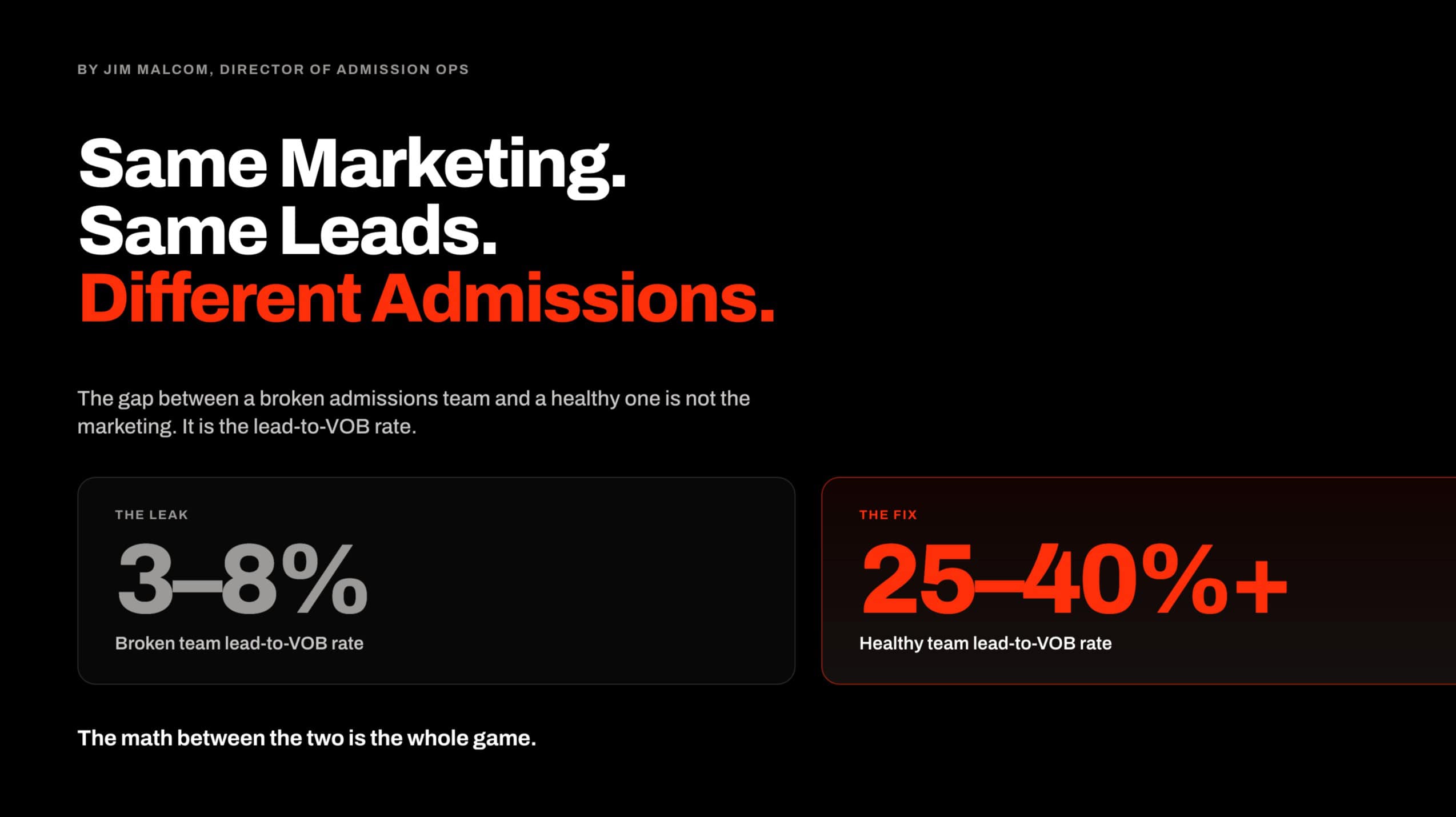
Marketing produces leads. Admissions produces admits. The math between those two is the whole game for a treatment center.
Most operators I audit are losing money in the gap between them. Their marketing works. Their clinical program works. Their admissions process, sitting between the two, is where the revenue disappears. Fixing that process is what I do inside our admission operations program at Webserv.
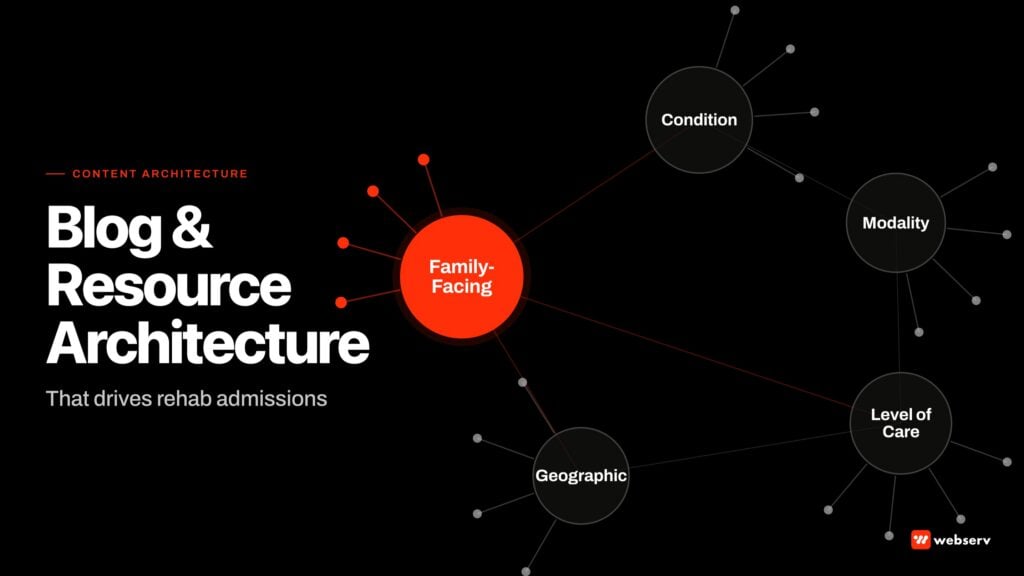
This is a complete guide for treatment center operators who want to build an admissions process that actually converts inbound leads into admitted patients.
It covers the 15-minute diagnostic I run at the front of every engagement, the five stages of a working admissions call, the two client archetypes I can most reliably turn around, the staffing math that most operators underestimate, and the close-rate benchmarks you should hold your team to.
Key Takeaways
- The single most reliable diagnostic on whether a treatment center’s admissions process is broken is the lead-to-VOB conversion rate. Healthy call-center accounts run above 25 percent, sometimes above 40 percent. Broken teams run 3 to 8 percent on the same marketing campaigns.
- A working admissions call has five stages: the first 60 seconds, the VOB pull, the two non-negotiables (emergency contact and commitment date), the clinical assessment, and the recommendation. The stages are sequential. Skipping any of them collapses everything downstream.
- The two client archetypes I can most reliably help are operators who have lost control of their admissions team to a hostage dynamic, and operators who have tried Google Ads and failed once or twice and now understand the 120-day investment math. Both are ready for the process rebuild.
- The staffing math most operators get wrong: seven days a week, sun up to past sundown, staffed double what you think. You do not need 24/7 coverage. You do need enough coordinators that a call never rings unanswered while another coordinator is on the phone.
- The cost math on a bad closing rate is brutal. A team closing at 10 percent on $4,000 viable prospects produces $40,000 cost per admit. The same leads worked by a team closing at 40 percent produce $10,000 cost per admit. An underqualified admissions rep is the most expensive person in your organization, period.
- The 120-day ramp is real. Building a working admissions process, calibrating paid media around it, and generating attributable admits takes four months of investment before the returns land. Operators who try to compress this timeline usually break the ramp.
The 15-Minute Diagnostic
The first thing I look at on any new engagement is the lead-to-VOB conversion rate week over week. If the number is under 10 percent while the marketing campaigns are producing real volume, I have the answer before I finish scrolling.
25-40%+
healthy lead-to-VOB rate at call-center-scale accounts
3-8%
typical broken-team VOB rate on the SAME campaigns
15 min
time to diagnose the process problem from the account data
The contrast is what tells the story. When I look at our blue-chip call center accounts, VOB rates run consistently above 25 percent and often above 40.
When I look at a broken team, the VOB rate is running 3 to 8 percent week over week on the same marketing campaigns, in the same paid search category, targeting the same prospects.
The gap is not marketing. The gap is admissions. Specifically, the coordinators are disqualifying phone calls.
They are hearing something in the first 30 seconds (“I want IOP,” or “I’m in New Orleans”) and telling the prospect no, we do not do that here, no you have the wrong number. Instead of running the qualification process, they are trying to get off the phone.
The 15-minute diagnostic identifies the pattern. The rebuild is what fixes it.
The Five-Stage Admissions Call
DEFINITION
The Admissions Funnel
The sequence a treatment center prospect moves through from first inbound touch to admitted patient: inbound lead, VOB, viable VOB, assessment, recommendation, commitment, admission. The funnel is measured at each stage, not at the top and bottom alone. Missing measurement in the middle is where most treatment centers lose track of their real conversion economics.
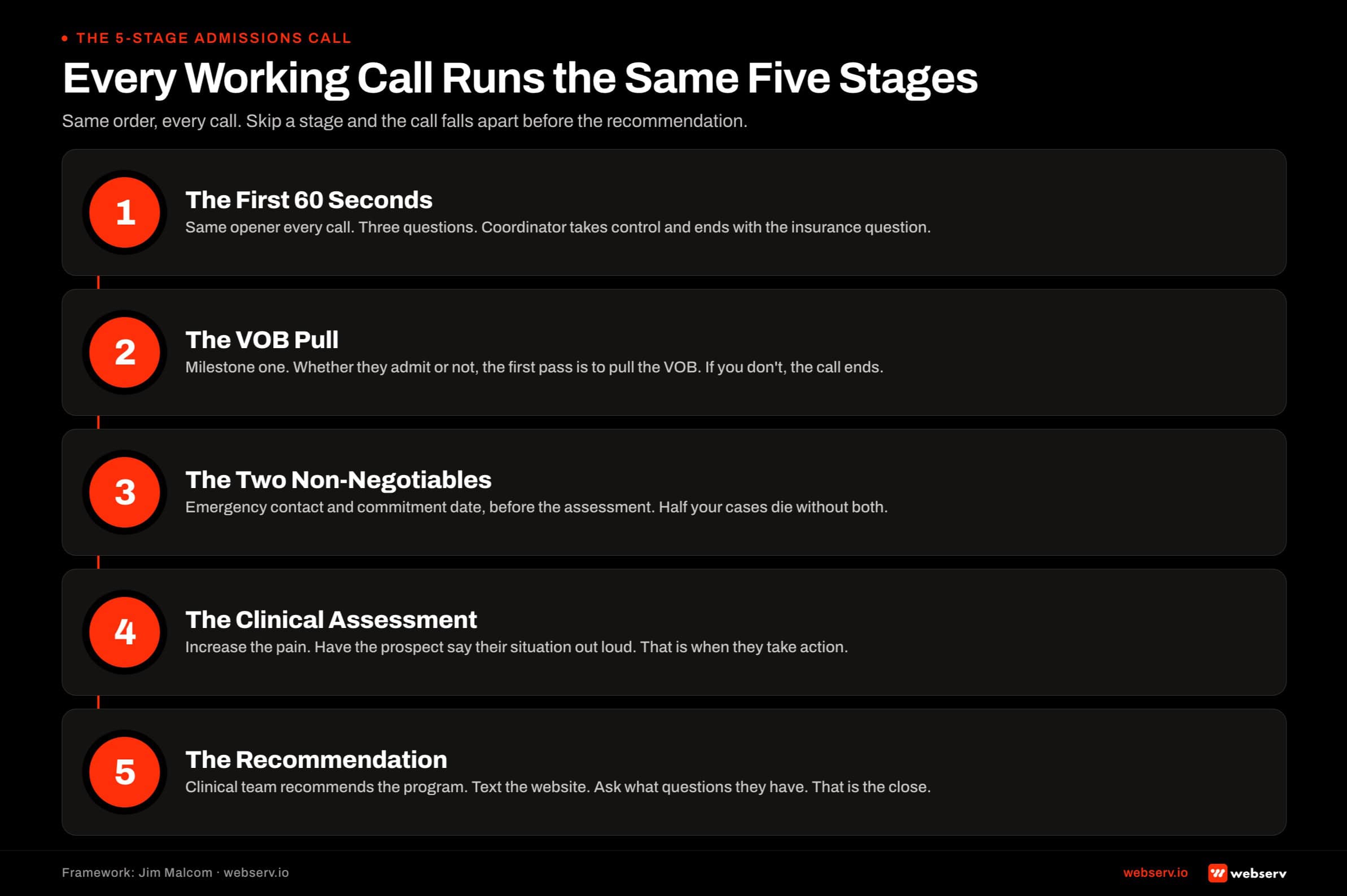
Every admissions call runs through the same five stages when it is working. The stages are sequential. Skipping any of them collapses the downstream conversion rate.
- The First 60 Seconds. Same opener every call. Coordinator asks three questions (name, self-or-loved-one, tell me how I can help). Coordinator takes back control. Coordinator delivers the expert insert and frames the process. Coordinator asks for insurance. The first 60 seconds ends with the transition to VOB.
- The VOB Pull. Milestone one on every call. Whether the prospect ends up admitting or not, the goal of the first pass is to pull the VOB. Some agencies run a bonus structure on VOB pulls for exactly this reason. If you get the VOB, you have a viable prospect to work with. If you don’t, the call ends and nothing downstream matters.
- The Two Non-Negotiables. Before the assessment starts: get the emergency or support-system contact, and get a commitment date. You lose half your cases without the support-system number. The commitment date establishes urgency and gives you something concrete to work toward on the recommendation call.
- The Clinical Assessment. The purpose is to increase the pain. The coordinator asks about use, consequences, family dynamics, treatment history. The prospect says it out loud. The coordinator reacts and stays interactive. People learn to live mediocre lives and adjust to them. When they say the pain out loud, they take action.
- The Recommendation. Based on the assessment, the clinical team recommends the appropriate program. The coordinator delivers the recommendation, texts the website, and asks what questions the prospect has. That is the whole pitch. The recommendation is the close. Objections get worked from there.
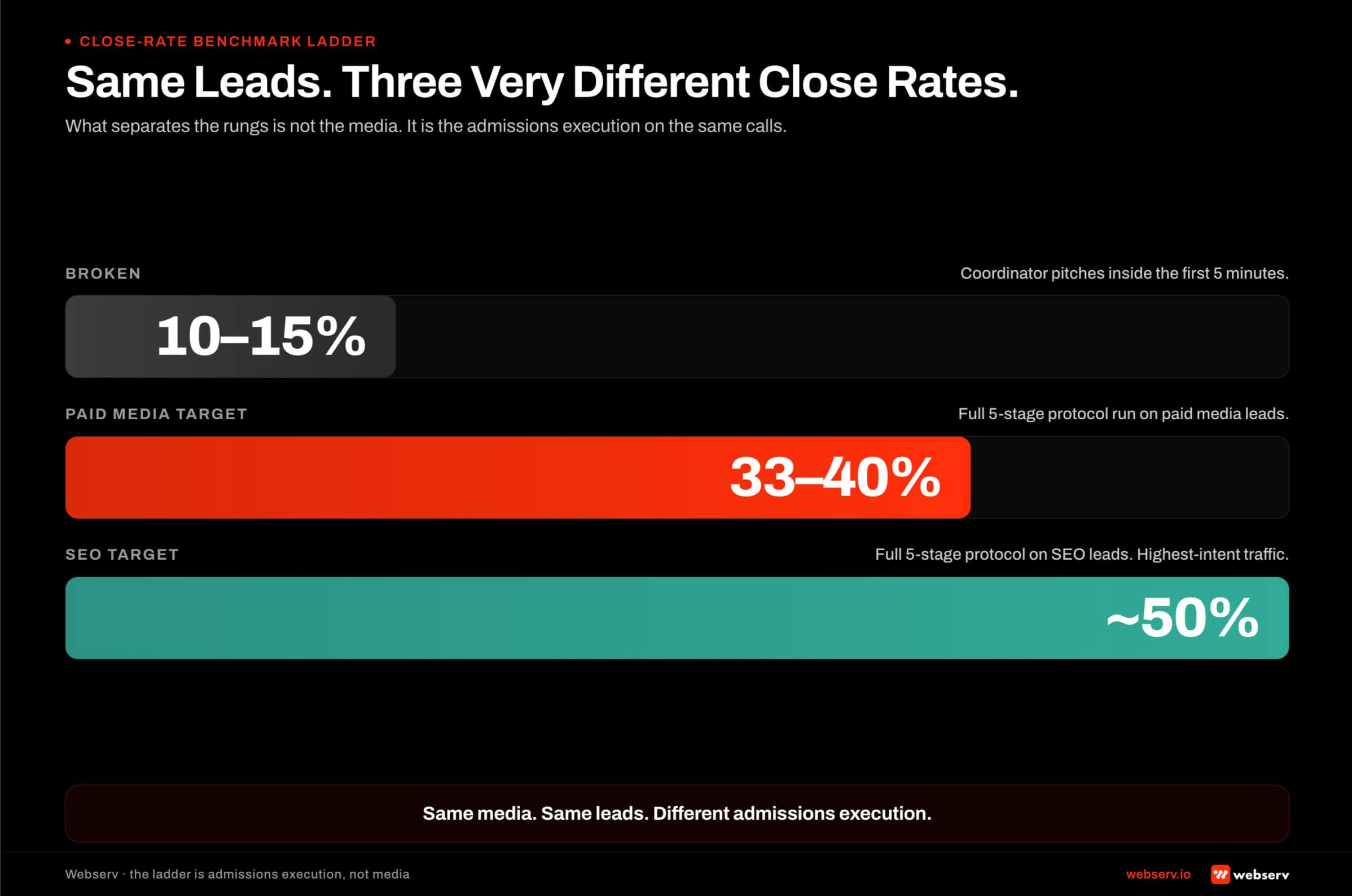
The most common failure I see is coordinators trying to close in the first five minutes. They hear “I want treatment” and start pitching the facility. That closes about 10 to 15 percent of viable prospects.
Prospects who lay down and admit without work happen. Most don’t. Running the full protocol gets you 33 to 40 percent on paid media leads and closer to 50 percent on SEO leads.
The Militant Rule
NEVER REVEAL YOUR LOCATION OR LEVEL OF CARE BEFORE THE VOB AND ASSESSMENT ARE COMPLETE
This is the rule that separates working admissions teams from broken ones. Prospects will ask both questions in the first 30 seconds of every call. Coordinators who answer either question before the qualification is complete lose the prospect. Being militant about this rule is not stubborn. It is what preserves your ability to make the right clinical recommendation instead of matching the prospect’s guess.
The pattern I see over and over: a prospect calls from Ohio, the coordinator answers “we’re in Southern California,” and the call ends.
The prospect never told the coordinator that their family would fly them out. The coordinator never told the prospect that the recommended program is the right clinical fit. The location conversation happens in minute two of a call that should have gone 25 minutes.
The same pattern applies to level of care. A prospect calls asking about outpatient treatment. If the coordinator says “we don’t offer outpatient here,” the call ends.
If the coordinator runs the assessment, the clinical team may recommend residential or PHP instead. The prospect never had the information to ask for the right level of care because they are not a clinician. They are calling for help.
The militant rule is what preserves the coordinator’s ability to do the actual job.
The Two Non-Negotiables After the VOB
THE SUPPORT-SYSTEM CONTACT AND THE COMMITMENT DATE ARE THE TWO FIELDS THAT SAVE MOST CASES
After you pull the VOB and before the assessment starts, get both. The support-system contact is who is going to help this prospect actually get on the plane, in the car, into the facility. Without that person’s number, half your cases evaporate between the recommendation and the admit. The commitment date establishes urgency and gives you something concrete to work back from.
The support-system contact is what closes cases that would otherwise slip. A prospect who commits on the phone and then hangs up alone is talking themselves out of treatment by minute 30.
A prospect whose support-system contact is called immediately after the admissions call has someone driving them to the airport in the morning. The difference between those two outcomes is one field on the CRM record.
The commitment date is not a promise. It is a target. Ask the prospect: if this works out, what day do you want to get started?
Their answer tells you what you are working with. Someone who says “next Monday” is close to ready. Someone who says “I need to think about it for a month” needs a different follow-up cadence. Either answer is useful. No answer at all means you did not ask.
The Clinical Assessment: Increase the Pain
The clinical assessment is where most admissions teams either compound their close rate or throw it away. The purpose of the assessment is not to fill out a form. It is to have the prospect say their situation out loud and understand its weight.
People learn to live mediocre lives, and when they do, they adjust to the pain. They stop feeling it as pain. The addiction becomes background. The consequences become normal.
The coordinator’s job during the assessment is to ask the questions that make the prospect describe their situation in their own words, and to react interactively as they hear the answers.
When the prospect says it out loud and hears the coordinator react, the pain surfaces again. That is when they take action.
The clinical framework underneath this approach is well-documented. SAMHSA’s TIP 35 on enhancing motivation for change in substance use disorder treatment is the underlying evidence base. Motivational interviewing does the same work in a clinical setting that the coordinator does on the phone.
The tone shift into the assessment matters. Do not tell the prospect how long the assessment will take. Move into it directly.
Set the frame: “Hey, I need you to be as honest as possible with me so I can get you to the right program. This is a judgment-free zone. If you’re not honest, I can’t help you.”
Have the prospect step away from their loved one if they need privacy. Then run the assessment.
The Recommendation Is the Close
At the end of the assessment, put the prospect on hold. Put them on mute. Listen to what they are saying to themselves. You will hear whether they are ready.
When you come back, deliver the recommendation. “Based on everything you told us today, our clinical team is recommending [program]. We’re going to help with the travel coordination. I’m going to text you the website right now. What questions do you have for me?”
That is the whole pitch. It is a recommendation based on a clinical assessment. There is nothing to sell. It is the prospect’s decision. Objections get worked from there.
Most coordinators are trying to sell the facility. Stop selling the facility. Prospects do not care about the swimming pool or the personal trainer. They care about themselves. Get them talking about themselves, increase the pain during the assessment, and deliver the clinical recommendation. That is the close.
The Client Archetypes We Turn Around
WHERE OUR ADMISSIONS OPS PROCESS WORKS
- Owners who have lost control of their admissions team to a hostage dynamic (internal or outsourced)
- Operators who have tried Google Ads and failed once or twice and now understand the 120-day / $50K math
- Educated startups that have been around the industry long enough to know what real admissions ops looks like
- Facilities in a crisis moment where the pain is great enough to force change
- Teams whose CRM data hygiene is at least workable, or whose owner will invest in fixing it
WHERE OUR ADMISSIONS OPS PROCESS STRUGGLES
- Owners who insist their existing admissions team is working when the VOB rate says otherwise
- Operators looking for a 30-day admissions turnaround with no infrastructure investment
- Teams that are ‘kind of working’ with senior egos protecting the current process
- Facilities where the pain isn’t great enough. Status quo is expensive but survivable
- Teams whose CRM is a graveyard of half-filled records and nobody will own the cleanup
The “kind of working” archetype is the hardest situation any of us walk into. The pain is not great enough to force the change, but the operation is not producing the admits the facility needs to grow.
In that situation, I usually recommend the operator wait until the pain forces the conversation, or we walk away from the engagement. Neither party wins if we take the work and cannot deliver the outcome.
The Staffing Math Most Operators Get Wrong
DEFINITION
The Coverage Window
The hours during which a treatment center’s admissions team must be actively staffed to answer inbound calls. For most centers, the coverage window is sun-up to past sundown, seven days a week. It is not 24/7. Prospects rarely call in the witching hours, but they call heavily on Sunday mornings and Saturday afternoons.
The math most operators get wrong on admissions team staffing has three components. The first is coverage window. Seven days a week, sun up to past sundown. You do not need overnight coverage in most cases. You do need weekends fully staffed.
The second is redundancy. When one coordinator is on the phone with a live call, every other inbound call is going unanswered. If you have one coordinator, half your calls miss.
If you have two coordinators, you drop fewer calls, but still miss calls during peak volume. The math is that you need to staff double what you think, because active-call time removes an agent from the answering pool.
The third is the cost of missed calls. On a paid media program producing $400 calls, missing three during a 90-minute active call costs $1,200 of media spend that produced no engagement.
If one of those three would have converted, the cost of the missed call was the value of the missed admit.
The staffing math is not about being open 24/7. It is about being open when your prospects actually call, with enough redundancy that a live call does not shut down the answering pool.
The Close-Rate Benchmark Ladder
10-15%
close rate when coordinators pitch inside the first 5 minutes
33-40%
target close rate on paid media leads with the full protocol
~50%
target close rate on SEO leads with the full protocol
The benchmark ladder is what I hold every admissions team to. If your team is running below 20 percent on paid media leads with the full protocol in place, the coordinators are the problem, not the protocol.
If your team is running above 40 percent on paid media, you are close to the ceiling on that lead source and the constraint has moved somewhere else in the funnel.
The cost math on the ladder is what most operators do not think about clearly. If your paid media is producing viable prospects at $4,000 apiece, a 10 percent close rate produces a $40,000 cost per admit.
Same media, 40 percent close rate, produces $10,000 cost per admit. The difference is not the marketing. The difference is the admissions team.
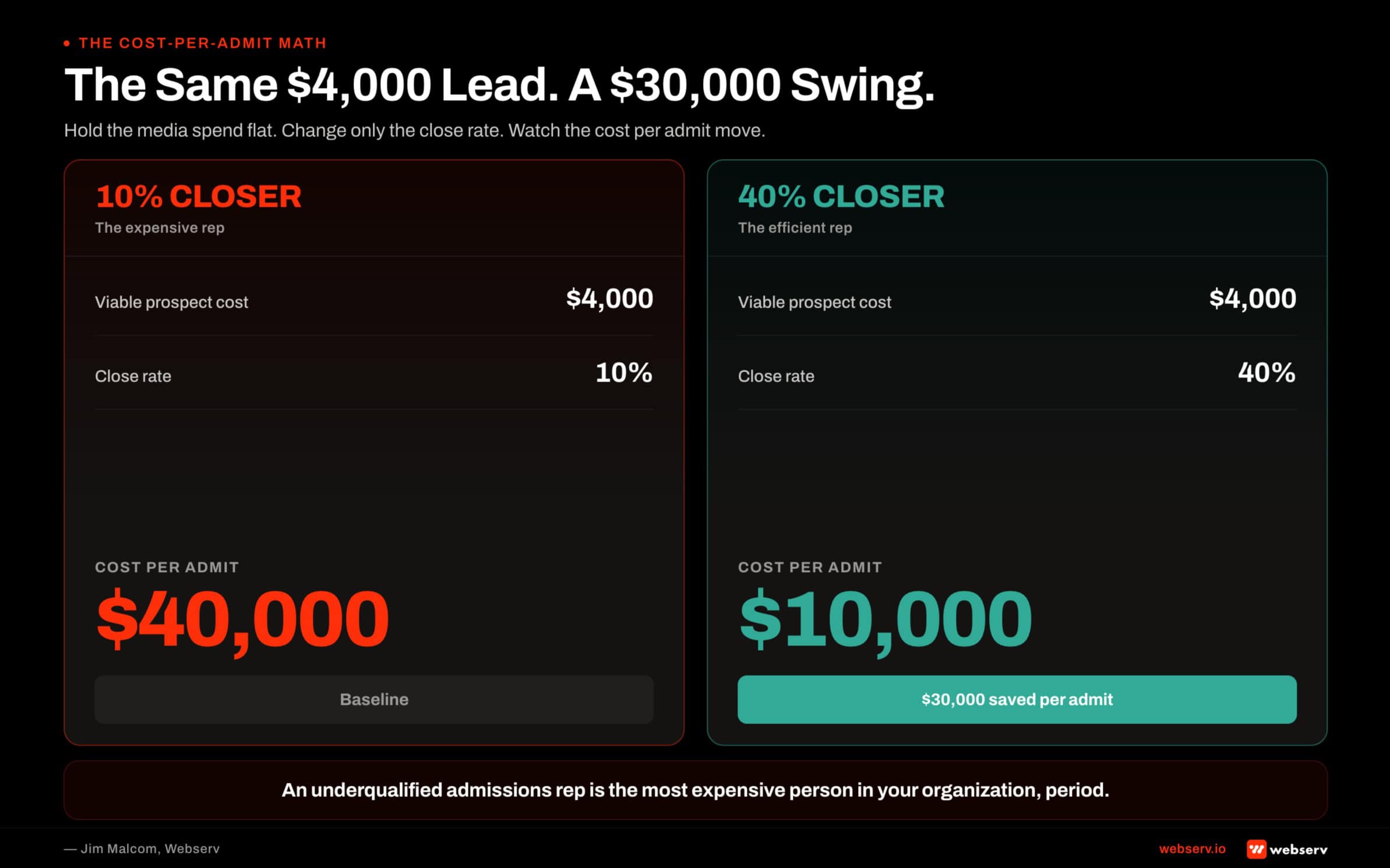
An underqualified admissions rep is the most expensive person in your organization, period. A 10 percent closer compared to a 40 percent closer on the same $200,000-a-month paid media program is millions of dollars in revenue difference across a year.
You have to work off actual data, not feelings about which coordinators are your top performers. Everyone says they are willing to check the numbers. Not everyone actually is.
The 120-Day Ramp
BUILDING A WORKING ADMISSIONS PROCESS TAKES 120 DAYS MINIMUM
Investing roughly $50,000 a month during that ramp before the returns land is the honest math. Operators who try to compress the ramp usually break it. The paid media has to run. The admissions team has to be trained. The CRM has to be configured. The reporting has to be reconciled. Four months of investment produces the process that pays back for the next four years.
The ramp is where operators either commit or bail out. The first 30 days build the foundation: audit, protocol design, coordinator training, CRM configuration.
The next 30 days deploy the protocol into live calls and start collecting real conversion data. The next 30 days calibrate the protocol against the data and refine. By day 120, the process is producing attributable admits at benchmark close rates.
Operators who pull the ramp at day 60 because they are not seeing enough admits usually made a call before the data was in. Operators who honor the ramp usually end up with an admissions operation that runs itself for years. Book an intro meeting if you want to walk your admissions data with our team live.
Frequently Asked Questions
Jim Malcom is the Director of Admission Ops at Webserv, where he leads admissions operations engagements for behavioral health treatment centers. He brings 13 years of experience in digital marketing and admissions within the behavioral health treatment space, spanning CRM systems, call center operations, and admissions team development. His focus is on turning marketing spend into measurable admissions outcomes.