You’ve invested heavily in service pages that explain your clinical programming, then wonder why these pages neither rank in search results nor generate qualified admissions inquiries. The problem isn’t the quality of the treatment you’re providing. It’s a fundamental misunderstanding of how families research treatment options and what questions they need answered before they’ll pick up the phone.
Most rehab service pages are written from the provider’s perspective rather than the searcher’s. You detail credentials, methodologies, and facility amenities without addressing the underlying concerns that bring someone to the page in the first place. The result is content that satisfies internal stakeholders but fails to connect with the families making urgent, high-stakes decisions under extreme emotional pressure.
Search engines reward pages that comprehensively address user intent. Conversion optimization demands pages that build trust and resolve objections. These aren’t competing goals. They require the same foundation: understanding what someone searching for “dual diagnosis treatment” or “medication-assisted treatment” actually needs to know before they can take the next step.
How Rehab Service Pages Differ from Location Page Intent
Service pages and location pages serve fundamentally different functions in the decision journey. Your location pages address geographic access and logistical constraints. Your rehab service pages address clinical fit and treatment approach.
A family searching “dual diagnosis treatment near me” has already decided they need specialized care for co-occurring disorders. They’re not still deciding whether dual diagnosis treatment exists or matters. They’re evaluating whether your specific approach to dual diagnosis treatment aligns with their situation and whether they can trust you to deliver effective care.
This creates a unique challenge for your rehab service pages. The content must simultaneously establish clinical authority to earn search rankings while building emotional trust to generate conversions. Medical accuracy alone doesn’t accomplish this. Neither does optimization focused purely on keyword placement.
Your service page must address both the clinical question (what is this treatment and why does it work) and the practical questions (how do I know if this treatment fits my situation, what should I expect from the process, and why should I trust this particular provider).
Quick Signs Your Service Pages Are Underperforming
COMMON FAILURE PATTERN
The pages rank for “[service] definition” or “[service] explained” but not for “[service] near me” or “[service] [city].” That gap is the tell. Time-on-page under 60 seconds on a 2,000-word article, bounce rate above 70% from organic, and impressions climbing while clicks flatline all point at the same root cause: the page is written to define the service, not to fit a specific patient at a specific location. Rewrite to lead with fit criteria and local context, not encyclopedic definitions.
Your rehab service pages likely need restructuring if:
- Pages rank for “[service] definition” or “[service] explained” but not for “[service] near me” or “[service] [city]”
- Time on page is under 60 seconds despite pages being 2,000+ words long
- Bounce rates exceed 70% from organic search traffic
- Pages generate impressions but minimal clicks in search console data
- Inquiry forms at the bottom of pages convert poorly despite significant scroll depth
The Anatomy of a High-Performing Rehab Service Page
Every effective service page follows a similar architecture, though the specific content varies by service. Understanding this structure helps you diagnose problems with your existing pages and build stronger pages for new services.
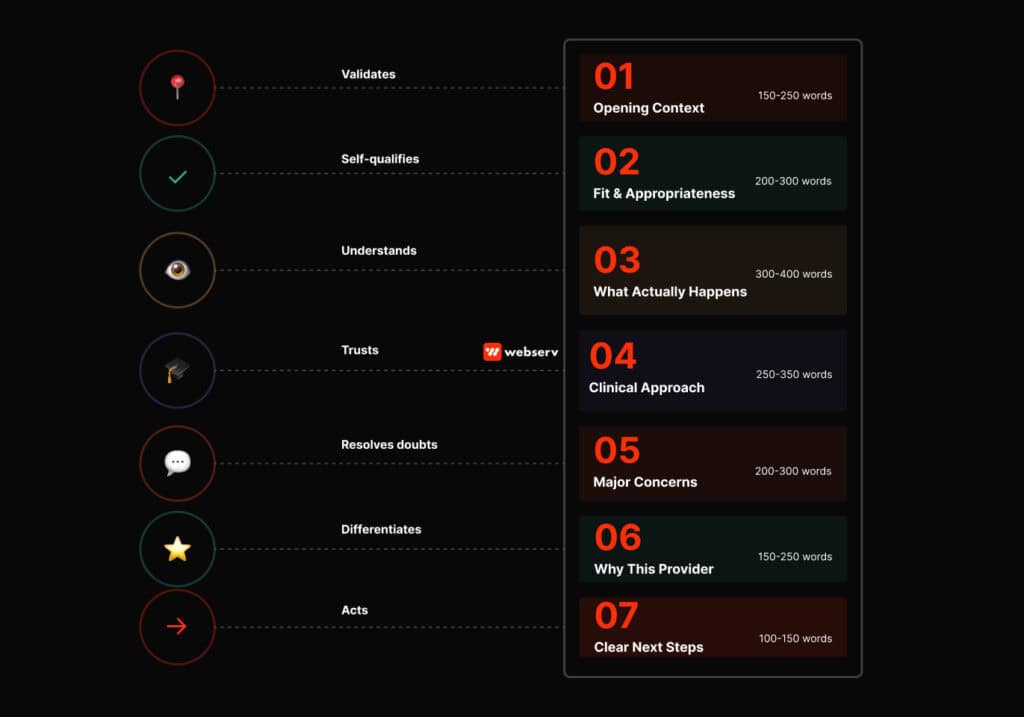
Component 1: Opening Context (150-250 words)
Purpose: Help readers immediately determine if they’re in the right place and if your service matches their situation.
What to include:
- One sentence explaining what the service is in plain language
- Who this service is designed for (severity level, life circumstances, co-occurring conditions)
- Common scenarios that indicate someone needs this level of care
- Brief mention of major accessibility requirements (time commitment, housing stability, etc.)
What this looks like: “Partial hospitalization programs (PHP) provide structured, full-day treatment for people who need more support than outpatient care but don’t require 24-hour medical supervision. Our PHP typically serves individuals transitioning down from residential treatment or those whose addiction severity requires intensive daily programming but who can maintain stable housing. If you’re struggling to stay sober between weekly therapy appointments but don’t need medical detox or constant monitoring, PHP may be the right fit.”
Common mistakes to avoid:
- Leading with your facility’s history or credentials
- Starting with a clinical definition written for other providers
- Burying who the service is for beneath methodology explanations
- Assuming readers already know whether they need this level of care
Component 2: Fit and Appropriateness (200-300 words)
Purpose: Help readers self-assess whether your service matches their needs before they invest time in clinical details.
What to include:
- Clear indicators that someone needs this level of care
- Signs that someone might need a different level of care instead
- Common misconceptions about who this service is for
- How this service differs from similar options (IOP vs PHP, residential vs inpatient, etc.)
What this looks like: “You might benefit from our intensive outpatient programming if you’ve completed residential treatment and need continued structure, if you’ve relapsed after standard outpatient care, or if your work and family obligations prevent residential treatment but you need more than weekly therapy. IOP isn’t appropriate for everyone. If you’re still experiencing withdrawal symptoms, if you lack stable housing, or if your environment includes active substance use, you likely need a higher level of care first.”
Common mistakes to avoid:
- Making every service sound appropriate for everyone
- Using clinical assessment criteria that families can’t self-evaluate
- Skipping this section entirely and jumping to “what we offer”
- Being vague about who shouldn’t pursue this service
Component 3: What Actually Happens (300-400 words)
Purpose: Demystify the treatment experience so families can visualize what participation involves.
What to include:
- Typical daily or weekly schedule in concrete terms
- Time commitment and duration expectations
- What a typical session or day involves (group therapy, individual counseling, etc.)
- Family involvement opportunities
- What happens during the first week vs. later stages
What this looks like: “Our intensive outpatient program meets three evenings per week from 5:30pm to 8:30pm, allowing participants to maintain employment. Each session includes 90 minutes of group therapy, 60 minutes of skills development (CBT, DBT, or relapse prevention), and 30 minutes of case management. You’ll work with the same counselor and group throughout the 12-week program. Individual therapy sessions happen weekly outside of group times. Most participants complete the full program in three months, though some extend to four months based on progress.”
Common mistakes to avoid:
- Describing what treatment includes without explaining what participants actually do
- Using vague timeframes like “several weeks” or “as long as needed”
- Focusing only on clinical activities and ignoring practical logistics
- Omitting information about evening/weekend availability, scheduling flexibility, or time off work
Component 4: Clinical Approach and Evidence (250-350 words)
Purpose: Establish clinical credibility and explain why your treatment approach works.
What to include:
- The therapeutic modalities or clinical approaches you use
- Brief explanation of why these approaches are effective for addiction (evidence-based context)
- How your specific implementation differs from basic standard of care
- Relevant outcome data or research citations if available
What this looks like: “Our dual diagnosis program integrates evidence-based addiction treatment with psychiatric care because co-occurring disorders require simultaneous treatment to achieve lasting recovery. We use cognitive behavioral therapy to address thought patterns that contribute to both substance use and mental health symptoms, dialectical behavior therapy for emotional regulation, and medication management when appropriate. Research consistently shows that treating addiction and mental health conditions together produces better outcomes than treating either in isolation. Our integrated approach means your addiction counselor and psychiatrist collaborate on your treatment plan rather than working separately.”
Common mistakes to avoid:
- Leading with this section before establishing fit and expectations
- Using clinical terminology without explaining what it means for the patient experience
- Making outcome claims without any supporting evidence or context
- Focusing on credentials and accreditations instead of treatment approach
Component 5: Addressing Major Concerns (200-300 words)
Purpose: Proactively resolve the objections and questions that prevent inquiry.
What to include:
- Insurance and payment information (even if brief)
- How people balance treatment with work/family obligations
- What happens if this level of care isn’t sufficient
- Privacy and confidentiality considerations
- Success factors and realistic expectations
What this looks like: “Most commercial insurance plans cover intensive outpatient treatment with prior authorization. We accept most major carriers and can verify your coverage before admission. Because IOP sessions occur in the evening, most participants continue working full-time during treatment. We understand that unexpected work conflicts happen and offer make-up sessions when needed. If you’re not making progress in IOP, we’ll reassess together and may recommend a higher level of care. Treatment works best when you’re committed to recovery, attend consistently, and actively participate in sessions.”
Common mistakes to avoid:
- Deferring all insurance questions to “call us for details”
- Ignoring work/family concerns entirely
- Overpromising outcomes or guaranteeing success
- Using so much compliance language that you undermine confidence
Component 6: Why Choose This Provider (150-250 words)
Purpose: Differentiate your program from other providers offering the same service.
What to include:
- Specific program features that distinguish your approach
- Specialized expertise or certifications relevant to this service
- Concrete examples of how your program differs from standard implementation
- Brief, relevant testimonial or outcome data if available
What this looks like: “Unlike many medication-assisted treatment programs that focus only on medication management, our MAT program includes weekly individual counseling and optional group support. Our medical director specializes in addiction medicine and is certified in both Suboxone and Vivitrol administration. We offer flexible dosing schedules including weekend appointments because we know work schedules vary. Most importantly, we view MAT as treatment, not just maintenance. Our goal is helping you build the skills and support systems for long-term recovery, with medication as one tool in comprehensive care.”
Common mistakes to avoid:
- Generic statements like “compassionate care” or “individualized treatment” that every provider claims
- Focusing on amenities (chef-prepared meals, yoga classes) for outpatient services where they’re irrelevant
- Leading with this section before establishing service fit
- Making this section longer than the “what actually happens” section
Component 7: Clear Next Steps (100-150 words)
Purpose: Make it easy for families to take action while offering options for different readiness levels.
What to include:
- Primary call to action (schedule assessment, verify insurance, call for consultation)
- Secondary lower-commitment option (chat, download guide, insurance verification)
- What happens after they take the next step
- Reassurance about the inquiry process
What this looks like: “Ready to learn more about our intensive outpatient program? Call us at [number] to speak with an admissions counselor who can answer questions and help determine if IOP is right for you. We can typically verify insurance coverage within one business day and schedule an intake assessment within 48 hours. Not ready to call? Use our online insurance verification form or chat with us during business hours. All conversations are confidential and there’s no obligation.”
Common mistakes to avoid:
- Offering only a generic contact form with no context
- Including multiple competing calls to action that create decision paralysis
- Ending the page without any clear next step
- Making the inquiry process sound complicated or intimidating
Writing Guidelines: Who Should Write Your Service Pages and How
Your service pages require collaboration between clinical expertise and communication skill. The best approach involves a marketer or content writer drafting accessible content based on clinical input, then having your clinical staff review for accuracy.
The Right Writer for Rehab Service Pages
Primary writer should be: Someone who can translate clinical concepts into accessible language while maintaining accuracy. This is typically a marketer, content specialist, or professional writer with healthcare experience.
Primary writer should NOT be: A clinician writing in their clinical voice, an SEO specialist focused purely on keyword optimization, or a sales-oriented copywriter without healthcare understanding.
Why this matters: Your clinicians often write at a technical level appropriate for peers but inaccessible to families in crisis. Pure marketers often oversimplify or make unsupported claims. The right writer bridges clinical accuracy with accessible communication.
Who Provides Input and Review
Effective service page development involves multiple perspectives from your team:
- Your clinical staff provide information about treatment approaches, evidence base, typical patient scenarios, appropriate expectations, and any luxury rehab amenities
- Your admissions staff identify the most common questions families ask before admission and the concerns that prevent inquiry
- Your marketing/SEO staff ensure content addresses search intent and includes appropriate semantic keyword coverage
- Your compliance/legal review verifies claims are supportable and regulatory language is appropriate
The process works best when your writer interviews these stakeholders, drafts content, circulates for review, and revises based on feedback. Trying to write by committee produces unfocused content that satisfies no one.
Reading Level and Tone Guidelines
Your rehab service pages should be written at approximately an 8th grade reading level. This doesn’t mean oversimplifying or talking down to readers. It means using straightforward sentence structure, defining medical terms when you use them, and avoiding unnecessarily complex language.
The tone should be:
- Authoritative but not academic
- Warm but not emotional
- Confident but not overpromising
- Direct but not cold
Avoid these tone problems:
- Overly clinical language that creates distance (“individuals seeking treatment for substance use disorders”)
- Overly casual language that undermines credibility (“we’ll help you kick the habit for good!”)
- Fear-based language that manipulates (“without treatment, addiction will destroy everything you love”)
- Vague inspirational language that says nothing concrete (“begin your journey to wellness today”)
Common Content Problems and How to Fix Them
Problem: Your Page Focuses on What You Offer Instead of What the Reader Needs
How to identify: The page uses “we” and “our” more than “you” and “your.” Section headers are about your facility rather than the service.
How to fix: Rewrite your section headers and opening sentences to focus on reader questions and needs. Instead of “Our Approach to Dual Diagnosis Treatment,” use “How Dual Diagnosis Treatment Addresses Both Conditions Simultaneously.”
Problem: Technical Clinical Language Creates Barriers to Understanding
How to identify: Your page includes terms like “evidence-based modalities,” “individualized treatment planning,” or “continuum of care” without explaining what these mean in practice.
How to fix: Either replace clinical terminology with plain language or immediately define terms in accessible ways. Instead of “our program utilizes CBT modalities,” write “our program uses cognitive behavioral therapy, which helps you identify and change thought patterns that contribute to substance use.”
Problem: Your Page Answers Questions Nobody’s Asking
How to identify: Large sections cover your accreditations, facility history, or staff credentials before addressing basic service information. Content focuses on provider priorities rather than patient concerns.
How to fix: Review your admissions call recordings or survey your admissions staff to identify the actual questions families ask. Restructure content to address these questions in order of frequency.
Problem: Critical Information Is Buried or Missing
How to identify: Insurance information only appears at the very bottom, time commitments aren’t specified, duration is vague, or there’s no clear explanation of what participation actually involves day-to-day.
How to fix: Create a content inventory checklist of must-include elements (who it’s for, time commitment, duration, what happens, insurance) and ensure each appears prominently. Move practical information higher in your page hierarchy.
Problem: Your Page Is Indistinguishable from Competitors
How to identify: You could swap your facility name with a competitor’s name and the content would still make sense. All your differentiators are generic (“experienced staff,” “personalized care,” “proven methods”).
How to fix: Identify 2-3 specific ways your implementation of this service actually differs from standard care. Include concrete examples, specific features, or measurable distinctions rather than generic quality claims.
Content Elements to Avoid
These elements appear frequently on treatment center service pages but typically hurt rather than help:
Stock photography of diverse people in group therapy circles: Families research treatment at midnight on their phones. Generic stock photos add no information and slow page loading. If you use images, use real photos from your facility or infographics that convey information.
Long lists of every possible service component: Detailed lists of “individual therapy, group therapy, family therapy, medication management, nutritional counseling, fitness activities, recreational therapy…” create wall-of-text problems without helping readers understand what treatment actually involves.
Separate sections for each evidence-based modality: Pages that have individual sections for CBT, DBT, MI, trauma therapy, etc. become repetitive and overwhelming. Integrate these into an explanation of your overall treatment approach rather than listing them separately.
Testimonials that could apply to anything: Generic quotes like “this place saved my life” or “the staff really cares” don’t build specific credibility. If you use testimonials, choose ones that address specific concerns (“I was worried about missing work but the evening IOP schedule made it possible”).
Lengthy disclaimers and qualifications: While necessary for compliance, disclaimers like “individual results may vary” and “no treatment guarantees success” should appear once at the bottom, not repeatedly throughout the content where they undermine confidence.
Multiple competing calls to action: Pages that simultaneously ask people to call, submit a form, start a chat, verify insurance, download a guide, and schedule a tour create decision paralysis. Offer one primary action and one secondary option.
How to Audit Your Current Service Pages
Use this framework to evaluate whether your existing rehab service pages need revision:
The 30-Second Test
Open your page and read only the first 200 words. Can you answer these questions:
- What is this service?
- Who is it for?
- What’s the basic time commitment or format?
If not, your opening needs restructuring.
The Scan Test
Scroll through your page at normal reading speed without stopping. Do your section headers tell a clear story about:
- Whether this service fits a situation
- What participation involves
- Why this approach works
- What makes your program distinct
If your section headers focus on internal topics (Our Facility, Our Team, Our Philosophy) rather than reader questions, restructure the content.
The Bounce Test
Look at your analytics for time on page and bounce rate:
- If average time on page is under 90 seconds for a 1,500+ word page, readers aren’t engaging
- If bounce rate exceeds 70%, your content isn’t matching search intent
- If scroll depth shows most visitors never reach the middle of the page, your opening content isn’t pulling them in
These signals indicate content problems, not just SEO issues.
The Inquiry Test
Track where people exit your page and whether they take any action:
- If significant traffic reaches the bottom but doesn’t convert, you may be missing conversion options or not addressing final objections
- If most people leave mid-page, identify where they exit and what content appears at that point
- If you get questions via phone that your page should answer, add that content prominently
The Differentiation Test
Read your page and your top three competitors’ pages for the same service. If you removed all facility names and branding, could you tell the pages apart? If not, you need to add specific differentiators rather than relying on generic quality claims.
Measuring Your Service Page Performance Beyond Rankings
You typically evaluate service page success by tracking rankings for target keywords and overall organic traffic. These metrics matter but they don’t indicate whether your pages are actually generating qualified inquiries or serving families effectively.
Engagement Signals That Indicate Content Effectiveness
Time on page provides the most straightforward signal of whether your content holds attention. Your rehab service pages should typically see average time on page of 2-3 minutes minimum for content in the 1,500-2,000 word range. Pages with 30-60 second average time on page aren’t being read regardless of their rankings.
Scroll depth reveals whether readers engage with your full content or bounce after scanning the opening. Your service pages should see at least 50% of visitors scrolling to the midpoint and 25-30% reaching the bottom.
Pages where 80% of visitors never scroll past the opening indicate content that fails to draw readers in.
Conversion Metrics That Matter More Than Form Submissions
You often fixate on inquiry form submission rates as the primary conversion metric for rehab service pages. This ignores that many qualified prospects take alternative conversion actions like calling directly, initiating chat, or clicking through to verify insurance.
Tracking only form submissions misses significant conversion volume.
Track all conversion actions: form submissions, phone calls from tracked numbers, chat initiations, insurance verification starts, supporting page views that indicate serious research, and return visits. These combined actions provide a fuller picture of how your service pages move prospects toward admission.
Resources for Understanding Treatment Service Standards
The Substance Abuse and Mental Health Services Administration publishes treatment improvement protocols that provide evidence-based guidance on various treatment modalities at samhsa.gov. These protocols can inform how you describe clinical approaches and evidence base without requiring independent literature review.
The American Society of Addiction Medicine provides clinical guidance and standards that can inform content about levels of care and treatment matching at asam.org. Their ASAM criteria for treatment placement are widely used and can provide authoritative backing for how you describe service appropriateness.
Service Pages as Part of Your Comprehensive Content Strategy
Your service pages don’t exist in isolation. They work alongside your location pages, supporting content, blog posts, and resource pages to create comprehensive topical coverage that establishes domain authority and captures traffic across the full spectrum of treatment-related searches.
The strategic question isn’t whether your individual rehab service pages rank well. It’s whether your complete content ecosystem comprehensively addresses the topics and questions relevant to your services and geography in ways that build cumulative authority and trust.
Treatment centers that create strong service pages but neglect supporting content miss opportunities to capture long-tail traffic and build topical depth. Those that create comprehensive resource libraries but weak service pages generate traffic that doesn’t convert. Your goal is integration: service pages that convert supported by content ecosystems that drive awareness and establish authority. If you’d rather have a partner build that ecosystem with you, book an intro call with Webserv.