
Most rehab Meta accounts we audit have three of the 18 tactics below working. A few have eight. Almost none have all 18. The accounts with most of them running consistently produce cost per private-policy VOBs in the $1,800 to $2,400 range. The accounts with three to five running pay $3,500 to $5,000 for the same admit. It is the same gap we surface in every paid social audit for treatment centers we run for a new client.
The gap is not creative quality. The gap is operational discipline. Meta Ads in 2026 rewards the accounts that have built the full stack and punishes the accounts that bolted three plays onto a campaign template and called it done.
If your treatment center is running under $20K monthly on Meta, the constraints shape the playbook differently. Our 14 Meta Ads strategies for sub-$20K budgets sequences these 18 tactics for the constrained-budget context.
Three to five of these 18 will produce a campaign. Twelve will produce a profitable campaign. Eighteen will produce a campaign your competitors cannot reverse-engineer because the work is in the stack, not in the creative.
Mitch Marowitz, Director of Paid Admissions, Webserv
Key Takeaways
- The 18 tactics break into six layers: foundation (LegitScript Meta cert, HIPAA CAPI, offline VOB conversions), audience strategy (broad prospecting + income-tier + family targeting + VOB lookalikes), campaign structure (Advantage+, ad set consolidation, VOB bidding), creative volume, creative direction, and post-click + measurement.
- Accounts running 5 of 18 produce a $250-$400 Meta CPL with private-policy mix below 15% and cost per VOB above $4,000. Accounts running 18 of 18 produce a $120-$200 Meta CPL with private-policy mix at or above 25% and cost per VOB between $1,800 and $2,400. The difference is stack depth, not creative quality.
- Retargeting does not exist for SUD on Meta. The audience play is broad prospecting with structural filters (income-tier proxies, family-member targeting, VOB lookalikes). Interest stacks look targeted in the builder and underperform in practice.
- Consolidate ad sets aggressively. Five ad sets at $400/day each will optimize worse than one ad set at $2,000/day because the fragmentation splits conversion volume below the 50-events-per-week learning-phase threshold.
- Report on hook rate (25%+), hold rate (35%+), and cost per private-policy VOB at the variant level. Account-level CPL is theater. If the agency cannot produce the variant-level breakdown, that is the diagnosis.
The 18 tactics below are organized into six layers: foundation, audience strategy, campaign structure, creative volume, creative direction, and post-click plus measurement. Each tactic is short, opinionated, and field-tested across the 40+ behavioral health accounts Webserv runs in any given month.
If you audit your own account against this list and run fewer than 12 of these, you have your answer for why your Meta CPL is rising.


Foundation (tactics 1 through 3)
MOST COMMON MISTAKE
Rehab operators treat LegitScript certification as one event. It is three: LegitScript issues it, Google approves it, Meta approves it — each with a separate queue. Accounts running cleanly on Google can sit perpetually under review on Meta because the Meta-side application was never submitted. Fix is a week of paperwork. Every month you delay is a month of paid social you cannot buy.
The work that happens before the first ad ever serves. Most rehab accounts skip steps here and pay for the skip every month.
Tactic 1. Get LegitScript-certified on Meta specifically, not just Google
Most operators believe LegitScript certification is one event. It is two. LegitScript issues the certification through one workflow. Google approves it through a second workflow. Meta approves it through a third — with its own queue, dispute path, and review cycle.
We see rehab accounts that have Google running cleanly and Meta perpetually under review because the Meta-side application never got submitted. The fix takes a week. Most operators do not know it is needed until an agency audits the account.
Tactic 2. Route conversions through a HIPAA-compliant intermediary with a signed BAA
The standard Meta pixel transmits page-level signals that can be associated with health-related behavior. On a rehab website, that pattern is a HIPAA marketing compliance exposure.
The compliant stack: remove the standard pixel, route conversion events through a HIPAA-compliant intermediary (Freshpaint, Liveramp Health, or a similar tagging layer), get the BAA signed, and pass de-identified events to Meta via the Conversions API. The full mechanics are in our Meta CAPI HIPAA guide and the broader policy frame is in our HIPAA Facebook ads playbook.
No BAA on file means the engagement is not compliant. Ask any prospective agency to show you their BAA. If they cannot, they are not ready.
Tactic 3. Build offline conversion imports for VOB-level events
Form fills and lead-form submissions are the surface events Meta sees by default. The deeper signal Meta needs to optimize against admit value is the VOB outcome, which lives in your CRM.
The fix is an offline conversion import that sends VOB and approved-VOB events back into Meta through the Conversions API, with conversion values weighted ($200 lead / $2,000 VOB / $5,000 approved VOB). The architecture pattern matches what we walk through in our conversion tracking guide for addiction treatment Google Ads.
Within 60 days of this being live, Meta’s algorithm starts favoring traffic that produces VOBs over traffic that produces low-quality form fills.
Audience strategy (tactics 4 through 7)
Retargeting does not exist for SUD on Meta. The audience play is broad prospecting with structural filters layered on. The four tactics below are how that works.
Tactic 4. Default to broad prospecting, not interest-stacked audiences
Meta’s Health and Wellness ads policy kills retargeting and limits custom audience-based health targeting. The audience play is broader than most operators expect.
Run broad geo and demographic audiences with strong creative and let Meta’s algorithm do the audience finding. Interest stacks (“substance abuse” + “recovery” + “rehabilitation”) look targeted in the campaign builder and underperform in practice because the algorithm reaches the same converters faster without the constraints.
Tactic 5. Layer income-tier targeting via custom audiences
For out-of-network programs, the audience that converts is the audience with PPO coverage. PPO carriers correlate with the top 40% to 50% of household income. The bottom 50% rarely carry PPO plans.
Meta does not expose income brackets directly, but the same effect can be approximated through ZIP-code custom audiences derived from census data, lookalike audiences seeded on past private-policy converters, and education-level proxies. The income filter does not need to be a Meta input. It needs to be a layered effect.
Tactic 6. Target family members, not patients
The person searching for treatment is usually not the patient. It is the spouse, the parent, the adult child. The conversion-attribution chain in BH paid social runs through family members 60% to 70% of the time.
Build audiences explicitly around the family member profile. Parents aged 35 to 65 with adult children. Spouses with partner-search behavioral signals. Adult children of aging parents. The creative needs to address those audiences. The targeting parameters need to find them.
Tactic 7. Seed lookalikes from your offline VOB list
Standard lookalikes built from form-fill seed lists carry the same quality issues as form-fill optimization: the algorithm finds more people who look like cheap leads.
The better seed is your verified-VOB list from the CRM. The lookalike built on that seed converges faster on the audience that actually produces admits, because Meta’s algorithm is matching against the policy-verified outcome rather than the form-fill event.
Campaign structure (tactics 8 through 10)
How the account is architected determines how much budget the algorithm can effectively deploy. Most rehab accounts under-consolidate and over-fragment.
Tactic 8. Default to Advantage+ for the primary campaign
Advantage+ (the campaign format formerly called ASC) consolidates targeting, placement, and creative optimization into a single automated campaign. For BH operators, Advantage+ tends to exit the learning phase faster than manually structured campaigns because the consolidated event volume meets the 50-events-per-week threshold sooner.
This is not the right answer in every account. Tier 1 budgets ($10K to $20K) sometimes need manual campaigns for control reasons. Tier 2 and Tier 3 accounts default to Advantage+.
Tactic 9. Consolidate ad sets aggressively
Five ad sets at $400/day each will optimize worse than one ad set at $2,000/day. The fragmentation splits the conversion volume below the learning-phase threshold for each ad set.
The default architecture is one ad set per campaign with all creative variants running inside it. The exceptions are real audience splits (English vs. Spanish, distinct populations) where the conversion patterns are likely to differ enough that consolidated learning would smooth out the differences.
Tactic 10. Bid for VOB events, not form fills
If your offline conversion imports are working (Tactic 3), set Meta’s conversion goal to the VOB event, not the lead event. The algorithm will optimize against the higher-value signal and shift spend toward traffic that actually converts to private-policy VOBs.
Most BH accounts fail to ever flip this switch. The form-fill conversion goal stays in place because nobody changed it during setup. The campaign optimizes for the wrong outcome.
Creative volume (tactics 11 through 13)
Meta’s 2026 algorithm needs more creative than most operators understand. The three tactics below are the volume discipline. The full creative-investment thesis is in our guide to under-investment in rehab Facebook creative.
Tactic 11. Run 20 to 30 active creative variants minimum
Below 15 active variants, Meta’s Advantage+ system cannot run meaningful tests. The sweet spot for most BH operators is 20 to 30 active variants at any given time. Below that, the account is starved.
The variants do not need to be 30 separate productions. Ten distinct concepts each in two to three format variants (vertical video, static, carousel) gets you to 20-30 active assets without exhausting your creative budget.
Tactic 12. Refresh winning concepts every 2 to 4 weeks
Even winning creative fatigues. Operators who let a winning ad run six months are paying creative-fatigue premiums on every impression past week four.
Track frequency by creative. When frequency exceeds 4.0 on a single audience and CPL begins rising in sync, the creative is fatigued. The right response is replacement, not a frequency cap.
Tactic 13. Ship 5 to 10 new variants per week
The continuous pipeline is what separates top-quartile rehab Meta accounts from the rest. Operators who treat creative as a quarterly deliverable are running a 2019 playbook. Operators who ship five to ten new variants weekly are feeding Meta’s algorithm at the cadence it now requires.
The variants do not need to be brand-new productions. Hook swaps, open-shot changes, caption-hierarchy variations, and speaker rotations on talking-head assets all count.
How Profound Treatment drove 31 admits and a 42% drop in cost per viable in one quarter
Broad match pivot, negative keyword management, and intake-level conversion tracking turned a fragmented paid strategy into a predictable admissions engine.
Read the case study →68 viable VOBs at $4,529 cost per viable
Creative direction (tactics 14 through 16)
What the creative actually says matters as much as how much of it you produce. The three direction tactics below have outperformed in our portfolio across budget tiers and program types.
Tactic 14. Address the family member, not the patient
The strongest BH creative addresses the spouse, the parent, the adult child. The second-person diagnostic frame (“Are you struggling with addiction?”) gets flagged under Meta’s self-harm classification and underperforms even when it gets approved. The full headline-language pattern is in our compliant ad headlines guide.
The family-member frame (“When your son tells you he needs help, here is what to do next”) sidesteps the policy flag and addresses the actual audience doing the searching.
Tactic 15. Put real clinical leadership on camera
A 30-second vertical talking-head explainer from your named medical director outperforms stock-photo creative consistently. The named credential (Dr., LMFT, PhD), the real face, and the spoken delivery create trust signals Meta’s algorithm and the family-member viewer both reward.
Treatment centers with credentialed clinical leadership willing to appear on camera have a creative advantage other centers cannot replicate. The cost to produce the asset is one afternoon and one editor.
Tactic 16. Use real facility tours, not stock imagery
A 45-second phone-shot vertical tour of your actual facility, with the admissions counselor walking through real rooms, beats studio-grade stock imagery on conversion rate. The authenticity cues (real beds, real kitchen, real outdoor space, real staff) build trust at conversion.
The “diverse hand-holding circle on a beach” stock shot is dead. Every operator is running the same stock library. Real footage of your real facility is a differentiator that compounds over the life of the campaign.
Post-click and measurement (tactics 17 and 18)
The campaign delivers the click. The landing page and the reporting stack decide whether the click becomes an admit. These last two tactics are the post-click discipline.
Tactic 17. Mobile-first landing pages with confidentiality above the fold
98% of Meta users access the platform on mobile. The landing page needs to be designed mobile-first, not desktop-first with mobile fallback.
Above the fold on mobile: a clear unique selling proposition, a static call button visible during scroll, accreditation signal (Joint Commission seal, named medical director credential), and a confidentiality assurance (“100% confidential. We do not contact employers or insurers without your permission.”).
Many family members hesitate because they assume the call is not confidential. Saying so removes the hesitation.
Tactic 18. Report on hook rate, hold rate, and cost per VOB by variant
The standard agency report shows account-level CPL, click-through rate, and impression volume. None of those metrics tell you whether the creative is working.
The metrics that matter: hook rate (3-second video views divided by impressions; strong creative produces 25%+), hold rate (75% video views divided by 3-second video views; strong creative produces 35%+), and cost per private-policy VOB at the variant level.
If your report does not show those three numbers per creative variant, the report is theater. Ask for the variant-level breakdown. If the agency cannot produce it, that is the diagnosis.
Frequently asked questions about advanced rehab Meta tactics
Which of the 18 tactics moves cost-per-VOB the most?
Three tactics produce the largest cost-per-VOB lift when implemented correctly: the HIPAA-compliant Conversions API setup, the value-based optimization shift from raw lead optimization to private-policy-weighted conversion, and the creative volume scaling from 5 to 15+ active variants. Each can drop cost-per-VOB 25 to 40 percent on its own. The compounding effect across all three typically reduces cost-per-VOB by half.
The order matters. The CAPI setup is the prerequisite for everything else because without it the conversion signal is incomplete. Value-based optimization is the second priority because it shifts the algorithm’s optimization target from cheap leads to qualified policies. Creative volume is the third because the algorithm cannot optimize creative variants until the conversion signal is right.
Accounts that try to skip ahead to creative volume scaling without fixing the CAPI and conversion-value layers see modest gains. The fix sequence determines the size of the lift. Most accounts that flatten after a creative push had the underlying conversion infrastructure problem driving the issue.
How long should we wait before declaring a tactic effective?
Most Meta tactics require 14 to 21 days at meaningful spend to produce statistically reliable results, and 30 to 60 days for the compounding effects to show in cost-per-VOB. Less than 14 days produces variance noise, not signal. More than 60 days delays decisions on tactics that should be killed earlier and consumes budget that could be redeployed to working tactics.
The data thresholds matter alongside the time thresholds. A tactic running on 30 conversions across the testing window has more reliable signal than the same tactic running on 5 conversions, regardless of how many days have elapsed. Most accounts pull conclusions from conversion counts that are too small to support them.
The right discipline is to set the decision threshold (time + conversions + cost-per-VOB target) before launching the tactic. Then evaluate against the pre-set threshold rather than against in-flight intuition. Pre-commitment to decision rules is what separates a structured testing program from a reactive one.
Can we apply these tactics to Google Ads or are they Meta-specific?
Roughly half the tactics transfer cleanly to Google Ads (HIPAA-compliant conversion tracking, value-based bidding, creative-variant volume, audience exclusion logic). The other half is Meta-specific (Advantage+ campaign structure, Conversions API setup, lookalike audience construction, Meta-specific creative format strategy). The transferable layer is mostly the conversion infrastructure and account discipline.
The platform-specific tactics matter most where they apply. Google Ads has its own version of each Meta tactic that does not look the same on the surface but solves the same underlying problem. Trying to copy Meta tactics directly into Google Ads usually produces worse results than running the Google-native equivalents.
The right approach is to run both platforms in parallel with platform-specific tactical playbooks calibrated to each, while keeping the conversion infrastructure and reporting layer unified across both. The unified measurement layer is what lets the operator compare cost-per-VOB across platforms honestly. The platform-specific tactical layers are what produce the cost-per-VOB on each side.
Do these tactics work for outpatient programs or only residential?
Most of the 18 tactics work for both outpatient and residential programs, with three exceptions that need adjustment. Geographic targeting tightens substantially for outpatient (15 to 30 mile radius vs the wider radius for residential). Budget tiers are smaller for outpatient because the per-admit revenue is lower. Audience strategy shifts to local family-member targeting rather than the broader regional family-member targeting residential uses.
The conversion infrastructure layer (CAPI, HIPAA tracking, value-based optimization) applies identically to both. The creative layer applies identically too, though the angles often differ (outpatient creative usually emphasizes flexibility and ongoing care; residential creative emphasizes safety and structured environment).
The biggest risk for outpatient programs is over-applying residential tactics. Geographic and audience strategies that work for residential will inflate cost-per-VOB on outpatient because the local audience is smaller and more easily saturated. The 35 percent search impression share ceiling we describe in our paid search work applies similarly to Meta paid social for outpatient. Past saturation, additional budget produces diminishing returns.
What is the minimum monthly budget to run the full 18-tactic stack?
Most treatment centers running the full 18-tactic stack effectively spend at least $25,000 per month on Meta paid social, with the higher-impact spend tiers starting around $50,000. Below $25,000, the conversion data volume is insufficient to support all 18 tactics simultaneously, and several have to be deprioritized until budget scales. Below $15,000, the program is in foundation mode rather than full-stack mode.
The budget scaling is non-linear. A $50,000 monthly account running all 18 tactics typically produces cost-per-VOB 30 to 50 percent lower than a $25,000 monthly account running 10 of the 18, on the same audience and creative quality. The full stack reinforces itself when budget is sufficient to feed each layer.
Programs running below the full-stack threshold should prioritize the highest-impact tactics (CAPI setup, value-based optimization, creative volume) and run the remaining tactics as budget scales. The mistake is to try to run all 18 at insufficient budget. Diluted execution across 18 tactics underperforms concentrated execution on 8 of them at the same total spend.
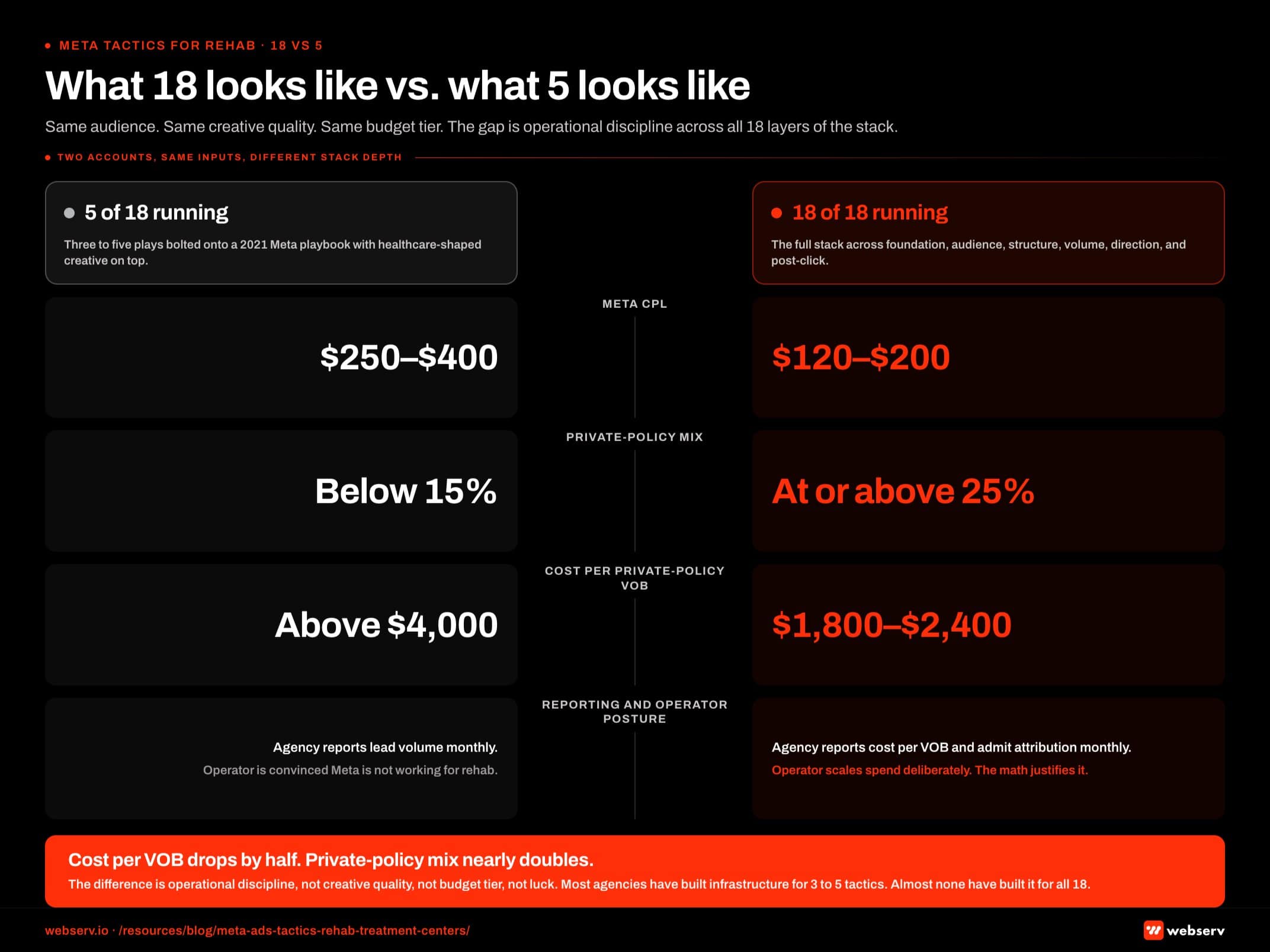
What 18 looks like vs. what 5 looks like
The account running 5 of the 18 tactics produces a Meta CPL between $250 and $400, a private-policy mix below 15%, and a cost per VOB above $4,000. The agency reports lead volume monthly. The operator is convinced “Meta is not working for rehab.”
The account running 18 of the 18 produces a Meta CPL between $120 and $200, a private-policy mix at or above 25%, and a cost per VOB between $1,800 and $2,400. The agency reports cost per VOB and admit attribution monthly. The operator is scaling spend deliberately because the math justifies it.
The difference is operational discipline across all 18 layers of the stack, not creative quality, not budget tier, not luck. Most rehab agencies have built infrastructure for 3 to 5 of them. A handful of agencies have built infrastructure for 12. Almost none have built infrastructure for all 18.
The accounts that win in 2026 are the accounts whose agency has built the stack. The accounts that lose are the accounts whose agency is running a Meta playbook from 2021 with healthcare-shaped creative bolted on top. Operators who want a head-start on identifying which firms have actually built all 18 layers can work from our curated list of paid social ad agencies for rehab marketing.
If you want to walk through which of the 18 are running in your account right now, book a discovery call. We will audit your account against this list and tell you honestly which tactics are live, which are partial, and which are missing. The audit is free. The honest answer is the deliverable, not the pitch.
The perspective in this article comes from 9 years working exclusively inside behavioral health.
We are a team built by people in recovery who understand that behind every admission is someone asking for help. If that resonates, get to know us.
Mitch Marowitz is the Director of Paid Admissions at Webserv. Webserv works with behavioral health and addiction treatment centers on paid media, performance creative, SEO, and full-funnel admissions strategy.






