BEHAVIORAL HEALTH BILLING & RCM AGENCY
You're Spending More on Marketing Than You're Collecting
Most treatment centers assume growth is a volume problem. The ones who scale profitably know the bottleneck isn’t at the top of the funnel, it’s between admit and cash.
Trusted by 200+ Treatment centers nationwide



THE PROBLEM
More Admits Doesn't Mean
More Revenue.
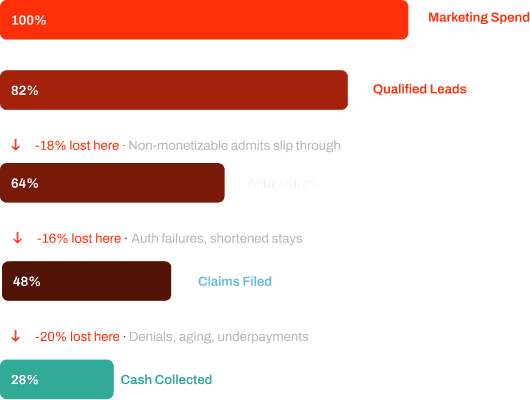
Every stage between admit and collected cash is an opportunity for revenue to disappear, and most facilities have no system built to stop it.
Non-Monetizable Admits
Leads that pass through intake but don't have qualifying insurance, costing you a bed and a missed opportunity
Authorization Failures
Shortened stays and denied auths that cut revenue per patient before they've even left
Delayed Claims Submission
Every day a claim sits unsubmitted is a day your cash is aging
Aging AR
Receivables stacking up past 90 days with no structured follow-up cadence
Underpayments Going Undetected
Payers paying less than contracted rates with no one catching it
No Visibility Into Cash
Reporting that shows census and leads but can't tell you what actually hit the bank
Here's Exactly Where It's Happening
Revenue doesn’t disappear all at once. It bleeds out at five specific points between admit and bank deposit, and most facilities can’t see any of them.
01
VOB
Non-monetizable admits
02
Authorization
Shortened stays
03
Claims
Delayed submission
04
Follow-Up
Aging stagnation
05
Reconciliation
Cash mismatch
When 2–3 of these break simultaneously, marketing metrics look strong — but your bank account tells a different story.
We Don't Patch Leaks.
We Rebuild the Pipe.
Four services that close every gap between admit and collected cash, so your marketing spend produces revenue you can actually bank.
VOB Performance
Fast, accurate benefits verification so your team only admits patients who are monetizable — before they take a bed.
What's Included
- VOB turnarounds under 2 hours
- Plan-level OON reimbursement predictions
- Nights and weekend coverage
- Insurance monetizability scoring
Utilization Review
Every patient tracked from approved to expiring — so authorized stays are maximized and no revenue walks out the door early.
What's Included
- Auth tracking across all active patients
- Clinically justifiable stay maximization
- SCA execution and documentation
- Payer appeal support
Collections
90% of claims processed within 90 days, with aggressive underpayment detection and structured follow-up so aging AR stops compounding.
What's Included
- Claims submission and follow-up
- Underpayment detection and recovery
- Denial management and appeals
- TPA negotiations
Payments Posted & Reporting
Cash reconciled to the bank — not just what's posted. Real-time dashboards and clean AR segmentation so you always know exactly where your revenue stands.
What's Included
- Bank-tied cash reconciliation
- Real-time Looker Studio dashboards
- Denial root-cause analytics
- Clean AR segmentation
THE OUTCOME
Marketing becomes a capital allocation engine.
When revenue realization is strong, everything downstream improves — and compounds.
01
Realized ROAS
Cash-based, not census-based
02
Defensible CAC Payback
Measurable and modelable
03
Smarter Budget Scaling
Confident, not anxious
04
Channel-Level ROI
Optimize toward profitability
05
Predictable Cashflow
Forecastable within 90 days
06
Board-Level Confidence
Clean books, credible reporting
$2.1M in Aging AR. Stabilized in 90 Days.
An Arkansas facility came to us with $2.1M in accounts receivable — 35% aged past 90 days. Within one quarter, the picture looked completely different.
Top Result
$1.1M Collected in 90 Days
From $2.1M starting AR
97% Collectible AR Recovered
1% Denial Rate
Down from 20%
<2hrs VOB Turnaround
Down from 24 hours
IS THIS RIGHT FOR YOU?
We're selective about who we work with.
If your marketing is working but your bank account doesn’t reflect it, this is designed for you.
Strong Fit If
- Spending $100K+/month on marketing — or actively scaling toward it
- OON, INN, or hybrid — SUD, MH, or ED programs
- Your marketing metrics and actual cash collected don't match
- Want one accountable system — not two vendors pointing at each other
Not a Fit If
- Currently in an active payer audit
- Not ready to invest in revenue operations alongside marketing
We'd rather tell you that now than take your business and underdeliver.
MARKETING SERVICES FOR REHABS
See The Whole Patient Acquisition System
Organic Admissions
Build sustainable, long-term patient acquisition through search visibility and content authority.
Paid Admissions
Drive immediate results with targeted advertising and optimized conversion experiences.
Admission Ops
Streamline your admissions process with data-driven operations and conversion tracking.
Performance Creative
Websites, landing pages, and ad creative built as part of the patient acquisition system.
COMMON QUESTIONS
Frequently Asked Questions About Behavioral Health Billing
Behavioral health billing is the end-to-end revenue-cycle process for mental health and substance use disorder treatment programs — covering verification of benefits, prior authorization, concurrent utilization review, claim submission, denial management, and patient-responsibility collection. It differs from medical billing because of ASAM-based authorization, longer levels of care, and 42 CFR Part 2 consent management.
The workflow has more handoffs than general medical billing. Each level-of-care transition (detox → residential → PHP → IOP) requires re-authorization and updated documentation. Programs that drop a single handoff routinely lose 5–15% of authorizable revenue to that one failure mode.
Strong BH billing isn't just claim submission — it's the operational discipline that turns clinical work into collected revenue. The two parts can't be separated; programs that try usually find the gap shows up in cash flow.
BH billing handles ASAM-based level-of-care placement, longer episode lengths with weekly concurrent review, single-case agreements for out-of-network admissions, and 42 CFR Part 2 record-handling. Generic medical RCM firms often underperform on BH because the workflow is fundamentally different from inpatient medical billing despite using overlapping CPT codes.
The CPT codes are where most generalist firms get confused. They see familiar codes and assume the workflow is familiar. But BH-specific authorizations, level-of-care transitions, and SCA negotiations don't exist in medical billing — and missing them means missed revenue.
We've audited BH programs being billed by national medical RCM firms and routinely find 8–15% of revenue going uncollected because of workflow gaps the medical firm doesn't recognize as gaps.
Best-in-class programs run BH denial rates under 8%, with leading programs under 5%. The most common denial sources are insufficient ASAM dimensional documentation, missed concurrent-review windows, and prior-authorization gaps at level-of-care transitions. Each is recoverable with disciplined UR documentation and a tight intake-to-billing handoff.
Programs with denial rates above 15% almost always have an upstream process problem, not a billing problem. The fix lives in clinical documentation discipline and concurrent-review cadence — fixing the billing team alone won't move the number.
Recovery is achievable. Programs that adopt structured ASAM documentation and disciplined UR cadence routinely cut denial rates in half within 90 days.
It depends on volume. Programs under 30 beds often outsource (4–9% of net collections is the typical rate). Programs over 50 beds frequently benefit from in-house VOB and UR with outsourced overflow billing and denial management. Hybrid is increasingly the dominant model — operators control the front-end revenue path while specialists handle volume claim work.
The decision shouldn't be cost-driven. The right question is which model gets the highest collection rate per dollar of operating cost. In-house VOB and UR almost always wins because those are the upstream activities that determine whether downstream billing is even possible.
We see programs flip the decision the wrong way often: outsourcing UR to save money, then losing 10% of revenue to documentation gaps. Penny wise, pound foolish.
Days Sales Outstanding (DSO under 50 days), clean-claim rate (above 95%), denial-overturn rate on appeal, net-collection rate, and authorization-win rate. Programs tracking only AR aging miss the upstream KPIs — VOB completeness, UR documentation quality — that drive every downstream outcome.
DSO is the headline metric most operators watch, but it's a lagging indicator. By the time DSO drifts above 50, the upstream problems started 60–90 days earlier. Tracking VOB completeness and UR documentation quality weekly catches issues before they show up in DSO.
Clean-claim rate is the second-highest-leverage KPI. Every claim that requires rework costs 3–5x more in operational time than a clean claim. Pushing clean-claim rate from 85% to 95% is usually a 30–40% reduction in billing operating cost.
Because admit volume without collected revenue isn't growth. Marketing brings inquiries to the door; billing closes the financial loop. Webserv treats billing as upstream of marketing efficiency — every dollar of unbilled or under-billed revenue is a dollar that can't fund the next acquisition cycle. The two are inseparable for sustainable growth.
The traditional model treats marketing and billing as separate departments. That model fails for treatment centers because the two are economically linked. A center that improves billing collections by 15% can effectively double its marketing budget without spending a dollar more.
We've watched programs spend 6 figures on marketing while leaking revenue at the billing stage, then run out of cash before the marketing investment paid back. Fixing billing first is often the highest-ROI marketing decision a program can make.
Most programs see meaningful AR cleanup within 60–90 days of process changes. Underlying revenue-cycle improvements — DSO compression, denial-rate reduction — typically take 4–6 months to show in P&L. Programs with stuck legacy AR over $1M may require parallel claim-rework sprints alongside the new-process build.
The first 30 days are usually about diagnosing root causes — VOB completeness, UR documentation quality, claim scrubbing patterns. The next 60 days are about implementing process changes that prevent the same patterns from recurring.
Legacy AR over $1M usually has a long-tail of partially-collectible claims that need targeted rework. We treat that as a separate sprint from the new-process build, because trying to do both at once dilutes both.
Direct and consequential. A program with weak billing converts a marketing-driven admit at 60–70% of true revenue value vs a strong-billing program. Said another way: a 30% billing leak means every $100K of marketing spend is effectively performing as $70K. Fixing billing is often the highest-ROI marketing decision a program will make.
Treatment center CFOs and CEOs we work with often don't see this connection until we show it in their numbers. The marketing team gets blamed for low ROAS while the billing team gets blamed for slow collections, and neither sees that they're describing the same gap.
Fixing billing first frees operating cash to fund marketing aggression. Programs that try to outpace a billing leak through more marketing spend almost always run out of cash before the marketing pays back.
Ready to Grow?
Your marketing is working. Your cash shouldn't tell a different story.
30-minute strategy session to discuss your census goals, current challenges, and how we can help you scale admissions sustainably.
- 9 years exclusively serving behavioral health
- Helped clients generate 2,000+ admits in 2025
- We'll create a custom roadmap for your facility
Trusted by 200+ Treatment centers nationwide