Most agencies pitch behavioral health centers the same content-first SEO playbook they pitch SaaS and ecommerce clients, and most operators pay for the program before realizing the playbook produces traffic that does not convert. A real behavioral health SEO program reverses the standard build order: service pages and location pages come first, technical foundation and internal linking second, blog content last.
The reason is structural. Behavioral health search is crisis-driven, mobile, and family-initiated. The user typing “detox near me” at 2am is not in the awareness stage. They are not going to read a 2,400-word explainer on PHP versus IOP before calling. They are going to call the first defensible operator they find.
This piece walks through the funnel as it actually exists for behavioral health operators, why the standard content-first sequence breaks under those conditions, and the build order that produces admissions instead of blog traffic that nobody converts.
Key Takeaways
- Behavioral health search is crisis-driven, mobile, and family-initiated. The highest-return queries are commercial (“detox near me,” “outpatient rehab [city],” “[insurance] addiction treatment”), not informational.
- Service pages, location pages, and Google Business Profile coverage are the revenue surfaces. Blog content is the authority and AI-citation layer that supports them, not a substitute for them.
- The correct build order is: (1) service pages, (2) location and modality pages, (3) technical foundation and internal linking, (4) blog and AEO content. Skipping ahead to step four is the single most expensive mistake operators pay agencies to make.
- SAMHSA’s 2024 NSDUH found 52.6 million Americans needed substance use treatment and only 10.2 million received it. Most of that demand is searching, and most of those searches are commercial, not “what is rehab.”
- 2026 AI Overview data shows informational queries trigger AI Overviews 36% of the time versus 8% for commercial queries. Commercial pages still own the click; blog content increasingly owns the citation. Both matter. They are not interchangeable.
A treatment center we audited last quarter had eight service pages, four of them under 250 words, two with the wrong level of care in the H1, and one that 301’d to the homepage.
Their agency had spent six months and roughly forty thousand dollars writing blog posts about “the science of addiction” and “what to expect in early recovery.” The blog had 47 posts. None of them ranked. The service pages had never been touched.
The owner called us because organic admissions had flatlined. We pulled GSC. The pages driving the few admissions inquiries they did get from search were three thin service pages and a Google Business Profile with two photos. Nothing the blog produced was in the top thirty for any commercial query.
That mismatch is the most common SEO failure pattern in behavioral health. Agencies sell content-first programs because content programs are easy to staff and easy to invoice. Treatment center operators buy them because the pitch sounds like real marketing.
Six months later, the service pages are still broken, the location pages still don’t exist, and the commercial queries are still being lost to competitors with cleaner foundations.
The fix is a different build order. In behavioral health SEO, the SEO program gets built from commercial intent down to informational intent, not the other way around.
That order is determined by how families actually search when someone they love is in crisis, and by what each surface on Google can and cannot do for an admissions funnel.
Why behavioral health breaks the content-first playbook
MOST COMMON MISUNDERSTANDING
A family member typing “detox near me” at 2 a.m. is not in the awareness stage. They are not going to read three articles about the neuroscience of addiction before they call. They click two or three results, scan for trust signals, look for a phone number, and dial — often inside five minutes of the query. Selling a content-first flywheel to a treatment center on the same playbook you'd run for B2B SaaS builds the wrong asset first. Service pages have to exist before the blog does any lifting.
Most SEO programs are sold around a content-marketing flywheel. Write helpful articles, build topical authority, earn backlinks, and the commercial pages rise on the rising tide. That flywheel works in B2B SaaS, in e-commerce, and in long-consideration consumer categories.
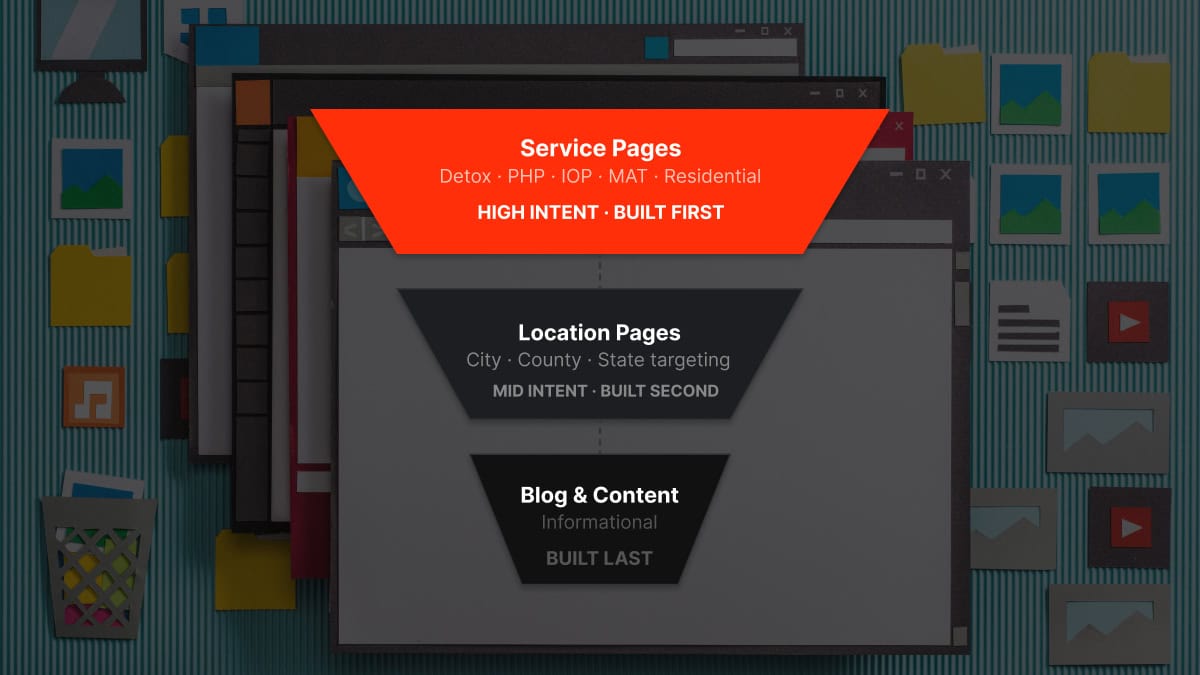
 Infographic titled ‘The 4-stage behavioral health SEO build order’ showing the operator-distinctive build sequence for behavioral health treatment center SEO. Stage 1 Service pages includes the PHP page, IOP page, detox page, residential page, and outpatient page covering every level of care and treatment type; these are the revenue surfaces where commercial intent converts. Stage 2 Location and modality pages includes city and state pages by service, modality pages for TMS and ketamine and medication-assisted treatment, and insurance-specific pages; these capture near-me queries and map-pack visibility. Stage 3 Technical foundation and internal linking includes mobile-first audit, Core Web Vitals, schema markup, site architecture, and internal link structure connecting Stage 1 and Stage 2 pages; this gets pages indexed and propagates ranking signals. Stage 4 Blog and AEO content includes authority articles, topical cluster coverage, FAQ depth, semantic triples, and AI citation surfaces; this is the authority layer that supports Stages 1 through 3, not a substitute for them. Compounding arrow indicates each stage compounds on the stage before, and skipping ahead is the most expensive mistake operators pay agencies to make. Bottom band notes that the standard agency pitch starts at Stage 4, leaving operators with six months of blog posts and zero admissions because the commercial pages were never built.
Infographic titled ‘The 4-stage behavioral health SEO build order’ showing the operator-distinctive build sequence for behavioral health treatment center SEO. Stage 1 Service pages includes the PHP page, IOP page, detox page, residential page, and outpatient page covering every level of care and treatment type; these are the revenue surfaces where commercial intent converts. Stage 2 Location and modality pages includes city and state pages by service, modality pages for TMS and ketamine and medication-assisted treatment, and insurance-specific pages; these capture near-me queries and map-pack visibility. Stage 3 Technical foundation and internal linking includes mobile-first audit, Core Web Vitals, schema markup, site architecture, and internal link structure connecting Stage 1 and Stage 2 pages; this gets pages indexed and propagates ranking signals. Stage 4 Blog and AEO content includes authority articles, topical cluster coverage, FAQ depth, semantic triples, and AI citation surfaces; this is the authority layer that supports Stages 1 through 3, not a substitute for them. Compounding arrow indicates each stage compounds on the stage before, and skipping ahead is the most expensive mistake operators pay agencies to make. Bottom band notes that the standard agency pitch starts at Stage 4, leaving operators with six months of blog posts and zero admissions because the commercial pages were never built.It does not work in behavioral health, because the underlying buyer journey is fundamentally different.
A family member typing “detox near me” at two in the morning is not in the awareness stage. They are not going to read three articles about the neuroscience of addiction before they call. They are going to click two or three results, scan for trust signals, look for a phone number, and dial. The window from query to call is often under five minutes.
Long-form content written for the same person two weeks earlier might have planted a brand impression, but the conversion event is happening on a service page.
This is consistent with what SEO operators in the space have been documenting publicly. Crisis searches like “detox near me” or “best inpatient treatment in [city]” run mobile-first and single-tap, driven by high emotion. Families search from hospital waiting rooms and parked cars. They will not fill out a ten-field form.
They want a page that confirms three things in the first ten seconds: you treat what they need, you take their insurance, and you can be reached now.
Blog content does not do that work. A 2,400-word explainer on “the difference between PHP and IOP” is useful, but it is not the page someone calls from. The page someone calls from is the service page for PHP at your specific facility, with the level of care defined in the H1, the population served clearly stated, and the call path one tap away.
The mistake most operators make is letting an agency confuse the role of those two assets. The blog post supports search visibility for educational queries and increasingly earns citations inside AI Overviews and ChatGPT answers. The service page captures the actual admission. One is air cover. The other is ground game. Building the air cover before the ground game exists is the most expensive ordering error in this category.
What the data actually says about funnel design
Two data points anchor the case for service-pages-first sequencing.
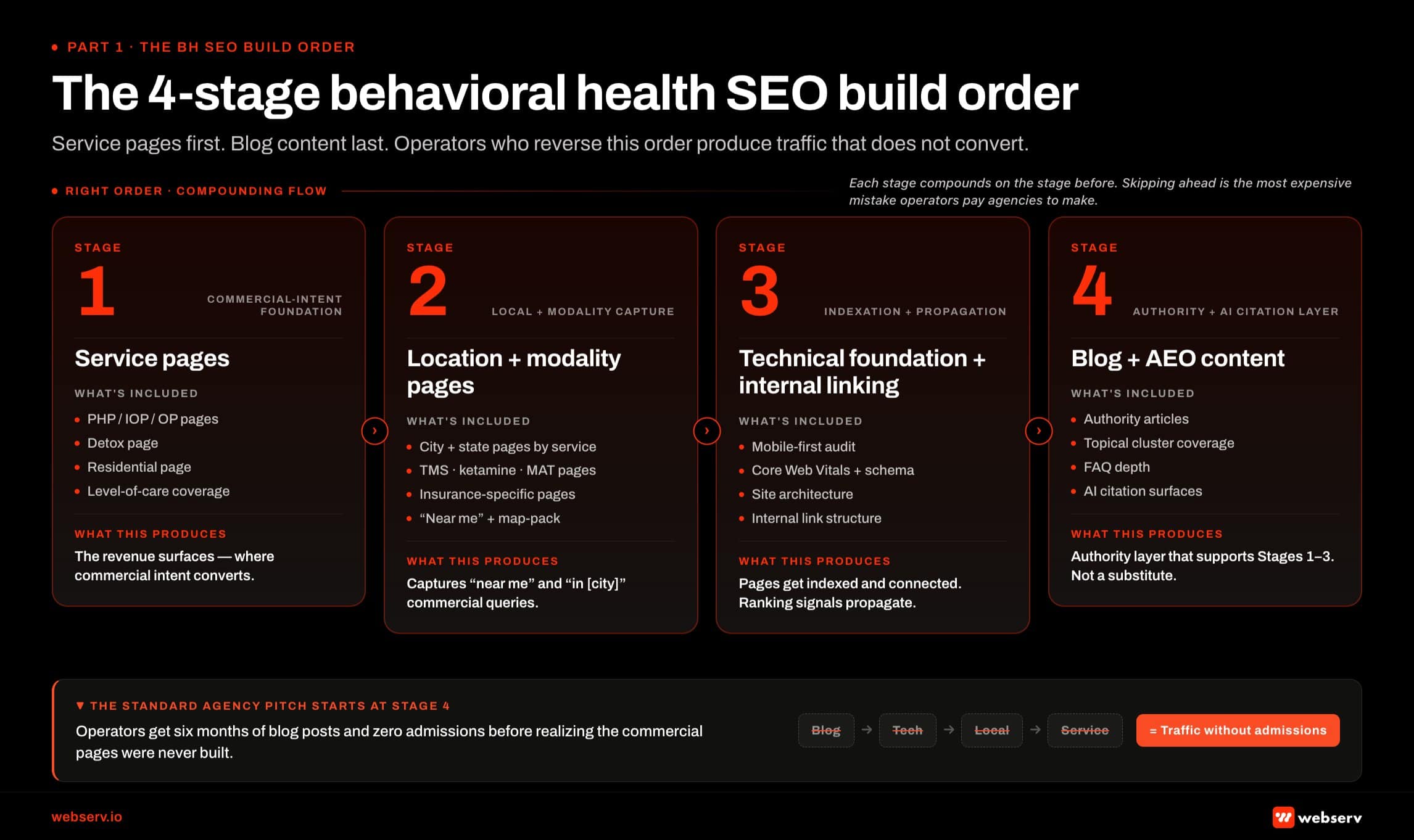
 Infographic titled ‘Where the conversions actually live in BH search’ showing a two-by-two matrix mapping behavioral health search queries against intent stage on the horizontal axis (informational to commercial) and audience on the vertical axis (patient to family member). Top-right quadrant commercial and family includes queries like detox near me, best inpatient treatment in city, insurance-specific rehab queries, and brand-name searches; the quadrant is shaded in brand red and represents the highest-converting zone where service pages and location pages compete. Mid-quadrant commercial and patient includes outpatient rehab in city, PHP in city, MAT clinic near me, and ketamine treatment city; this is mid-intent territory often family-initiated despite patient as searcher. Mid-quadrant informational and family includes how to get someone into rehab, PHP versus IOP comparison, how long detox takes, and insurance coverage questions; this is authority and AEO layer territory that drives brand recognition rather than single-page conversion. Bottom-left quadrant informational and patient is greyed and includes what to expect from rehab, what is addiction, stages of recovery, and substance-specific informational queries; this is the blog-content default with the largest content volume in the category and the lowest conversion contribution. Bottom strip: a treatment center that ranks for 30 informational queries and zero commercial queries has built brand recognition without revenue, so the build order has to start at the top right of the matrix.
Infographic titled ‘Where the conversions actually live in BH search’ showing a two-by-two matrix mapping behavioral health search queries against intent stage on the horizontal axis (informational to commercial) and audience on the vertical axis (patient to family member). Top-right quadrant commercial and family includes queries like detox near me, best inpatient treatment in city, insurance-specific rehab queries, and brand-name searches; the quadrant is shaded in brand red and represents the highest-converting zone where service pages and location pages compete. Mid-quadrant commercial and patient includes outpatient rehab in city, PHP in city, MAT clinic near me, and ketamine treatment city; this is mid-intent territory often family-initiated despite patient as searcher. Mid-quadrant informational and family includes how to get someone into rehab, PHP versus IOP comparison, how long detox takes, and insurance coverage questions; this is authority and AEO layer territory that drives brand recognition rather than single-page conversion. Bottom-left quadrant informational and patient is greyed and includes what to expect from rehab, what is addiction, stages of recovery, and substance-specific informational queries; this is the blog-content default with the largest content volume in the category and the lowest conversion contribution. Bottom strip: a treatment center that ranks for 30 informational queries and zero commercial queries has built brand recognition without revenue, so the build order has to start at the top right of the matrix.The first is the demand picture. SAMHSA’s 2024 National Survey on Drug Use and Health found that 52.6 million Americans aged 12 or older needed substance use treatment in the prior year, and only 10.2 million received any. That is an 80% treatment gap, the largest in any major healthcare category.
The unmet demand is enormous, and almost all of it is searching at the commercial end of the funnel: “treatment near me,” “rehab that takes [payer],” “[city] outpatient drug treatment.” If your site is not built to capture commercial intent, that demand routes to a competitor whose site is.
The second is the query-type behavior inside AI Overviews. Seer Interactive’s 2026 data on AI Overview triggers shows informational queries surface AI Overviews about 36% of the time, while commercial queries surface them about 8% and transactional queries 5%. Comparison queries trigger AI Overviews on 95.4% of searches; “near me” informational searches trigger them on 76.9%. Brands cited inside an AI Overview earn 35% more organic clicks and 91% more paid clicks than uncited brands.
Read those numbers together and the funnel design becomes obvious. Commercial queries still belong to the traditional blue links. Service pages, location pages, and the local SEO playbook for GBP and citations are what win those queries. Informational queries are being consolidated into AI Overviews, which means the older “rank a blog post for an educational keyword and harvest the traffic” model is degrading fast.
Blog content is shifting from a traffic asset to a citation asset, and citations help every page on your site, including the service pages, get found.
The build order that respects both data points is the order Webserv runs. Commercial first because the demand is commercial. Authority and AEO content layered second because they amplify, not replace, the commercial surfaces.
The four-layer build order
A behavioral health SEO program gets built in four layers, in this order. Skipping a layer compounds the cost of every layer after it.
Layer 1: Service pages
This is the page that captures the admission. There is one service page per distinct offering: PHP, IOP, residential, detox, MAT, dual diagnosis, trauma, and any specialty population the facility serves. Each page answers the question of what level of care it covers, who it serves, how it works, what insurance is accepted, and how to start.
Most operator sites we audit have between four and eight service pages, half of which are under 400 words, with H1s that say things like “Our Programs” or “Treatment Options” instead of the specific level of care. That is a thin-content problem and a relevance problem at the same time.
Fixing the service-page layer is the highest-ROI SEO work an operator can do, and it has to happen before anything downstream of it earns its keep.
Layer 2: Location and modality pages
Once the core service pages are solid, the next layer is geographic and modality coverage. This means location pages for the cities and metros the facility serves, modality pages for specific clinical approaches (TMS, ketamine-assisted therapy, EMDR-led residential, and similar), and insurance pages for the payers driving the most admissions.
This is the layer that captures the “service + geo” and “insurance + service” queries that make up the bulk of commercial demand.
Operators who skip from service pages straight to blog content often plateau at the regional level. They rank for the brand and the primary level of care, then nothing. The location and modality layer is what gives the site enough commercial surface area to compete in more than one market or for more than one buyer.
Layer 3: Technical foundation and internal linking
With the commercial pages in place, the next layer is the foundation under them. This is the technical SEO work: crawl health, indexation, site speed, mobile rendering, structured data, internal linking architecture, and the Google Business Profile coverage that mediates local pack visibility.
None of this work has any value on a site without commercial pages worth indexing. It has enormous value on a site that has them.
This is also the layer where a keyword strategy gets operationalized. Mapping the commercial queries to the right pages, sorting which queries belong on the PHP page versus the detox page versus the location page, and clustering the long-tail variants by intent. Without commercial pages already built, this mapping has nowhere to land. With them, it becomes the spine of every downstream optimization.
Layer 4: Blog and AEO content
Only after the commercial layers and the foundation are in place does the blog layer pay off.
This is where authority content earns external links, where 2,500-word explainers get AI Overview and ChatGPT citations, and where the long-tail informational queries that lift the entire domain’s topical authority get captured.
Blog content built on top of solid commercial pages compounds. Blog content built on a site with broken service pages does not. It might generate sessions, but the sessions do not convert because the commercial pages are not there to receive them.
How SoCal Sunrise generated 85 admissions and 2,297% ROI from SEO in 6 months
A ground-up SEO rebuild using the Pathfinder Parents Methodology turned an invisible online presence into a top-ranking admissions engine.
Read the case study →85 admits and 3,152 leads attributed to organic
What this looks like in week one versus month six
The order matters because it changes what the program is doing at every point in the engagement.
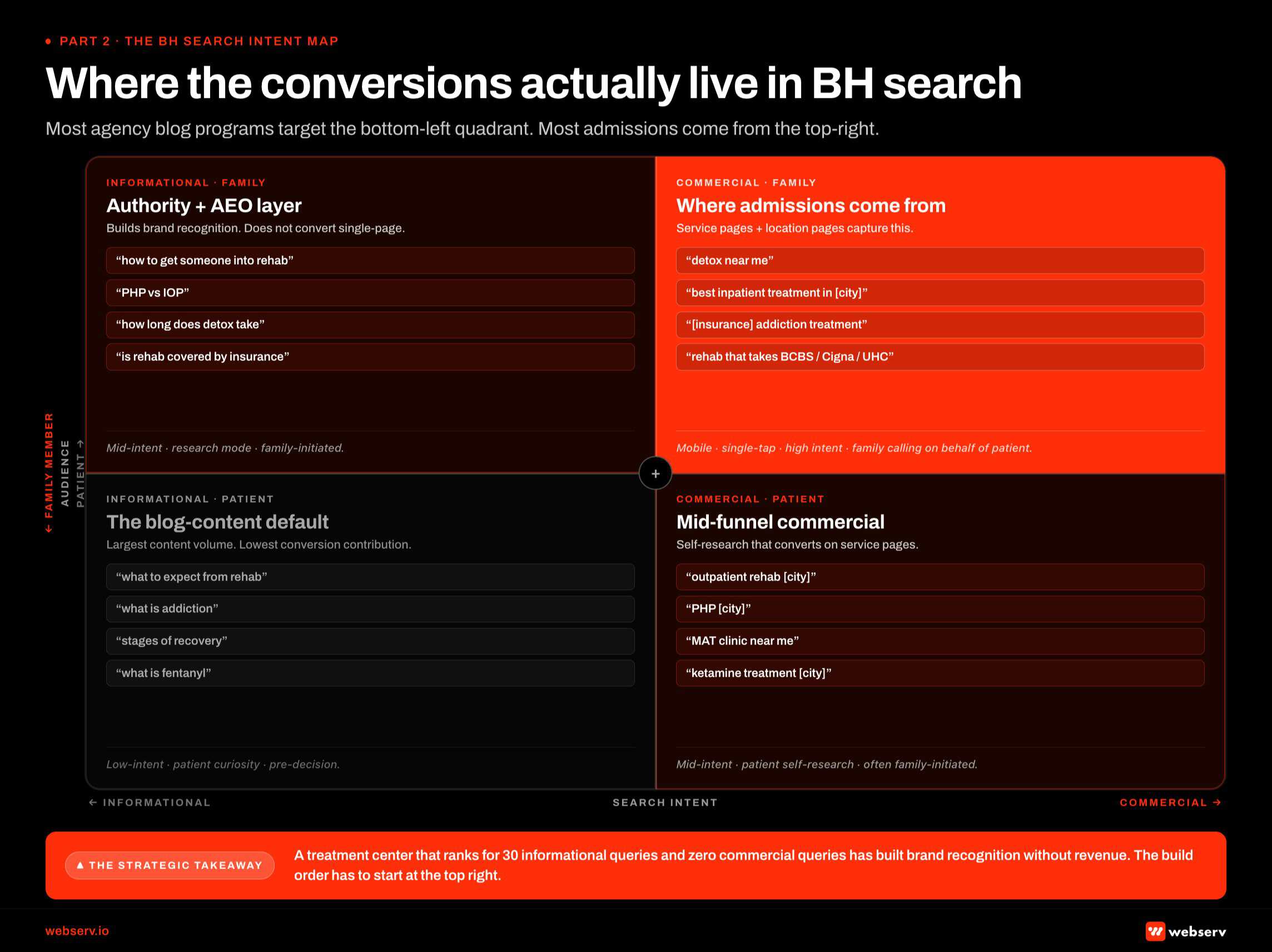
 Infographic titled ‘The cost of starting with blog content’ showing a side-by-side comparison of two 12-month SEO programs for behavioral health treatment centers, identical in spend but different in build order. Right column right order with service pages first: months 0 to 3 service and location pages go live with tech foundation and GBP coverage tightened, months 4 to 6 commercial rankings start and first organic admissions land, months 7 to 12 the program produces 3 to 8 organic admissions per month at typical Tier 2 spend with compounding pattern visible, 12-month spend of $90K to $144K, first admit timing in months 4 to 6, total 12-month admissions of 36 to 96 organic. Left column wrong order with blog content first: months 0 to 3 see 8 to 12 blog posts published with no commercial pages built and tech foundation untouched, months 4 to 6 produce informational rankings with zero commercial conversions, months 7 to 12 produce 20 to 40 thousand monthly impressions on informational queries with approximately zero admissions and the agency under pressure to defend the program, 12-month spend of $90K to $144K identical to the right column, first admit timing month 9 or later after operator forces a commercial pivot, total 12-month admissions of 0 to 6 organic. Bottom callout: the variable that produces the gap is sequence not budget, so operators paying the same monthly invoice for two different build orders walk away with two different admission counts.
Infographic titled ‘The cost of starting with blog content’ showing a side-by-side comparison of two 12-month SEO programs for behavioral health treatment centers, identical in spend but different in build order. Right column right order with service pages first: months 0 to 3 service and location pages go live with tech foundation and GBP coverage tightened, months 4 to 6 commercial rankings start and first organic admissions land, months 7 to 12 the program produces 3 to 8 organic admissions per month at typical Tier 2 spend with compounding pattern visible, 12-month spend of $90K to $144K, first admit timing in months 4 to 6, total 12-month admissions of 36 to 96 organic. Left column wrong order with blog content first: months 0 to 3 see 8 to 12 blog posts published with no commercial pages built and tech foundation untouched, months 4 to 6 produce informational rankings with zero commercial conversions, months 7 to 12 produce 20 to 40 thousand monthly impressions on informational queries with approximately zero admissions and the agency under pressure to defend the program, 12-month spend of $90K to $144K identical to the right column, first admit timing month 9 or later after operator forces a commercial pivot, total 12-month admissions of 0 to 6 organic. Bottom callout: the variable that produces the gap is sequence not budget, so operators paying the same monthly invoice for two different build orders walk away with two different admission counts.In week one, a service-pages-first program is auditing the existing service pages, rewriting the thinnest ones, fixing the wrong H1s, adding missing levels of care, and identifying the location and modality pages that don’t exist yet. The first measurable improvements show up in 30 to 60 days as the commercial pages start ranking on terms they should have been ranking on for years.
In month three, the same program is finishing the location layer, running a technical pass, and tightening the GBP coverage. Inquiries from organic search start growing because there are more commercial surfaces visible to more buyers in more geographies.
In month six, the program is producing the first authority pieces of blog and article content, targeting informational queries that map to the commercial pages already in place. Those pieces get AI Overview citations and external link mentions, both of which lift the commercial pages they reference.
Compare that to a content-first program. In week one, the agency is publishing a blog post about coping strategies. In month three, they have published twelve more. In month six, none of them rank because the site’s commercial relevance signal is weak. The agency points to traffic growth on the blog as proof of progress. Inquiries from organic have not moved. The operator is paying for activity, not outcomes.
If a treatment center pays a content agency for six months and the service pages still don’t have insurance information in them, the operator did not buy SEO. They bought a content factory.
Trevor Gage, Director of Marketing, Webserv
The pull quote is uncomfortable on purpose. Most agencies in this space sell the wrong order because the wrong order is easier to deliver against. Operators evaluating partners should ask which surface gets built first and why.
Where blogs actually pay off
This argument is not anti-blog. Blog content earns its keep, but only in the right position in the funnel.
Three things blog content does that service pages cannot:
It earns external links. Authority content is what other sites cite. A 3,000-word piece on level-of-care decision making attracts links from clinician resources, recovery community sites, and journalist references. Those links flow domain authority that lifts every commercial page on the site. A systematic digital PR program is what converts content gravity into earned media.
It captures AI Overview citations. The same content that earns external links also earns inclusion in AI Overview summaries and ChatGPT responses. As AI search consolidates the informational query layer, this citation surface is becoming the new “rank a blog post” play.
It signals topical expertise to Google’s quality systems. Google’s guidance on helpful, people-first content makes clear that E-E-A-T evaluation for YMYL categories like behavioral health rewards depth and breadth of expert content. The blog is where that depth shows up. Service pages signal commercial intent. Blog posts signal that the operator’s team actually knows the clinical and operational reality of the work.
None of those three benefits change the order. They are downstream effects that compound on commercial pages that already exist. The blog earns its keep when the commercial pages it supports are worth supporting.
Common objections to this sequence
Three objections come up consistently when operators or agencies see this argument for the first time.
The first is the topical-authority objection. The claim is that Google needs to see deep informational content before it will rank a site’s commercial pages. The data does not support this. We see treatment centers rank competitively for commercial queries inside 90 days of fixing their service pages, with zero new blog content. The topical-authority signal Google rewards on commercial pages is the depth of the commercial pages themselves, plus the local and operational signal layered around them.
The second is the link-building objection. The claim is that nobody will link to a service page, so blog content is the link-bait engine that has to come first. This conflates two different programs. The site needs external links to grow. Those links come from a digital PR program and from authority content, both of which can run in parallel with the commercial build. They do not have to come before it. They cannot replace it.
The third is the user-experience objection. The claim is that blog content makes the site useful and trustworthy to visitors. This is true, and it is also true that a thin service page makes the site untrustworthy regardless of how good the blog is. The fastest path to a trustworthy site is fixing the page someone is actually trying to admit from, not adding more material to read on the side.
Frequently asked questions about the behavioral health SEO funnel
How long does it take to see SEO results when service pages get built first?
Most treatment centers see measurable commercial-query movement within 60 to 90 days of a real service-page rebuild. The pages we touch on day one start ranking for the terms they should have been ranking on for years, because the relevance signal finally matches the intent. Inquiries from organic typically move first; full ranking lift across the cluster follows over 90 to 180 days as Google reweights the site.
That timeline is faster than a content-first program because the work is closer to the commercial query. Blog content takes 6 to 9 months to build the authority needed to rank, and even then it does not convert at the rate a service page does. Fixing the commercial layer is the shorter path to admissions, full stop.
The trade-off is that the early work is less visible. There are no flashy traffic charts in month two of a service-page program. There are pages that didn’t rank now ranking, and there are inquiries from organic that didn’t exist before. Operators who want a deck full of “content published” metrics will not love this order. Operators who want admissions will.
Do we still need a blog if we are building service pages and location pages first?
Yes, eventually, but not in month one. The blog is layer four, after commercial pages, location pages, and the technical foundation are in place. Once those layers exist, the blog becomes the authority engine that earns external links, captures AI Overview citations, and signals topical expertise to Google.
The right way to think about it is that the blog amplifies a site that is already working. It does not fix a site that is not. Operators who try to use the blog to do the commercial work end up with traffic that does not convert and a site that still cannot capture admissions.
A useful sequencing check is whether the new blog post links to a service page or a location page that actually answers the commercial query the post is anchored on. If the blog post has nowhere to send the reader because the commercial page does not exist or is too thin to convert, the blog is being asked to do a job it cannot do.
What does “service-pages-first” actually mean for our content team?
It means the content team’s first 90 days are spent rewriting service pages, drafting location pages, and producing the modality and insurance pages the site is missing. It does not mean the team stops producing content. It means the content the team produces in the first 90 days is commercial content, not blog content.
For most teams, this is a workflow change rather than a staffing change. The writers are the same people. The brief is different. Instead of “write 1,800 words on the science of addiction,” the brief is “rebuild the IOP service page with the new clinical detail, insurance information, and call paths.” The writing skill is the same. The output is closer to admissions.
Most agencies will resist this because it disrupts their content calendar and their invoicing. Operators should expect that pushback. The agencies that lean into commercial-first work tend to be the ones with admissions-focused operating models behind them. The agencies that resist tend to be the ones whose model is volume of blog posts.
Does AI search change any of this?
It strengthens the case for the order, not weakens it. AI Overviews surface most often on informational queries. They surface much less often on commercial and transactional queries, which is where admissions happen. The traditional blue-link result is still the dominant surface for the page someone actually calls from.
What AI search changes is the role of blog content. Blog content used to win by ranking number one for a head term and harvesting the traffic. Now it wins by being cited inside the AI Overview, which builds brand authority and lifts every commercial page on the site. That citation game is the new flywheel, but it runs on top of commercial pages, not instead of them.
The order is the same. The reason for the order is now reinforced by how AI search behaves.
Are there exceptions to the service-pages-first order?
A few. A facility that already has strong service pages, location pages, and a clean technical foundation can start a content program on day one because the commercial layer is not the bottleneck. A facility entering a brand-new market with no commercial pages at all should build the local commercial layer before anything else. A facility relaunching after a website rebuild needs technical work before either commercial pages or blog content can perform.
For the median operator we audit, the service-pages-first order is the right order because the commercial layer is the bottleneck. The exceptions exist; they are not the rule.
If you want to talk through where your site sits in the four-layer build, reach out for a service-page audit on the commercial layer and we will tell you exactly which pages are blocking admissions today.
The perspective in this article comes from 9 years working exclusively inside behavioral health.
We are a team built by people in recovery who understand that behind every admission is someone asking for help. If that resonates, get to know us.
Trevor Gage is the Director of Marketing at Webserv, a digital marketing agency for treatment centers.