Most digital PR sold to treatment centers is link buying with a press release wrapper. The agency takes a retainer, places a quarterly batch of paid posts on healthcare-adjacent blogs, marks the links up 3x to 5x, and reports a “PR campaign.” The links look real until Google looks at them. It is one of the most common failure modes we surface across treatment center SEO programs we inherit from another agency.
Google’s Helpful Content Updates and the SpamBrain AI system have neutralized that play. Per Google’s link spam policies, the March 2025 and December 2025 core updates explicitly demoted unattributed, generic, and AI-generated filler content in healthcare categories. Treatment centers running paid link networks in 2026 are not building authority. They are buying penalties on a delay.
Most rehab digital PR is link buying with a press release wrapper. The links look real until Google looks at them.
Trevor Gage, Director of Earned & Owned Media, Webserv
Key Takeaways
- Most digital PR sold to treatment centers is link buying with a press release wrapper. Google’s SpamBrain and the March/December 2025 core updates explicitly demoted unattributed, generic, and AI-generated filler content in healthcare categories. Paid link networks in 2026 are buying penalties on a delay.
- Real earned media is the strongest authority-building moat the industry has. Treatment centers we audit hold links from Forbes, va.gov, the American Legion, Healthline, Smithsonian, Police Magazine, and Military Families Magazine. None of those domains sell links — they cover real stories.
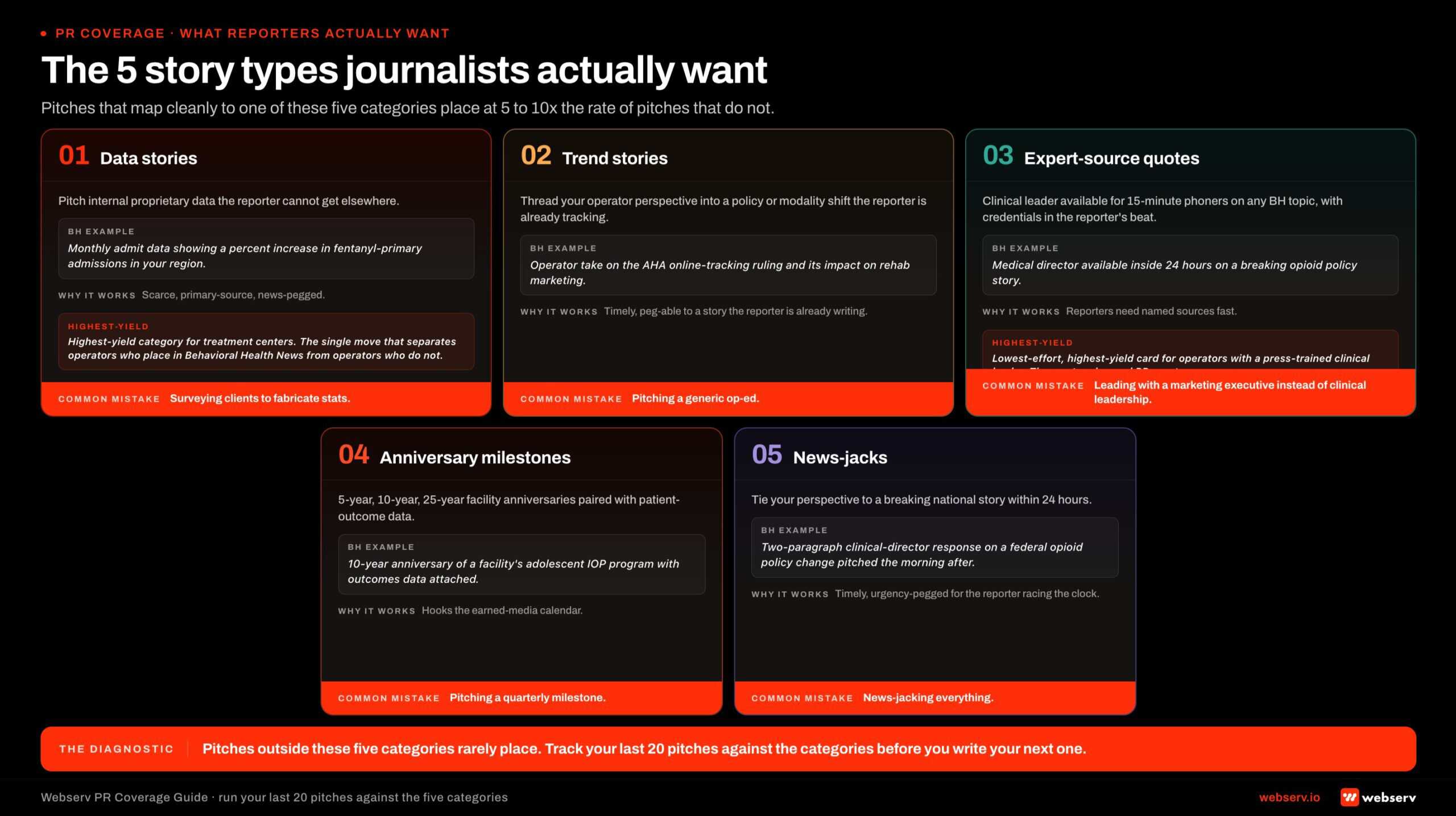
- Seven tactics produce that kind of earned coverage: original data studies, clinical leadership bylines, expert sourcing via journalist query platforms, population-specific partnerships, awards and “best of” rankings, news-cycle reactive PR, and HIPAA-respecting alumni storytelling.
- The strongest single play is proprietary data. Treatment centers sit on operational data (authorization rates, length of stay by level of care, comorbid diagnosis patterns) that journalists want and academics cannot easily access. A quarterly data report under a stable URL earns ten pickups over six months as journalists return to it.
- Measure referring domain growth from editorial sources, authority concentration in your specialization, bylined author footprint, AI citation share trend, and cost per earned placement. Placement count is theater. Most agencies report it because the better metrics expose the bought-link share.
The good news is that earned media is the strongest authority-building moat the industry has. The audits we run regularly include treatment centers with links from Forbes, va.gov, the American Legion, Healthline, Smithsonian, Police Magazine, and Military Families Magazine. Real coverage, real placements, no payments. Those domains do not sell links. They cover real stories.
This article is the seven tactics we use to build that kind of earned coverage for treatment centers. Each one has a playbook. Each one is grounded in what behavioral health publications, journalists, and award programs actually respond to. None of them involve buying links, sponsored placements without disclosure, or PBN networks.
What we mean by digital PR (and what we don’t)
Digital PR for a treatment center is earned editorial coverage that builds authority signals on your domain, the named clinical leadership, and the population specialization your program is built for. The output is real journalists writing real stories that cite your facility, your medical director, or your data. The same authority signal feeds topical authority at the domain level and shows up as one of the seven layers in our AEO guide for getting cited in Google AI Overviews and ChatGPT.
Digital PR is not:
Sponsored posts on healthcare-adjacent blogs. If a publication accepts a payment to post a piece with a link to your site and does not disclose it as sponsored content, the placement violates FTC endorsement guidelines and the link violates Google’s link spam policies.
Press release distribution with link insertions. Generic distribution services exist to satisfy the agency reporting metric. They produce syndicated copies on low-authority domains and zero earned coverage.
Guest posting on irrelevant sites for the link. Treatment center guest posts on small business blogs, generic health blogs, or unrelated lifestyle sites read as link buying to Google’s ranking systems and to journalists evaluating your brand.
Private blog networks. A PBN is a collection of domains an agency owns and uses to insert links into. Every Google core update since 2018 has been better than the last at detecting PBN networks. Treatment center sites linked from a discovered PBN can lose rankings overnight.
The tactics below all produce links Google does not penalize because Google does not read them as link building. They read as the byproduct of being newsworthy.
Tactic 1. Original research and proprietary data studies
The single most productive digital PR play in healthcare. Treatment centers sit on data that journalists want and academics cannot easily access. Quarterly outcome trends. Regional admission patterns. Insurance authorization rates. Average length of stay by level of care. Time-to-readmit data. Demographic shifts in who is seeking care.
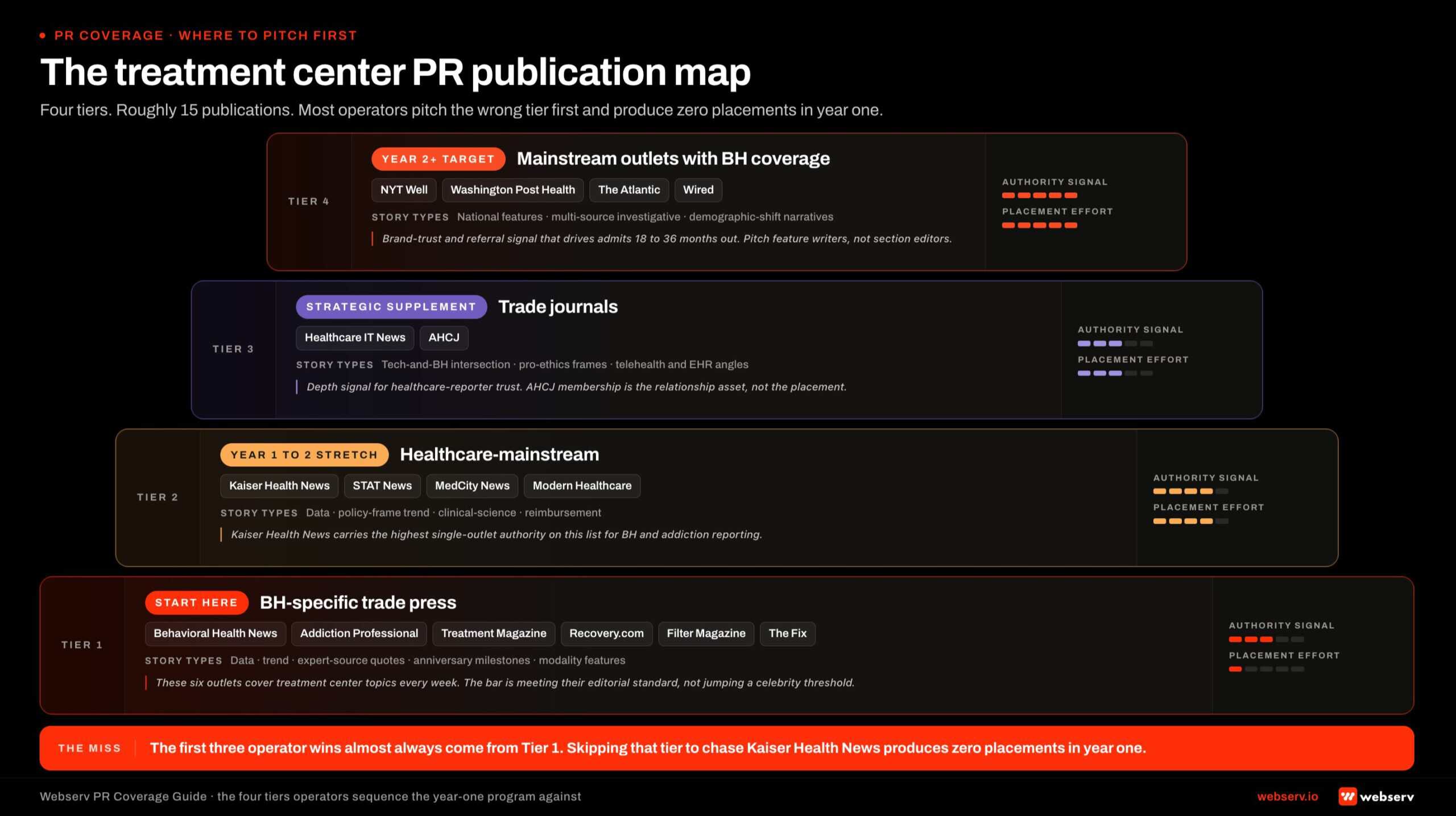
A proprietary data study turns that operational data into a publishable asset. The center publishes a report on its owned site. A press release announces the findings. Journalists at MJBizDaily, Behavioral Health Business, STAT News, Healthcare Brew, and consumer outlets like Forbes Health and the Washington Post pick up the data. Each pickup includes a link.
What this looks like in practice. The veterans and first responders program we recently audited has roughly 900 referring domains. A substantial portion of those links came in because the program publishes data about the populations it treats. The Forbes feature, the Military Families Magazine pickup, the Police Magazine coverage all trace back to data and stories that journalists could not get anywhere else.
The playbook.
Identify three to five data points your operations team already tracks that would be of interest outside the facility. Insurance authorization rates by carrier. Average length of stay by level of care. Most common comorbid diagnoses by population.
Publish a quarterly or annual report on your owned site under a stable URL. The same URL gets updated each release. Schema the report as Article with datePublished and dateModified.
Pitch the report to three vertical media outlets (Behavioral Health Business, MJBizDaily, STAT News), two consumer outlets, and any trade association that publishes for your population (VA Magazine, Police Chief Magazine, NABH publications).
Track citation share, not just placements. The same data report can earn ten pickups over six months as journalists return to it. Owned-site data reports are the single most durable digital PR asset a treatment center can build.
Tactic 2. Clinical leadership thought leadership bylines
The named medical director, the clinical psychologist, the founder with lived experience. Each one is a journalist-attractive expert source. The byline they earn in Forbes, HuffPost, Psychology Today, or Healthline links back to their bio page on your site and signals authorship credibility Google and AI search platforms both reward.
73% of top-ranking YMYL pages now display detailed author credentials. The byline footprint of a named clinician is one of the strongest EEAT signals available to a treatment center.
What this looks like in practice. The California adolescent center we audited has a medical reviewer with a PhD and LMFT credentials. The Healthline link in their referring domain set came in because that medical reviewer is a published expert. The Forbes link did the same. Real clinical leadership produces real bylines.
The playbook.
Identify the one or two members of your clinical team whose credentials and voice are journalist-ready. Medical director, lead psychologist, founder. Not everyone needs to be a public-facing expert. Pick the two who are.
Build out their bio pages on your site with full credentials, license numbers, schools, and specializations. Schema each bio as Person with Physician extension where credentials warrant.
Pitch two to three target publications per quarter. Editor inquiries, not cold guest post offers. The pitch is “Dr. [X] is available to comment on [emerging treatment trend]” or “Dr. [X] has new data on [outcomes signal].” Specific. Newsworthy. Tied to what the publication is already covering.
Repurpose every published byline on your site. Link from the bio page. Add to the clinician’s curriculum vitae. Cross-reference in your Person schema as a subjectOf published Article reference.
Tactic 3. Expert sourcing via journalist query platforms
Featured (the relaunched HARO), Qwoted, Source of Sources, Featured.com, and the smaller verticals like Help a B2B Writer. Journalists post queries asking for expert input on stories. Treatment center clinicians answer the queries. Pickups credit the clinician and link to the facility.
This is the cheapest digital PR tactic that exists. It costs the clinician’s time and the platform subscription. The placements compound because journalists return to expert sources who responded well the first time.
What this looks like in practice. A treatment center responds to a Qwoted query from a journalist writing for SELF on signs of high-functioning alcoholism. The clinician provides a quote with specific clinical detail. The piece runs with a link back to the clinician’s bio on the facility site. The journalist returns three months later for a follow-up piece on family interventions. The same clinician is the expert source.
The playbook.
Subscribe to at least three query platforms. Featured (formerly HARO) is back as of April 2025 and remains the largest. Qwoted is the highest-quality healthcare vertical. Source of Sources covers business and consumer queries with strong healthcare overlap.
Assign one team member to monitor queries daily. Twenty minutes a day, not a once-a-week sweep. The high-quality queries close fast.
Build a clinician-voice response template for the most common query types. Signs of addiction in a family member. Differences between residential and outpatient. How insurance verification works. The expert answer is faster to deliver when the structure is already drafted.
Track placements weekly. The compounding pattern is the strongest signal. A clinician who lands three placements in their first quarter will usually land twelve in the second.
Tactic 4. Population-specific partnerships and earned coverage
A treatment center built for veterans should be in regular conversation with the VA, the American Legion, the VFW, the Wounded Warrior Project, and the regional veteran service organizations.
A center built for first responders should be in regular conversation with regional police chiefs, the IAFC, the IAFF, and the national peer support coalitions.
A center built for adolescents should be in regular conversation with school district counselors, juvenile court systems, and youth-focused nonprofits.
Those relationships produce earned coverage and link equity because the partner organizations publish content, host events, and credit the centers that genuinely participate. The same partnership posture overlaps with the citation work we cover in our local SEO playbook for rehab centers.
What this looks like in practice. The veteran-focused residential program we audited has direct links from va.gov (DR 91), the American Legion (legion.org), and Military Families Magazine. None of those links were bought. They came in because the program is in real partnership with each organization. The va.gov link in particular is one of the highest-authority signals a treatment center can hold.
The playbook.
Identify the three partner organizations most relevant to your specialization. Veterans: VA, American Legion, regional VSOs. First responders: regional police chief associations, fire chief associations, peer support nonprofits. Adolescents: school district networks, juvenile justice consortia.
Invest in one partnership-grade activity per quarter. Co-host a webinar. Speak at the partner’s regional event. Co-author a clinical brief. Sponsor a peer support meeting at the partner’s facility. The work has to be real, not transactional.
Document the partnership on your site. The partner usually links back when the documentation is genuine. The partner page on your site should describe the relationship, the work, and the contact at the partner organization.
Track partner-driven coverage separately. These links tend to be high-authority and slow-decaying. One genuine VA partnership can produce three to five referring domains over twelve months.
Tactic 5. Awards and “best of” rankings as PR vehicles
Newsweek’s America’s Best Addiction Treatment Centers is the highest-impact award in the category. The 2026 survey runs through May 31, 2026. Methodology is 55% reputation (peer survey of medical professionals), 35% accreditation, 5% care services, 5% Google reviews. Statista runs the data collection. Newsweek publishes the list.
US News Best Hospitals (for treatment centers attached to hospital systems), Newsweek Best Online Therapy Platforms (for telehealth components), Forbes Health rankings, and regional rankings in publications like Boston Magazine, Texas Monthly, and Los Angeles Magazine all serve the same purpose. Earned media that produces editorial-quality links and durable brand authority.
What this looks like in practice. A treatment center recognized on Newsweek’s list typically picks up coverage in regional press, trade publications, and the parent organization’s other media properties. The single Newsweek placement compounds into eight to fifteen secondary placements over the following year.
The playbook.
Apply to every relevant award program annually. Newsweek opens its survey window each spring. The deadline is non-negotiable. Calendar the application date the day the previous year’s list is published.
Optimize the inputs to the methodology. For Newsweek specifically, reputation among medical professionals is 55% of the score. That means peer network development in your region is part of the award strategy. Active participation in NABH, ASAM, and regional behavioral health networks moves the score.
Promote every recognition on your owned site. Award badge on the homepage above the fold. Award page in the trust section. Press release through your owned distribution. Pitch trade and regional press the same week the list publishes.
Build the recognition into client-facing materials. The Newsweek badge on admissions decks, insurance pre-auth letters, and family-facing print materials creates durable brand authority outside the SEO context.
Tactic 6. News-cycle reactive PR
Behavioral health is in the news constantly. Fentanyl deaths. Veteran suicide rates. College student mental health crises. State Medicaid policy changes. New FDA approvals on addiction medications. Surgeon General advisories. Every news cycle creates a window for treatment centers to provide expert commentary.
The center that consistently produces clinician quotes within four hours of a relevant news event becomes the journalist’s default expert source over twelve months.
What this looks like in practice. When a state announces a new fentanyl policy, journalists covering the story need expert reaction within the day. The treatment center whose clinical director is reachable, has a relevant credential set, and is set up to deliver a usable quote within hours earns the citation. The competitor with a slower communications function does not.
The playbook.
Build a journalist contact list for your region and population. Beat reporters at the major regional papers. Trade press contacts at Behavioral Health Business, MJBizDaily, STAT News. Specialty publications for your population.
Maintain a rapid-response protocol. When a news event hits, the marketing team should be able to assess whether the topic warrants a response within thirty minutes and deliver an approved clinician quote within four hours.
Develop pre-approved quote templates by topic. Fentanyl policy. Veteran mental health. Adolescent substance use. The template gives the clinician 80% of a usable response. Customization for the specific news event takes ten minutes.
Track which reactive quotes earn placement. The pattern reveals which topics, which clinicians, and which publications convert. The reactive PR motion compounds: the journalists who used a quote once tend to come back.
Tactic 7. Alumni storytelling done correctly
The most powerful storytelling asset a treatment center has is its alumni. The constraint is HIPAA and the ethical reality of recovery storytelling. The play is to produce alumni narratives that respect both, distribute them through earned channels, and let the human-interest pickup do the link work.
The testimonial page on the site is a separate asset. We mean durable long-form storytelling produced for outside distribution. The framing and consent posture is part of how we approach creative strategy across all channels in this category.
What this looks like in practice. A residential program produces a documentary-style profile of an alumnus three years post-discharge, in collaboration with the alumnus and a journalist. The piece runs in a regional publication, a recovery-focused podcast, or a documentary outlet. Pickups credit the program. The story becomes a multi-platform asset that earns links from human-interest publications, recovery-focused podcasts, and trade press for years.
The playbook.
Build a structured alumni storytelling program. Identify five to ten alumni per year who are willing to share their story publicly, are stable in their recovery, and have given informed consent for HIPAA-respecting publication.
Partner with a real journalist or documentary producer for each story. The center does not produce the piece in-house. The journalist produces it, the center facilitates access, and the alumnus tells the story. The third-party authorship is what makes the resulting pickups credible.
Distribute through earned channels. Recovery-focused podcasts, regional press, documentary outlets, and trade publications for your population. The center does not publish the piece on its own site as the primary surface.
Document the storytelling program on your site. A page describing the program, the consent process, and the stories produced. The page itself earns links from journalism schools, ethics-focused outlets, and trade press covering the storytelling craft.
How SoCal Sunrise generated 85 admissions and 2,297% ROI from SEO in 6 months
A ground-up SEO rebuild using the Pathfinder Parents Methodology turned an invisible online presence into a top-ranking admissions engine.
Read the case study →85 admits and 3,152 leads attributed to organic
What to avoid
COSTLIEST MISTAKE
Buying links from healthcare-adjacent blogs that accept payment and do not disclose the placement. Google's SpamBrain detects the pattern, the links lose value, and the surrounding site loses ranking. Same failure mode from a different angle: PBN-driven link insertions. Discovered PBNs trigger manual penalties, and the cost to recover is higher than the cost of starting over. Layer on undisclosed influencer sponsorships and you have three FTC-adjacent tactics that read as manipulative to both regulators and Google.
Five patterns we audit and see fail:
1. Buying links from healthcare-adjacent blogs. The blog accepts payment, posts a piece with your link, does not disclose the placement. Google’s SpamBrain detects the pattern. The links lose value and the surrounding site loses ranking.
2. Generic press release distribution as a link tactic. Press release wire services produce dozens of syndicated copies of the same release on low-authority domains. Each copy is a duplicate. None of them count as earned media.
3. PBN-driven link insertions. An agency operates a network of domains and inserts links from them into client sites. Discovered PBNs trigger manual penalties. The cost to recover is higher than the cost of starting over.
4. Influencer-style sponsored posts without disclosure. Healthcare influencers paid to mention a treatment center without disclosing the relationship violate FTC guidelines and Meta and Google policy. The placements get pulled. The earned media value evaporates.
5. Guest posts on unrelated sites for the link. Treatment center guest posts on small business blogs or general lifestyle sites pattern-match to link buying. The links produce no authority signal and risk pulling the linked page down with them.
How to measure earned media performance
Most agencies report on placement count. That is the wrong metric.
The metrics that predict whether digital PR is building authority are:
Referring domain growth from editorial sources. Track the count of unique referring domains in tier-1 and tier-2 publications, separately from total referring domains. The latter can be gamed. The former cannot.
Authority concentration in your specialization. What percentage of new referring domains in the last 90 days are publications that cover your population specifically? A veteran rehab earning ten links from veteran-focused publications outperforms the same center earning ten links from generic health blogs.
Bylined author footprint. How many unique pieces did each of your clinical leaders publish or get quoted in over the last twelve months? The count is a forward-looking signal of EEAT depth.
AI citation share trend. How often is your center cited by ChatGPT, Perplexity, AI Overviews, and Claude on queries relevant to your specialization? The 5W 2026 AI Platform Citation Source Index shows AI citation share can shift within weeks. Earned media is the strongest predictor of which sites get cited.
Cost per earned placement. The total spend on the digital PR program divided by the count of placements that meet a quality threshold. Most agencies report cost per link including PBN-driven and paid placements. The honest version excludes those entirely.
Frequently asked questions about digital PR for treatment centers
What budget should a treatment center allocate to digital PR?
Most treatment centers running a serious digital PR program spend $4,000 to $12,000 per month, with budget scaling primarily by the depth of the original research and the number of pitch-able clinical leaders. Below $4,000 per month, the program produces occasional placements without compounding authority. Above $12,000, the budget supports original research production at a level most centers do not need to sustain.
The budget conversation should always be downstream of the asset conversation. A treatment center with no original research, no clinical thought leadership, and no awards history cannot productively spend $10,000 per month on PR outreach because there is nothing to pitch. Build the assets first, then size budget against the outreach work needed to place them.
Centers running the budget effectively typically allocate it 60 percent to asset production (research, data studies, clinical thought leadership writing) and 40 percent to outreach and relationship development. The reverse ratio (80 percent outreach, 20 percent assets) is where most digital PR programs underperform.
Should we handle digital PR in-house or hire an agency?
Most treatment centers under $20M in revenue do best with a specialist agency producing digital PR rather than in-house staffing. The journalist relationships, asset production capability, and outreach discipline take years to build and are not cost-effective to hire for at single-facility scale. Larger programs sometimes run hybrid models with in-house clinical thought leadership plus agency-side outreach.
The exception is when in-house marketing leadership has prior agency PR experience and existing journalist relationships in healthcare. We have seen mid-size programs run effective in-house PR when the lead came from a healthcare PR firm and brought the rolodex with them. Without that, in-house digital PR tends to ship a handful of low-impact placements and burn marketing-team capacity that could be better used elsewhere.
The model that consistently fails is hiring a generalist PR firm that does not specialize in behavioral health. They take the retainer, produce activity reports, place a few low-authority links, and report results in vanity metrics. The cost of those placements often exceeds the cost of a specialist agency producing fewer but higher-impact ones.
How long until digital PR shows up in admissions?
Most treatment centers see the first measurable admissions impact from digital PR between months 6 and 9. The first 90 days are typically asset production and initial outreach: original research published, clinical thought leadership bylined in healthcare publications, first journalist relationships established. Days 90 to 180 see the first earned placements compound into ranking lift on cluster pages.
The admissions attribution is rarely direct. A patient does not typically arrive at the facility because they read a New York Times piece quoting your medical director. The path is indirect: the placement builds domain authority, the domain authority lifts organic rankings on commercial pages, the commercial pages capture more qualified search traffic, and the traffic converts.
Programs measuring digital PR against direct admissions in the first 90 days will conclude it is not working. Programs measuring it against organic ranking lift on commercial pages in months 6 to 12 see the compounding effect clearly. The metric you measure determines whether you stay invested long enough to see the return.
Are paid placements ever worth it?
Sponsored content with proper disclosure on a high-authority healthcare publication can produce branding value, but the link is almost always rel=sponsored or nofollow, which means the SEO authority signal is minimal. Paid placements pitched as ‘high-DA backlinks’ typically violate Google’s link spam policies and produce penalty risk that outweighs any short-term benefit.
The category where paid placements work is awards and recognition programs from credible industry bodies (Behavioral Health News awards, CARF features, journal-affiliated recognition). These produce trust signals that families and clinicians both recognize, and the editorial review by the awarding body provides the credibility a paid blog placement never has.
The rule we follow with clients: if the link would be unattributed editorial coverage with no disclosure required, the placement is worth pursuing. If the publication requires sponsored disclosure or charges a placement fee, the value is brand awareness rather than SEO authority. Both can be worth it, but they should be budgeted differently.
How is digital PR for treatment centers different from healthcare digital PR generally?
Three differences shape treatment center digital PR. First, the audience is family members making crisis decisions, not patients researching elective procedures. Family-member-focused placements (parenting publications, employee assistance content, family-system clinical journals) produce more qualified attention than patient-focused ones. Second, the YMYL stricture is tighter than for most healthcare verticals.
Third, the regulatory environment is meaningfully more constrained. FTC enforcement on outcome claims tightened sharply after the March 2026 warning letters to substance use providers. Digital PR content has to pass legal review for any claim, statistic, or alumni story. Generalist healthcare PR firms without behavioral health experience routinely ship placements that would not clear behavioral health legal review.
The placements that work are also different. Top-tier business publications cover treatment center stories when the angle is operations, regulatory, or industry consolidation. Healthcare trade publications cover clinical innovation and policy. Local and regional outlets cover community impact. A digital PR program in this category needs to know which placement type fits which asset, which most generalist programs do not.
What the centers earning real authority actually do
Treatment center digital PR works when the center is genuinely newsworthy. The clinical leadership is real. The data is real. The partnerships are real. The alumni stories are real. The award applications are submitted on time.
The centers that earn coverage from Forbes, va.gov, Healthline, the American Legion, and Police Magazine are not the centers running the biggest digital PR retainers. They are the centers whose operations produce the news the publications want to cover.
The agency’s job is to surface what is already true about the program, package it for the audiences that should know, and place it where the right journalists can find it. The work is upstream of link building. The link is the byproduct. The same logic underpins how we build technical SEO foundation to make sure the earned coverage compounds against the rest of the SEO program rather than sitting in isolation.
If you want to talk through whether your digital PR program is earning authority or buying penalties, book a discovery call. We will audit your referring domain set and tell you what we see. Honest assessment, no pitch.
The perspective in this article comes from 9 years working exclusively inside behavioral health.
We are a team built by people in recovery who understand that behind every admission is someone asking for help. If that resonates, get to know us.
Trevor Gage is the Director of Earned & Owned Media at Webserv. Webserv works with behavioral health and addiction treatment centers on SEO, paid media, and full-funnel admissions strategy.