I’ve been having the same conversation on every sales call for the last six months. The operator on the other end of the phone is hurting on Google.
CPAs are up, reimbursements are down, and the search campaigns that worked two years ago are facing higher CPCs with cost-per-admit rising accordingly in 2026. So I bring up paid social for behavioral health.
And about 70 percent of the time, the response is some version of “we tried Meta, it didn’t work.”
What that response actually means, almost every single time, is that the operator’s admissions team wasn’t built to handle Meta leads. The campaign was fine. The targeting was fine. The creative was fine. The leads came in.
Then the admissions person treated them like Google leads, reached out twice, and quit.
The treatment centers winning admissions on Meta Ads in 2026 share one trait: they treat Meta as a separate workflow with its own follow-up cadence, its own admissions training, and its own expectations. The ones losing on Meta share the opposite trait.
This article is about how to tell which one you’re going to be before you spend the money.
Key Takeaways
- Google PPC in 2026 is harder than at any point in the last five years. CPAs are up, reimbursements are down, auction inventory is crowded, and the campaigns that worked in 2023 are producing materially fewer admits at the same spend.
- Meta delivers cheaper leads but the follow-up cadence is roughly 10x what Google requires. A Google lead converts on two or three contacts. A Meta lead frequently needs ten or more.
- Paid-channel inoculation periods extended in 2026. Google paid search now takes about six weeks to settle (up from four), and Meta inoculation runs around two weeks depending on spend. Operators using 30-day trial windows are pulling the plug before either channel has produced a fair read.
- Operators who fail on Meta typically fail at admissions handling, not at the campaign layer. The single biggest determinant of Meta-program success is how fast the admissions team responds to the lead. Near-immediate, not five-minute.
- Top performers on Meta share one trait. Immediate text follow-up plus a persistence cadence of ten-plus contacts is the floor, not the ceiling.
- The right move in 2026 is Meta plus Google, not Meta instead of Google. Each channel produces a different lead psychology. The admissions team needs a workflow for each.
- Stop evaluating Meta on Google’s economics. The CPL is lower. The follow-up cost is higher. The net cost-per-admit math still favors a Meta-plus-Google program for most operators who do the admissions work.
What changed for treatment center PPC in 2026
Operators who built their paid program in 2022 or 2023 are running into the same wall in 2026. The CPAs they used to see are gone. The campaigns that once produced reliable admit volume now produce inconsistent leads at higher cost. Three things compounded to make this happen.
First, the Google Ads auction got more crowded. Big spenders absorbed more inventory. Mid-size operators bidding against private-equity-backed national rollups are getting outbid on the same intent terms they used to win.
The shared auction is no kinder to small operators than the inventory math allows.
Second, reimbursements compressed. The patient who admits today produces less revenue than the equivalent admit produced 18 months ago. The cost-per-admit you can absorb at a 60 percent collection rate is materially different from the cost-per-admit you could absorb at 75 percent.
Most operators haven’t recalibrated their target CPAs to account for this.
Third, the entire 2026 paid environment is sitting under the AI-Mode shift Google rolled out at I/O 2026. AI Overviews are absorbing query intent that used to drive clicks.
The paid auction below the AI answer is being asked to do more work, against a smaller click pool, with the same budget.
This is industry-wide, not Webserv-specific. People who know me reach out and ask what’s going on with their Google campaigns. Multi-vendor operators talk about it on the call. Everyone is feeling the same compression.
The operators producing the best 2026 results are the ones who recognized the shift early and started moving spend.
The cleanest move for most treatment centers is to add Meta to the channel mix without cutting Google. The full paid social playbook for treatment centers covers the channel architecture in operational depth.
The short version: Meta is cheaper per lead, requires more admissions work per lead, and produces a different family-of-the-patient buyer than Google does.
The four objections we hear most about Meta
The same four objections come up in basically every sales call where Meta is on the table. They are all reasonable on the surface. They are all wrong in ways that matter.
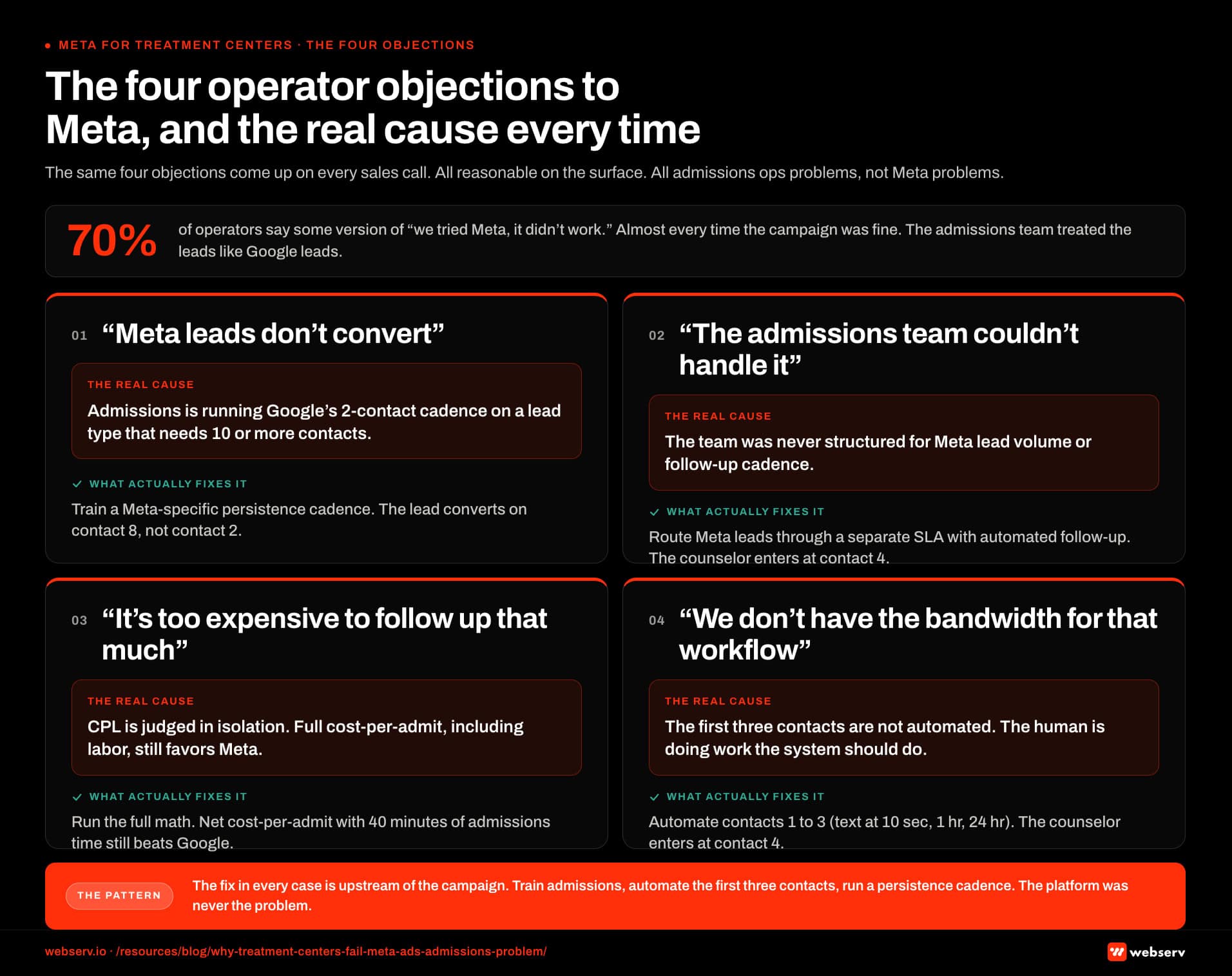 admissions operations cause for each. Panel 1 objection ‘Meta leads don’t convert’: what the operator is reporting is that leads come in but admissions cannot close them; the real upstream cause is that the admissions team is running Google’s two-contact cadence on a lead type that needs ten or more contacts; what actually fixes it is training admissions on a Meta-specific persistence cadence because the lead converts on contact eight, not contact two. Panel 2 objection ‘We tried it and the admissions team couldn’t handle it’: what the operator is reporting is that volume overwhelmed a team built for Google inbound; the real upstream cause is that the team was never structured for Meta lead volume or follow-up cadence, and operators who fixed this dropped cost-per-admit 30 to 50 percent in 90 days; what actually fixes it is routing Meta leads through a separate SLA with automated immediate follow-up where the admissions counselor enters at contact four. Panel 3 objection ‘It’s too expensive to follow up that many times’: what the operator is reporting is that ten contacts per lead feels like unsustainable labor; the real upstream cause is that the cost-per-lead math is being evaluated in isolation, and the full cost-per-admit including admissions labor still favors Meta; what actually fixes it is computing the full math because net cost-per-admit on Meta with 40 minutes of admissions time still beats Google by a wide margin. Panel 4 objection ‘We don’t have the bandwidth for that workflow’: what the operator is reporting is that the intake counselor is already over capacity; the real upstream cause is that the first three contacts have not been automated and the human is doing work the system should be doing; what actually fixes it is automating contacts one through three with a text inside ten seconds, a text inside the first hour, and a text at twenty-four hours, with the counselor entering at contact four when the lead has self-selected. Top strip: 70 percent of operators Mitch talks to say some version of ‘we tried Meta, it didn’t work,’ and almost every time the campaign was fine because the admissions team treated the leads like Google leads. Bottom strip: the fix in every case is upstream of the campaign, train admissions, automate the first three contacts, run a persistence cadence; the platform was never the problem.” class=”wp-image-24957″/>
admissions operations cause for each. Panel 1 objection ‘Meta leads don’t convert’: what the operator is reporting is that leads come in but admissions cannot close them; the real upstream cause is that the admissions team is running Google’s two-contact cadence on a lead type that needs ten or more contacts; what actually fixes it is training admissions on a Meta-specific persistence cadence because the lead converts on contact eight, not contact two. Panel 2 objection ‘We tried it and the admissions team couldn’t handle it’: what the operator is reporting is that volume overwhelmed a team built for Google inbound; the real upstream cause is that the team was never structured for Meta lead volume or follow-up cadence, and operators who fixed this dropped cost-per-admit 30 to 50 percent in 90 days; what actually fixes it is routing Meta leads through a separate SLA with automated immediate follow-up where the admissions counselor enters at contact four. Panel 3 objection ‘It’s too expensive to follow up that many times’: what the operator is reporting is that ten contacts per lead feels like unsustainable labor; the real upstream cause is that the cost-per-lead math is being evaluated in isolation, and the full cost-per-admit including admissions labor still favors Meta; what actually fixes it is computing the full math because net cost-per-admit on Meta with 40 minutes of admissions time still beats Google by a wide margin. Panel 4 objection ‘We don’t have the bandwidth for that workflow’: what the operator is reporting is that the intake counselor is already over capacity; the real upstream cause is that the first three contacts have not been automated and the human is doing work the system should be doing; what actually fixes it is automating contacts one through three with a text inside ten seconds, a text inside the first hour, and a text at twenty-four hours, with the counselor entering at contact four when the lead has self-selected. Top strip: 70 percent of operators Mitch talks to say some version of ‘we tried Meta, it didn’t work,’ and almost every time the campaign was fine because the admissions team treated the leads like Google leads. Bottom strip: the fix in every case is upstream of the campaign, train admissions, automate the first three contacts, run a persistence cadence; the platform was never the problem.” class=”wp-image-24957″/>“Meta leads don’t convert”
What’s actually true is that Meta leads don’t convert on Google’s follow-up cadence. A Google paid-search lead is a person who typed an intent query into a search box and clicked through to your landing page. They are mid-funnel by the time they fill out the form.
A Meta lead is earlier in the journey. They saw an ad while scrolling. They self-identified by clicking. They are not yet in the same buying state as the Google lead. The cost-per-admit math works if the admissions team does the additional work to bridge that gap.
It does not work if the admissions person calls twice and gives up.
“We tried it and the admissions team couldn’t handle it”
This is the most honest objection on the list. Most admissions teams are not built to handle Meta lead volume on a Meta lead follow-up cadence. They are built to handle inbound calls from Google clicks.
The fix is not to abandon Meta. The fix is to train the admissions team, automate the immediate follow-up, and route Meta leads through a different SLA than Google leads.
The operators we work with who made this shift saw their cost-per-admit on Meta drop 30 to 50 percent within 90 days. The ones who didn’t make the shift cut Meta and blamed the platform.
“It’s too expensive to follow up that many times”
The math on this is wrong in both directions. Yes, ten contacts costs more admissions labor than two contacts. No, that does not make Meta more expensive than Google when you compute the full cost-per-admit.
A Meta lead, with a 10-contact follow-up cadence and patient admissions ops, often produces a cost-per-admit competitive with a Google lead that converts faster but costs several times more on the media side. Run the numbers on your own data before you decide.
The economics shift with level of care, in-network versus out-of-network status, and geography.
The admissions overhead is real. The media savings are bigger.
“We don’t have the bandwidth for that workflow”
This is the operator-honesty version of the previous objection. The admissions team is small. The intake counselor has too much on their plate. Adding a 10-contact cadence on Meta leads to an already-stretched team is a real operational concern.
The answer is to automate the first three contacts. An automated text firing inside 10 seconds of form submission, a second text inside the first hour, and a third inside the first 24 hours can all run without admissions-counselor labor.
The admissions counselor enters the workflow at contact four, when the lead has self-selected by responding. The bandwidth concern is real, and the answer is engineering, not avoidance.
What a treatment-center-ready Meta program actually requires
If you are evaluating whether your operator setup can run Meta at scale, the four operational requirements below are the floor. Programs that ship without one of these consistently underperform. Programs that ship with all four consistently outperform Google-only operators at the same spend level.
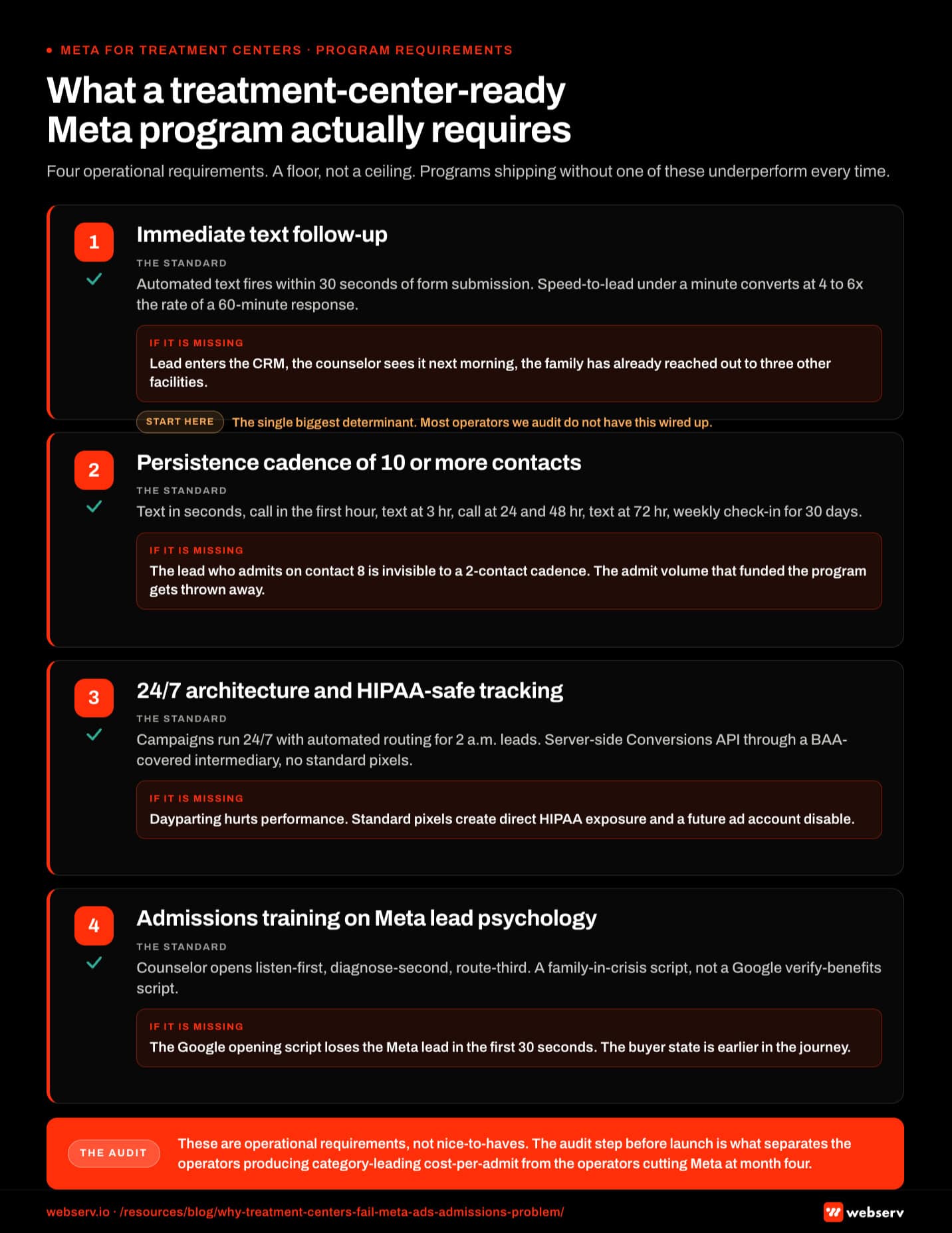
Immediate text follow-up (under 30 seconds)
The single biggest determinant of Meta program success is whether the lead gets an automated text within seconds of form submission. Not a phone call. A text. Phone calls from unknown numbers get ignored. Texts from a treatment center get read.
Speed-to-lead inside one minute converts at four to six times the rate of speed-to-lead at sixty minutes.
Most operators we audit do not have automated text follow-up wired up. The lead form fires, the lead enters the CRM, and the admissions counselor sees it the next morning. By then the family member has reached out to three other facilities and the comparison is over.
Persistence cadence of ten-plus contacts
The follow-up does not end after the first text.
The treatment centers winning on Meta run a structured cadence: an automated text inside seconds of submission, the first human call attempt inside the first hour, text at three hours, and call at 24 hours.
The cadence continues with a call at 48 hours, text at 72 hours, then a weekly check-in cadence for the next 30 days.
The lead that admits on contact eight is invisible to the operator running a two-contact cadence. The lead exists. The opportunity exists. The admissions team that gives up after contact two is throwing away the admit volume that funded the program.
24/7 campaign architecture with text automation backing it
Meta campaigns run 24/7. You can dayparting-restrict them but that hurts performance. A working program accepts that leads will come in at 2 a.m. and routes them through automated text immediately. The admissions counselor enters the workflow during business hours when the lead has self-selected by responding.
The HIPAA-safe tracking architecture underneath all of this is non-optional. Standard Meta pixels firing on a treatment center site create direct HIPAA exposure. The right pattern routes through server-side Meta Conversions API with a BAA-covered intermediary.
Operators who skip this layer run the same paid program with a disabled ad account in their future.
Admissions training on Meta lead psychology
Meta leads do not sound like Google leads on the phone. The Google lead has done the comparison research. They know what level of care they need. They are calling to verify benefits. The Meta lead is earlier. The family member is in crisis.
They have not yet figured out the level of care. They are looking for someone to help them figure out what comes next.
The admissions counselor handling a Meta lead opens the conversation differently. They listen first. They diagnose the situation second. They route to the right level of care third. The same scripts that work for Google leads will lose Meta leads inside the first 30 seconds.
How Profound Treatment drove 31 admits and a 42% drop in cost per viable in one quarter
Broad match pivot, negative keyword management, and intake-level conversion tracking turned a fragmented paid strategy into a predictable admissions engine.
Read the case study →68 viable VOBs at $4,529 cost per viable
The inoculation reality across paid channels
The inoculation period is the window between launch and stable cost-per-admit performance. Both Google paid search and Meta have seen that window stretch since 2024, and the gap shows up in operator evaluation conversations every month.
Google paid search inoculation extended from around four weeks in 2024 to about six weeks in 2026 as match-type behavior shifted and Smart Bidding signal periods lengthened.
Meta inoculation runs around two weeks depending on spend, up from a faster pre-2025 baseline, after healthcare advertisers were moved into a sensitive category framework and audience targeting restrictions tightened.
Operators who quit at four weeks on Google now do so just before the campaign was about to find its footing. Operators who pull Meta after 10 days are pulling it just before the optimization signal stabilizes.
The contracting implication is straightforward. A 30-day Meta trial is not a fair test of the channel in 2026. A 90-day trial is the minimum useful evaluation window. Operators who write 30-day exit clauses into their paid social agreements are setting up a self-fulfilling failure pattern.
The same dynamic applies when an existing campaign is heavily restructured. Major changes to audience, creative, or conversion event reset the optimization signal and the inoculation clock starts over. Operators who keep iterating in the first 30 days never let the campaign mature.
The economics: media savings versus admissions ops cost
The honest version of the Meta-versus-Google math has three lines. The cost-per-lead is lower on Meta. The cost-per-admit is competitive once the admissions workflow is dialed in. The total program economics favor running both channels with admissions ops sized to handle each lead type.
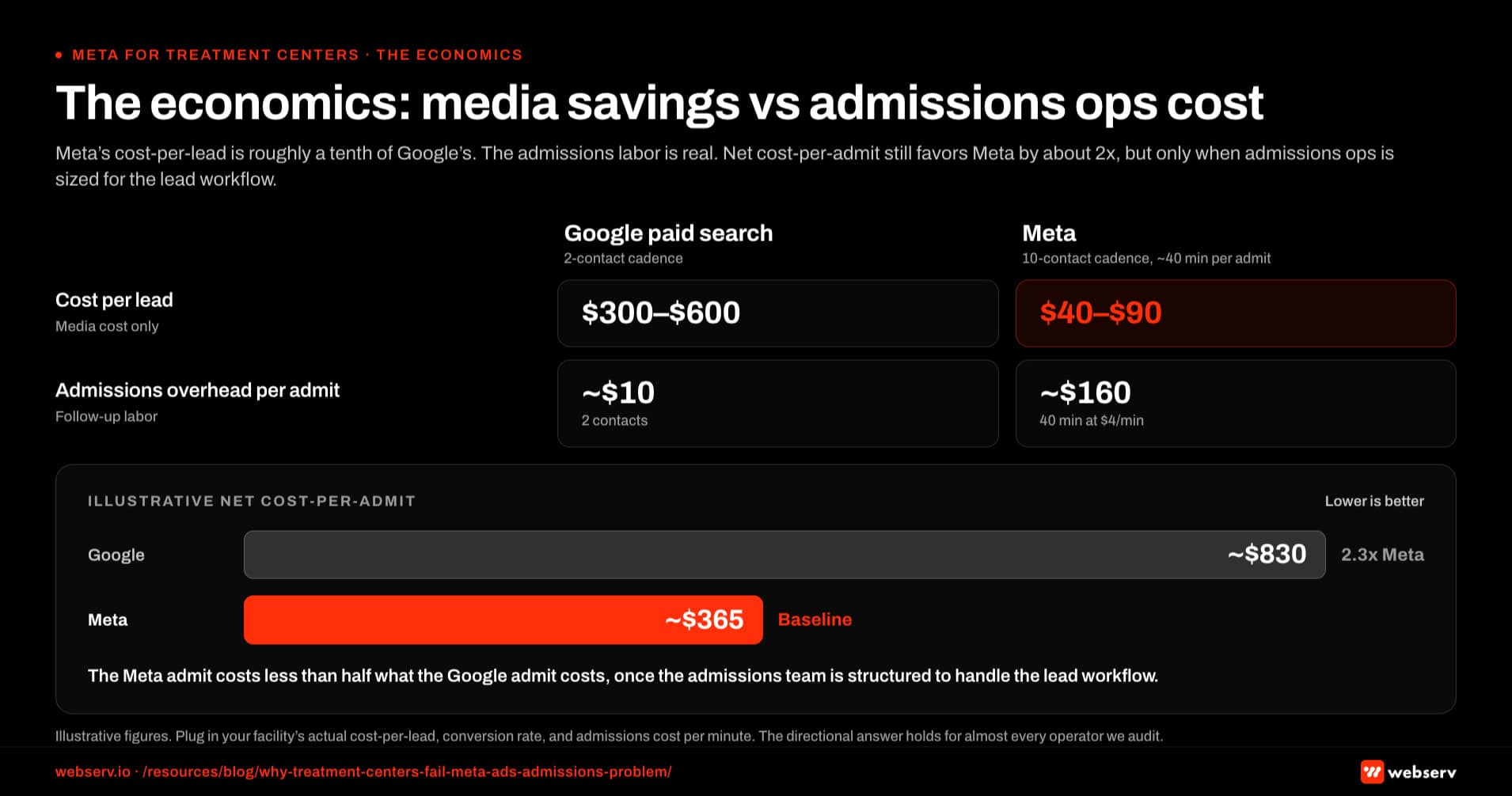
The directional ranges for a typical 2026 mid-size operator look like this. Google paid search for high-intent treatment-center queries tends to land in the range of $300 to $600 cost-per-lead, with cost-per-admit ranging from $3K to $15K depending on level of care, in-network versus out-of-network status, and geography.
Meta lands at $40 to $90 cost-per-lead, with cost-per-admit also in the $3K to $15K range under the same variables. The CPA range is wide on purpose. Where you land inside it is a function of admissions ops as much as media performance.
Meta admits carry more admissions labor than Google admits. A 10-contact cadence at four minutes per contact is roughly 40 minutes of admissions time per converted Meta lead. That labor is real cost.
Whether you charge it back to the channel as cost-per-minute or absorb it into fixed overhead, Meta’s lower CPL pays back only when the admissions operation is sized to handle the extra contact load.
The Google admit costs roughly $10 of admissions overhead at a 2-contact cadence.
Net cost-per-admit including admissions ops: Google at roughly $830, Meta at roughly $365. The Meta admit costs less than half what the Google admit costs once the admissions team is structured to handle it.
Operators who skip the admissions structuring step never see this math.
Verify the numbers on your own facility. Plug in your actual cost-per-lead, your actual conversion rate, and your actual admissions cost per minute. The exact figures change. The directional answer holds for almost every operator we audit.
Where Meta belongs in the channel mix
This is not a Meta-instead-of-Google argument. The treatment centers winning admissions in 2026 run both channels with a clear allocation pattern and admissions ops structured to handle each lead type. The right split depends on operator scale.
For Tier 1 operators (under $50K total paid monthly), Meta typically sits at 25 to 35 percent of paid spend.
The admissions team is small, the Meta workflow has to be tightly automated, and the program leans on Google for the high-intent traffic the admissions counselor can convert without the full 10-contact cadence.
For Tier 2 operators ($75K to $150K total paid monthly), Meta typically sits at 40 to 55 percent of paid spend. The admissions team is structured enough to run the persistence cadence at scale. The media savings on Meta funds additional volume without hitting Google’s auction ceiling.
For Tier 3 operators ($200K to $500K total paid monthly), Meta typically sits at 50 to 60 percent of paid spend. At this scale, Google’s auction starts producing diminishing returns above a certain spend level. The marginal admit gets cheaper on Meta as the admissions team scales its capacity.
The full channel-mix framework sits inside the broader behavioral health marketing umbrella we publish. The framework treats paid as one pillar of a five-pillar program. Meta is the most consequential paid channel for most operators in 2026, but it does not stand alone.
How we coach clients into a working Meta program
The procedure we run with new paid social clients at Webserv has four steps. The order matters. Skipping any step produces the same failure pattern operators see when they hire a generalist agency.
Step one is the admissions readiness audit. Before we touch the ad account, we look at how the admissions team handles inbound. We audit speed-to-lead, the follow-up cadence, the script the counselor uses, and the CRM workflow.
If the admissions side is not ready, we say so before any media dollar gets spent.
Step two is the HIPAA-safe tracking architecture. The HIPAA-compliant Facebook Ads stack walks through the technical pattern. Server-side Conversions API through a BAA-covered intermediary is the minimum.
Operators who skip this layer face ad account disables and HHS-OCR exposure. Meta’s official Conversions API documentation sets out the server-side parameters and event-deduplication rules required for the integration to send valid attribution signals without exposing PHI through standard browser pixels.
Step three is the campaign architecture. We structure the account around the buyer persona the operator’s facility actually serves. For residential and PHP programs, that means family-member voice and creative built for the parent or partner. For outpatient programs, that means patient-direct creative.
Mixed-acuity facilities run both in parallel campaign structures.
Step four is the creative production cadence. Meta’s algorithm performs best with roughly 12 active creative variants per campaign, refreshed every six to eight weeks.
The treatment centers we work with who underinvest in Meta creative production cadence starve the algorithm of the signal it needs to optimize.
The pattern is engineered, not improvised. We do not skip steps because the operator wants to start spending faster. The 30-day delay from a proper admissions audit produces 90 days of better admit volume on the back end.
Every operator we’ve seen skip the audit has come back later asking us to rebuild what the early launch broke.
Common mistakes that kill Meta programs at treatment centers
COSTLIEST MISTAKE
Cutting Meta at month four is the failure pattern we see most. Six mistakes cluster together: no server-side conversion API, no HIPAA-compliant intermediary, creative fatigue from under-investment, admissions ops not trained on lower-intent Meta leads, no first-party audience seed, and no learning phase completion before optimization. Any two of those in combination cap program performance at 40 to 50 percent of what the same media budget produces once the setup is fixed. The right move on a struggling Meta program is a diagnostic, not a shutdown.
Six failure patterns show up consistently in treatment center Meta programs that underperform. Recognizing them upstream of a campaign restart is the difference between a program that compounds and one that gets cut at month four.
Operators evaluating Meta for the first time tend to run into mistakes 1 through 3. Operators restarting Meta after a failed attempt typically run into 4 and 5. Mistake 6 is universal and underrated.
Sub-$20K operators have an additional set of constraints. The shortcuts that make smaller programs work sit in our broader paid social tactics coverage for operators below that spend tier. Operators ready to outsource the build can start from our shortlisted paid social ad agencies that handle the compliance stack, which filters out the generalist shops that produce the failure patterns above.
Frequently asked questions about Meta ads for treatment centers
Should we run Meta if our admissions team is small?
A small admissions team can run Meta if the immediate follow-up is automated and the admissions counselor enters the workflow at contact four when the lead has self-selected by responding. The bandwidth concern is real, and the solution is engineering, not avoidance.
The operators we work with who have two-person admissions teams successfully run Meta programs by leaning on text automation for the first three contacts. The lead receives an automated text inside seconds of submission, a second inside the first hour, and a third inside the first 24 hours, all on automation. The human counselor steps in when the lead responds.
If your admissions team cannot handle automated workflows because of CRM or operational constraints, fix that before adding Meta. The campaign will produce leads. The leads will go cold without the automation. The operator-honest version of the decision is whether you are willing to invest in the admissions ops infrastructure first.
How long before we see admits from Meta?
First Meta admits typically land in weeks three to five for treatment centers running the proper admissions workflow alongside the campaign. The Meta optimization signal itself calibrates faster than most operators expect, in roughly two weeks depending on spend, but the admit cycle adds its own lag on top.
The 30-day trial that operators frequently write into paid social agreements is not a fair evaluation window in 2026. The Meta inoculation period stretched after healthcare advertisers got moved into a sensitive category framework. Google’s inoculation extended in parallel, from about four weeks pre-2025 to around six weeks now. Either channel needs the admit-cycle lag layered on top before a fair read.
The minimum useful evaluation window for a treatment center Meta program is 90 days. Operators who pull the plug at 30 days lose the next 60 days of compounding performance. The patient capital required for a Meta program is real, and the operators who have it produce category-leading cost-per-admit numbers as a result.
What’s the right Meta budget for a treatment center?
The right Meta budget depends on operator scale. Tier 1 operators (under $50K total paid monthly) typically run $12K to $20K on Meta. Tier 2 ($75K to $150K total paid) run $35K to $80K on Meta. Tier 3 ($200K to $500K) run $100K to $300K on Meta as the channel proportion grows with admissions capacity.
Spending less than $10K monthly on Meta does not produce a useful evaluation signal for most treatment centers. The lead volume at that spend is too low to give the algorithm the conversion signal it needs to optimize. Operators who try Meta at $2K to $5K monthly typically conclude the channel does not work and reallocate to Google. They are evaluating a campaign that never had enough budget to perform.
If your total paid budget will not support a $10K minimum on Meta, the right move is to delay the Meta launch until the program scales, not to underfund the channel and conclude it failed.
How does Meta interact with our Google Ads spend?
Meta and Google produce different leads at different points in the family decision journey. Google captures high-intent search demand from people who already know they need treatment and are comparing facilities. Meta captures earlier-stage demand from family members who are still figuring out what comes next.
The interaction is additive, not substitutive. Operators who add Meta without cutting Google typically see total admit volume increase by 40 to 80 percent inside six months as the program scales. The Meta spend is not stealing from the Google spend; it is reaching a buyer population Google does not capture.
The right way to allocate between channels is to set Google at the spend level where the auction stops producing useful incremental volume, then put the remaining paid budget into Meta with admissions ops sized to handle the lead workflow. Most operators are underspending on Meta and overspending on Google at the marginal-admit level.
What’s the difference between a Meta lead and a Google lead psychologically?
A Google paid search lead is mid-funnel. They typed a query, clicked through to your landing page, and filled out a form. They already know they need treatment and are comparing options. The admissions counselor’s job is to close the comparison and route to admission.
A Meta lead is earlier in the journey. They saw an ad while scrolling, recognized something in the message, and clicked. They are not yet certain about treatment as the answer. The family member might be researching for a loved one. The admissions counselor’s job is to listen first, diagnose the situation second, and route to the right level of care third.
The same script will not work for both. Treatment centers that run a single admissions playbook lose the Meta lead inside the first 30 seconds because the opening assumes a buying state the lead has not yet reached. Train the admissions team on two scripts, one for each channel.
Do families actually respond to Meta ads for treatment?
Family members of patients are the highest-converting Meta audience for residential treatment, PHP, and high-acuity outpatient programs. In our client portfolio, the family member is the buyer 70 to 85 percent of the time for these levels of care. Meta’s targeting capabilities and creative format are well-suited to reaching them inside their daily scrolling behavior.
The creative that converts family members looks different from the creative that converts patients. Family-voice ads run in the parent’s or partner’s first-person perspective: “I watched my son disappear and I didn’t know what to do.” Patient-voice ads run in the patient’s perspective and convert better for outpatient and MAT programs where the patient is the direct decision-maker.
Mixed-acuity facilities run both audience playbooks in parallel campaign structures because the buyer pattern, the voice, the audience signals, and the conversion economics all diverge between family-driven and patient-driven inquiry.
What does an admissions team need to do differently to make Meta work?
The admissions team handling Meta leads needs three operational shifts from how they handle Google leads. First, they need an automated text follow-up workflow that fires inside seconds of every Meta lead form submission, no exceptions. Second, they need a persistence cadence trained into the team: at least ten contacts across the first 30 days for any Meta lead that has not declined.
Third, the admissions counselor handling Meta leads needs a different opening script. The Meta lead is earlier in the buying journey than the Google lead. The script that asks “are you ready to admit?” on contact one loses the Meta lead. The script that asks “what’s been happening with your loved one?” on contact one keeps the conversation open.
The admissions team can be taught these shifts. Most operators we audit have never been told their admissions playbook is the upstream determinant of Meta program performance. The training works. The operators who invest in the admissions side outperform the operators who only invest in the campaign side at every spend tier.
Where to start: a 30-day Meta readiness audit
The treatment centers winning on Meta in 2026 share one thing the failing centers do not: they did the admissions ops work before they spent the first dollar on media. The audit is the entry point, not the campaign.
Three things to do in the next 30 days if Meta is on your roadmap.
First, run a speed-to-lead audit on your existing inbound. Time the gap between a form submission on your current site and the first text or call to the lead.
If that gap is longer than 60 seconds during business hours or longer than 5 minutes overnight, the automation is the first thing to fix. Meta will not save you from a slow follow-up.
Second, document your current admissions cadence. How many contacts does a lead receive before the admissions team marks it cold? If the answer is fewer than five, the cadence is upstream of any media decision. Train and document the new cadence before launching Meta.
Third, audit your HIPAA-safe tracking. Standard Meta pixels firing on a treatment center site create direct HIPAA exposure under HHS-OCR online tracking guidance, which classifies any third-party tag capable of capturing PHI on a covered-entity site as a HIPAA breach risk requiring a BAA. The right pattern routes through server-side Conversions API with a BAA-covered intermediary. The compliance work is non-negotiable in 2026.
The treatment centers running Meta correctly in 2026 are producing cost-per-admit numbers that paid-only competitors cannot afford to match. The work to get there is real. The operators willing to do it are winning the next 12 months of admissions.
The ones who are not are losing share to the ones who are.
The perspective in this article comes from 9 years working exclusively inside behavioral health.
We are a team built by people in recovery who understand that behind every admission is someone asking for help. If that resonates, get to know us.
Mitch Marowitz is Director of Paid Media at Webserv. He has spent the last decade managing paid search and paid social programs for behavioral health operators, with current oversight on more than $4M in monthly behavioral health ad spend across Google Ads, Meta, TikTok, and emerging channels.
He writes here in his operator-to-operator voice; the data points reflect aggregated patterns across the Webserv client portfolio.