
At a glance: This is a working reference of the most current U.S. drug abuse statistics, sourced primarily from the SAMHSA 2024 National Survey on Drug Use and Health (released July 2025) and CDC NCHS provisional overdose data through 2024. The numbers reflect the population aged 12 or older in the noninstitutionalized civilian U.S. unless otherwise noted. Where statistics are dated to specific years (2021–2024), we cite the original SAMHSA or CDC release. Every percentage in this article has a named source so it’s safe to cite, share, or quote directly.
Key Takeaways
- 48.4 million Americans aged 12+ had a substance use disorder in 2024 (16.8% of the population). Alcohol use disorder accounted for 27.9 million, drug use disorder for 28.2 million, and 7.7 million people had both.
- Only 19.3% of people who needed substance use treatment received it in 2024. That’s 10.2 million people treated out of 52.6 million who needed it. The 80% treatment gap holds despite multi-year overdose death declines.
- Drug overdose deaths fell 26.9% in 2024 to approximately 80,391, the largest single-year reduction on record. Synthetic opioid deaths dropped from 83,140 in 2023 to 54,743 in 2024.
- Fentanyl is still the leading cause of death for Americans aged 18–44 despite the 2024 decline. Polysubstance overdose remains the dominant pattern, with 47% of 2023 overdose deaths involving both opioids and stimulants.
- Marijuana use disorder is rising as overall substance use disorders fall. Past-year marijuana use disorder grew from 16.7 million people (6.0%) in 2021 to 20.6 million people (7.1%) in 2024.
- Co-occurring conditions are massively undertreated. 21.2 million adults had both any mental illness and a substance use disorder in 2024. Of those, 58.8% received no treatment for either condition.
- Youth suicide indicators are trending down but remain serious. 700,000 adolescents aged 12–17 attempted suicide in 2024 (2.7%), down from 940,000 (3.6%) in 2021.
A note before the statistics
Operators ask us for “the latest stats” several times a week. We tell them the same thing every time.
The headline statistic (48.4 million Americans have a substance use disorder) hasn’t shifted in five years. The treatment gap (80% of people who need care don’t receive it) hasn’t moved either. What has changed is the drug supply, the overdose death curve, and the specific sub-conditions driving the numbers.
If you build a treatment program around 2019 data, you’ll fail patients in 2026. Fentanyl-contaminated cocaine and methamphetamine, xylazine and medetomidine adulterants, and counterfeit pills now dominate the operational reality. The treatment gap is partly a marketing problem and mostly a market access problem.
This article is the working reference we maintain for treatment center operators, marketers, and clinicians who need cite-able numbers without hunting through 132 pages of NSDUH appendix tables and CDC press releases.
The primary source for substance use disorder, treatment receipt, and mental health prevalence is the SAMHSA 2024 National Survey on Drug Use and Health (NSDUH), released July 2025. The primary source for overdose deaths is the CDC NCHS Vital Statistics Rapid Release and associated press releases through May 2025.
We added a brief commentary block after each section to translate the statistic into an operational implication for treatment centers. The numbers themselves are neutral. The implications are not.
How we sourced and dated these statistics
Statistics in this article are organized by data type, dated to the most recent available release, and cited to the original government source. We follow three rules:
| Rule | Application |
|---|---|
| Cite to original release, not aggregators | NSDUH directly from SAMHSA, overdose deaths directly from CDC NCHS |
| Date every statistic to the survey year, not publication year | A statistic from the 2024 NSDUH was published in July 2025; we date it as a 2024 estimate |
| Note methodology changes that affect comparability | The 2021–2024 NSDUHs used multimode collection; older data is not directly comparable on some measures |
The SAMHSA 2024 NSDUH completed 70,241 interviews across all four quarters of 2024, with a weighted response rate of 11.3% for people aged 12 or older. CDC overdose mortality data through 2024 reflects provisional National Vital Statistics System counts with continued lag-adjustment.
When a stat without a year is referenced casually online (often from 2018–2020 surveys), it’s almost always outdated by at least one major epidemic phase. Use the dated versions in this article instead.
Drug use prevalence in 2024
The most current SAMHSA NSDUH data for people aged 12 or older shows the following past-month and past-year substance use estimates.
| Substance | Use period | Number of users | Percentage | Source |
|---|---|---|---|---|
| Any substance (tobacco/alcohol/illicit) | Past month | 168.0 million | 58.3% | SAMHSA 2024 NSDUH |
| Alcohol | Past month | 134.3 million | 46.6% | SAMHSA 2024 NSDUH |
| Tobacco products | Past month | 48.0 million | 16.7% | SAMHSA 2024 NSDUH |
| Nicotine vaping | Past month | 27.7 million | 9.6% | SAMHSA 2024 NSDUH |
| Any illicit drug | Past month | 48.2 million | 16.7% | SAMHSA 2024 NSDUH |
| Any illicit drug | Past year | 73.6 million | 25.5% | SAMHSA 2024 NSDUH |
| Marijuana | Past month | 44.3 million | 15.4% | SAMHSA 2024 NSDUH |
| Cocaine (incl. crack) | Past year | ~4.8 million | 1.7% | SAMHSA 2024 NSDUH |
| Methamphetamine | Past year | 2.5 million | 0.9% | SAMHSA 2024 NSDUH |
| Heroin | Past year | 556,000 | 0.2% | SAMHSA 2024 NSDUH |
| Prescription opioid misuse | Past year | 7.6 million | 2.6% | SAMHSA 2024 NSDUH |
| Hallucinogens | Past year | ~10.4 million | 3.6% | SAMHSA 2024 NSDUH |
What this means for treatment centers: The aggregate prevalence numbers stay relatively flat year over year. What changes is the substance mix.
Marijuana use has risen consistently while tobacco and cigarette use continues to decline. Polysubstance use is the operational reality, not single-substance use.
Alcohol-specific 2024 data
| Metric | 2024 estimate | Trend vs 2021 | Source |
|---|---|---|---|
| Past-month alcohol use, 12+ | 134.3 million (46.6%) | No change | SAMHSA 2024 NSDUH |
| Past-month binge drinkers, 12+ | 57.9 million (20.1%) | Down from 21.7% | SAMHSA 2024 NSDUH |
| Past-month heavy drinkers, 12+ | 14.5 million (5.0%) | Down from 5.7% | SAMHSA 2024 NSDUH |
| Underage drinkers (aged 12–20) | 5.1 million (13.3%) | Down from 15.6% | SAMHSA 2024 NSDUH |
| Underage binge drinkers | 2.9 million (7.6%) | No change | SAMHSA 2024 NSDUH |
| Past-year alcohol use disorder | 27.9 million (9.7%) | Down from 10.6% | SAMHSA 2024 NSDUH |
What this means for treatment centers: Alcohol use disorder remains the largest single SUD category by population. Underage past-month drinking declined 2.3 points from 2021 to 2024, but binge drinking among the same age group held flat, which signals a problem of drinking intensity rather than drinking initiation.
Marijuana use trends
| Metric | 2021 | 2024 | Direction |
|---|---|---|---|
| Past-month marijuana use, 12+ | 13.2% (37.0M) | 15.4% (44.3M) | Up |
| Past-month, adults 26+ | 12.3% (27.1M) | 15.1% (34.3M) | Up |
| Past-year marijuana use disorder | 6.0% (16.7M) | 7.1% (20.6M) | Up |
| Adults 26+ with marijuana use disorder | 4.7% (10.4M) | 6.1% (13.8M) | Up |
What this means for treatment centers: Marijuana use disorder is the fastest-growing past-year SUD by population. Operators expecting THC concentrations and use patterns from 2015–2019 are clinically out of date. Vaping and dabbing concentrates dominate use modes among young adults.
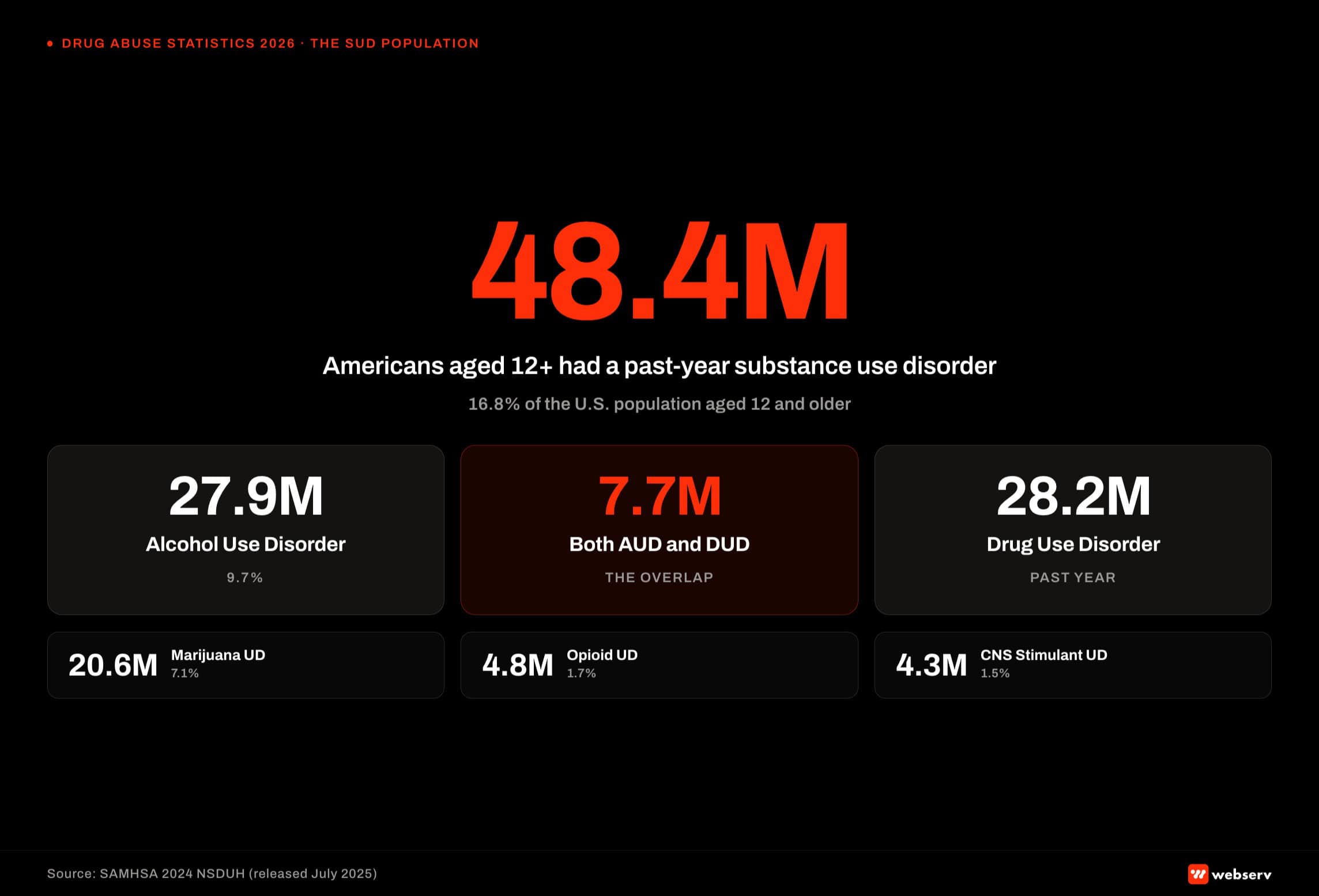 Hero infographic titled ‘U.S. substance use disorder population in 2024.’ 48.4 million people aged 12 or older (16.8 percent of the population) had a substance use disorder in 2024 per SAMHSA NSDUH data. Breakdown shows 27.9 million with alcohol use disorder, 28.2 million with drug use disorder, and 7.7 million with both. A second row breaks out the largest drug-specific disorders: marijuana use disorder, opioid use disorder, and stimulant use disorder. Source attribution: SAMHSA 2024 National Survey on Drug Use and Health.
Hero infographic titled ‘U.S. substance use disorder population in 2024.’ 48.4 million people aged 12 or older (16.8 percent of the population) had a substance use disorder in 2024 per SAMHSA NSDUH data. Breakdown shows 27.9 million with alcohol use disorder, 28.2 million with drug use disorder, and 7.7 million with both. A second row breaks out the largest drug-specific disorders: marijuana use disorder, opioid use disorder, and stimulant use disorder. Source attribution: SAMHSA 2024 National Survey on Drug Use and Health.Substance use disorders in 2024
48.4M
Americans aged 12+ with a substance use disorder in 2024 (16.8% of population). SAMHSA 2024 NSDUH.
19.3%
Share of people who needed substance use treatment and received it in 2024. Only 10.2M of 52.6M.
80,391
Total U.S. drug overdose deaths in 2024. Down 26.9% year-over-year — the largest single-year drop on record. CDC NCHS provisional.
21.2M
U.S. adults with co-occurring mental illness and SUD in 2024. 58.8% received neither treatment.
SAMHSA estimates that 48.4 million people aged 12 or older (16.8%) had a substance use disorder in the past year, based on DSM-5 criteria.
| Disorder | 2024 estimate | Source |
|---|---|---|
| Any substance use disorder | 48.4 million (16.8%) | SAMHSA 2024 NSDUH |
| Alcohol use disorder | 27.9 million (9.7%) | SAMHSA 2024 NSDUH |
| Drug use disorder | 28.2 million | SAMHSA 2024 NSDUH |
| Both alcohol and drug use disorder | 7.7 million (16.0% of SUD pop) | SAMHSA 2024 NSDUH |
| Marijuana use disorder | 20.6 million (7.1%) | SAMHSA 2024 NSDUH |
| Opioid use disorder | 4.8 million (1.7%) | SAMHSA 2024 NSDUH |
| CNS stimulant use disorder | 4.3 million (1.5%) | SAMHSA 2024 NSDUH |
| Severe opioid use disorder | 19.3% of OUD cases | SAMHSA 2024 NSDUH |
What this means for treatment centers: The DSM-5 SUD criteria changed in how NSDUH applies them between 2020 and 2021, so cross-year comparisons require care. The 16.8% population prevalence has been stable for three consecutive years. Marijuana use disorder is the only major category showing year-over-year growth.
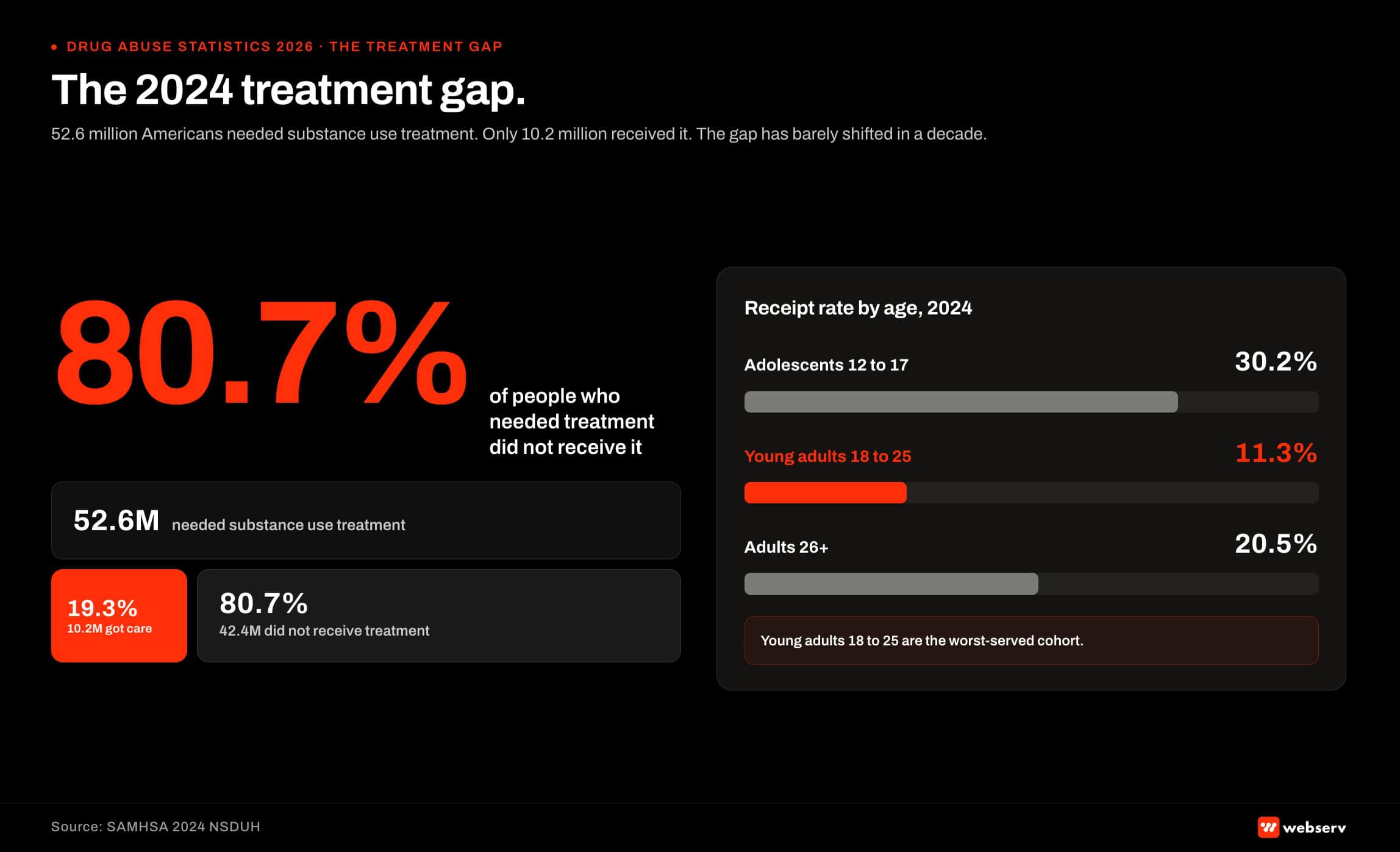 Treatment gap funnel infographic titled ‘The 2024 treatment gap.’ 52.6 million people aged 12 or older needed substance use treatment in 2024. Only 10.2 million (19.3 percent) received treatment. An age-band breakdown shows the 18 to 25 cohort at 11.3 percent treatment receipt rate, the worst-performing cohort. Source: SAMHSA 2024 National Survey on Drug Use and Health.
Treatment gap funnel infographic titled ‘The 2024 treatment gap.’ 52.6 million people aged 12 or older needed substance use treatment in 2024. Only 10.2 million (19.3 percent) received treatment. An age-band breakdown shows the 18 to 25 cohort at 11.3 percent treatment receipt rate, the worst-performing cohort. Source: SAMHSA 2024 National Survey on Drug Use and Health.The treatment gap: the most-cited statistic on this list
This is the operational statistic that matters most to treatment center operators and the one that has barely shifted in a decade.
| Metric | 2024 estimate | Source |
|---|---|---|
| People aged 12+ needing substance use treatment | 52.6 million | SAMHSA 2024 NSDUH |
| Of those, people who had an SUD in past year | 48.4 million | SAMHSA 2024 NSDUH |
| Of those, received substance use treatment | 10.2 million (19.3%) | SAMHSA 2024 NSDUH |
| Adolescents 12–17 needing treatment who received it | 30.2% | SAMHSA 2024 NSDUH |
| Young adults 18–25 needing treatment who received it | 11.3% | SAMHSA 2024 NSDUH |
| Adults 26+ needing treatment who received it | 20.5% | SAMHSA 2024 NSDUH |
“The treatment gap isn’t a marketing problem first. It’s an access problem first. The operators who win in this category understand that intake speed, insurance verification fluency, and same-day admission capacity matter more than any single ad campaign.”
Preston Powell, CEO, Webserv
Treatment delivery breakdown (2024):
- Outpatient treatment: 7.1 million people (2.5%)
- Telehealth treatment: 3.6 million people (1.3%)
- Inpatient treatment: 2.6 million people (0.9%)
- Medication for opioid use disorder (MOUD): 2.2 million people (0.7%)
- Medication for alcohol use disorder (MAUD): 1.3 million people (0.5%)
- Treatment in prison, jail, or juvenile detention: 819,000 people (0.3%)
What this means for treatment centers: Of the 4.8 million Americans with opioid use disorder, only an estimated 818,000 received MOUD in 2024 (about 17%). That’s the single most actionable gap in the dataset. Operators that can credentialize for MOUD, build telehealth capacity for ongoing care, and lower admission barriers (waiting list, insurance, motivation requirements) have the strongest 2026 opportunity.
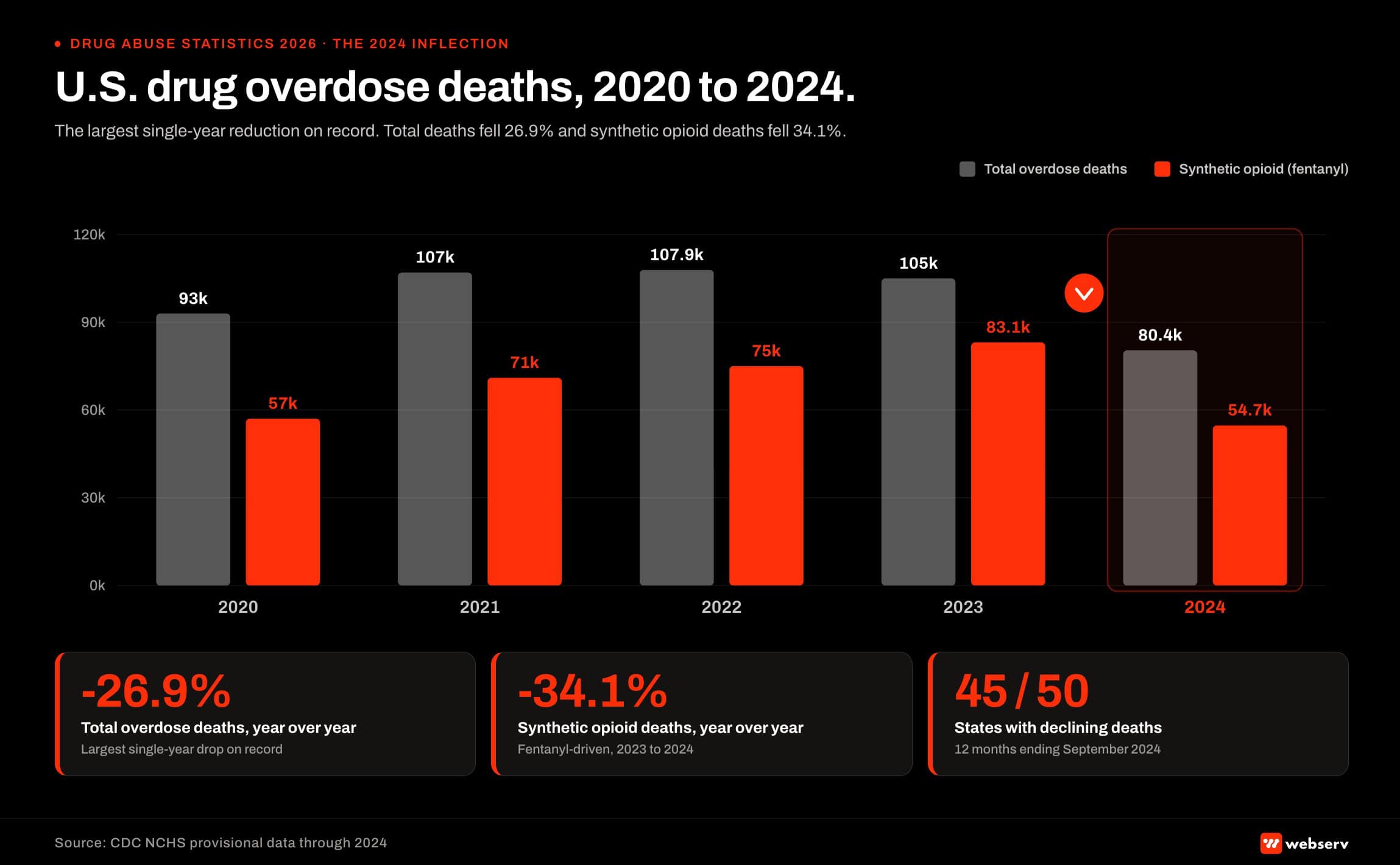 Paired bar chart titled ‘U.S. drug overdose deaths 2020 to 2024.’ Total overdose deaths and synthetic opioid (primarily fentanyl) deaths shown side by side for each year from 2020 through 2024. 2024 marks the largest single-year reduction on record, a 26.9 percent decline from 2023. Synthetic opioid deaths declined in tandem, reflecting both supply changes and naloxone distribution scale. Source: CDC National Center for Health Statistics provisional data.
Paired bar chart titled ‘U.S. drug overdose deaths 2020 to 2024.’ Total overdose deaths and synthetic opioid (primarily fentanyl) deaths shown side by side for each year from 2020 through 2024. 2024 marks the largest single-year reduction on record, a 26.9 percent decline from 2023. Synthetic opioid deaths declined in tandem, reflecting both supply changes and naloxone distribution scale. Source: CDC National Center for Health Statistics provisional data.Overdose deaths: the 2024 inflection
CDC NCHS provisional data shows the largest single-year reduction in drug overdose deaths on record.
| Year | Total overdose deaths | Synthetic opioid deaths (primarily fentanyl) | Source |
|---|---|---|---|
| 2020 | ~93,000 | ~57,000 | CDC NCHS |
| 2021 | ~107,000 | ~71,000 | CDC NCHS |
| 2022 | 107,941 | ~75,000 | CDC NCHS |
| 2023 | 105,007 | 83,140 | CDC NCHS |
| 2024 (provisional) | ~80,391 (-26.9%) | 54,743 (-34.1%) | CDC NCHS (May 2025 release) |
Other 2023 / 2024 overdose data points:
- 76% of 2023 overdose deaths involved an opioid (prescription or illegal)
- 69% of 2023 overdose deaths involved synthetic opioids (primarily IMF)
- 47% of 2023 overdose deaths involved both opioids and stimulants (“fourth wave”)
- 29,449 deaths involved cocaine in 2023 (up 85% from 2019)
- 34,855 deaths involved psychostimulants (primarily methamphetamine) in 2023
- 10,870 deaths involved benzodiazepines in 2023, with nearly 70% co-involving fentanyl
- 45 states showed declining overdose deaths in the 12 months ending September 2024; 5 states (Alaska, Montana, Nevada, South Dakota, Utah) showed increases
- West Virginia: highest fentanyl overdose death rate at 69.2 per 100,000 in 2023
- Overdose remains the leading cause of death for Americans aged 18–44
What this means for treatment centers: The 2024 decline is real and historic, but it’s not over. Naloxone access expansion, the elimination of the X-Waiver requirement (under the MAT Act of 2023), broader buprenorphine prescribing, and shifts in the illicit supply all contributed.
The five states with rising overdose deaths in 2024 are the markets where census pressure on existing programs is highest.
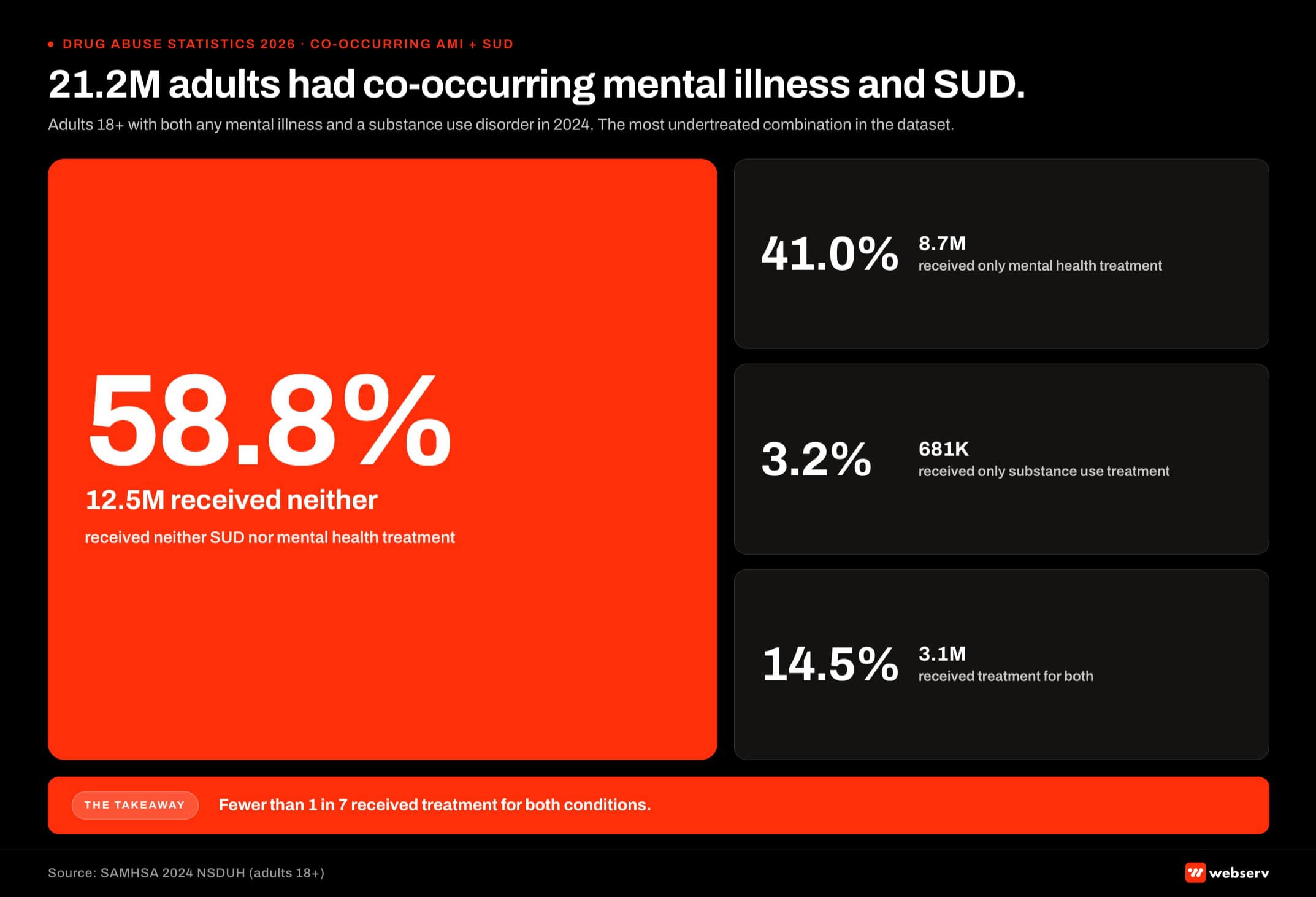 Two by two grid infographic titled ‘21.2M adults had co-occurring mental illness and substance use disorder in 2024.’ The 2×2 maps the co-occurring AMI plus SUD population by treatment receipt. Quadrants: received treatment for both (top left), received treatment for AMI only (top right), received treatment for SUD only (bottom left), and received neither (bottom right). 58.8 percent of the 21.2 million co-occurring population received neither, the largest quadrant by far. Source: SAMHSA 2024 National Survey on Drug Use and Health.
Two by two grid infographic titled ‘21.2M adults had co-occurring mental illness and substance use disorder in 2024.’ The 2×2 maps the co-occurring AMI plus SUD population by treatment receipt. Quadrants: received treatment for both (top left), received treatment for AMI only (top right), received treatment for SUD only (bottom left), and received neither (bottom right). 58.8 percent of the 21.2 million co-occurring population received neither, the largest quadrant by far. Source: SAMHSA 2024 National Survey on Drug Use and Health.Mental health and co-occurring conditions
The mental health prevalence data for adults aged 18+ comes from the NSDUH AMI and SMI modules.
| Metric | 2024 estimate (adults 18+) | Source |
|---|---|---|
| Any mental illness (AMI) | 61.5 million (23.4%) | SAMHSA 2024 NSDUH |
| Serious mental illness (SMI) | 14.6 million (5.6%) | SAMHSA 2024 NSDUH |
| Major depressive episode | 21.6 million (8.3%) | SAMHSA 2024 NSDUH |
| Co-occurring AMI + SUD | 21.2 million (8.1%) | SAMHSA 2024 NSDUH |
| Co-occurring SMI + SUD | 6.8 million (2.6%) | SAMHSA 2024 NSDUH |
| Either AMI or SUD | 86.6 million (33.0%) | SAMHSA 2024 NSDUH |
| Adults with AMI who received mental health treatment | 32.0 million (52.1% of AMI) | SAMHSA 2024 NSDUH |
| Adults with SMI who received mental health treatment | 10.3 million (70.8% of SMI) | SAMHSA 2024 NSDUH |
Co-occurring AMI + SUD treatment receipt
This is the most-undertreated combination in the dataset.
| Treatment outcome | Percentage | Number |
|---|---|---|
| Received neither SUD nor mental health treatment | 58.8% | 12.5 million |
| Received only mental health treatment | 41.0% | 8.7 million |
| Received only substance use treatment | 3.2% | 681,000 |
| Received both | 14.5% | 3.1 million |
What this means for treatment centers: Of 21.2 million adults with both AMI and an SUD, fewer than 15% received treatment for both conditions in 2024. Dual-diagnosis-capable programs have a defensible market position because the demand is genuinely unmet.
Suicide indicators
| Indicator | 2024 estimate | Source |
|---|---|---|
| Adults 18+ with serious thoughts of suicide | 12.7 million (4.9%) | SAMHSA 2024 NSDUH |
| Adults who made a suicide plan | 4.6 million (1.8%) | SAMHSA 2024 NSDUH |
| Adults who attempted suicide | 2.2 million (0.8%) | SAMHSA 2024 NSDUH |
| Adolescents 12–17 with serious thoughts of suicide | 2.6 million (~10%) | SAMHSA 2024 NSDUH |
| Adolescents who made a suicide plan | 1.2 million (4.6%) | SAMHSA 2024 NSDUH |
| Adolescents who attempted suicide | 700,000 (2.7%) | SAMHSA 2024 NSDUH |
Adolescent suicide attempt rate declined from 3.6% in 2021 to 2.7% in 2024. Young adult (18–25) suicide attempt rate also declined, from 2.8% in 2021 to 2.0% in 2024. Adults aged 50+ showed an increase, from 0.2% in 2021 to 0.6% in 2024.
What this means for treatment centers: Adolescent and young adult indicators are improving. Adult 50+ indicators are deteriorating. Programs serving older adults should expect to see this in intake.
Drug supply trends 2024–2026
These trends are not from NSDUH (which doesn’t track supply); they come from DEA seizures, CDC mortality, and recovery-research aggregations.
Fentanyl and synthetic opioids:
- Synthetic opioid deaths fell 34% from 83,140 (2023) to 54,743 (2024) per CDC
- Fentanyl pill seizures rose 2,300× from 2017 (49,657) to 2023 (115.5 million) per DEA
- Pills now represent 49% of fentanyl seizures vs. 10% in 2017
- Counterfeit pills containing lethal fentanyl doses rose from 40% (2020–2021) to 70% (2023–2024) per DEA lab analysis
Polysubstance and adulterants:
- 47% of 2023 overdose deaths involved opioids + stimulants (the “fourth wave”)
- Cocaine-involved deaths up 85% from 2019 to 2023
- Xylazine (“tranq”) involved in approximately 11% of U.S. overdose deaths in 2022, up from near zero in 2015
- Medetomidine, a stronger veterinary anesthetic than xylazine, detected in 37% of opioid samples in October 2025 vs. 4% in May 2024
- Nitazenes (synthetic opioids up to 100× stronger than fentanyl) emerged in the U.S. supply 2023–2025
Youth-specific exposure:
- Fentanyl is the leading cause of death among Americans aged 15–24
- An estimated 80% of teen and young adult fentanyl poisoning deaths can be traced to social media contact (DEA “Operation Last Mile” data)
What this means for treatment centers: Intake assessments built around the 2018–2020 supply environment will miss adulterant exposure, social media procurement patterns, and counterfeit pill identification. Toxicology screens beyond standard drug panels are increasingly necessary. Naloxone protocols sized for fentanyl may not reverse xylazine sedation effects.
What treatment center operators should do with these numbers
The point of a statistics article isn’t the statistics. It’s what an operator does next.
1. Calibrate market sizing to the treatment gap, not to SUD prevalence: your addressable market isn’t 48.4 million people with an SUD. It’s the 10.2 million people currently receiving treatment plus the prospective subset of the 42.4 million unmet-need population whose access barriers your program can credibly resolve.
2. Update intake assessments for polysubstance and adulterant reality: a patient who reports “just cocaine” or “just Xanax” in 2026 may be fentanyl- or xylazine-exposed, and standard naloxone protocols don’t reverse xylazine. Toxicology screens beyond standard 5-panel and 10-panel testing are clinically warranted.
3. Lower admission barriers where you can: same-day access, low-barrier entry, telehealth options, and meeting patients at their current stage of change all move the conversion rate from “needed treatment” to “received treatment.” Waiting lists, insurance complications, and requirements for prior abstinence keep people out of the 19.3% who actually receive care.
4. Build dual-diagnosis capacity: 21.2 million adults have co-occurring AMI and SUD in 2024, and only 14.5% receive treatment for both. The gap is the largest single under-served population in the dataset.
5. Plan for MOUD-led care: only 17% of the 4.8 million people with opioid use disorder received MOUD in 2024. Programs that can credentialize for methadone, buprenorphine, and naltrexone have a defensible operating model in the 2026 supply environment.
Webserv works with treatment center operators to translate statistics like these into admit-attributable marketing programs, authority content, and admissions ops infrastructure that lower the access barriers operators can actually move. If you want a partner that operates on the operational implications of statistics like these, book an intro meeting.
A closing position on statistics articles in 2026
Most drug abuse statistics articles online cite 2018–2020 data because the publishers don’t update them. Google and AI search engines penalize that.
The opportunity for treatment center operators isn’t to publish the deepest statistics article. It’s to publish the most accurately-dated, government-source-cited, operationally-translated version of the statistics that already exist in primary releases. Operators who plan to old numbers underestimate both the polysubstance and the adulterant realities driving 2026 admissions.
We update this article when SAMHSA releases the next NSDUH (typically July or August), when CDC releases the next overdose mortality update (quarterly), and when supply trends change materially. The next update is expected in late summer 2026 when the 2025 NSDUH publishes.
If you spot a statistic in this article that conflicts with a more recent government release, send us the source. We will update the number and credit the catch.
Sources
- Substance Abuse and Mental Health Services Administration. (2025). Key Substance Use and Mental Health Indicators in the United States: Results from the 2024 National Survey on Drug Use and Health (HHS Publication No. PEP25-07-007, NSDUH Series H-60). Center for Behavioral Health Statistics and Quality. SAMHSA NSDUH national releases.
- Centers for Disease Control and Prevention. (2025, May 14). U.S. overdose deaths decrease almost 27% in 2024 [Press release]. CDC NCHS Press Room.
- Centers for Disease Control and Prevention. (n.d.). Vital Statistics Rapid Release: Provisional Drug Overdose Death Counts. CDC NCHS VSRR.
- Centers for Disease Control and Prevention. (n.d.). Understanding the Opioid Overdose Epidemic. CDC Overdose Prevention.
- National Institute on Drug Abuse. (2024, August 21). Drug Overdose Deaths: Facts and Figures. NIDA.
- Drug Enforcement Administration. DEA Lab Analysis and Operation Last Mile. Federal seizure data through 2024.
Olivia Birkbeck supports content production at Webserv, a behavioral-health-first SEO and digital marketing agency. Statistics in this article are sourced from primary U.S. government data releases; the operational commentary is Webserv’s own.






