A treatment center we audited last quarter had an average Quality Score of 0.85 across their entire Google Ads account. Same keywords as their main competitors. Same bid range. The CPCs they were paying ran 60% to 80% higher than the market.
The cause was Quality Score, which most operators treat as an opaque Google-internal scoring system. The score is opaque, but the components are not. Each one has specific levers, and each one in behavioral health faces vertical-specific drag that does not exist in other industries.
We rebuilt that center’s QS over a quarter. The keyword list did not change. The budget did not change. CPCs dropped from $48 to $29. The campaigns produced 2.4 times more clicks for the same spend.
The lazy approach to Quality Score in behavioral health is to accept that healthcare just costs more. The right approach engineers each QS component for the constraints of the vertical. The CPC delta between those two postures is 50% to 100%.
Mitch Marowitz, Director of Paid Admissions, Webserv
This guide explains what Quality Score actually is, what each of its three components measures, why each one is harder to optimize in behavioral health, and the practical levers operators can pull to bring CPCs into the range a clean account should be paying.
Key Takeaways
- Quality Score is a keyword-level 1-to-10 diagnostic that determines both whether the ad serves and what the advertiser pays per click. Two accounts running the same keywords at the same bids can have CPCs 60% to 80% apart based on QS alone.
- Three components feed Quality Score: expected click-through rate, ad relevance, and landing page experience. Each one faces vertical-specific drag in behavioral health: language constraints depress expected CTR, intent-mixing depresses ad relevance, and HIPAA-compliant tracking architecture depresses landing page experience signals.
- LegitScript certification gates ad serving entirely. The compliance language that earns the certification also lowers expected CTR, which is a structural trade-off that has to be engineered around, not eliminated.
- The premium is closable in a quarter. A treatment center that audits QS, rebuilds ad group structure, rewrites ad copy to match keywords, and engineers HIPAA-compliant landing pages can drop CPCs 30% to 50% on the same bids and budget.
What Quality Score actually is
Quality Score is Google’s diagnostic for how relevant and useful an ad and its landing page are to the user who searches a given keyword. The score is calculated on a 1-to-10 scale at the keyword level inside a Google Ads account.
The score does three things simultaneously. It influences the ad rank that determines whether the ad serves at all.
It modifies the actual cost-per-click the advertiser pays relative to their bid. It affects the eligible inventory the campaign can compete for, including premium positions on the search results page.
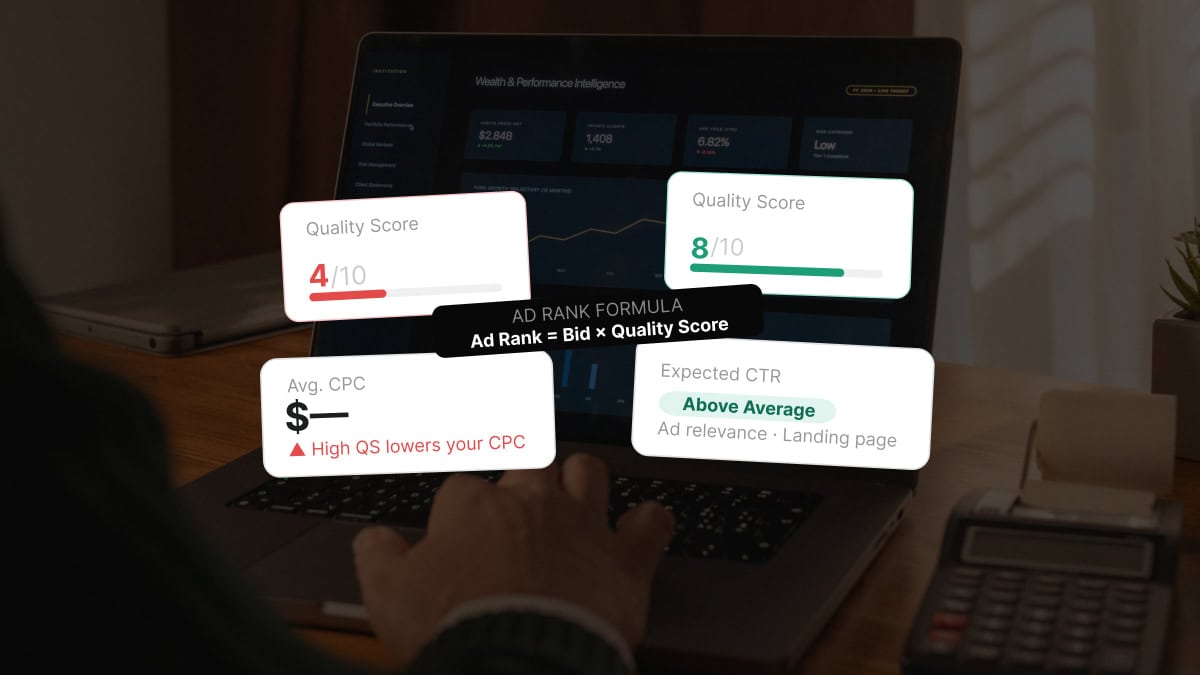
The simplified version of the math: a higher Quality Score means the advertiser pays less per click and shows in better positions. A lower Quality Score means the advertiser pays more per click and shows in worse positions or does not show at all.
Quality Score is calculated against three components: expected click-through rate, ad relevance, and landing page experience. Each component is reported as Above Average, Average, or Below Average inside the Google Ads interface.
That reported state is the visible surface. The underlying math is more granular. Two keywords with the same three component states can have actual Quality Scores that differ by 30% or more depending on the deeper signals Google evaluates.
The three components and what they measure
Expected click-through rate. Google’s predicted likelihood that a user who sees the ad for the given keyword will click it. The prediction is based on historical CTR for the keyword within the account, plus signals from the broader auction including ad copy patterns, position, and seasonality.
Ad relevance. How closely the ad copy matches the search intent of the keyword that triggered the auction. Google measures this through semantic analysis of the keyword, the ad headlines, the description lines, and the destination URL.
Landing page experience. Google’s evaluation of how well the destination page serves the user who clicked. This includes content relevance to the keyword and ad, page load speed, mobile usability, transparent navigation, and the absence of intrusive interstitials or misleading elements.
The three components are evaluated independently, but they interact. A landing page experience problem can suppress the predicted CTR. An ad relevance issue can drive down landing page experience signals if the wrong audience is arriving on the page.
For Google’s full mechanics, each component combines into a final keyword-level Quality Score that is updated as new data arrives. The system never stops re-evaluating.
Why each component faces vertical-specific drag in behavioral health
Expected CTR drag. Behavioral health ads operate under stricter language constraints than most verticals. Words that drive CTR in non-regulated categories trigger reviews in healthcare.
Direct outcome claims, urgency framing, and emotional language are the highest-CTR levers in many industries and the most heavily constrained in this one.
Ad copy that complies with Google’s healthcare policies and LegitScript expectations tends to be more neutral, which produces lower expected CTR before the auction even runs.
Ad relevance drag. Treatment centers often run keywords across a wide range of intent, from informational (“what is opioid addiction”) through evaluative (“dual diagnosis treatment Austin”) to commercial (“opioid rehab admissions”).
Tight ad-to-keyword relevance requires careful campaign structure. Most accounts we audit lump keywords together at the ad group level, which produces the relevance drag that suppresses QS across the board.
Landing page experience drag. This is the largest source of QS drag in behavioral health. HIPAA-compliant tracking architecture often requires consent prompts, neutral URL paths, and stripped pixel implementations that affect Google’s measurement of page experience.
Healthcare landing pages also carry mandatory legal and clinical disclaimers that increase page weight and reduce content relevance signals. The pages have to be deliberately engineered to score well despite these constraints.
The cumulative drag across all three components is what produces the 60% to 80% CPC premium most behavioral health accounts pay relative to non-regulated competitors targeting similar query volumes. That premium is closable.
How LegitScript certification interacts with Quality Score
LegitScript certification is the gating credential for treatment center advertising. It is also a Quality Score factor in ways that are not always obvious.
Certified status enables ad serving. Without LegitScript certification, the ads do not run at all in healthcare-restricted categories. Quality Score becomes irrelevant because the inventory is closed.
Approved keyword set is constrained. LegitScript-certified accounts can run a specific set of keywords in healthcare-restricted categories. Keywords outside that set are blocked, regardless of Quality Score. This indirectly affects QS measurement because the certified account is operating against a smaller, more curated keyword universe.
Compliance review affects ad relevance scoring. Ads that pass LegitScript review tend to be more conservative in language. The conservatism is what scores well on compliance and what underperforms on expected CTR. The trade-off is structural.
Mid-cycle revocation kills QS instantly. If LegitScript certification is revoked mid-cycle and Google catches the lapse, the account loses both serving eligibility and its accumulated QS history. Recovery after re-certification often requires rebuilding QS over months, even after the account is technically eligible to serve again.
The interaction is real and program-specific. A serious paid search audit on a behavioral health account always includes a LegitScript compliance check alongside the Quality Score analysis.
Practical levers for each component
Levers for expected CTR. Tight keyword-to-ad-group structure (one tightly themed group per intent cluster). Ad copy that uses the keyword in the H1 of the ad.
Sitelinks and structured snippets that match the keyword theme. Negative keywords that exclude irrelevant traffic and protect the historical CTR signal.
The compliance constraint means the copy will never match an unrestricted vertical, but a deliberately structured account closes most of the gap.
Levers for ad relevance. Single-keyword or single-theme ad groups (SKAGs/STAGs). Three to five responsive search ad headlines per ad group, each tightly mapped to the keyword theme.
Description lines that elaborate on the headline rather than introducing new themes. Final URL set to a landing page that mentions the keyword in the H1.
Levers for landing page experience. Page load speed under 2.5 seconds on mobile, validated through Google PageSpeed Insights. Mobile usability with clear primary CTAs above the fold.
Compliance-required disclaimers placed in the footer rather than in the main content area. Tracking architecture that uses a HIPAA-compliant intermediary to avoid direct PHI transmission while still firing the conversion events Google needs to score the page.
Levers that work across all three components. Quarterly QS audits at the keyword level. Active negative keyword lists. Bid strategy that rewards Quality Score (manual CPC or maximize conversions, not maximize clicks).
The numbers agencies quote you mean very different things depending on payer mix.
Before you benchmark your performance or compare quotes from other agencies, read this. Real data from real OON treatment center campaigns with no cherry-picked numbers.
Read the report → Free and ungatedHow CPC compounds with Quality Score in this vertical
The CPC math compounds in behavioral health in ways that operators outside the vertical do not always recognize.
A non-regulated vertical paying $5 per click at QS 7 might pay $7 per click at QS 4. The competitive disadvantage is real but bounded. The campaign continues running.
The same QS 4 in a healthcare-restricted category often produces a different outcome. Ads stop serving on premium queries because the system requires both QS and policy approval to clear at higher thresholds.
The CPC math does not get a chance to play out because the impression volume drops first.
This is why behavioral health accounts that ignore Quality Score sometimes report “high CPCs” without realizing the deeper issue. The CPCs they see are the impressions that did serve. The impressions that did not serve at all are invisible in the report.
The cumulative effect across a quarter is the difference between a campaign that produces consistent admit volume and a campaign that runs at half its potential reach for the same monthly spend.
What success looks like at twelve weeks
A treatment center that engineers Quality Score deliberately should see measurable improvement inside a quarter.
The starting point is an audit. Pull the QS for every keyword in the account. Identify the keywords scoring 1 to 4 and tag them as the priority remediation set. Identify the keywords scoring 7 to 10 and use them as the structural template for the rebuild.
Week one through four covers the structural work. Rebuild ad groups around tighter keyword themes. Rewrite ad copy to mention the keyword in the H1 and structure the rest around the search intent.
Update landing pages to load faster, comply with HIPAA tracking architecture, and reference the keyword in the page H1.
Week five through eight is the data collection period. The new structure needs impression volume to update its expected CTR signals. Quality Score will shift gradually rather than overnight. Resist the urge to keep changing the structure during this window, because each change resets the data collection clock.
Week nine through twelve is the evaluation phase, when the comparison against baseline becomes meaningful. Compare the new QS to the baseline. Compare the new average CPC to the baseline. Compare the click volume at the new average CPC to the click volume at the prior average CPC.
The center we worked with started this process at $48 average CPC and finished at $29. The work is real. The result compounds over time as Quality Score signals strengthen with continued data.
What to ask your paid search partner this week
Three questions surface whether a paid search partner is operating with the right Quality Score discipline.
First, ask for the average Quality Score across the account. If the partner cannot pull it in 5 minutes, the metric sits outside their operating cadence, which is the root cause of most behavioral health CPC inefficiency.
Second, ask which keywords are scoring 1 to 4 and what the remediation plan is for each one. Specific answers indicate active management. Vague answers indicate the partner is paying the QS premium without trying to recover from it.
Third, ask how the partner thinks about the LegitScript and HIPAA constraints in the context of Quality Score optimization.
A serious answer references the trade-offs and the levers that work despite the constraints. A generic answer indicates a partner who is treating the account the same way they treat ecommerce or B2B SaaS.
Quality Score is the metric that determines whether a treatment center pays $29 or $48 per click for the same keyword and the same bid. Most operators never look at it.
The fix is closeable in a quarter, and the foundation it builds is what every other paid search optimization gets to stand on.
The perspective in this article comes from 9 years working exclusively inside behavioral health.
We are a team built by people in recovery who understand that behind every admission is someone asking for help. If that resonates, get to know us.
Mitch Marowitz is the Director of Paid Admissions at Webserv. Webserv works with behavioral health and addiction treatment centers on SEO, paid media, and full-funnel admissions strategy.