
A client called us in February. Three outpatient facilities in LA, $1.4 million sitting in legacy accounts receivable, and a previous billing company that had stopped working anything that required a phone call.
Most of these mistakes trace back to either a misaligned billing partner or a missing operational checklist. The structural fixes are: better RCM partner selection, prior authorization discipline, and a documented billing operations workflow. Those three changes separate centers that grow census from centers that quietly leak revenue.
Most of those claims were not hard. They just weren’t being worked.
Two months in, we collected about $700,000.
This is what billing failure actually looks like up close. Not a single dramatic event. A slow, consistent leak from the parts of the process nobody wants to do. If you want to understand the full system behind why this happens, our guide to revenue cycle management for rehab centers walks through the entire process from intake to collections.
Key Takeaways
- A slow VOB doesn’t just lose a patient. It burns a five-figure marketing spend with nothing to show for it.
- A bed full of bad coverage is worse than an empty bed. The slot is gone and there is no recovery.
- Most operators negotiate on the billing fee they can see, not the collection rate they cannot.
- Every billing failure is a marketing failure that never gets attributed to billing.
Behavioral health billing has a low skill floor and a very high skill ceiling. Almost anyone can submit a clean claim to a Cigna PPO. The work is in everything that happens around it.
Verification of benefits, utilization review, denial response, payer-specific code rules, audit defense, and the willingness to push back on insurance company tactics that exist purely to slow-walk your money. (Our preferred internal description of what we do is “professional escalation.”)
Most of the mistakes operators make aren’t really their fault. They’re the result of trusting a billing partner who quietly optimized for the parts of the work that are easy to invoice, and walked away from the parts that require fight.
By the time the trend shows up in revenue, six months of admissions are already gone. Some of these mistakes show up at intake. Some show up in utilization review. A few show up months later, when the audit letter arrives.
They all kill census the same way. A patient who never admits, a stay that ends three days early, or a claim that pays $11,000 instead of $43,000.
The mistake was never the treatment center. They just hired a billing company that focused on the easy 80% and walked away from the rest.
Kyle McHenry, Founder, Revenue Logic
Below are seven of the most expensive ones we see.
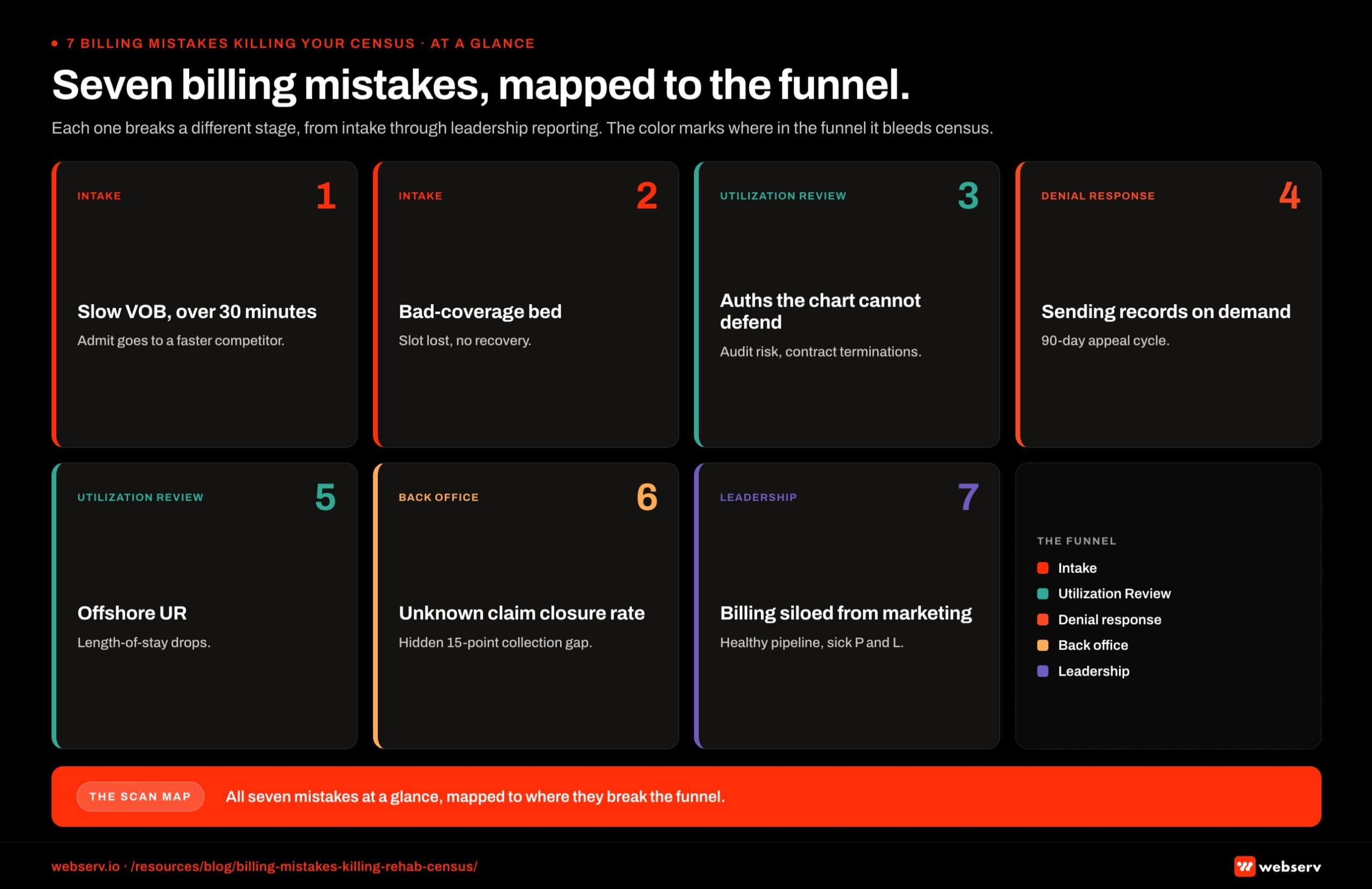
1. A verification of benefits process that takes more than 30 minutes
| What we see: | A facility loses an admit because the VOB took six hours to come back. Sometimes a full day. By the time the rep reaches back out, the patient has already admitted somewhere else. The competing facility had a faster billing partner. That is the entire story |
| Why it matters: | VOB turnaround is the first lever that determines whether you ever see a patient. Marketing spends thousands of dollars to get an inquiry call. The billing process either completes that handoff in under an hour or it forfeits it. |
| The cost: | A $1,500 per day detox stay across a 30-day continuum runs $45,000. Push to PHP and IOP and the lifetime value sits closer to $60,000 to $70,000 per admit, depending on the policy. Each lost admit is a five-figure marketing failure that didn’t happen in marketing. |
| The fix: | Run a 90-day audit on your average VOB turnaround time. Demand 30 minutes plus reasonable hold time as a service standard. If your billing partner cannot tell you what their median turnaround actually is, that is its own answer. |
2. Filling beds with policies that will never reimburse
| What we see: | A six-bed facility takes a policy without checking whether the plan type, alpha prefix, or state of issue will actually pay for behavioral health care at the level the patient needs. The bed is occupied. The next call gets refused. We saw a run of these last quarter when Blue Cross Blue Shield of Maine deleted roughly 14,000 policies from their database. Out-of-state residents had been claiming Maine residency to access those plans, then getting treatment in California. The plans collapsed. The admits came with them. |
| Why it matters: | A bed full of bad coverage is worse than an empty bed. You can’t move the patient out without a clinical reason and you can’t move the next caller in. |
| The cost: | Same math as the slow-VOB problem, but inverted. The slot is gone. There is no recovery. |
| The fix: | Build a pre-admit policy filter into your VOB workflow. Out-of-state exchange plans get extra scrutiny. Group plan types and historical reimbursement data should sit in front of the admissions team before the bed is offered. |
3. Letting your billing company lie on your behalf about authorizations
| What we see: | We take over a new client. We open the EMR. The notes are thin. The authorizations are full. That gap is one of the most consistent red flags in the industry. Somebody got those auths. The clinical record does not support them. When the insurance company eventually requests medical records for a claims review, the discrepancy becomes the treatment center’s problem, not the previous billing company’s. |
| Why it matters: | This is how facilities end up in audits, recoupment letters, and contract terminations. The previous billing company is long gone by the time the bill comes due. |
| The cost: | Audit defense runs from $25,000 to well into six figures depending on scope. Removal from a contract network can take six figures of monthly revenue off the books overnight. None of that money was ever yours to begin with. You will spend years explaining it anyway. |
| The fix: | Run a quarterly chart-to-auth audit. Pull a sample of recent authorizations. Read the notes that supported them. If a UR person could not have built that auth from those notes, you have a problem. (Our deep dive on the prior authorization workflow in addiction treatment covers what good chart-to-auth alignment looks like step by step.) |
4. Sending medical records every time the insurance company asks
| What we see: | A claim denial comes back asking for medical records. The denial cites missing authorization, ineligible provider type, or coding issues. Sometimes more than one in the same letter. Most of those flags are not real. The insurance company knows the auth exists. They are throwing up obstacles to slow the payment. |
| Why it matters: | Once medical records leave the building, the insurance company has a much bigger surface area to look for things to deny on, and they almost always find something. |
| The cost: | A claim that was going to pay can turn into a 90-day appeal cycle. Some claims never recover at all. |
| The fix: | Train the team to push back before they pull a single chart. The first move is to quote the auth number and force the payer to name the specific clinical record they want, and why. If they cannot, the records stay. |
5. Outsourcing utilization review overseas
| What we see: | A growing number of billing companies have moved their utilization review operations to firms in India. The cost savings make sense on paper. The downstream effect on authorizations does not. A care manager at the insurance company has wide latitude on what to approve. They approve more for people they recognize and trust. They approve less for callers who do not know the patient or the program and who carry a language barrier into a clinical conversation. |
| Why it matters: | UR is the second checkpoint after VOB that determines what your admit is actually worth. Lose three days of residential and you lose roughly $4,500 at typical reimbursement. |
| The cost: | Multiply across 30 admits a quarter and the math becomes obvious. We have seen length-of-stay drop materially inside a single quarter when offshore UR replaces domestic UR. |
| The fix: | Ask your billing company directly where their UR team sits. Ask how long the lead UR clinician has been working with your specific payer mix. The answer takes ten seconds and tells you everything you need to know. |
6. Not knowing your actual claim closure rate
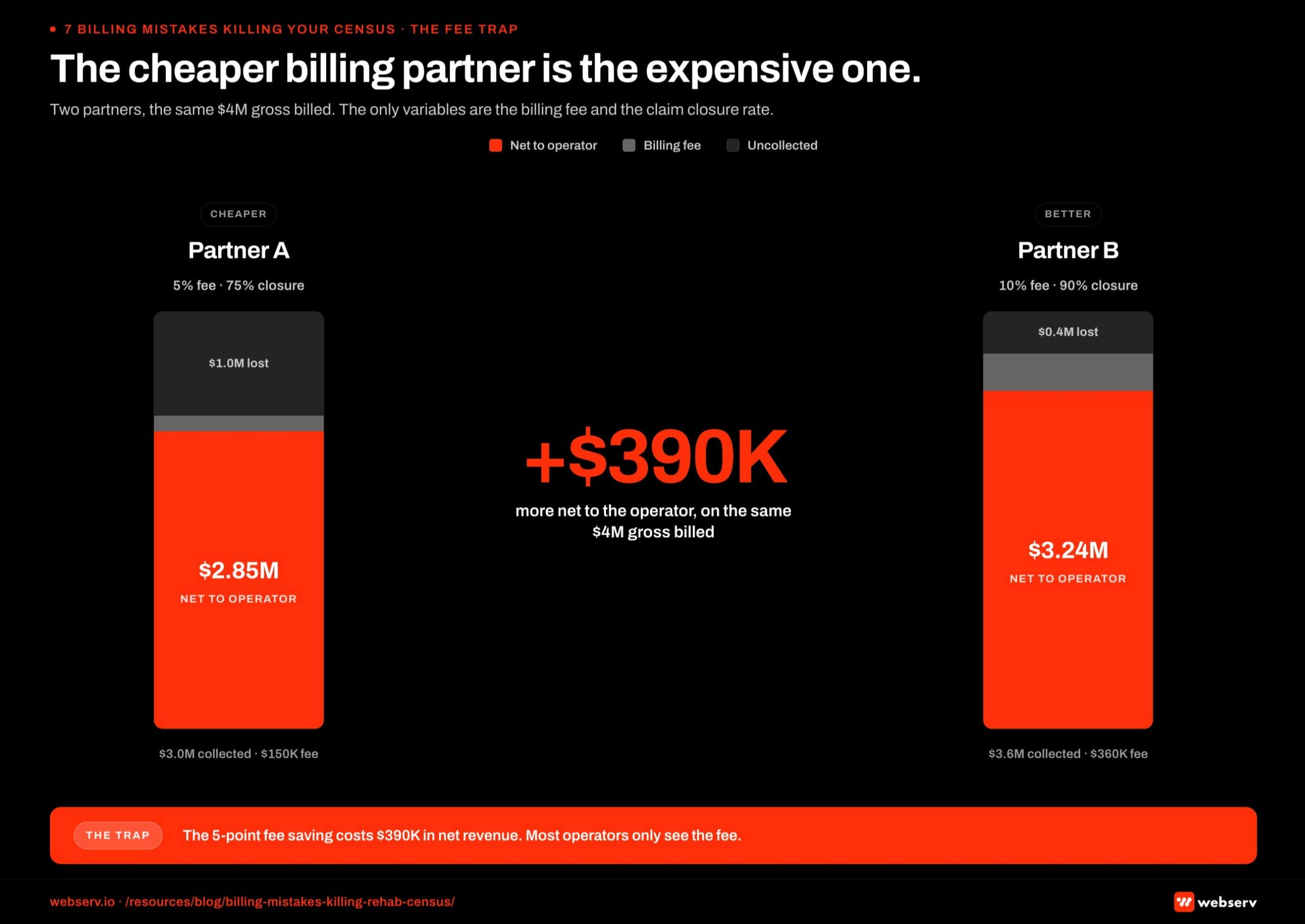
| What we see: | Operators tell us they pay 5% to their current billing company. They cannot tell us what percentage of their submitted claims are actually closing. That is the most expensive missing data point in this industry. |
| Why it matters: | A 5% fee at a 75% closure rate costs more than a 10% fee at a 90% closure rate. The math is not close. Most operators have never been shown either number, so they negotiate on the fee they can see and not the revenue they cannot. |
| The cost: | Run the math on $4 million in annual gross billed. The difference between 75% and 90% closure is roughly $600,000 of recovered revenue per year. The 5-point fee delta is $200,000. The operator saved $200,000 on the fee and walked away from $600,000 in collections. |
| The fix: | Demand a monthly dashboard from your billing partner that shows submitted, closed, denied, and outstanding claims with aging. If they will not build it, they aren’t in a position to defend their performance. (Our billing operations checklist documents the rest of the weekly and quarterly cadence that surfaces these numbers without a separate ask.) |
The hidden attrition is the worst kind. It doesn’t appear in any system because it never existed.
Kyle McHenry, Founder, Revenue Logic
7. Treating billing as a back-office expense instead of a marketing input
| What we see: | Marketing measures admissions. Billing measures collections. The two teams almost never look at the same dashboard. That is how a treatment center ends up with a healthy admit pipeline and a sick P&L at the same time. |
| Why it matters: | Return on ad spend is not the right metric. Return on invested capital is. The ad dollar that produced the admit only converts when the claim collects. Every billing failure is a marketing failure that never gets attributed to billing. |
| The cost: | The hidden attrition is the worst kind. It does not appear in any system because it never existed. The lost length of stay, the slow-VOB no-show, the claim that never appealed, all of it sits outside the marketing report. |
| The fix: | Run one weekly meeting that pulls the marketing team and the billing team into the same room. Look at admissions, average reimbursement per admit, length of stay, and aging together. The patterns surface within two cycles. |
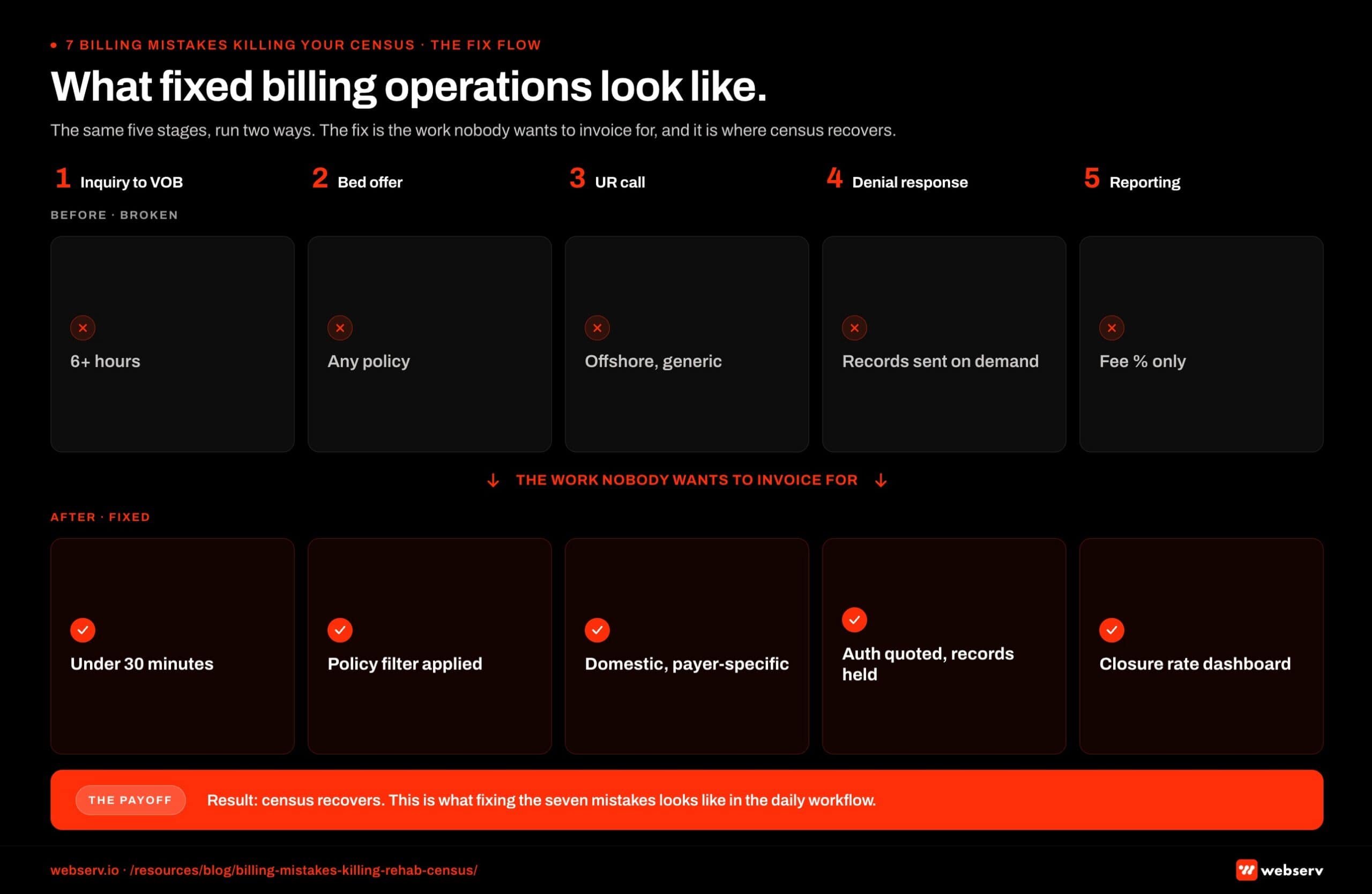
The difference is in the work nobody wants to do
There is a base skill set in behavioral health billing that almost any company can deliver. Clean VOBs, simple authorizations, and basic claim submission you can teach in a quarter.
The work that separates a serviceable billing partner from a strong one is the work nobody wants to invoice for. That work is also where your census lives. It is also exactly what our behavioral health billing services are built around.
A billing company that pushes back on what you ask for is doing its job. The treatment center talks to patients. The billing company talks to insurance companies.
We see the audit before it arrives. The payer that quietly changed its accepted code set last week, that visibility is ours too. State exchange plans about to disappear come up in our data weeks before they show up in your admissions report.
Listen to the people who are looking at that side of the house, even when what they tell you contradicts what the state licensing body said last week. The state guidelines don’t pay your bills. The insurance company does.
Frequently asked questions about treatment center billing mistakes
How can we tell if our billing company is making these mistakes?
Most billing problems show up as patterns in three metrics: days sales outstanding (DSO) trending above 50 days, denial rate above 12 percent, and inability to produce payer-specific underpayment data on demand. Any one of those is a sign of process problems. All three together is a sign of fundamental dysfunction.
The harder symptom to spot is what you do not see. A billing partner that consistently reports clean numbers but cannot show you the underlying claim-by-claim detail is hiding something. A billing partner that pushes back on detailed performance reviews or treats them as adversarial is usually managing a portfolio they cannot defend.
We recommend a quarterly billing performance review even when numbers look fine. The review should examine specific claims, not just aggregate metrics. Operators who only see summary reports miss the patterns that compound into the seven mistakes covered in this article.
Is it worth switching billing partners mid-year?
Sometimes. The switch carries operational risk (aging AR can stall, payer relationships need re-onboarding, in-flight authorizations need careful handoff) and most botched transitions lose 60 to 90 days of cash velocity. Programs that switch on impulse mid-year often regret the decision.
Programs that switch with discipline (planned transition, parallel running of both partners during handoff, documented claim status at switch) typically come out ahead within one to two quarters. The discipline matters more than the timing.
The cleanest decision framework is to evaluate the switch on annualized net revenue impact. If the new partner can defend a 3 to 5 percent improvement in net collections per admit and the transition cost is manageable, mid-year switches usually pay back inside one quarter.
What questions should we ask before hiring a new billing partner?
Six questions surface the patterns that matter: What is your current DSO across your treatment center book? What is your denial overturn rate on appeal? Can you show me payer-specific underpayment data for a current client? How is your UR team structured and where is the work performed? What is your authorization-to-claim alignment process? How do you handle continuation-of-stay requests when initial auth runs out?
Each question forces specifics rather than marketing claims. Billing partners that answer in concrete numbers and named processes are usually competent. Billing partners that answer in vague principles and aspirational statements are usually not.
We also recommend reference calls with two to three current clients of any prospective billing partner. The right reference is not a happy testimonial but a candid conversation about denial trends, AR aging, and communication quality. References that cannot speak to specific operational details are usually scripted.
Can we fix these issues without changing partners?
Sometimes, depending on which mistakes are happening and whether the partner is willing and able to change. Process mistakes (slow VOB, inadequate UR documentation, weak denial follow-up) can usually be fixed within the existing partner if leadership engages. Capability mistakes (outsourced UR offshore, lack of payer-specific analytics infrastructure, inadequate technology) usually cannot be fixed in place because they require capability the partner does not have.
The decision usually comes down to a candid conversation with the existing partner. Programs that escalate to billing partner leadership with specific evidence of the mistakes and a clear remediation request often see improvement within 60 to 90 days. Programs that escalate and get pushback or vague commitments usually need to switch.
The fastest signal is response speed and specificity. A billing partner that engages immediately with a detailed remediation plan after escalation is salvageable. A billing partner that defers, dismisses, or delays is signaling that change is not coming.
How much revenue is typically at stake when these mistakes happen?
For most mid-sized treatment centers, the seven mistakes together typically account for 15 to 30 percent of potential collected revenue. That translates to high six figures or low seven figures annually for a 50-bed residential program with reasonable payer mix.
The mistakes compound. Each individual mistake is usually responsible for 2 to 5 percent of potential revenue. Programs accumulating four to six of them simultaneously can lose more than a third of their collectible revenue without realizing why census revenue is below census admit count.
The math justifies the operational investment in fixing them. A 15 to 30 percent collected revenue lift is equivalent to a comparable lift in marketing budget capacity at the same admit volume. The difference is that fixing billing operations costs less and produces more durable returns.
The perspective in this article comes from 9 years working exclusively inside behavioral health.
We are a team built by people in recovery who understand that behind every admission is someone asking for help. If that resonates, get to know us.
Kyle McHenry is the founder of Revenue Logic, a behavioral health revenue cycle management firm. He has spent 15 years working with treatment center operators on verification, utilization review, and claims management. Webserv partners with Revenue Logic to surface RCM-side guidance for behavioral health admission operations.





