 60 to 120 days of test runtime, not 14 to 21 days.
- HIPAA constraints shape what tools you can use. A/B testing platforms that touch form data flowing through the page are business associates under HIPAA in 2026, which means they require a signed BAA before they can be used on the form. Most popular testing tools do not sign BAAs.
- The highest-impact tests in BH are form field count, CTA copy and placement, social proof framing, and insurance verification flow. The lowest-impact tests (and the most common time-wasters) are button color, font size, and minor copy variations.
- Calls and forms compete for the same attention. Most BH landing pages should test the call-versus-form decision before testing within either CTA. Roughly 60 to 75% of BH admission inquiries come in by phone; pages optimized only for form fills miss the dominant conversion path.
A 42-bed treatment center asked me to audit their landing page A/B test results last fall. The prior agency had been running tests on the primary admissions form for six months, claiming a 28% conversion lift on the “winning variant” over the control.
The operator was happy with the numbers and was about to push the variant live across the rest of the site. I pulled the data.
The test had been running for six months because the agency could not get statistical significance on any individual two-week window.
The “winning” variant had won across the full six months only after the agency ran the same test through three different statistical methods and picked the one that produced significance. The primary metric was form fills, not admission inquiries.
When I ran the variant against admissions data instead of form-fill data, the variant was actually 14% worse at converting form fills to admissions because it captured lower-intent users who never followed through. The “28% lift” was 28% more useless form fills.
We threw out the six-month test result, redesigned the testing program around admissions as the primary metric, and ran one clean test over 90 days that produced a real 17% admission lift on a single variant change.
The operator was running blind for the prior six months because the test design was wrong from the start.
That pattern is the norm in behavioral health A/B testing, not the exception. The mechanics of testing in this category are different from testing in general SaaS or e-commerce, and most agencies have not adapted.
This piece covers what A/B testing actually looks like for a treatment center contact form or CTA in 2026, with the BH-specific constraints that change what works.
Our conversion rate optimization practice treats every test as a hypothesis about admissions, not about clicks or fills, because admissions are what produce revenue.
Why A/B testing breaks in behavioral health unless you control for specifics
The standard A/B testing playbook from the SaaS and e-commerce world transfers poorly to BH. Four structural differences change what works.
The first is volume. SaaS A/B testing typically runs on landing pages with 5,000 to 50,000 monthly visitors. Behavioral health treatment center pages typically see 500 to 5,000 monthly visitors, with form fills running 200 to 800 a month.
The statistical sample sizes that produce significance in SaaS in 7 to 14 days require 60 to 120 days in BH. Tests run shorter than the actual significance window produce false positives that look like wins but disappear when the test is extended.
The second is the buyer journey. A SaaS lead form fill is usually close to the conversion event (a demo, a trial). A BH form fill is 14 to 60 days from the conversion event (the admission).
The lag breaks the assumption that optimizing for fills optimizes for revenue. A variant that increases form fills by 30% but reduces fill-to-admission conversion by 25% produces a small net admission gain or a net loss, depending on the specific numbers.
SaaS A/B testing rarely surfaces this because the lag is shorter.
The third is the call channel. Roughly 60 to 75% of BH admission inquiries come in by phone, not by form. A form-only A/B test ignores the channel that produces most of the revenue.
Tests that optimize the form at the expense of the call (a more aggressive form layout that pushes the phone CTA below the fold, for example) can boost the form metric while reducing total conversions.
The fourth is HIPAA. A/B testing tools that touch form data flowing through the landing page are business associates under HIPAA, which means they require a signed BAA before they can legally process the data.
Most A/B testing platforms (Optimizely, VWO, AB Tasty, Convert.com) do not sign BAAs by default. Operators running these tools on forms that capture any health-related information are creating compliance exposure on top of the testing program.
Each of these four differences can be controlled for. Most testing programs do not control for any of them, which is why the test results so often produce the “28% lift that produced zero admissions” pattern.
Pick the right primary metric
The most consequential design decision in a BH A/B test is the primary metric. The wrong choice invalidates every test result that follows.
The two candidates are usually form fills and admission inquiries. Form fills are easy to measure (the page tracks them directly) and produce quick statistical significance because the volume is higher.
Admission inquiries are harder to measure (they require CRM integration, call tracking, and a lag window of 14 to 30 days) but they reflect the metric the operator actually cares about.
The right primary metric for BH is admission inquiries, with form fills as a secondary metric. Every test should be evaluated against both. The pattern to watch for is the divergent test: form fills up, admission inquiries flat or down.
This pattern shows up frequently when the variant reduces form friction (fewer fields, smaller copy, more aggressive CTA placement) in ways that capture lower-intent users.
The operational requirement is that conversion tracking has to be configured to capture both metrics with attribution back to the specific variant. The conversion tracking framework is the same infrastructure that powers paid media attribution; it needs to be in place before A/B testing produces reliable results.
For multi-location operators or operators with multiple level-of-care offerings, the primary metric should be admissions per level of care, not aggregate admissions.
The exclude-zip framework for geo targeting also matters here because per-location admission attribution depends on which geographies the traffic comes from. A variant that lifts residential admissions and reduces PHP admissions may or may not be a net win depending on the revenue mix.
The minimum sample size problem
Small-volume BH accounts cannot run the 14-day tests that SaaS marketing blogs recommend. The math does not work.
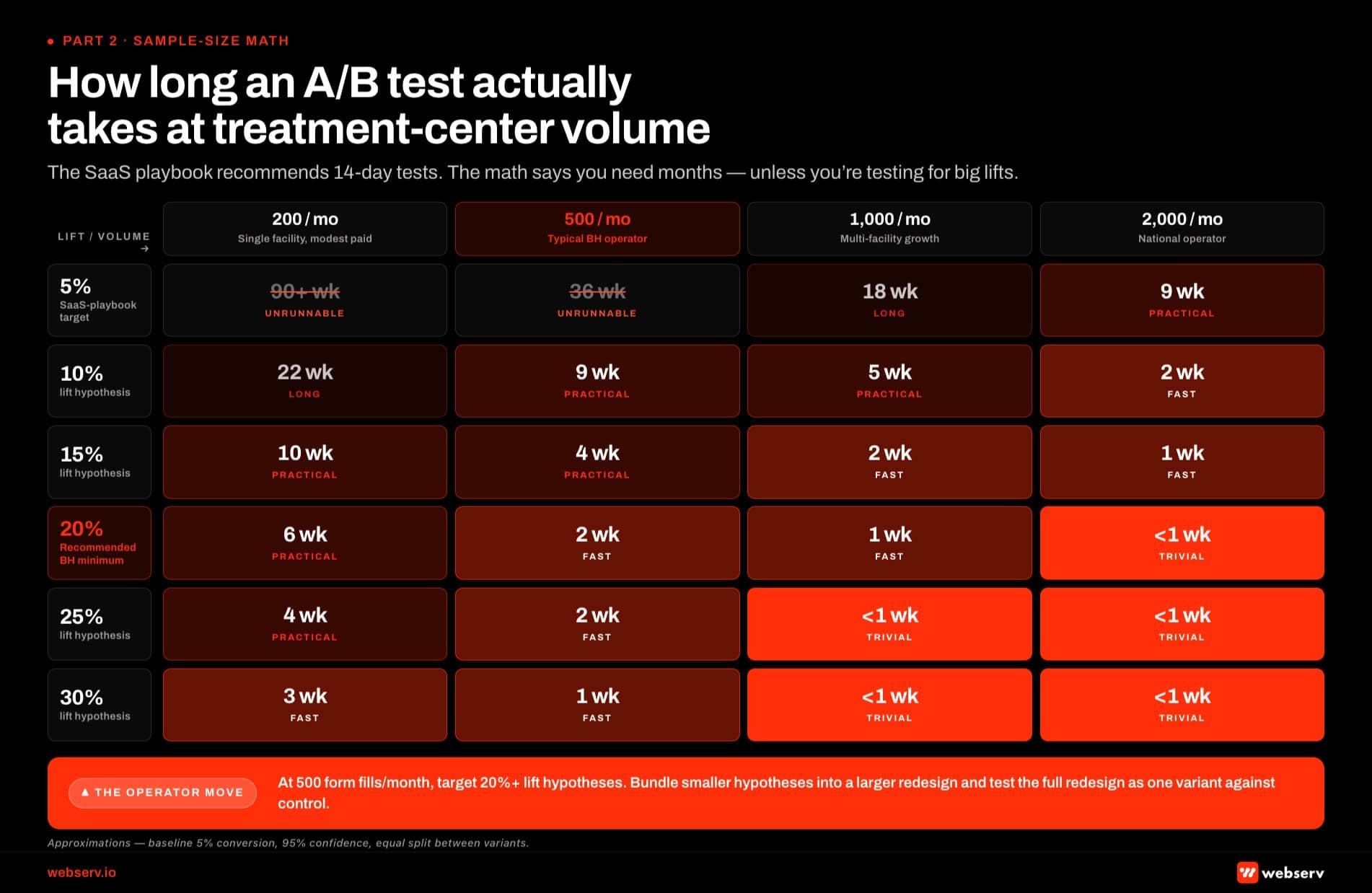 Infographic titled ‘How long an A/B test actually takes at treatment-center volume’ showing a chart visualizing the relationship between monthly form-fill volume on the horizontal axis (200, 500, 1000, and 2000 per month) and lift hypothesis size on the vertical axis (5 through 30 percent). Each cell shows the approximate test runtime in weeks required to reach 95 percent statistical confidence. Cells representing runtimes longer than 26 weeks are greyed and marked unrunnable; cells representing achievable runtimes at typical BH volume are highlighted in brand red. At 500 form fills per month, a 5 percent lift takes roughly 36 weeks (unrunnable), a 10 percent lift takes 9 weeks, a 15 percent lift takes 4 weeks, and a 20 percent lift takes 2 weeks. At 200 form fills per month, a 10 percent lift takes 22 weeks, a 15 percent lift takes 10 weeks, and a 20 percent lift takes 6 weeks. The chart contrasts with the SaaS testing playbook which recommends 14-day tests because SaaS sites operate at the upper right of the chart where volume is high and small lifts can be detected quickly. Bottom strip: at 500 form fills per month, operators should target 20 percent or greater lift hypotheses and bundle smaller hypotheses into a larger redesign tested as one variant against control.
Infographic titled ‘How long an A/B test actually takes at treatment-center volume’ showing a chart visualizing the relationship between monthly form-fill volume on the horizontal axis (200, 500, 1000, and 2000 per month) and lift hypothesis size on the vertical axis (5 through 30 percent). Each cell shows the approximate test runtime in weeks required to reach 95 percent statistical confidence. Cells representing runtimes longer than 26 weeks are greyed and marked unrunnable; cells representing achievable runtimes at typical BH volume are highlighted in brand red. At 500 form fills per month, a 5 percent lift takes roughly 36 weeks (unrunnable), a 10 percent lift takes 9 weeks, a 15 percent lift takes 4 weeks, and a 20 percent lift takes 2 weeks. At 200 form fills per month, a 10 percent lift takes 22 weeks, a 15 percent lift takes 10 weeks, and a 20 percent lift takes 6 weeks. The chart contrasts with the SaaS testing playbook which recommends 14-day tests because SaaS sites operate at the upper right of the chart where volume is high and small lifts can be detected quickly. Bottom strip: at 500 form fills per month, operators should target 20 percent or greater lift hypotheses and bundle smaller hypotheses into a larger redesign tested as one variant against control.A typical treatment center landing page producing 500 form fills a month would need roughly 5,000 to 8,000 form fills in each variant to detect a 10% lift at 95% confidence (the standard threshold). That is 20 to 32 weeks of test runtime at the typical volume, not 2 weeks.
Evan Miller’s widely-cited A/B test sample size calculator confirms the order of magnitude. A baseline conversion rate of 5 percent with a 10 percent relative lift hypothesis at 95 percent confidence requires roughly 6,200 visitors per variant for the test to detect significance (Evan Miller, A/B Test Sample Size Calculator).
For a treatment center landing page producing 500 form fills a month, that is months of runtime per test, which is why the SaaS playbook does not transfer.
The practical implications:
Test for bigger lifts, not smaller ones. A 25% lift can be detected in 8 to 12 weeks at typical BH volume. A 10% lift takes 5 to 7 months.
Most BH A/B tests should target hypotheses with 20+% expected lift, which means the variants should be sharply different from the control, not minor tweaks.
Use sequential testing methods when available. Modern testing platforms support sequential analysis (Bayesian methods, Optimizely Stats Engine, similar) that can detect significance earlier than the classical fixed-sample approach. These methods are not perfect but they reduce the runtime for genuine lifts by 30 to 50%.
Run fewer tests, not more. Operators who run 5 tests at once on the same page with 500 monthly fills will produce 5 tests with no significance after 8 weeks.
The same operator running 1 test on the same page over the same 8 weeks will produce a result. Sequencing the tests is faster than parallelizing them at small volume.
Accept that some hypotheses cannot be tested. Hypotheses that produce 3 to 5% lifts are real but unrunnable at typical BH volume. The right move is to bundle them into a larger redesign rather than test them individually, and to test the full redesign as one variant against the control.
What to test (and what to ignore)
The high-impact tests in BH cluster around four areas. The low-impact tests, often pitched by agencies, cluster around aesthetic minutiae.
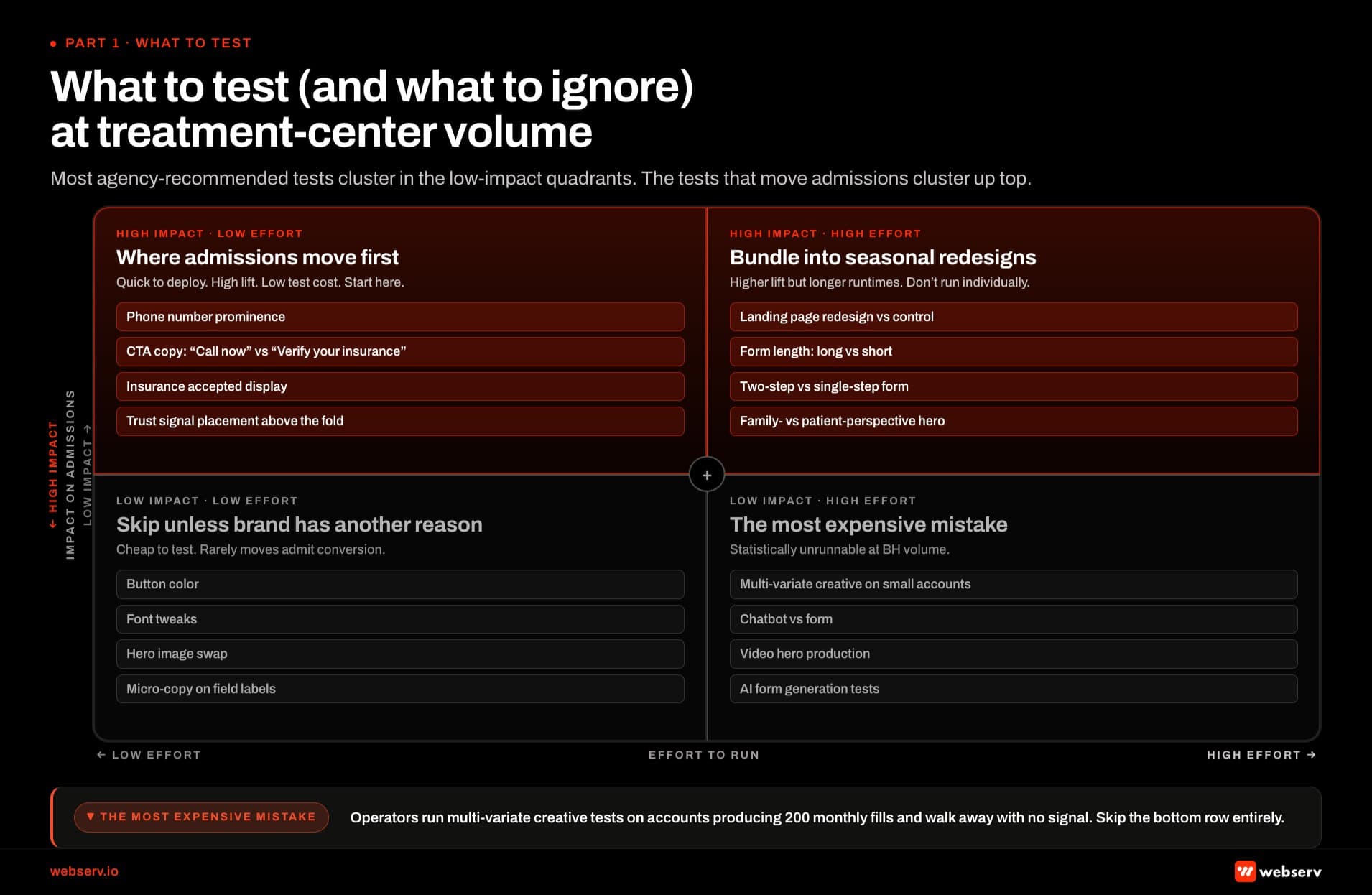 Infographic titled ‘What to test (and what to ignore) at treatment-center volume’ showing a two-by-two matrix mapping A/B test types against effort on the horizontal axis and impact on admission conversions on the vertical axis. Top-left quadrant high impact and low effort, shaded brand red, contains the highest-priority tests for behavioral health operators: phone number prominence on the page, CTA copy variants like ‘call now’ versus ‘verify your insurance,’ insurance accepted display, and trust signal placement above the fold; this cluster is quick to deploy with high lift and low test cost and is the recommended starting point. Top-right quadrant high impact and high effort, also shaded brand red, contains tests with higher lift but longer runtimes: full landing page redesign versus control, form length restructure of long versus short, two-step versus single-step form, and family-perspective versus patient-perspective hero; these should be bundled into seasonal redesigns rather than run individually. Bottom-left quadrant low impact and low effort, greyed, contains cheap-to-test variants like button color, font tweaks, hero image swap, and micro-copy on field labels; these rarely move admit conversion and should be skipped unless there is a brand reason. Bottom-right quadrant low impact and high effort, also greyed, contains tests that are statistically unrunnable at typical behavioral health volume: multi-variate creative testing on small accounts, chatbot versus form comparison, and video hero production; this is the most expensive mistake operators repeat. Bottom-right corner callout notes that operators running multi-variate tests on accounts producing 200 monthly fills walk away with no signal.
Infographic titled ‘What to test (and what to ignore) at treatment-center volume’ showing a two-by-two matrix mapping A/B test types against effort on the horizontal axis and impact on admission conversions on the vertical axis. Top-left quadrant high impact and low effort, shaded brand red, contains the highest-priority tests for behavioral health operators: phone number prominence on the page, CTA copy variants like ‘call now’ versus ‘verify your insurance,’ insurance accepted display, and trust signal placement above the fold; this cluster is quick to deploy with high lift and low test cost and is the recommended starting point. Top-right quadrant high impact and high effort, also shaded brand red, contains tests with higher lift but longer runtimes: full landing page redesign versus control, form length restructure of long versus short, two-step versus single-step form, and family-perspective versus patient-perspective hero; these should be bundled into seasonal redesigns rather than run individually. Bottom-left quadrant low impact and low effort, greyed, contains cheap-to-test variants like button color, font tweaks, hero image swap, and micro-copy on field labels; these rarely move admit conversion and should be skipped unless there is a brand reason. Bottom-right quadrant low impact and high effort, also greyed, contains tests that are statistically unrunnable at typical behavioral health volume: multi-variate creative testing on small accounts, chatbot versus form comparison, and video hero production; this is the most expensive mistake operators repeat. Bottom-right corner callout notes that operators running multi-variate tests on accounts producing 200 monthly fills walk away with no signal.High-impact tests
Form field count. Each additional form field costs roughly 10 to 15% of conversions in healthcare benchmarks. Reducing fields from 8 to 4 is one of the most reliable lifts available.
Reducing from 4 to 2 produces additional lift but at the cost of lead quality. The 3-to-5 field range is usually the sweet spot.
CTA copy. “Get insurance verified” vs “Talk to a counselor now” vs “Start admission” produce notably different conversion rates because they signal different commitment levels. Test the copy that matches the actual buyer’s mental state at the page level (high-intent vs research-stage).
CTA placement and call/form competition. Above-the-fold vs below-the-fold call CTA, sticky phone bar vs static, dual CTA (phone + form) vs single CTA. The placement decision affects which channel captures the conversion.
Social proof framing. Generic testimonials vs specific outcome data vs family-perspective quotes. The compliance constraints in BH limit what proof can be shown, but the proof that is shown matters.
Insurance verification flow. Inline verification widget vs link-out to a separate verification page vs phone-only verification. This is the highest-stakes decision for OON-economics treatment centers.
Low-impact tests to skip
Button color (gray vs blue vs orange usually produces noise, not signal). Font size on body copy (rarely moves conversion much). Minor wording variations on form labels (“Email” vs “Email Address”). Hero image variations within the same emotional register. Privacy policy link placement.
The reason to skip the low-impact tests is not that they produce zero effect, but that the effect is usually too small to detect at BH volume.
The broader CRO techniques framework covers the high-impact pattern set in more depth. Running them produces 60 to 90 days of test runtime that does not return a result.
Form-specific tests that produce real lift
Three form-side tests produce the most reliable conversion gains in our BH practice.
The field count test. Build a variant of the form with 30 to 50% fewer fields than the control.
The Facebook vs Google Ads channel-mix decision affects which traffic sources hit the form, which in turn affects how field count interacts with intent. Move the removed fields to a follow-up screen or capture them via the admissions team during the verification call.
The typical lift is 15 to 35% on form fill rate, with most of that lift translating to admission inquiries because the fields removed are usually qualification fields the admissions team would re-verify anyway.
The multi-step test. Convert a single-page form to a 2-step or 3-step progressive form, where the first step captures only name and contact method (phone or email) and subsequent steps capture insurance and clinical details.
The same CRO techniques that drive form-side lift apply across the broader landing page. Multi-step forms typically convert 20 to 40% better than equivalent single-step forms because the perceived commitment at each step is lower.
The trade-off is that drop-off occurs between steps; the net depends on step design.
The social proof test. Add a single specific outcome stat next to the form (“87% of families who verified insurance with us admitted within 14 days”) versus a generic trust signal (an accreditation badge).
Specific stats with HIPAA-compliant framing typically produce 8 to 18% lifts on form completion. The same compliance discipline that powers Meta Conversions API setup governs what claims can appear on the landing page.
Generic badges produce 1 to 3% and are usually inside the noise floor for BH volume.
The forms that fail testing tend to ask for clinical details (substance, frequency, severity) on the first form view. Those fields produce meaningful drop-off and are usually unnecessary because the admissions team will collect them during the verification call regardless.
CTA-specific tests that move admissions
CTA testing in BH is more nuanced because the CTA mediates between the call channel and the form channel. Three patterns matter.
The phone CTA prominence test. Move the phone number from a small header treatment to a sticky bottom bar on mobile, or to a large above-the-fold display element on desktop.
The CallRail call tracking setup captures the phone-channel attribution that makes this test measurable. Phone CTA prominence usually lifts phone admissions by 15 to 30%.
The trade-off is that some of those phone admissions cannibalize form admissions, so the net is usually a 10 to 20% total lift rather than a 30% lift on phone alone.
The CTA copy commitment test. Test “Talk to a counselor” (low commitment) vs “Verify your insurance” (medium commitment) vs “Start the admission process” (high commitment). The same compliance constraints that govern healthcare advertising compliance mistakes apply to CTA copy.
The right answer depends on the page traffic source. Cold paid social traffic usually converts better with low-commitment copy; high-intent paid search traffic often converts better with medium- or high-commitment copy.
The compliant ad headlines framework applies to CTA copy as well.
The dual-CTA test. Run dual phone + form CTAs above the fold vs single-CTA variants. The dual CTA usually wins on total conversion rate but produces lower-quality leads in the form channel because the high-intent users self-select to phone.
The healthcare demographic targeting signals that feed paid media also inform which CTA copy resonates with which audience segment.
For OON-focused operators, the dual CTA is usually right because both channels produce admissions. For Medicaid-heavy or in-network-focused operators, single-CTA phone-priority is often right because the call channel is more efficient.
How Profound Treatment drove 31 admits and a 42% drop in cost per viable in one quarter
Broad match pivot, negative keyword management, and intake-level conversion tracking turned a fragmented paid strategy into a predictable admissions engine.
Read the case study →68 viable VOBs at $4,529 cost per viable
HIPAA constraints on testing tools
A/B testing tools that touch the form data flowing through your landing page are business associates under HIPAA.
Any tool that sits in the conversion path and can see form submissions, click events, or session recordings that include form interactions requires a signed Business Associate Agreement before it can legally process the data.
The HHS-OCR guidance on Business Associate Agreements defines what counts and what the contract has to cover.
The platforms that sign BAAs for healthcare:
PostHog signs BAAs for enterprise customers. Optimizely signs BAAs at the enterprise tier. AB Tasty signs BAAs through their Healthcare-specific package. VWO does not currently sign BAAs as of 2026. Convert.com signs BAAs at higher tiers.
If your A/B testing platform does not sign a BAA, the safer setup is to run testing tools only on non-PHI portions of the page (above the form, on educational content) and to test the form itself through other methods. The other methods include:
Sequential variant rollouts where the form is fully replaced (not A/B tested) and performance is measured before-and-after over a 90-day window.
Server-side testing where variants are assigned and rendered before any tracking pixel fires.
Manual testing where the operator runs two different forms on two different days or two different traffic sources and compares outcomes.
The before-and-after rollout method loses some statistical rigor but works at BH volume and avoids the HIPAA exposure. For operators who do not have a BAA-signed testing platform, this is usually the right approach. The broader compliance posture on tracking technologies shapes which tools can be used at all.
The HHS-OCR enforcement environment in 2026 is stricter than in any prior year, and treatment centers running A/B tests on PHI-exposing forms through non-BAA platforms are taking on enforcement risk that compounds the testing program’s other risks.
A 28% lift on form fills that produces 14% fewer admissions is not a winning test. It is an expensive way to capture lower-intent leads while the admissions metric the operator actually cares about silently degrades.
Mitch Marowitz, Director of Paid Media, Webserv
A 90-day test plan that actually works
For a treatment center starting from scratch on A/B testing, the right plan looks like this.
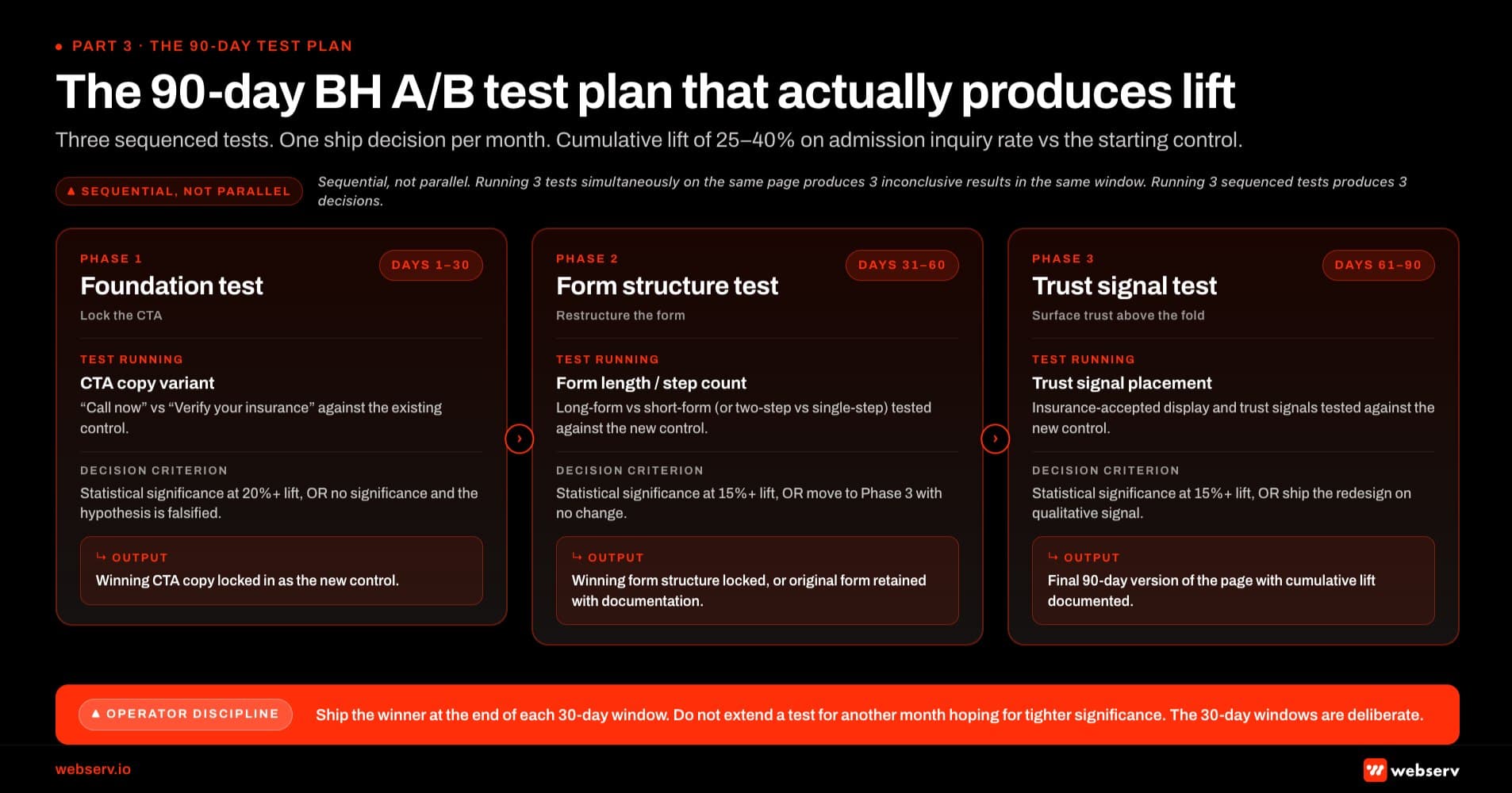 Infographic titled ‘The 90-day BH A/B test plan that actually produces lift’ showing the three-phase test sequence a treatment center should run from a standing start. Phase 1 Foundation test runs days 1 through 30 and tests a CTA copy variant such as ‘call now’ versus ‘verify your insurance’ against the existing control; the decision criterion is statistical significance at a 20 percent or greater lift, or no significance which falsifies the hypothesis; the output is winning CTA copy locked in as the new control. Phase 2 Form structure test runs days 31 through 60 and tests form length or step count variant against the new control; the decision criterion is statistical significance at 15 percent or greater lift, or move to Phase 3 with no change; the output is winning form structure locked or the original form retained with documentation. Phase 3 Trust signal test runs days 61 through 90 and tests trust signal placement and insurance-accepted display against the new control; the decision criterion is statistical significance at 15 percent or greater lift, or ship the redesign anyway based on qualitative signal; the output is the final 90-day version of the page with cumulative lift documented. Top callout: sequential tests not parallel, because at behavioral health volume running three tests simultaneously on the same page produces three inconclusive results in the same window while running three sequenced tests produces three decisions. Bottom strip: the operator discipline is to ship the winner at the end of each 30-day window without extending the test for another month hoping for tighter significance; the 30-day windows are deliberate.
Infographic titled ‘The 90-day BH A/B test plan that actually produces lift’ showing the three-phase test sequence a treatment center should run from a standing start. Phase 1 Foundation test runs days 1 through 30 and tests a CTA copy variant such as ‘call now’ versus ‘verify your insurance’ against the existing control; the decision criterion is statistical significance at a 20 percent or greater lift, or no significance which falsifies the hypothesis; the output is winning CTA copy locked in as the new control. Phase 2 Form structure test runs days 31 through 60 and tests form length or step count variant against the new control; the decision criterion is statistical significance at 15 percent or greater lift, or move to Phase 3 with no change; the output is winning form structure locked or the original form retained with documentation. Phase 3 Trust signal test runs days 61 through 90 and tests trust signal placement and insurance-accepted display against the new control; the decision criterion is statistical significance at 15 percent or greater lift, or ship the redesign anyway based on qualitative signal; the output is the final 90-day version of the page with cumulative lift documented. Top callout: sequential tests not parallel, because at behavioral health volume running three tests simultaneously on the same page produces three inconclusive results in the same window while running three sequenced tests produces three decisions. Bottom strip: the operator discipline is to ship the winner at the end of each 30-day window without extending the test for another month hoping for tighter significance; the 30-day windows are deliberate.Days 1-14: Baseline and infrastructure. Set up admission inquiry attribution back to landing page variants. Verify call tracking is integrated. Confirm BAA status on the testing platform. Pull baseline conversion rates on each landing page over the prior 90 days.
Days 15-30: Test 1 setup and launch. Pick the highest-impact hypothesis (usually form field count reduction). Build the variant. Configure the test with admission inquiries as primary metric and form fills as secondary. Launch.
Days 30-90: Test 1 runs. Resist the urge to call winners early. Watch the secondary metrics for divergence (form fills up, admission inquiries flat would be a red flag). At day 90, evaluate.
Days 90-105: Test 1 evaluation and Test 2 setup. If Test 1 produced a winner on admission inquiries, roll the variant to the full page. If Test 1 was inconclusive, archive the result and design Test 2 for a different hypothesis. Either way, Test 2 launches around day 105.
Days 105-180: Test 2 runs. Same discipline. By month six, the operator has run two tests, learned two specific things about what moves admissions, and rolled at least one variant if it won.
Operators who try to run 4 to 6 tests in the same 6-month window at typical BH volume produce 6 inconclusive results. Operators who run 2 tests with rigor produce 1 or 2 real wins. The patience pays off; the impatience does not.
Frequently asked questions about A/B testing for treatment centers
How long should a single A/B test run for a treatment center?
For BH landing pages producing 200 to 800 form fills a month, a single test typically needs 60 to 120 days to reach statistical significance on a 15 to 25% expected lift. Tests shorter than 60 days at this volume rarely produce reliable results; the early “winners” frequently revert when the test extends.
The honest answer is that operators who want faster results need either higher traffic volume (which usually means more paid media spend, which is its own conversation) or larger hypothesis swings (a full page redesign rather than a single-element test). Both approaches change the testing math.
The wrong approach is calling early winners. The pattern I see most often is an agency declaring victory at day 21 with a 15% lift, the operator rolling the variant, and the lift disappearing within 60 days as the sample size catches up to the real signal. Rolling early loses the discipline of the test program.
Should we test the contact form or the phone CTA first?
For most BH operators, test the phone CTA prominence first. Phone calls represent 60 to 75% of admission inquiries in this category, and most landing pages underweight the phone CTA in favor of the form. Moving the phone number to a more prominent position usually produces faster, more durable lift than form-side optimization.
After the phone CTA test is settled, then test the form. The order matters because the form test will be confounded by the call channel if the phone CTA is in the wrong place at the start. A form test run against a page where the phone CTA is below the fold will produce different results than the same test run after the phone CTA has been moved to a sticky bottom bar.
The exception is operators whose intake operation cannot handle inbound calls during the test window (limited after-hours coverage, intake team capacity constraints). For those operators, fix the intake operation before optimizing for more calls, then run the phone CTA test. The intake-team capacity decision sits alongside the paid social channel mix because both depend on the operations team’s ability to absorb the inbound flow.
Can we A/B test if our admissions team is small?
Yes, but the primary metric should still be admission inquiries, not form fills. A small admissions team produces lower-volume but still attributable conversion data. The test runtime is longer (90 to 180 days for small operators) but the same statistical principles apply.
The constraint to watch for is intake variance. If your admissions team’s conversion rate swings week-to-week (because of staff turnover, training periods, or seasonal volume), the A/B test will pick up that variance as noise. The fix is to run tests over longer windows that smooth across the intake variance, or to focus tests on the parts of the funnel that the intake team does not control directly.
The smaller the operation, the more important the test discipline becomes because each individual admission represents a larger percentage of total monthly admissions. Lucky weeks and unlucky weeks distort the data more than they do for larger operators.
Is it worth running A/B tests if we have under 200 form fills a month?
Mostly no. At 200 monthly fills, even aggressive 30% lift hypotheses require 4 to 6 months of test runtime to reach significance. Most operators at that volume are better off making bigger-picture changes (full page redesigns based on principles rather than testing) and measuring before-and-after rather than running parallel variant tests.
The principles-based redesign approach uses the heuristics that consistently produce gains in BH (fewer form fields, more prominent phone CTA, specific social proof, single clear hierarchy) without trying to A/B test each one. The trade-off is less statistical rigor on which specific change drove the result, but the operator gets the result without the multi-month wait.
Operators at this volume should focus their testing budget on the highest-impact hypotheses (form field count, phone CTA prominence) and skip the smaller optimization plays entirely.
What testing tools work best for BH treatment centers in 2026?
The platforms that sign BAAs for healthcare are Optimizely (enterprise), AB Tasty (Healthcare package), Convert.com (higher tiers), and PostHog (enterprise). These are the safer options for operators running tests on forms that capture any health-related information.
For operators without a BAA-signed platform, the workable alternatives are server-side variant rollouts (full-page replacement with before-and-after measurement over 90 days) and manual A/B testing through traffic source segmentation. Both approaches avoid the HIPAA exposure of running non-BAA tools on PHI-handling forms.
Google Optimize was discontinued in 2023 and is no longer an option. Some operators are still trying to run tests through it through legacy implementations; this should be retired.
How does A/B testing fit with our broader paid media program?
A/B testing on landing pages compounds with the paid media work that drives traffic to those pages. A variant that lifts admission rate by 15% multiplies the effective ROAS of every paid channel feeding the page. The math is simple: better landing page conversion = lower effective CPA across Google Ads and Meta = either lower spend for the same admissions or the same spend for more admissions.
The right sequencing is to get the paid media tracking infrastructure in place first (server-side conversion tracking, call tracking integration, attribution from ads to admissions), then layer A/B testing on top once the attribution is clean. The compliant ad headlines framework that governs paid creative also informs CTA copy testing. Running tests on top of broken tracking produces unreliable results because the primary metric cannot be measured accurately.
The compounding effect of clean tracking plus disciplined testing is what produces the BH operators who consistently grow admissions without proportionally growing budget. Most operators try to grow budget first; the ones who grow conversion rate first see better economics over a 12 to 24 month window. If you want a second opinion on whether your current A/B testing program is producing real admission lift or testing noise, reach out for a CRO audit and we can walk through your test history, your primary metric setup, and your testing platform compliance posture before recommending the next test.
The perspective in this article comes from 9 years working exclusively inside behavioral health.
We are a team built by people in recovery who understand that behind every admission is someone asking for help. If that resonates, get to know us.
Mitch Marowitz is the Director of Paid Media at Webserv, a digital marketing agency for treatment centers.