A residential program we audited last year ran their entire Google Ads account through four ad groups. One was named “Rehab.” One was named “Treatment.” One was named “Detox.” One was named “General.”
Layered ad group structure assumes the account is already operating within the LegitScript and Google healthcare ads policy constraints. If you have not gone through that compliance gate yet, fix the gate before restructuring the campaigns.
Each group held between 80 and 200 keywords. The ad copy was generic across all four. The landing pages all pointed to the homepage.
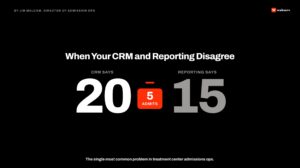
Quality Scores averaged 3 out of 10. CPCs averaged $52. The account produced 9 admits per month at a blended cost-per-admit of $4,800.
We rebuilt the structure over six weeks. The same keywords. The same budget. The same landing page domain. The work falls inside how we run paid search for treatment centers — structural rebuilds before any bidding or creative experimentation.
The discussion here assumes the account has already cleared LegitScript certification, which Google requires before any treatment center can serve Search ads. Without it, no ad group structure matters because no ads serve.
The new account had 47 ad groups. Quality Scores climbed to an average of 7 out of 10. CPCs dropped to $31. Admit volume rose to 14 per month at a blended cost-per-admit of $2,950.
Ad group structure is the architectural decision that determines what every other paid search optimization gets to stand on. Most behavioral health accounts skip it.
Mitch Marowitz, Director of Paid Admissions, Webserv
Key Takeaways
- Ad group structure is the architectural layer every other Google Ads optimization stands on. Behavioral health pays a 60–80% CPC premium at baseline, and loose structure compounds the premium until the account becomes uneconomic.
- A residential account needs to plan structure against four dimensions: search intent, treatment modality, level of care, and geography. The intersection of those four produces 20–35 ad groups for a typical mid-sized program.
- SKAGs (single-keyword) deliver the highest Quality Score but require volume to justify; STAGs (single-theme, 3–7 keywords) are the default pattern. The decision rule is data-driven — graduate any top-spend keyword inside a mixed-theme group to its own SKAG.
- A deliberate rebuild is a 4–8 week migration with a planned conversion-volume dip during cutover. The reference case moved from 4 ad groups, $52 CPC, $4,800 cost-per-admit to 47 ad groups, $31 CPC, $2,950 cost-per-admit inside a quarter.
This guide explains why ad group structure matters more in behavioral health than in most verticals. It walks through the four dimensions a residential program needs to plan against.
The back half provides a reference structure operators can adapt and outlines how to migrate from a poorly structured account to one that produces.
Why ad group structure matters more in behavioral health
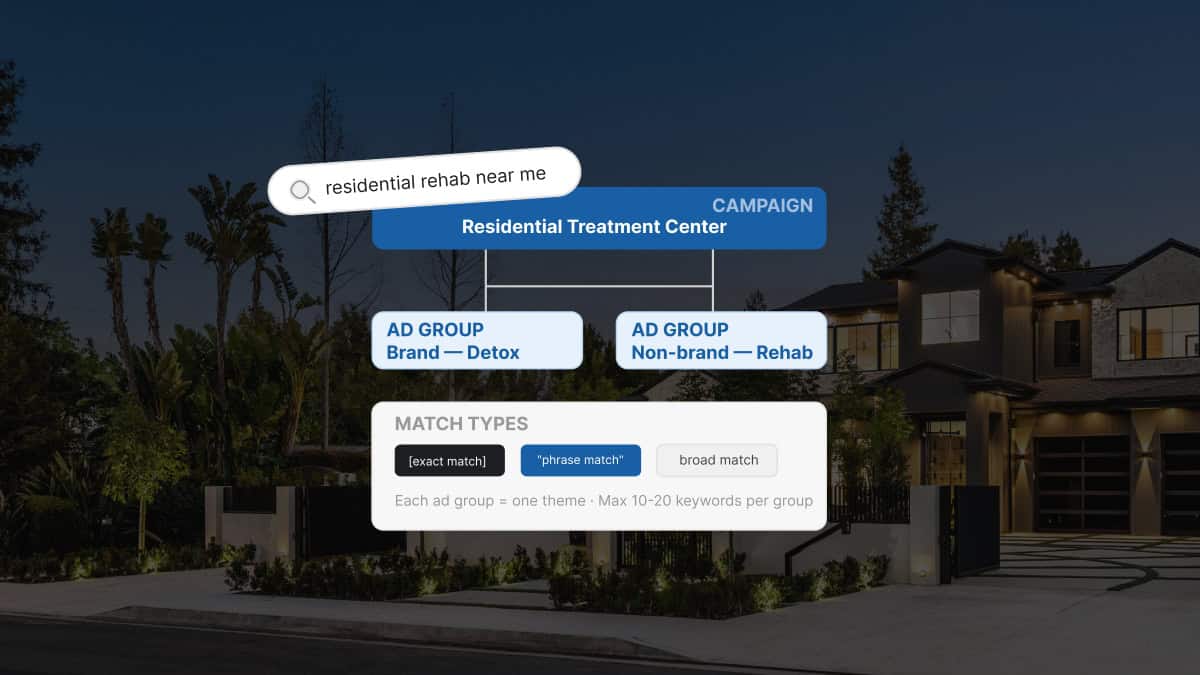
Ad group structure is how an advertiser tells Google what their account is about. Each ad group bundles a set of keywords, a set of ads, and a destination URL. The bundling is what Google scores against. Google’s official guidance on building ad groups frames it the same way — the tighter the thematic bundle, the more relevant the system reads the group as.
Tight bundles produce high Quality Scores. Loose bundles produce low Quality Scores. The CPC and serving consequences flow from there.
Most verticals can run loose bundles and still operate profitably. The CPC premium is bounded. The campaigns continue serving.
Behavioral health is different. The vertical pays a 60% to 80% CPC premium relative to non-regulated categories at baseline. Loose ad group structure compounds that premium until the campaigns become uneconomic.
The compounding works in two directions. Bad structure suppresses Quality Score — and per Google’s Quality Score documentation, the inputs that drive it (expected CTR, ad relevance, landing page experience) all degrade when an ad group bundles unrelated keywords. Bad structure also reduces the eligible inventory the campaigns can compete for. Premium positions on the search results page require both a sufficient bid and a sufficient Quality Score.
A treatment center running loose ad groups is paying more per click and getting fewer of the high-intent clicks at the prices they do pay. Structure is the lever that fixes both. It’s also the prerequisite for any compliant ad headline work to compound — tight ad groups let each headline carry the relevance signal it was written for.
The four dimensions a residential account needs to plan against
Residential treatment center accounts need to plan structure against four dimensions, and each dimension produces a different set of ad groups that has to be designed against the program’s actual mix. The combination is what makes the account work.
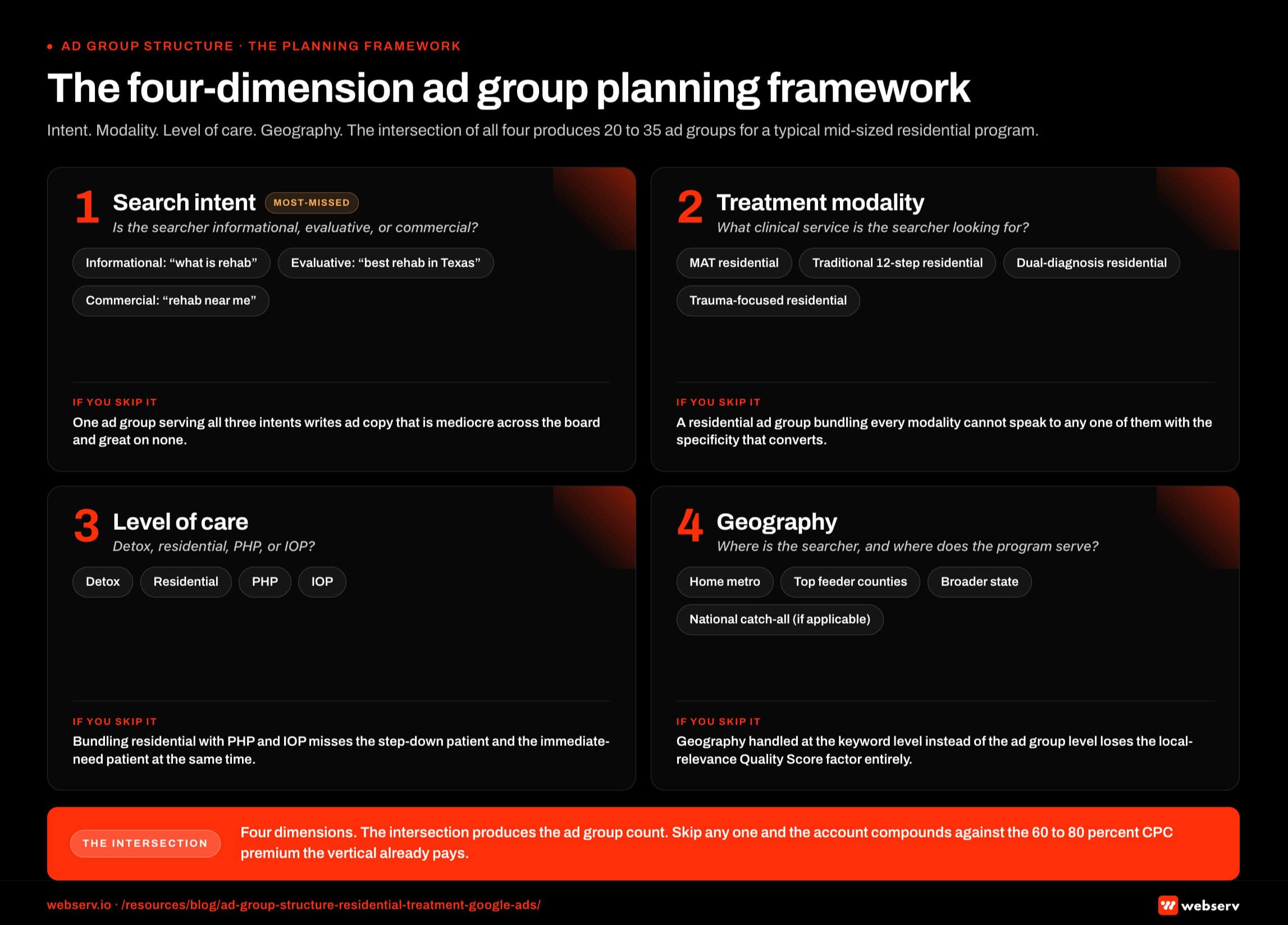
Dimension 1: Search intent. The same keyword can carry informational, evaluative, or commercial intent. “Rehab near me” is commercial. “What is rehab” is informational. “Best rehab in Texas” is evaluative.
The ad copy and landing page that score well for each intent are different. Bundling all three into one ad group produces a relevance signal that is mediocre across all of them and great on none.
Dimension 2: Treatment modality. A residential program offering MAT, traditional 12-step, dual-diagnosis, and trauma-focused care is selling four distinct services. Each one attracts different searchers. The ad group structure should reflect that.
A “MAT residential treatment” ad group performs differently than a “trauma-focused residential treatment” ad group, even within the same program.
Dimension 3: Level of care. Residential, PHP, IOP, and detox each carry different search intent and different commercial considerations. Bundling them produces ad copy that cannot speak to any one of them with precision.
Residential search intent skews toward immediate-need patients and family decision-makers. PHP and IOP skew toward step-down patients and outpatient-curious searchers. The ad copy that converts each segment is different.
Dimension 4: Geography. Residential programs serve specific catchment areas. Some attract national patients. Some run primarily local. The ad group structure should mirror the geographic footprint.
A national residential program needs separate ad groups for the home state, the top feeder states, and a national catch-all. A regional program needs separate ad groups for the metro area, surrounding counties, and the broader state.
The SKAG vs STAG decision
Two structural patterns dominate paid search account architecture, and the choice between them sets the ceiling on how much Quality Score the account can recover from a rebuild. Each has trade-offs.
Single-keyword ad groups (SKAGs). One keyword per ad group. The tightest possible relevance signal. The highest possible Quality Scores. Also the highest management overhead and the slowest data accumulation per group.
SKAGs work for high-volume, high-priority keywords where the additional Quality Score is worth the structural cost. “Residential treatment near me” might warrant a SKAG. A long-tail variant probably does not.
Single-theme ad groups (STAGs). Three to seven tightly related keywords per ad group. A balance between relevance and data efficiency. Quality Scores run slightly lower than SKAGs but data accumulation is faster, which is critical for newer accounts or smaller budgets.
STAGs are the default pattern for most behavioral health accounts. The exception is when a specific keyword is producing enough volume to justify graduating it to its own SKAG.
The decision rule is data-driven. Pull the search query report. Identify the top 10 keywords by spend. If any of them are inside an ad group with mixed themes, graduate them to SKAGs. If they are already in SKAGs, the structure is doing its job.
How Profound Treatment drove 31 admits and a 42% drop in cost per viable in one quarter
Broad match pivot, negative keyword management, and intake-level conversion tracking turned a fragmented paid strategy into a predictable admissions engine.
Read the case study →68 viable VOBs at $4,529 cost per viable
A reference structure for a residential treatment center account
The reference structure below works for a typical mid-sized residential program with one location, three to five service modalities, and a regional catchment area. Adapt it based on the specific program.
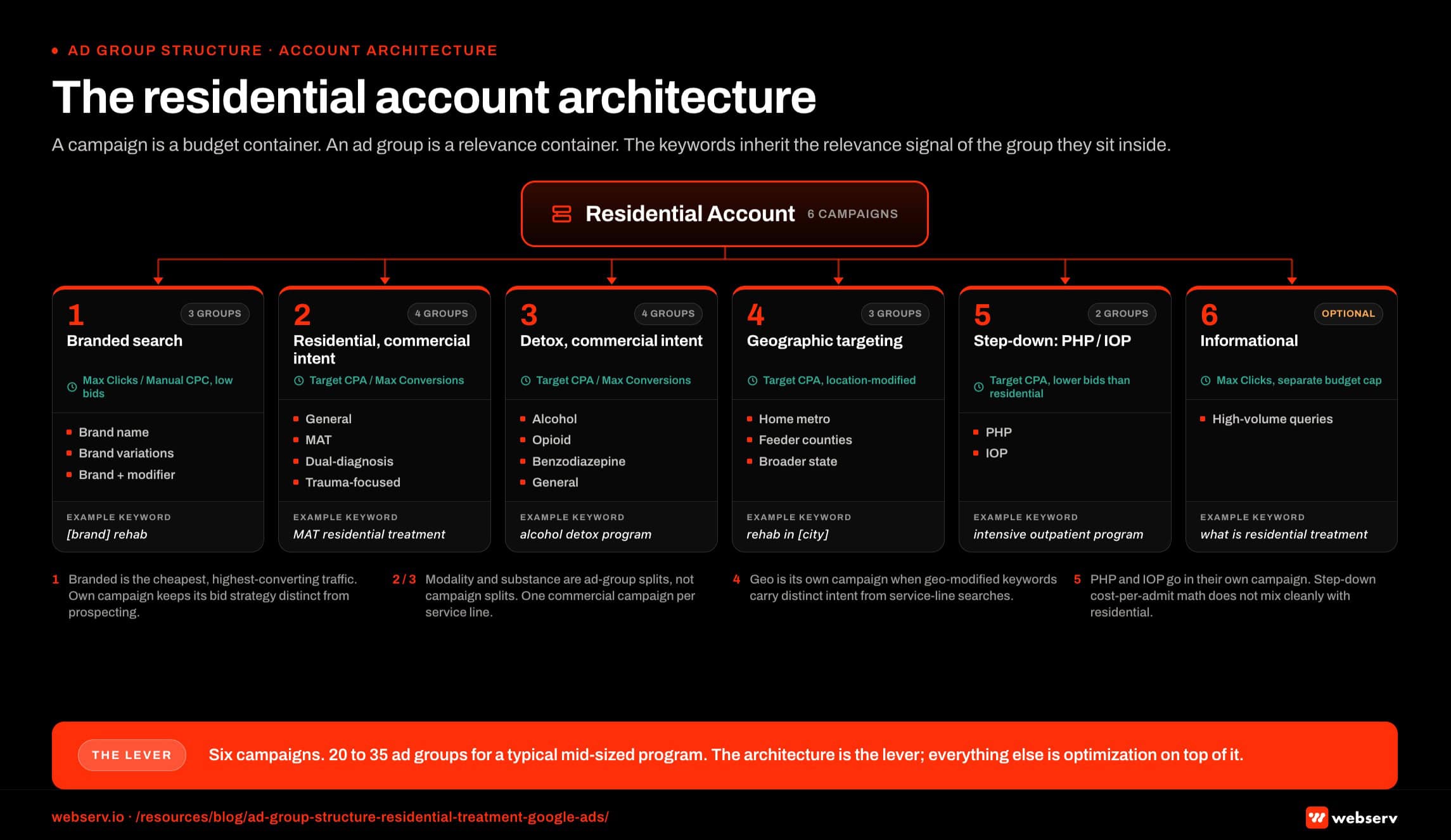
Campaign 1: Branded search. One ad group for the brand name. One ad group for brand variations and misspellings. One ad group for branded plus modifier (e.g., “[Brand] reviews,” “[Brand] cost”).
Campaign 2: Residential treatment, commercial intent. Ad groups split by modality. One for general residential. One for MAT residential. One for dual-diagnosis residential. One for trauma-focused residential. Each ad group runs phrase and exact match keywords.
Campaign 3: Detox, commercial intent. Ad groups split by substance. One for alcohol detox. One for opioid detox. One for benzodiazepine detox. One for general detox. Each ad group runs phrase and exact match.
Campaign 4: Geographic targeting. Ad groups split by region. One for the home metro. One for the top feeder counties. One for the broader state. Each ad group bids on local-modifier keywords (e.g., “rehab in [City]”).
Campaign 5: Step-down levels of care (PHP, IOP). One ad group per level of care. Tighter keyword sets. Different ad copy that speaks to step-down patients and outpatient-curious searchers.
Campaign 6: Informational queries (optional). Ad groups for high-volume informational queries that drive top-of-funnel awareness. Different bidding strategy. Different landing pages. Most residential programs do not need this campaign in the first year.
The reference structure above produces 20 to 35 ad groups for a typical mid-sized account. The exact count depends on the program’s specific mix. Each campaign’s conversion logic depends on privacy-safe conversion tracking being wired correctly so the structural Quality Score lift actually reads out in the optimization layer.
Common structural mistakes that suppress account performance
DO
- Split ad groups along intent lines: informational, evaluative, commercial each get their own group with matched copy and landing page
- Split geo at the ad group level: Austin, Houston, Dallas each get their own group with copy that names the city
- Graduate each modality (MAT, trauma, dual diagnosis) to its own ad group so copy can speak to the specific clinical hook
- Match the landing page URL to the intent and geo of the ad group, not just the campaign
DON’T
- Mix informational and commercial keywords in one ad group — Quality Score collapses across the board
- Handle geography at the keyword level with a shared generic ad — Google punishes the missing local relevance signal
- Bury modality keywords inside a general residential ad group — copy cannot speak to MAT and general residential at the same time
- Duplicate the same landing page across ad groups with different intents
Three structural mistakes surface most often in audits, and any one of them is enough to suppress Quality Score across the account and inflate CPC against the bids the program is willing to pay. Watch for these.
Mistake 1: Mixed-intent ad groups. Informational, evaluative, and commercial keywords inside the same ad group. The ad copy cannot match all three intents. Quality Score suffers across the board.
The fix is to split the ad group along intent lines. Each new ad group gets ad copy and a landing page tuned to its specific intent.
Mistake 2: Geography handled at the keyword level instead of the ad group level. “Rehab Austin,” “rehab Houston,” and “rehab Dallas” inside the same ad group with the same generic ad copy.
The fix is to split by metro and write ad copy that mentions the specific city. Local relevance is a Quality Score factor, and Google rewards it.
Mistake 3: Modality keywords mixed with general residential keywords. “MAT residential” and “trauma residential” inside the same ad group as “residential treatment.” The ad copy cannot speak to the specific modality without losing relevance for the general term.
The fix is to graduate each modality to its own ad group with modality-specific ad copy. The general residential ad group keeps the general keywords and the general copy. The same modality discipline shows up on the Meta side — it’s the prerequisite for running HIPAA-compliant Facebook ads at any meaningful scale, because the targeting and creative both need a clean group-level anchor.
How to migrate from a bad structure to a good one
Migrating from a poorly structured account to a well-structured one is a 4 to 8 week project for a typical mid-sized program. The work is real but the payoff compounds for the lifetime of the account.
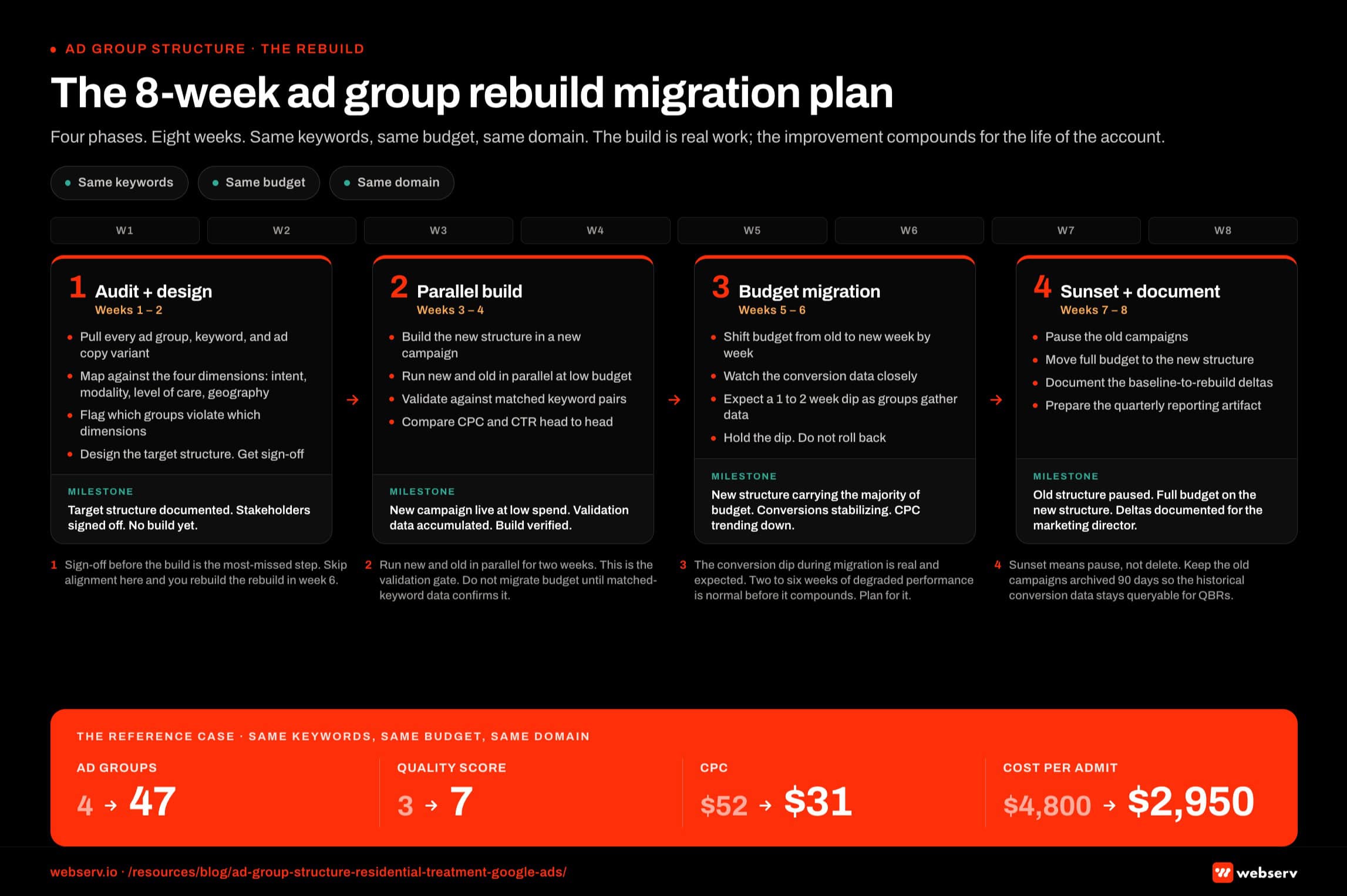
Week 1: Audit the existing structure. Pull every ad group, every keyword, and every ad copy variant in the account. Map them against the four-dimension framework above. Identify which ad groups are violating which dimensions. Cross-reference against the compliance mistakes that suppress rehab Google Ads to catch the language-level issues that sit on top of the structural ones.
Week 2: Design the target structure. Use the reference structure as a starting point and adapt to the program’s specific mix. Document the new campaign-to-ad-group-to-keyword hierarchy. Get sign-off before building.
Week 3 and 4: Build the new structure in a new campaign. Run the new structure in parallel with the old one for 2 weeks at low budget to validate the build. Compare CPC and CTR against the old structure on matched keyword pairs.
Week 5 and 6: Migrate the budget. Shift the budget from the old structure to the new structure week by week. Watch the conversion data closely during the shift. The new structure should produce more clicks per dollar at equivalent or better conversion rates.
Week 7 and 8: Sunset the old structure. Pause the old campaigns. Move the budget fully to the new structure. Document the baseline-to-rebuild deltas for reporting.
The migration period is the highest-risk window in the project. Conversion volume can dip during the cutover as the new ad groups accumulate impression data and Google’s predicted CTR signals stabilize. Plan for the dip and budget through it.
What success looks like at twelve weeks
A residential treatment center that rebuilds ad group structure deliberately should see measurable improvement inside a quarter.
The starting point is the audit. Document the current ad group count, the average Quality Score, the average CPC, and the cost-per-admit. These are the baseline metrics the rebuild will be measured against.
Weeks one through eight cover the migration. By the end of week eight, the new structure should be running at full budget. CPC should be trending down, though not yet at the new floor.
Weeks nine through twelve are the stabilization period. Quality Scores continue rising as Google accumulates impression data on the new structure. CPC continues falling. The full effect of the rebuild is visible by week 12.
The center we worked with finished the rebuild at 47 ad groups, a 7 average Quality Score, $31 CPC, and $2,950 cost-per-admit. The starting point was 4 ad groups, 3 QS, $52 CPC, and $4,800 cost-per-admit.
The relative improvement matters more than the specific numbers. A residential program operating with deliberate ad group structure should see a 30% to 50% reduction in CPC and a corresponding lift in admit volume at the same budget.
What to ask your paid search partner this week
Three questions surface whether a paid search partner is operating with the right ad group discipline. Ask them.
First, ask how many ad groups are in the account today. If the answer is fewer than 15 for a residential program with multiple modalities and a meaningful budget, the structure is too loose. More than 100 ad groups can be a different problem: over-engineering that creates data sparsity.
Second, ask the partner to walk through the logic behind the current ad group structure. A serious answer references intent, modality, level of care, and geography. A vague answer indicates the structure was inherited rather than designed.
Third, ask what the average Quality Score across the account looks like and whether the partner has a plan to improve it through structural work. If the answer focuses on bidding tactics rather than structure, the partner is treating symptoms instead of the cause.
Ad group structure is the architectural decision the rest of the account stands on. Most behavioral health programs run loose structures because the work to fix it is unglamorous and slow. The fix is closeable inside a quarter, and the savings compound for years. Book an intro call and we’ll walk through what a rebuild would look like for your account.
Frequently asked questions about Google Ads structure for residential treatment
How many ad groups should a typical residential account have?
Most residential treatment center accounts run cleanly with 12 to 25 ad groups across 4 to 6 campaigns. Below 10 ad groups, the account is usually too broad and Quality Score drags across the board. Above 30 ad groups, the account is usually over-segmented and individual groups starve for data.
The right number depends on the program’s clinical specialties, insurance contracts, and geographic footprint. A single-location program serving 5 primary substances and 4 primary payers can run effectively at 15 to 20 ad groups. A multi-location program serving the same substance/payer set needs 25 to 40 because location adds a multiplier.
We size ad groups against minimum traffic volume. Each ad group should produce at least 30 to 50 clicks per month within 60 days of launch to give Google’s algorithm enough signal to optimize. Groups below that floor get consolidated or paused.
Should we restructure if our current campaigns are performing?
Usually yes, but carefully. Performance in a poorly structured account is often the floor, not the ceiling. We have seen accounts producing acceptable cost-per-admit at 4 ad groups improve 30 to 50 percent after restructuring to 16 to 20. The performance gain is from Quality Score lift and cleaner audience signal, both of which require structural change to access.
The risk is the restructure dip. Migrating from poor structure to good structure resets the algorithm’s learning, which produces 2 to 6 weeks of degraded performance before the new structure starts compounding. Operators who restructure during a critical census quarter sometimes regret the timing.
The safer pattern is phased restructuring. Build the new campaign structure alongside the existing one, run both in parallel for 2 to 4 weeks, then migrate budget over once the new structure has stable conversion data. The cost is a few weeks of duplicate spend, paid back in months of better performance.
How does ad group structure affect Quality Score?
Quality Score is calculated at the keyword level but heavily influenced by ad group cohesion. Ad groups where keywords, ad copy, and landing page all align on a single search intent produce higher Quality Scores than ad groups that mix substances, levels of care, or geographies. The lift is meaningful: Quality Score from 5 to 8 typically reduces CPC by 30 to 50 percent.
The mechanism is relevance. Google rewards tight keyword-to-ad-to-landing page matches because they produce better user outcomes. An ad group containing ‘opioid detox,’ ‘alcohol detox,’ and ‘inpatient rehab’ as keywords cannot produce ads that satisfy all three search intents simultaneously, so Quality Score for each suffers.
The fix is structural, not creative. Splitting that ad group into three (one per substance/service) lets each group write tight ad copy and route to a specific landing page. Quality Score climbs within 30 days of the split as the new groups accumulate impression data.
Do we need separate campaigns per level of care?
For most residential programs, yes. PHP and IOP have different search intent, different audience qualification (insurance, geographic radius), and different cost-per-admit economics than residential. Mixing them in a single campaign forces the algorithm to compromise on bid strategy and audience signal.
The exception is programs where one level of care dominates. A program where 90 percent of admits are residential can run PHP and IOP as ad groups inside the residential campaign rather than as separate campaigns. Below that concentration, the campaign-level split usually pays for itself in performance.
Geographic level-of-care splits matter too. Programs serving multiple states often split campaigns by state because state-specific insurance regulations and patient mobility patterns affect what should bid where. A national PHP campaign rarely outperforms state-segmented PHP campaigns.
What is the right campaign budget allocation across ad groups?
Campaign budgets in Google Ads are allocated at the campaign level, not at the ad group level. Within a campaign, the algorithm distributes spend across ad groups based on impression opportunity and conversion likelihood. Operator control happens through bid strategy at the keyword level and campaign budget caps at the top.
The implication is that ad group performance imbalance inside a campaign is usually a signal rather than a budget problem. If one ad group consistently captures 60 percent of campaign spend and produces 80 percent of conversions, that group probably deserves to be its own campaign. If one ad group consistently captures 60 percent of spend but produces 20 percent of conversions, that group has a Quality Score or audience problem to fix.
We rebalance budgets by adjusting campaign-level spend caps and keyword-level bids quarterly. The right ratio is whatever produces the lowest cost-per-admit. We do not move budget on monthly variance; we move it on quarterly trend confirmation.
The perspective in this article comes from 9 years working exclusively inside behavioral health.
We are a team built by people in recovery who understand that behind every admission is someone asking for help. If that resonates, get to know us.
Mitch Marowitz is the Director of Paid Admissions at Webserv. Webserv works with behavioral health and addiction treatment centers on paid media, SEO, and full-funnel admissions strategy.