The Asset That Keeps Working When Your Ads Don't
Paid media is a faucet. Turn it on, leads flow. Turn it off, or watch performance dip, and the pipeline dries up almost immediately. Most facilities understand this intuitively, but fewer act on what it implies: if paid is your only channel, you're one bad month away from a census problem.
Organic is different. It builds slowly, requires real investment, and won't show meaningful results in the first 90 days. That's exactly why most facilities underprioritize it, and exactly why the ones that commit to it end up with such a durable advantage. An SEO engine that's been running for two or three years doesn't care if your Google Ads account has a bad quarter. It keeps generating leads regardless.
For smaller facilities with limited budgets, the organic argument is even more important. Every dollar invested in SEO compounds over time. The content you publish this month is still driving traffic 18 months from now. The rankings you build this year are an asset on your balance sheet in ways that paid spend never will be. We've seen facilities acquired by private equity where the website itself — the domain authority, the content library, the organic traffic — was a meaningful part of the valuation conversation. That's not a marketing outcome. That's a business outcome.
Technical foundation, keyword strategy built around treatment intent and payer mix, and rankings that attract patients who are ready to call, not just browsing.
Learn more →Content that answers the questions families ask in a crisis. Every piece mapped to search intent, insurance viability, and level of care, not just traffic volume.
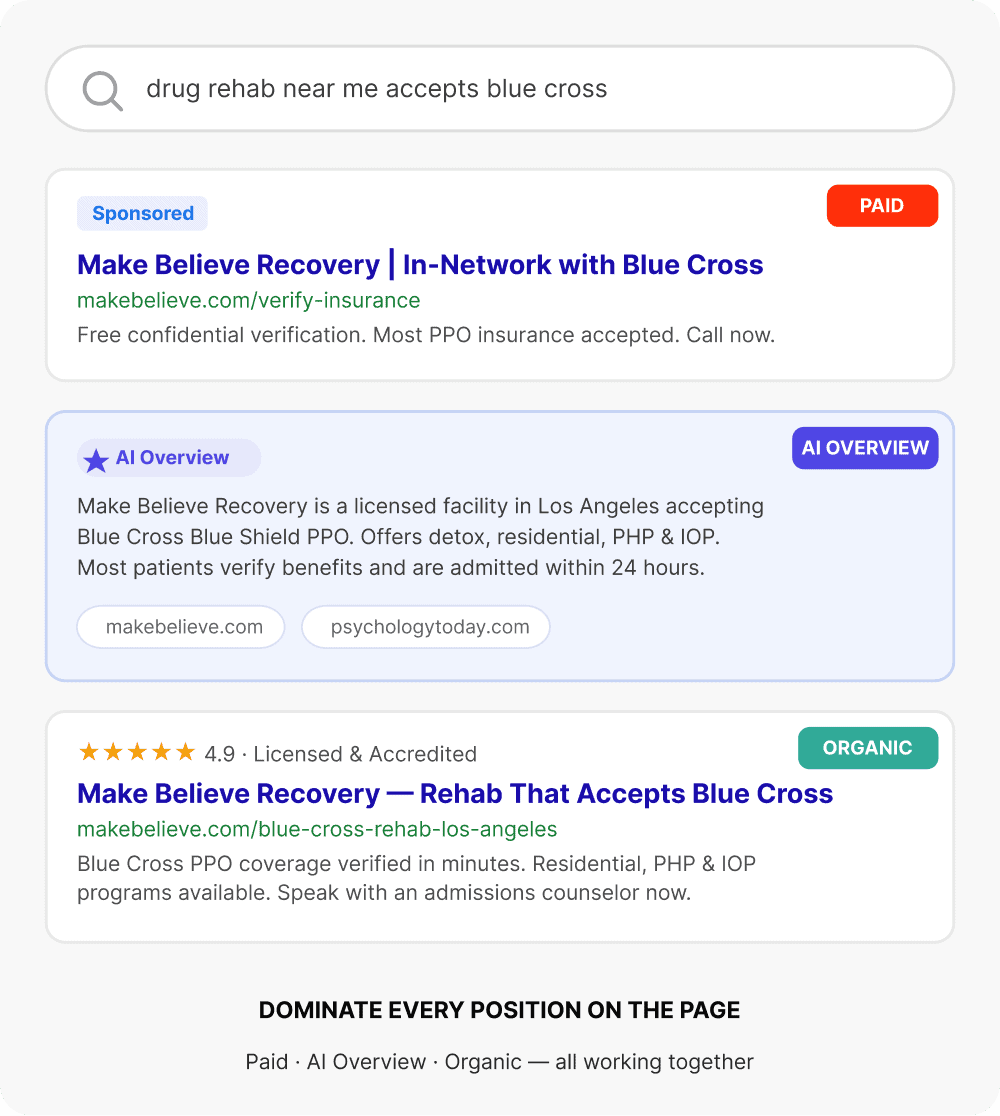
Learn more →Treatment center operators are starting to ask how to show up in AI-generated search results. The answer is authoritative, well-structured content, but the execution is different. We build for both.
Learn more →Backlinks from behavioral health directories, treatment resources, and industry publications that build domain authority and reinforce topical relevance in the eyes of search engines.
Learn more →SoCal Sunrise
SoCal Sunrise committed to organic as a primary channel. Eighteen months later: 85 admits attributed directly to organic search, 2,297% ROI, and a website that was generating leads on nights, weekends, and the three days their PPC campaign went dark during a billing issue. That's not a campaign result. That's what the asset looks like when it's mature.
Read the full case study →Organic isn't the fast play. It's the right play. For facilities that want to stop being entirely dependent on paid spend to fill beds, it's the most important long-term investment in the system.
Tools & Resources
Everything Referenced in This Guide — In One Place
Every tool, benchmark, playbook, and case study we've built for behavioral health operators. Start with what's relevant to where you are in your patient acquisition system right now.
Benchmarks
Industry data on CPL, cost per VOB, cost per admit, and LTV:CAC across 50+ behavioral health facilities.
Tools
Free calculators and diagnostic tools built specifically for treatment center operators and behavioral health marketers.
Playbooks
Deep-dive guides on every component of the patient acquisition system — written for operators who want to understand the strategy.
Blog
Tactical articles on SEO, paid media, CRO, and admissions operations from nine years in behavioral health marketing.
Glossary
Plain-language definitions for every metric and concept in behavioral health patient acquisition — CPL, LTV:CAC, payer mix, and more.


Paid Admissions Playbook
Paid search, paid social, and CRO strategy built for behavioral health.
Organic Admissions Playbook
SEO, content, digital PR, and AEO as a connected system.
Admission Operations Playbook
CRM, VOB workflow, speed to contact, and team enablement.


